Home » Dementia (Page 2)

‘Living better with dementia': a global perspective
My book, to be published in June 2015, is intended as a ground-breaking analysis of the challenges for living w ell with dementia, highlighting innovation and good practice for improving dementia care practice and policy in the future. What do national dementia strategies, constantly evolving policy and ongoing funding difficulties mean for people actually living well with dementia?
Adopting a broad and inclusive approach, I present a thorough critical analysis of existing dementia policy with emphasis on the English jurisdiction (but mindful of the global perspective), and I tackle head on current and controversial topics at the forefront of public and political debate, such as diagnosis in primary care, access to services for marginalised groups, stigma and discrimination, integrated care, personal health budgets, personalised medicine and the use of GPS tracking.

Drawing on a wealth of diverse internally peer-revieweed research, and including voices from all reaches of the globe, I identify current policy challenges for living well with dementia, and highlights pockets of innovation and good practice to inform practical solutions for living better w ith dementia in the future.
This is intended to be a unique and cohesive account of where dementia care practice and policy needs to head, and why, and how this can be achieved, this is crucial reading for dementia care professionals, service commissioners, public health officials and policy makers, as well as academics and students in these fields.
Synopsis
Chapter 1 provides an introduction to current policy in England, as it currently stands, including a review of the need for a ‘timely diagnosis’ as well as a right to timely post-diagnostic care. This has been a vocal concern of Baroness Sally Greengross, the current Chair of the All Party Parliamentary Group for dementia. This chapter also provides an overview of the current evidence base of the hugely popular “Dementia Friends” campaign run very successfully by the Alzheimer’s Society and Public Health England, to raise awareness about five key ‘facts’ about dementia. Indeed, Prof Martin Prince, Dr Renata Bryce and Dr Cleusa Ferri had previously introduced the critical topic of “The benefits of early diagnosis and intervention” in the World Alzheimer’s Report 2011.
A focus of this chapter is inevitably on prevention and risk factors, aligning itself well with the aims of the World Dementia Council.
Chapter 2 comprises a preliminary analysis of stigma, citizenship and the notion of ‘living better with dementia’. This chapter explains the urgency of the need to “frame the narrative” properly. This chapter also introduces the “Dementia Alliance International” group, which has fast become a highly influential campaigning force by people living with dementia for people living with dementia.
Critically, it has just been announced people living with dementia will be more involved in the work of the Alzheimer’s Disease International.
The statement from ADI reads thus:
The Board has agreed to start collaborating with Dementia Alliance International (DAI), an independent international group of people living with dementia. This will be done with a Memorandum of Understanding (MOU), with ADI agreeing to support the expansion of DAI to increase representation of people with dementia around the world, including those in lower and middle-income countries.
Overcoming stigma has become a massive issue.
Chapter 3 looks at the various issues facing the timely diagnosis and post-diagnostic support of people living with dementia from diverse cultural backgrounds, including people from black, Asian and ethnic minority backgrounds, people who are lesbian, bisexual, gay or transsexual, and people with intellectual difficulties. Attention is paid to the various intricate ways in which exact culture can impact not only on the timely diagnosis of dementia but also in the post-diagnostic care.
Here, for example, the diagnostic algorithm of 10/66 has been particularly influential.
Chapter 4 looks at the issue of how different jurisdictions around the world have formulated their national dementia strategies. There is remarkable convergence in the efforts of various jurisdictions, and it is here I first introduce the critical importance of collaboration.
A new report, ‘Improving Dementia Care Worldwide’ (PDF), reviews existing national dementia plans from around the world, and puts forward recommendations for governments on what a best practice plan should include and how it should be developed and implemented. The report was commissioned by ADI and Bupa, and written by Prof Anne Margriet Pot and Dr Ionela Petrea from the Netherlands Institute of Mental Health and Addiction (Trimbos-institute).
Chapter 5 looks at the intense care vs care debate which has now surfaced in young onset dementia. There is a potentially problematic schism between resources being allocated into drugs for today and resources being used to fund adequately contemporary care to promote people living better with dementia. The needs of people with young onset dementia are certainly distinct.
Chapter 6 focuses on delirium, or the acute confusional state, and dementia. It attempts to explain why delirium and dementia might converge in policy, after all.
Chapter 7 is the largest chapter in this book, and takes as its theme care and support networks. I make no apologies about the length of this chapter, as I have been hugely influenced by the Dementia Action Alliance Carers Call to Action in the last year. The need to help carers is certainly writ large in global policy.
Chapter 8 considers eating for living well with dementia. main focus of the chapter is how people with dementia might present with alterations in their eating behaviour, and how the mealtime environment must be a vital consideration for living better with dementia. In 2014, the ADI published their report on nutrition and dementia.
Chapter 9 looks at a particular co-morbidity, incontinence. Focusing on the various co-morbidities will be an opportunity of a whole person approach for a person living with dementia, during health as well as illness. The transition to a residential/care home, for example, can be profoundly influenced by difficulty in managing unmet needs such as incontinence; so unsurprisingly the efficacy of conservative approaches at home has experienced renewed scrutiny amongst a number of different jurisdictions.
Chapter 10 argues how the needs for people living better with dementia would be best served by a fully integrated health and social care service in the form of “whole person care”.
The World Alzheimer Report 2013 went into a foray of the “journey of care”. One of the key recommendations was:-
Health and social care systems should be better integrated so that there are co- ordinated care pathways that meet people’s needs. Case managers (one for up to every 60 people with dementia) are likely to add value when working from the community, across the journey of care, as part of a fully integrated long-term care system for older people.
Chapter 11 considers the importance of the social determinants of health. The framework, I argue, is eminently sensible for organising one’s thoughts about dementia friendly communities. Housing for living well with dementia is not just about buildings, and is pivotally enmeshed with the person centred care philosophy of projected English policy.
This is a critical part of WHO policy. There is more work to be done here to align this (and WHO “friendly cities”, which has found considerable interest in Alzheimer Europe) with global dementia policy as regionally implemented in local jurisdictions.
With such a broad brush tool as equality and “dementia friendly communities”, the scope for squashing diversity is enormous. Few topics enter the realms of “one glove does not fit all” to the same degree as the potential use of global positioning systems for dementia. Chapter 12 considers whether ‘wandering’ is the most appropriate term. The main emphasis of this chapter is the legal and ethical considerations in the use of ‘global positioning systems’ in enhancing the quality of life of persons with dementia and their closest ones.
Chapter 13 considers head-on a number of important contemporary issues, with a main emphasis on human rights and “rights based approaches”. While there is no universal right to a budget, the implementation of personal budgets is discussed. Dementia being defined as an equality totally alters the nature of the narrative of discussion, and that these principles apply across the world is bound to attract interest (such as the UN Convention on the rights of persons with disabilities).
Too often the debate about dementia can be engulfed in a diatribe about ‘cost’ not ‘value’. Persons living better with dementia wish to contribute effectively with the outside world, and the feeling is mutual. Chapter 14 is primarily concerned with art and creativity, which can be incredibly empowering for some people trying to live better with dementia. I feel that arts-based therapies offers much untapped potential for the future.
Too often the focus in international policies is on medications. Chapter 15 looked at the triggering of football sporting memories in people living well with dementia. This chapter considers the cognitive neuroscience behind this.
Chapter 16 looks at the impact of various innovations in English dementia policy, giving as examples including service provision (such as the policy on reducing inappropriate use of antipsychotics or the policy in timely diagnosis) and research.
This is within the construct of a major worldwide drive to innovations in service provision and research (as for example described here in a report on a workshop on “Enhancing Translational Research and Clinical Development in Alzheimer’s Disease and other Dementia: The Way Forward”, held on 11-12 November 2014, Lausanne, Switzerland.
Chapter 17 looks at how leadership could be promoted by people living with dementia themselves. I first introduce the need for this in Chapter 2. Chapter 17 considers who might lead the change, where and when, and why this change might be necessary to ‘recalibrate’ the current global debate about dementia.
Finally, I attempt a Conclusion at Chapter 18.

Living well with the dementia app. Back to the future?
Various inventions were predicted for 2015 in the film “Back to the Future”.
Of course, an invention is not the same as an innovation.
There is a subtle difference between these two words, but the difference is an important one.
An invention is the formulation of new ideas for products or processes, but an innovation is all about the practical application of new inventions into marketable products or services.
According to top HSJ pioneer, Dr Amir Hannan, innovation has a specific definition.
About doing or making something completely new that has never been done before, which leads to a material change in thinking, behaviour or outcomes.
One of the brilliant inventions/innovations was the “hover board”.

Probably a good thing these haven’t been invented for the mass market yet – though some clever bod has come up with a prototype – the baggy jeans and Converse look is just so Nineties.
The background to the modifiable factors relating to dementia are well rehearsed.
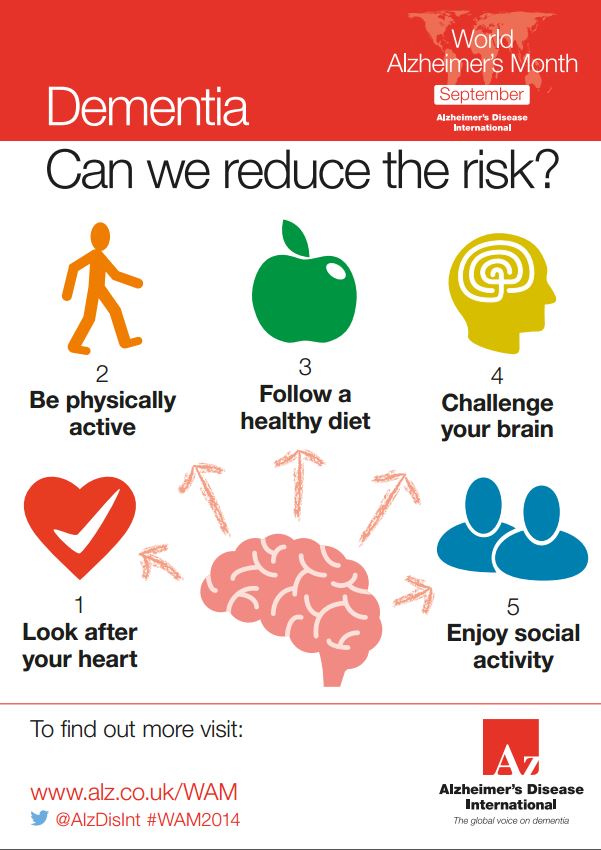
Approximately half of dementia cases might be attributable to known modifiable protective and risk factors (Smith and Yaffe 2014). The protective factors include the factors that determine brain development in early life such as maternal nutrition and health, and nutrition and cognitive development in early years. Education and lifelong learning also protect against dementia as does involvement in social networks. The risk of dementia is raised by substance abuse in adolescents and young people, head injuries and depression. Dementia also shares important risk factors with the major non-communicable diseases (NCDs) including cardiovascular disease, diabetes, cancers. These are the behavioural risk factors of physical inactivity, smoking, alcohol and poor diet, and the linked intermediate risk factors such as high blood pressure, raised cholesterol and obesity.
There has been some difficulty in getting this relatively simple public health message across.
This is illustrated, for example, by the rather resistant belief amongst people that ‘nothing can be done about dementia’. In fact, an enormous amount can be done to promote living well with dementia. And some factors may indeed slow rate of progression or delay onset, in a way we don’t properly understand yet.
Some campaigning initiatives have started to gain momentum, though. This infographic is from the Alzheimer’s Disease International “World Alzheimer Month”.
And there are developments afoot in the provision of information for patients.
Here’s an example of what Highbury Grange Medical Practice seem to be offering.
The aim is for all patients in England will have access to their GP medical records online by 31st March 2015. This means you can have secure access to relevant parts (current medications, immunisations and allergies)of your record from devices that can access the internet.
And now Sir Bruce Keogh has got really into ‘wearable technology':
It sounds reasonably convincing.
Prof Sir Bruce Keogh believes that gadgets similar to fitness trackers, which are growing in popularity, and others resembling games consoles will revolutionise the monitoring of patients’ health, especially those with a serious condition.
And…
“Technology is emerging which enables those to be brought together and transmitted through mobile phones or other methods where health professionals can analyse them and act upon any warning signs,” Keogh says.
Wearable technology could easily prove useful for people with heart failure – one of the most common causes of admission to hospital – and thus relieve the strain on overcrowded hospitals.
“I see a time where someone who’s got heart failure because they’ve had a previous heart attack is sitting at home and wearing some unobtrusive sensors, and his phone goes, and it’s a health professional saying: ‘Mr Smith, we’ve been monitoring you and we think you’re starting to go back into heart failure. Someone’s going to be with you in half an hour to give you some diuretics’,” says Keogh.
Technology “enables you to predict things, to act early and to prevent unnecessary admissions, thereby not only taking a load off the NHS but, more importantly, actually keeping somebody safe and feeling good”.
For people living well with dementia, simple apps could be made which could be installed on smartphones.

For certain persons living with dementia, prone to “wandering” (a term I very strongly dislike), GPS location devices might be of interest; but by no stretch of imagination are these devices relevant to all people living with dementia.
The app might also be able to monitor aspects of cardiovascular health. There is a strong link between cardiovascular health and cerebrovascular health, and indeed the success of tackling cardiovascular risk factors in primary care has caused some interest in the possible falling in England of the prevalence of dementia.
I have often ‘complained’ to other specialists in dementia how little we know about how easily people living with dementia, across different types of dementia, at different extents of ‘severity’, cope with all technology designed to help them live with dementia.
But it is possible that such apps could be designed to be compliant with the Equality Act (2010), offering giant lettering for those people with visual object perception problems, or ‘read aloud’.
There could be a set of questions like ‘Do you have trouble remembering dates?’, ‘Do you have problems remembering phone numbers”, “Do you have problems cooking?”, which could trigger further intervention by a community occupational therapist.
If someone living with dementia notices their legs going stiff, or they have trouble walking, a referral to a community physiotherapist could be triggered.
If someone living with dementia notices the development of a ‘sweet tooth’, a referral to a community dietitian could be triggered.
And so on.
There might be ‘menus’ which are more suitable to caregivers, who are often spouses, or children (particularly daughter and daughter in laws), but including paid carers. There are clearly ethical issues here.
I anticipate such apps will be of interest to people who’ve just been given a diagnosis of dementia, but the usual criticisms will hold (i.e. it’s another ‘to sell’ to someone with a personal budget, it’s “typical privatisation of health and care). But I feel we should be looking into the social prescribing of facility to those who desire them, as an alternative to expensive drugs which can have limited efficacy.
Back to the future..
or back to planet Earth.
Further reading
Smith D. and Yaffe K. (2014) Letter: Dementia (Including Alzheimer’s Disease) can be Prevented: Statement Supported by International Experts. Journal of Alzheimer’s Disease 38: 699–703 DOI 10.3233/JAD-132372
Leading Change in Dementia Diagnosis and Support: Actions to Inform Future National Strategy
It is estimated that in 2015 there will be 850,000 people living with dementia.
Having decided at the beginning of last year that I would to any conferences on dementia, I found myself attending the Alzheimer’s Show in London Olympia and Manchester; the Alzheimer’s Association conference in Copenhagen of a book signing, Alzheimer’s Europe conference in Glasgow (which was themed on autonomy and dignity; and human rights), Alzheimer’s BRACE in Bristol on the future, Dementia Action Alliance Annual conference 2015 and the Dementia Action Alliance Carers’ Call to Action 2015. So, in other words, I utterly failed.
I will be a guest on a panel in the plenary discussion for “Leading Change in Dementia Diagnosis and Support: Actions to Inform Future National Strategy” to be held at the King’s Fund on Tuesday 24th February 2015.
Full details of this one-day conference are here.
The hashtag for this event is
#kfdementia
.
Details of our discussion are as follows.
| 3.40pm | Panel discussion: shaping a new national strategyTake this opportunity to put your comments and questions to our expert panel about the key issues that need to be addressed when designing and delivering the next national strategy. George McNamara, Head of Policy and Public Affairs, Alzheimer’s Society in conversation with:
Beth’s father had vascular dementia for approximately the last 19 years of his life. She is now one of the U.K.’s leading campaigners on dementia and a Consultant, Writer and Blogger
Chris is in his early 50s and is living with young onset vascular dementia. Chris is a dementia friend champion and writes a regular blog to raise awareness. |
The following are very familiar “mutual tweeps” to me, and I wish them all well for their involvement on the day too.
- Professor Alistair Burns (@ABurns1907), National Clinical Director for Dementia
NHS England and Professor of Old Age Psychiatry, University of Manchester - Jean Tottie (@Jean_Tottie), Chair of the Life Story Network and Former Carer
- Jeremy Hughes (@JeremyHughesAlz), Chief Executive, Alzheimer’s Society
- Dr Martin Brunet (@DocMartin68), GP, Programme Director, Guildford GP Training Scheme
- Rachel Thompson (@raheli01), Admiral Nurses Lead, Dementia UK (invited)
- George McNamara (@George_McNamara), Head of Policy and Public Affairs, Alzheimer’s Society
- Richard Humphries (@RichardatKF), Assistant Director of Policy, The King’s Fund
- Beth Britton (@BethyB1886), Expert by Experience
Beth’s father had vascular dementia for approximately the last 19 years of his life. She is now one of the U.K.’s leading campaigners on dementia and a Consultant, Writer and Blogger - Gary Rycroft (@garyrycroft), Solicitor and Partner, Joseph A. Jones & Co Solicitors and Member, The Law Society Wills & Equity Committee
- Chris Roberts (@mason4233), Expert by Experience
- Tony Jameson Allen (@SportsMemNet), Director, Sporting Memories Network, and Winner of the Best National Initiative Award at Alzheimer’s Society National Dementia Friendly Awards 2014
Last year, I got off my backside and published my first book on dementia. Called “Living well with dementia: the importance of the person and the environment“, the aim of it was not to sell the ideology of ‘person centred care‘. It was instead a well meant introduction to the original work of Prof Tom Kitwood and personhood, which has been pivotal in double declutching away from the Pharma stranglehood on dementia postdiagnost pathways. My point was that a person living with dementia had a past and present which were going to influence his or her future, and an interaction with the environment (such as the outside world or ‘built environment’, assistive technology, design of the home, design of the ward, dementia friendly communities) were major determinants of a positive wellbeing.
The book was broad-ranging, and I felt signified a change in direction of the narrative away from ‘treatments for dementia’. I also tried to cover in a balanced and fair way how the National Screening Committee had arrived at their original decision not to recommend screening for dementia. This decision has now been upheld. As it happens, I agree with the conclusion of the National Screening Committee, but for slightly different reasons. I feel a lot of people focus on the lack of sensitive and specific inexpensive screening tests – and this must be correct. But I also feel that because of the minimal effort to build up an extensive coherent evidence base on the effect of psychosocial interventions on living well with dementia, you are never going to be able to satisfy the last requirement, of improving morbidity (if you cannot improve mortality).
I have previously written about this here.
I essentially don’t want to rain on the parade of wanting to find a cure or effective symptomatic treatments before 2025. But this expectation, I feel, has to be much better, as the track record in developing treatments thus far has been poor. It is now well appreciated that G8 dementia was ultimately contrived as a reaction to Big Pharma on dementia, and it must be acknowledged, I feel, resources allocated into Pharma should not be at the expense of relatively inexpensive methods for promoting living well with dementia for people who are currently living with a diagnosis.
My original contents were therefore as follows:
Foreword by Professor John R Hodges; Foreword by Sally- Ann Marciano;Foreword by Professor Facundo Manes; Acknowledgements; Introduction; What is ‘living well’?; Measuring living well with dementia; Socio-economic arguments for promoting living well with dementia; A public health perspective on living well with dementia, and the debate over screening; The relevance of the person for living well with dementia; Leisure activities and living well with dementia; Maintaining wellbeing in end-of-life care for living well with dementia; Living well with specific types of dementia: a cognitive neurology perspective; General activities that encourage wellbeing Decision-making, capacity and advocacy in living well with dementia; Communication and living well with dementia; Home and ward design to promote living well with dementia; Assistive technology and living well with dementia; Ambient assisted living and the innovation culture; The importance of built environments for living well with dementia; Dementia- friendly communities and living well with dementia; Conclusion; Index.
The essence of my emotions about ‘living well with dementia’ is that living well with dementia is not a slogan to sell a product or service. It is a genuine change in philosophy from the medical model, of diagnosis and treatment, to one which requires a long term care revolution. As Prof Sube Banerjee said last year at the Dementia Action Alliance annual conference, we don’t need high volume diagnoses which are of low quality; although we all agree that it is unacceptable that people should be languishing for ages waiting for a diagnosis, and diagnostic rates of people who want to be diagnosed appear poor. We need high quality diagnoses. And even Baroness Sally Greengross, the Chair of the All Party Parliamentary Group for dementia, readily admits that the post-diagnostic care and support could and should be much better.
Against quite a lot of resistance from people in the medical profession which at best was complete indifference and lack of recognition of my work, I found many people in the general public who have thanked me for my work. I am completely independent, so I do not draw an income from any of my work apart from minimal royalties for the book. I paid my way to go to all conferences I went to last year. I will again be paying my own way for travel and accommodation to go to the 30th Alzheimer’s Disease International conference in April 2015 in Perth, on “cure, care and the lived experience“.
I was specifically asked last year by a panel representing the General Medical Council which people had benefited the most from my book. They expected me to say Doctors, but in all honesty I reported that the book had been extremely positively received by caregivers and people with dementia.
And I was staggered when a colleague of mine sent out this innocuous tweet which was well receive which had 151 ‘favourites’.
I do passionately want things to change for people with dementia and caregivers, but I don’t think of myself as a player in change. I don’t call myself anything in wanting change to living well with dementia; this is particularly because I really don’t believe in job descriptions or titles. I get fussy about the fact I am a person living well with recovery from alcohol, and physically disabled, but I am not ‘ill’ and as such I don’t see myself as a ‘patient’. I am on the medical register, but I do not feel defined by that (I have spent a few years not on the medical register due to consequences from when I was actually exhibiting symptoms of an illness). I have written numerous papers and two books on dementia, but I do not see my self as an ‘academic’. But I am hugely passionate about English and global policy.
I don’t want post-diagnostic care and support in my jurisdiction to be so haphazard. I totally sign up to the drive towards better inclusivity and accessibility for people with dementia, but I personally wouldn’t call this policy drive in this country or abroad “dementia friendly communities”. I would feel uneasy with a policy called “black friendly communities” or “gay friendly communities”, as these terms encourage division for me. Besides, I know from my personal experience with disability that all manifestations of disability are not necessarily evident to external observers. To take as an example, I see double all the time due to a problem with my brain, after my six week coma due to meningitis in 2007 when I was in a coma. But no-one, from looking at me, would know that. I understand that some people who are disabled, even if they fit the ‘criteria’ of the term, do not wish to call themselves ‘disabled’.
But the point is that there is now extensive legal advice about the relationship between equality and human rights law and mental health (for example chapter 3 in the new code of practice over the Mental Health Act just published). I have in fact been invited to be on a panel to review what I anticipate to be a very influential document looking at how the law is influencing dementia policy from the Mental Health Foundation early this year. Putting this stuff on a legal footing means that it’s a serious requirement for facilities to be more than aspiration in meeting ‘dementia friendliness‘; it then becomes a legal obligation. Under this view, one would provide adequate signage for people known to have spatial navigation difficulties from a dementia, in the same way that you might build a wheelchair ramp for employees who used wheelchairs in your company.
I feel that this narrative is moving my way, and in the direction away from being given your diagnosis and the conclusion ‘nothing can be done’. Kate Swaffer, in Australia, has elegantly articulated this in detail as “prescribed disengagement” (for an excellent article on this, please see here). Kate has also written a paper on stigma in the Dementia Journal, which is particularly interesting as Kate lives with a dementia herself.
It is a general ignorance of dementia that was thought to contribute to stigma and discrimination against dementia. I often ask London cabbies what they know about dementia; these individuals tend to be extremely well informed about many things, but I have found that unless they have a personal ‘connection’ with someone with dementia they can know very little (but are extremely regretful about not knowing more). The “Dementia Friends” in the UK jurisdiction had an aspiration of making one million ‘dementia friends’, a figure arbitrarily plucked out of nowhere, but presumably based on the successful Japanese “befriending” campaigns.
They had a target of one million ‘dementia friends’ by March 2015 originally, but I understand that this initiative will now run for the whole of the year. And, at the time of speaking, they look as if they might just make it, according to their website:
I am a “Dementia Friends Champion”. I did my own Ph.D. in dementia at Cambridge under Prof John Hodges. I was the first person in the world to suggest a cognitive method for diagnosing behavioural variant frontotemporal dementia and explain its rationale. This paper is even cited in the chapter on dementia in the current Oxford Textbook of Medicine. I quite enjoy my sessions. I invariably get asked tougher questions in these sessions, which are well received, than I have ever received in academic conferences.
I have no doubt whatsoever that England will have its second national policy soon for 2015-20. An influential report from Alzheimer’s Disease International looked at the value of national plans in an excellent report last year. I have no involvement with the formation of the new strategy, but the composition of the group has been clearly provided.
Members of the ‘Dementia Advisory Group’ are:
- Chair Clara Swinson, Department of Health
- Deputy Chair Lorraine Jackson (Deputy), Department of Health
- Jeremy Hughes, Alzheimer’s Society
- Tom Wright, Age UK
- Helena Herklots, Carers UK
- Bruce Bovill, Carer
- Joy Watson and Tony Watson, person living with dementia and carer
- Graeme Whippy, Lloyds Banking Group (representative from the PM Challenge Dementia Friendly Communities Champion Group)
- Sarah Pickup, Hertfordshire County Council (representative from the PM Challenge Health and Care Champion Group)
- Martin Rossor, UCL (representative from the PM Challenge Research Champion Group)
- Paul Lincoln, UK Health Forum
- Helen Kay, The Local Government Association
- David Pearson, The Association of Directors of Adult Social Services
- Hilda Hayo, Chief Executive of Dementia UK
- Graham Stokes, Chair of Dementia Action Alliance
- Dawn Brooker, The University of Worcester
- Martin Knapp, London School of Economics
- Tim Parry, Alzheimer’s Research UK
- Simon Chapman, National Council for Palliative Care
- Jill Rasmussen, Royal College of General Practitioners Dementia Champions
- Martin Green, Care England
- Bridget Warr, UK Home Care Association
The terms of reference are here.
It is stated that the Advisory Group will:
1. Review the evidence on progress on dementia care and support over the last five years to identify where progress has been made, key challenges and gaps and priorities for action. This will include looking at the evidence on risk reduction and how the incidence of dementia could be reduced.
2. Consider what success could look like by 2020 in the following broad areas:
- Improving the provision and continuity of personalised health and social care for people with dementia and carers – this includes risk reduction, prevention, diagnosis, post-diagnostic support, the role of technology and new models of care.
- Promoting awareness and understanding.
- Building social engagement by actions of individuals, communities and businesses.
- Boosting dementia research capacity and capability, the opportunity for individuals to get involved in research and optimising knowledge transfer and pathways to impact.
- Improving support for carers including improving their health, wellbeing and experienc
- Cross-cutting: Supporting the education, training and development of the health and care and wider workforce.
- Cross-cutting: Global action on dementia
- Cross-cutting: Ensuring equity of access, provision and experience
This will include looking at what we can learn from international evidence and experience.
I feel that this would form a coherent strategy.
Whilst traditionally, it might be useful to consider campaigning for dementia in terms of ‘cure’, ‘care’ and ‘prevention’, in reality living well with dementia potentially straddles all three areas.
I believe it’s extremely important to have a large body of people with dementia and carers report back on what their needs are. Such committees have had a long history of involving people with dementia and carers which might appear tokenistic. The World Dementia Council has not even appointed a person living with dementia to sit regularly on their Council.
As far as future post-diagnostic care and support is concerned, we clearly can no longer have a situation where, once a diagnosis is made, some people with a diagnosis, friends and family are totally lost in the system, or even at worst lost to follow up. There appears to be little coordination of care, and sometimes there’s more signposting to services than actual services. There seems to be little coordination of information held for practitioner and professional care in primary and secondary care, and between health and social care. We have a ridiculous situation where people with dementia, some of whom can do very badly when they are admitted to hospital partly due to a distressing change in environment, cannot be discharged in a timely manner from hospital due to social care cuts in service provision.
There is a clear drive to person-centred care, and I feel a very good way of discovering personhood is to adopt a ‘life story’ approach. I anticipate that networks for life story and carers will be invaluable during the lifetime of the next parliamentary term 2015-20.
The current Government has continued with the longstanding policy drive towards personalisation promoting ‘choice and control’. However, there are nuances to how policy can be implemented; for example a rights-based advocacy approach might be considered by some preferable to the promotion of personal budgets, which poses issues about the lack of universality of care, scope for co-payments, further marketisation, and complete lack of choice if you run out of money.
The next Government will be bequeathed developments in the handling of NHS data for service care provision, and of course the new Care Act. Some reflections are here on the Care Act:
I feel the the main challenge, in my opinion, in policy is to introduce safely and in a competent way “whole person care“. It’s going to take a lot of bottle to integrate properly health and social care, with all the challenges which endure, including breaking down organisational boundaries, cultural silos, facilitating competent knowledge sharing sand transfer, and a complete cultural change unfreezing from the biomedical model to one which recognises abilities not making feel inadequate because of their disAbilities. I would very much like to see the medical profession put some effort into the annual ‘follow up’. The point of this check up is not to chart with meticulous accuracy has changed in brain scans, psychology, or blood tests, meritorious though these initiatives are. The point about these follow ups is to ensure that there is a synchronised system of post-diagnostic care and support and everything is being done to improve living well with dementia (for example encouraging social networks and mitigating against social isolation). I feel personally the next Government should implement a “year of care” for dementia.
This change can only come from a social movement led by the major stakeholders themselves – people living with dementia and caregivers. A “top down reorganisation” will not work.
And I would prefer leaders in dementia not to be a Prime Minister but in fact to a person living with dementia. I think that way the needs of people currently living well with dementia will be better addressed, not just in service provision but also in research spend. I believe strongly that people newly diagnosed should have access to ‘dementia advisers’ and a properly resourced network of clinical nursing specialists. These nursing specialists are vital in pro-active case management, but the evidence base does need exploring further. The development of the personalised care plan, which can hopefully avert crises to encourage relaxed effective care out of hospital where possible. I have written about dementia specialist nurses, previously, here.
My interests are reflected in my new book ‘Living better with dementia: looking to the future’ due to be published on June 18th, 2015.
The contents are here.
1. Introduction. 2. Framing the narrative for living well with dementia. 3. Thinking globally about living well with dementia. 4. Culture and living well with dementia. 5. Young onset dementia and living well with dementia. 6. Delirium and dementia: are they living well together in policy. 7. Care and support networks for people living with dementia. 8. Introduction to autonomy and living well with dementia. 9. Can living well with dementia with personal budgets work? 10. Incontinence and living well with dementia. 11. Nutrition and living well with dementia. 12. Art and creativity in living well with dementia. 13. Reactivating memories and implications for living well with dementia. 14. Why does housing matter for living well with dementia. 15. Networks, innovation and living well with dementia. 16. Promoting leadership. 17. Seeing the whole person in living well with dementia. 18. Conclusion.
I think this book is more ambitious than the first one. In keeping with my original research interests, I consider why art and music are so important for living well with dementia. I also propose a new theoretical framework, the first in the world to my knowledge, why reactivation of “sporting memories” works. The “Sporting Memories Network” has been a very impressive initiative thus far in promoting wellbeing.
Finally, I wish everybody luck in formulating our new English dementia policy to be implemented within the lifetime of the next Government. It is imperative that the views of the community of people living with dementia and the army of approximately 5.4 million unpaid caregivers are prioritised above the needs of others, I feel, above all.

Can #thoughtdiversity promote employment for persons living well with young onset dementia?

“Thought diversity“, I feel, is fundamentally in tune with what I feel about the ethos of living well with dementia: recognising what people can do, rather than what they can’t do.
This is particularly useful in one particular context. The general topic of thought diversity in the workplace recently has received some deserved attention. There are two important approaches in this context of performance management in the workplace: equality and diversity.
I am certainly not about to suggest what an employer should do; nor what a person who may be about to receive a diagnosis of probable young onset dementia might do. I am just going to think about how thought diversity could be used to produce an effective skills mix for the employer, so that any individuals with young onset dementia can still contribute to the full.
Equality legislation
Equality tackles an imbalance where some people may be considered treated badly due to the effect that a protected characteristic has (such as age, sexual orientation, or race, for example); diversity is simply accepting that everyone is different. Legally, dementia can be defined as a disability under the guidance of the Equality Act (2010).
It is essential to recognise the functioning of the Equality Act (2010) for dementia. Disability is a “protected characteristic” under that statutory instrument. Prohibited conducts, like indirect or direct discrimination, are unlawful; reasonable adjustments must be made for disability. The Act specifically states that employees are under a duty to take reasonable adjustments to provide aids/ auxiliary services if these could alleviate any disadvantages and costs and not be passed on to the employee.
What is this equality?
But in political philosophy, the question has, in sophisticated circles, become “equality of what?”
As Anne Phillips describes in a paper for the London School of Economics:
“Two themes have become part of the common-sense in current thinking about equality.
The first is that defining equality in terms of outcome – equalising where people end up rather than where or how they begin – displays a distressing lack of sophistication.
Such a definition immediately begs the question of what we are seeking to equalise (income? happiness? welfare?), and seems to forget that measures to deliver equality on one of these metrics will deliver inequality on another.
Equalising resources notoriously overlooks the diversity of preferences and tastes: since what people want varies enormously, any strict division of the world’s resources will leave each of us with an excess of what we consider worthless and probably too little of what we really desire.
Yet if we turn instead to equalising people’s sense of well-being, we may end up giving more to the constitutionally dissatisfied than to the easily content. Defining equality in terms of outcome presumes an easy answer to the ‘equality of what?’ conundrum, gliding over complex issues of what equality means.”
The “equality of outcome“, for example, causes a particular controversy, arguably.
“Researchers concluded that equality of outcome was patronising, humiliating and embarrassing to minority groups. It could be socially divisive and evidently fuelled hostility and resentment in areas where prejudice previously did not exist as a serious social problem.”
An approach based on equality for young onset dementia
The basic accusation is that attempts for equality end up being rather artificial, but it is true that treating dementia as a disability to promote equality, arguably, must be a more useful starting point that a policy where citizens are merely “friendly” to people living with dementia with cognitive impairments such as problems in memory. Dementia is considered ‘young onset’ when it affects people of working age, usually between 30 and 65 years old. It is also referred to as ‘early onset’ or ‘working-age’ dementia. And it might appear meritorious for an employer to everything in his or power to keep a person with young onset dementia in a job, by providing ‘reasonable adjustments’ such as adequate signage, diaries or memory aids.
But is this approach based on equality necessarily the right approach?
It’s already conceded there’s a fair distance to go to make enforcement against disability discrimination offences a reality. Making goods and services easier for disabled customers has been a policy rumbling on for some time (see for example this document). Only last month, it was described yet again that access for disabled citizens to high street shops was “shocking”. The legal underpinning of this failure in equality is in contrast to the aspirational nature of ‘dementia friendly communities’ involving high street shops, such as in Fareham. In theory, it is all very well to say that an employee newly diagnosed with young onset dementia should be given reasonable adjustments as dementia is a known disability.
But there are some problems here. Some people with ‘soft symptoms’ may not wish themselves to be labelled with a disability, or a diagnosis, even if this means that they might be able to access certain finances. Also, in the majority, people with cognitive problems, who later go onto receive a diagnosis of young onset dementia formally, leave formal employment long before they receive that formal diagnosis (at which point the reasonable adjustments would have kicked in). We all know of employers who would really not want the bother of having to make reasonable adjustments, either for a person developing a dementia. And we know that all sorts of excuses tend to crop up prior to appointment of some employees in the first place. Somebody applying for a job, who is open about the fact he may be developing an early dementia, is unlikely to receive a sympathetic hearing in shortlisting.
But hold on a minute. Is it actually the employers’ fault?
The situation is very serious.
Kate Swaffer describes, through the construct called ‘prescribed disengagement‘ she was the first in the world to articulate, how people who have received a diagnosis of young onset dementia are, rather, actively encouraged effectively to give up by professionals in the health and care sectors. Work engagement, with some focused attention, could conceivably work though the strong determination of employers. For example, Robertson and colleagues (Robertson, Evans, and Horsnell, 2013) recently described an innovative demonstration program called “Side by Side” that was initiated to assess the feasibility of supported workplace engagement for people with younger onset dementia. This is truly laudable. People with young onset dementia, even if they have been demoralised by a cultural phenomenon of ‘prescribed disengagement’, might instead be encouraged to pursue positions in their current place of employment playing on their cognitive strengths. And this is recognised in ‘thought diversity’.
Is #thoughtdiversity a better option?
According to Deloitte’s excellent paper on ‘Thought Diversity’, acknowledging different thinking styles or cognitive diversity can beneficial for organisations to ‘hire differently, manage differently, promote differently’. In other words, employees can be matched up to tasks according to their cognitive strengths, and this includes people living in early stage young onset dementia. Such an approach would be more positive, beneficial for the employer and employee, focusing on what a person living well with young onset dementia can do, rather than what he or she can’t do. Such a workforce, it is anticipated according to Deloitte, might show greater resilience, and also be far less prone to ‘group think’.
I feel we do need to think ‘outside the box’, innovatively, to think how we get the best out of people. People who are about to receive a diagnosis of dementia may wish to stay in employment for as long as possible, as that is where friends are made, and of course the source of income comes at a critical time when there might be other commitments such as family, a mortgage or pension. Human resources will in time need better tools for identifying different cognitive styles. There will be in any team people who are more suited to remembering things, people who are good with words, people who are good with planning. Cognitive assessments, whether relatively informal psychometric tests for different cognitive styles or more detailed, might be able to identify what individuals are good at, such that a team might as a whole consist of the ‘right skills’ and might display cognitive diversity. This would, I feel, be an altogether more constructive to approach the issue of employment for people with young onset dementia, based more on diversity than legal equality.
But I do think both employer and employee need to know that these legal equality rights do exist, as they are potentially extremely powerful indeed.
Reference
Robertson, J., Evans, D., Horsnell, T. (2013) Side by Side: a workplace engagement program for people with younger onset dementia, Dementia (London), 12(5), 666-74.

Thought diversity is necessary for people living well with dementia to get a fair hearing
It is not uncommon for ‘special event days’ on dementia to feature one or two people living with dementia. Sometimes there are logistic difficulties in providing fair representation of people living with dementia at international conferences, even.
People living well with dementia who instead attend these events witness these events stuffed full of ‘experts’ or directors providing their missives. They often complain that the minimal representation which is actually provided is tokenistic.
Deep down, there is a concern that people living with dementia are merely superficially involved as bit part actors in the weaponisation of a Pharma-led “war against dementia”. There are very few ‘good news stories’ about people successfully living well with dementia, say still in employment or contributing value in some important way.
But how big institutions act can be rather different in behaviour than that on the ground.
James Kouzes and Barry Posner indicated in “The Leadership Challenge” that there are several decision-making myths:
1. The chief executive decides.
2. Decisions are made in the room.
3. Decisions are largely intellectual exercises.
4. Managers analyse and then decide.
5. Managers decide and then act.
Both domestic and international policy for living well with dementia, rather, has converged on the notion that persons living with dementia should be included at an early stage in key features of service provision and research into dementia.
For this strategy to bear fruit in England in 2015-20, it is not adequate to have minimal involvement with people with dementia, while the script is in effect written by large charities and corporates.
There has been recent interest in “thought diversity“, often called “cognitive diversity”, in giving full attention to the plurality of different opinions about issues. It is thought that this is not simply an alternative to an anti-discrimination policy, but is fundamental to all features of fairness, equality, justice and integrity.
I feel thought diversity from people living well with dementia is essential to mitigate against the risk of undue influence on policy from ‘experts’, some of whom have not even met a person living with dementia. Conversely, when people living with dementia get together to discuss issues important to them, such as through the virtual cafés of the Dementia Alliance International (a global umbrella organisation for people living with dementia), the power of decisions collectively made can be much more convincing. This is akin to the well rehearsed phenomenon of “crowdsourcing” or “friend sourcing”.
My disappointment with the policy strand of ‘dementia friendly communities’ in any jurisdiction is that it does not really appear to have captured the public’s imagination for social change, in the same way that Marshall Ganz describes for the Obama Campaign.
I think vital to making this a box office issue is to emphasise that dementia is not a fringe policy issue. There are possibly about close to 900,000 people living with dementia in the UK as we speak.
Torie Osborn in the National Civic Review provided an elegant way of moving forward:
“A new era of cross-cutting change making has arrived. It favors linking communities and sectors together into public and political will for solutions on big, thorny issues affecting everyone—issues that America has not tackled head on for a long time, if ever, such as rising inequality in the global economy and climate change.”
But this has necessarily reframed the diversity narrative – perhaps, as discussed by Osborn, more to “Yes we can!”
Here the “Yes we can!” is being shouted from the rooftops by people living with dementia themselves.
Also, I feel the insights from people living with dementia are essential in formulating the policy of how a community might be improved to improve the wellbeing, say perhaps in housing design. Such decisions are likely to be of a much higher standard in quality, in keeping with previous research, for example, from the the Intelligence Advanced Research Projects Activity (“IARPA”).
This is not simply about hoping for the best, in getting a range of opinions, hoping that some opinions will gain legs. It is known that the first person to speak in a meeting often influences all subsequent opinions. The same effect could occur, for example, if a CEO of a regulator or a dementia charity talks at the top of a billing of a special event or world conference, with people living with dementia stuffed later down the programme (or even last).
Or if there is a room of ten people, and one with a disparate view, the nature of joint decision making will mean that the nine will tend to make the tenth person conform to a group view. This phenomenon is well known from the studies of decision making in legal juries.
Exactly the same issues crop up again in the development of “dementia friendly communities” policy. While there are huge problems with this policy, possibly inadvertently causing division rather than true integrity and inclusion, it is possible the best we have currently both domestically and internationally. Change is often much easier from within, as Maya Angelou amongst others famously said.
NHS Improving Quality (“NHSIQ”), NHS Confederation and NHS Horizons have now a great opportunity in building on this work of “thought diversity”, building on the momentum which is thought to have begun in late 2010. Deloitte were noteworthy first movers in this field with their report, “Diversity’s new frontier” published by the Deloitte University Press.
An introduction to thought diversity on the NHSIQ website is here.
It is perhaps helpful to look at this widely shared webinar on ‘thought diversity’ which indicates the direction of travel of this in encouraging creativity and innovation in health policy.
I am struck by the true nature of the ‘rebel’. Carmen Medina (@milouness) worked for the US Central Intelligence Agency (“CIA”) for over thirty years. There she will have been exposed to how decisions are made often on an urgent basis.
There, I am sure she will have been exposed to the ‘confirmation bias’. This is a thinking shortcut (or cognitive heuristic), where you tend to arrive at decisions which best corroborate your assumptions, rather than seeking out alternative hypotheses.
Whilst one interpretation of people living with dementia being happier shoppers in the high street comprises the ‘dementia friendly community’, other versions of it emphasise that it is not friendliness as such which is critical. Such ‘friendliness’ can inadvertently become patronising, but true equality and upholding of human rights hold the key to the autonomy and dignity of people living well with dementia.
Without a real mission for implementing ‘thought diversity’, there is a real danger that captains of industry will in effect construct policy on dementia friendly communities, without any real genuine consultation, and ‘use’ their one or two representatives with dementia on key boards to confirm their bias.
And the situation is, unbelievably, worse than that. There is currently no person living well with dementia who is a regular invited member of the World Dementia Council. Once the (?first) UK general election is over on May 7th 2015, I am hoping the head of the Civil Service will give a direction to the Prime Minister to facilitate this urgently needed appointment.
I am of course hoping that my thoughts in this blogpost are not brushed under the carpet by people working for Simon Stevens, current CEO of NHS England, when he comes to review the progress of dementia policy in keeping with the ‘Five Year Forward View’, which he has indeed contributed to.
There are indeed specific ways cited within the report from Deloitte how ‘thought diversity’ can be harnessed. In their application for the improvement of dementia friendly communities, one obvious step is to seek out whole teams of people living well with dementia who are able to meet and come to opinions on crucial subjects.
People with dementia can lead on such teams, and the conflicts to be mitigated against here are within people living with dementia, who may have opposing views about what a dementia friendly community is, and the contrast in aims of dementia friendly communities between people living with dementia and people not living with dementia. But, if it works well, thought diversity can provide the sharing of knowledge, expertise, problem-solving approaches, which is thought to be aim of English policy in the next few years in dementia.
As Margaret Heffernan is reported to have said,
“Diversity, in this context, isn’t a form of political correctness, but an insurance policy against internally generated blindness that leaves institutions exposed and out of touch” ;
as Deloitte put it, institutions are prone to appearing out of touch, including senior policy wonks comprising some form of ‘ideological echo chamber’.
This is perhaps epitomised as, “a revolution from the heart” (Martin Luther King).
True equality for people living with dementia is identifiable.
Ultimately, the hope is that the policy of ‘dementia friendly communities’ is resilient enough to withstand shocks, such as high street stores going into insolvency. I strongly feel that thought diversity is a necessary management step in giving people living well with dementia a fair hearing so that they can lead.

How do we interpret the significance of living well with dementia?
Strange through it may seem, I have been most influenced in my philosophy of living better with dementia by the late Prof Ronald Dworkin who died in 2013 at the age of 81 (obituary here).

One recent campaign has the tagline ‘Right to know’ from the UK Alzheimer’s Society – about the right for you to know if you have dementia as a diagnosis, a right to treatment, and right to plan for the future.
I feel that people newly diagnosed with dementia have other rights too. I would say that, wouldn’t I. Above all, I feel that people who have received a diagnosis of dementia have a right to live well. This is truly a legal right, as this is not negotiable under the Universal Declaration of Human Rights. Recent case law, in the judgment from Lady Hale in R v Cheshire West and Chester Council (et al), re-emphasises that human rights are inalienable. And given that dementia is a disability under law, the right of that person with dementia is a right to dignity, reinforced by our universal human rights.
Focusing on a right to treatment further consolidates the biomedical model which I think is utterly unjustified. We have just seen the peak of one of the most successful campaigns ever mounted by Pharma and large charities for dementia to raise funds for pharmaceutical approaches to dementia. But at the expense of offering jam tomorrow there was very little on offer for people currently living well with dementia. The answer given to Helga Rohra by the World Dementia Envoy gave little in the way of concrete help for people currently trying to live well with dementia. And the ignorance of this is not benign – for the millions of dollars or pounds sterling spent on molecular biology and orphan drugs for dementia to meet the deadline of 2020, this amount of money is being taken out of the pot for developing the evidence base for and for strategies for living better with dementia in a non-pharmacological way.
Just a minute. Look at the evidence. The medications known as cholinesterase inhibitors are generally thought not to slow down the progression of Alzheimer’s disease in humans, even if they have a short valuable time window of use for symptomatic treatment In the UK, and across the world, there has been a drive for reducing the number of inappropriate prescriptions of antipsychotics for people living with dementia; there is now a growing consensus that where symptoms exist they often are due to a fundamental failure in communication with that person living with dementia, and often other therapeutic routes are much more suitable (such as psychological therapies).
The great FR Leavis, intensely under promoted at Cambridge, reminded us that criticism had to be free and flexible: and hence the famous description of the ideal critical debate as an ongoing process with no final answer: “This is so, isn’t it?” “Yes, but …”
Criticism of the English dementia policy may seem like criticism of senior clinicians, senior personnel in charities or senior politicians, but Leavis gives us a powerful reminder to stand up for what it is right. Surely, people living well with dementia have a right to comprehensive high quality dementia care and support? The evidence in support of multidisciplinary teams, including social work practitioners, speech therapists, doctors, cognitive neuropsychologists, occupational therapists, speech and language therapists, working to produce pro-active plans is now overwhelming. There is now increasing evidence that specialist nursing could prevent many acute admissions to secondary care.
As the late Ronald Dworkin asked us to consider, we might think about what makes an “interpretation” true. As Dworkin notes, psychoanalysts interpret dreams, and lawyers interpret contracts. I would go as far as to say clinicians, of various backgrounds, interpret whether a person presenting with a particular cluster of mainly psychological symptoms is presenting with a dementia. I don’t think the diagnosis of dementia is necessarily easy to make. Given that you’re giving a diagnosis of dementia not just to a person with possible dementia but also to his friends and family it is essential to get right; not to misdiagnose depression as dementia for example. My gut instinct is that doctors of all variety do their utmost to get this diagnosis correct. I think there is also a degree of interpretation in how much a person will successfully adapt to their diagnosis in taking an attitude of ‘living well’, or how they will put their faith in pharmacological treatments. The drugs do work for some people for part of the time after diagnosis, so their importance must not be diminished either. I think there is also a degree of interpretation of how disruptive a diagnosis of dementia might be for that person and his or her community.
Dworkin also notes you would be prone to sack a Judge who said, “I am not sure if this person is guilty or not guilty. I think he’s guilty, but you could probably find great many judges who finds the person not guilty.” It is possible that in the more complicated cases a Doctor might find a person living with dementia, another one not living with dementia. Dementia is presented as a definite diagnosis, a binary decision; but this would be to ignore that even the diagnostic criteria, such as the critical importance of memory (or not), has changed with time. Likewise, there has been a growing conflation of whether you fail a series of tests is the same thing as having a diagnostic label; see for example how some people recorded as having ‘delirium’ in the medical notes have in fact, strictly speaking, failed a specific set of screening tools.
But we can say that there are non-medical routes which are not an idle exercise but are of a person flowing from the diagnosis of probable dementia. This is there is much which can do to enhance the living environment of a person, whether a hospital ward, home or town. Or somebody can be directed towards advocates who can help persons with dementia communicate decisions. Or a person can be directed to inexpensive assistive technologies or lifestyle adjustments that can allow a person to live with dementia just like any other disability. This is framing long term care as living with a condition, rather than the single hit treatment.
Dignity, independence and a vast array of other values will, I feel, are a very necessary outcome of this more helpful approach to dementia. The person who has received a diagnosis of dementia is as much of a need of an acknowledgement of uncertainty as a water-tight explanation. The person who has received a diagnosis of dementia needs to be partnership with the people who wish to share that diagnosis with him or her.
I feel it is now time to unmask the medical professional who may simply be not be able to cope with this cultural shift. The medical profession does not know all the answers, nor indeed do all the people who’ve signed up to the Pharma script.
People who want to live better with dementia can be secure in the knowledge that that is their human right. They have a right to this solution, wherever it comes from.
Reference
Is there truth in interpretation? Prof Ronald Dworkin

Can you have ‘half believe’ in dementia friendliness?

There have been numerous examples of refusal of handshakes over the years. In 2012, Luis Suarez refused a Patrice Evra handshake. On the other hand, a handshake can be extremely symbolic. In 2013, it was reported that there had been a brief, but important handshake, between Obama and Castro.
Indeed, using the “Handshake” app, sales reps can take orders on the company’s tablet application while in a store or at trade shows, with the latest data on inventory and previous sales histories at their fingertips. It is now reported that app developer Handshake has raised $8 million in new funding to grow its business selling a mobile wholesale sales ordering and fulfillment application.
There has been much media coverage about a leaked memorandum from the UK Labour Party about ‘changing the subject’ when immigration comes up on the doorstep in campaigning. But, it turns out on closer inspection, such a tactic is advised if a potential voter shows unwillingness to discuss the topic of immigration in a constructive way.
The handshake is the symbol of bilateral goodwill. In other words, for a handshake to work, it cannot be refused by one party. The concept of ‘dementia friendly communities’ critically depends on rational members of the public wanting to show goodwill to people living with dementia. There may be all sorts of reasons why a member of the public might be unwilling to have that conversation. Possibly, a person might demonstrate prejudice towards, and discrimination, against a person living with dementia out of sheer ignorance; or because of powerful preconceptions from media imagery.
It is inevitable that combating such imagery is only possible if the media play out their side of their bargain. In other words, they avoid words such as ‘battle’, ‘fight’, ‘war’, or ‘robbed of his mind’. But this is not always the case. It is possible that if you know absolutely nothing about what dementia is you might have formed very crystallised opinions. Such views are ‘bigoted’ in the sense that it will be difficult for any amount of campaigning to change one’s perception of dementia.
It is now possible that creativity could be one of the best tools in shifting cultural prejudices. The latest ‘illridewithyou’ trend is a testament to that. Many Australians are still showing their support for Muslims using the hashtag #illridewithyou.
The trend started even as the siege in Sydney was ongoing on Monday. But, perhaps inevitably, a backlash has hit Twitter: #iwontridewithyou has been tweeted more than 3,000 times. On a train, one passenger reportedly spotted a Muslim woman removing her hijab, ostensibly out of fear of being targeted. The passenger told her to put it back on and offered to walk with her in solidarity. And so began #IllRideWithYou. The hashtag went viral and is currently still trending worldwide, days after the end of the hostage crisis.
It is very hard to think you can half believe in ‘dementia friendliness’, however defined, in that you can’t be ‘half pregnant’. One would think you might either sign up to the notion of wanting to learn more about the dementias, inclusivity, or accessibility, in other words making a community welcoming to a person living with dementia – or not. But the unpalatable truth is, possibly, that we all have different degrees to which we should want to prioritise this. I have often heard at meetings ‘what makes people living with dementia so special?, albeit asked politely; a person who asks this might be a commissioner in mental health services who is genuinely asking what makes a person living with dementia a higher commissioning priority than, say, a person with first episode psychosis?
These are difficult questions. The current ‘Dementia Friends’ initiative, implemented by the Alzheimer’s Society, with Public Health England in support, officially runs next year too in 2015. But at the end of this time, whatever the exact number of new ‘Dementia Friends’, serious questions will need to be asked about the wellbeing for a person newly diagnosed with dementia is any better. The annual funding of social care is reported to have dropped in recent years, from official figures, with social care not having been ring fenced since 2010.
There has never been a campaign for dementia friendliness to match the vigour of ‘illridewithyou’. Admittedly, there are key differences between stigma and prejudice against a person living with dementia, and, say, that towards a Muslim lady wearing a burkha. But this relates to another aspect of the ‘dementia friendly communities’ policy strand I have been concerned about for a very long time. Proponents of ‘dementia friendly communities’ have often argued that you might be able to spot someone with dementia in a shopping queue by virtue of the fact he or she is having trouble with monetary change. But this is a difficult path to tread down.
Somebody having difficulty with change could be exhibiting such behaviour as he or she is thinking about his partner having just died. The screening test is not particularly sensitive or selective. More basically, many dementias are ‘invisible’ to the outward observer. It might not be obvious to a stranger that someone is living with a dementia, or he or she never talks about the night terrors, the changes in semantic language, or the change in complex visual perception.
More fundamentally, we might get to the end of 2015, and we find that nothing has particularly changed in public attitudes. People living well with dementia might not find that members of society want to ‘ride with them’, but I feel the ‘Dementia Friends’ initiative has been influential in changing around a culture of indifference. Lazy commissioners will have to find another initiative to hand their anti-stigma credentials upon. My gut instinct that we will get to know whether as a society we know whether it’s possible to ‘half believe’ in dementia friendliness by the actual behaviour of us as a society. This will be very difficult to ascertain, but we will need to look into this. One thing’s for sure, it won’t be easily determined by the abundance of stickers in shop windows promoting ‘awareness’.

Why I do “Dementia Friends”
Let me introduce to you to “Dementia Friends” (details here).
The aim is for you to learn some fundamental information about what dementia is, so you understand it better than you would’ve done otherwise.
Dementia is caused by diseases of the brain; it can affect any thinking depending on what part of the brain is affected.
It’s not a normal part of ageing; it’s important to live well with dementia.
There’s much more to a person that the dementia.
I’d like to say something which may surprise you, depending on how well you know me.
I don’t really like the term ‘dementia friendly communities’. I totally ‘get’ it is well meant, embracing the concept that people living with dementia can go out in their communities at large, talk to people, go shopping, and lead a happy life.
But there are problems with the concept. I think it ignores the fact there are so many different causes of dementia, each with different ways in which they affect a person’s life. These dementias can progress at different speeds too.
I’m also worried about inadvertently creating division. There are enough divisions in society, e.g. rich vs poor, disabled vs non disabled, sick v well, for example.
I worry about the issue that to be dementia friendly you can immediately recognise disability. I’ve always had to bite my touch when people claim you can easily spot dementia in the community, so much so young schoolchildren can spot dementia even when experienced GPs cannot.
Dementia, like all other disabilities, can be invisible.
The term ‘dementia friendly community’ poses the same issues in principle as ‘gay friendly community’, therefore, one could argue.
Nonetheless, I feel the starting point policy-wise is that there is a huge amount of public ignorance about the dementias. The media have been notorious at misrepresenting dementia; even the term ‘epidemic’ is problematic, whatever the exact truth about numbers and definition, given that there are some people who believe that the dementias are essentially contagious.
I regularly ask London cab drivers if they’ve heard of dementia. Invariably, after saying ‘yes’, those cab drivers then can’t tell me much about dementia. These are generally well informed individuals, however. They readily admit they wish they knew more.
For me, it’s easy to underestimate what people know about dementia. I did a medical junior job at the National Hospital for Neurology and Neurosurgery in it. I also did my Ph.D. in it.
But I am in no way an expert.
One of my best friends, Chris Roberts, living with a mixed dementia of Alzheimer’s disease and vascular dementia, is a Dementia Friends Champion. He says, if he is an expert, he is an expert in his own dementia at this particular time.

Chris is on the left of the picture above; Jayne on the right. The “thing” in the middle, by the way, is a “selfie stick”, currently all the rage in England.
Thanks to the audio visual unit at BPP Law School for their helping me for my Dementia Friends sessions.
Here’s a short excerpt of the Dementia Friends information session we gave on 4 December 2014, together with Jayne Goodrick.
Our details are here.

It shouldn’t be the case that people who’ve been given a diagnosis of dementia feel somewhat frightened to tell their friends or family. We know loneliness is a big problem for many who’ve received a diagnosis of dementia in England.
I love doing ‘Dementia Friends’.
We never ‘force’ our Dementia Friends infocards and badges onto people!

I came to the programme with the same cynicism as many, wondering what was ‘in it’ for the charity involved in implementing it. I am genuinely worried about lack of diversity in the dementia charity sector, and potential abuse by one or two key providers of ‘dementia services’.
I also came to the programme with concerns about whether the messages or activities of Dementia Friends would be accurate.
I am generally very happy with the messages which Dementia Friends gives out, and the feedback has been overall very positive. No initiative is perfect by any means, and I think ‘Dementia Friends’ is as good a national programme, for what it does, as it could be. It was a major proposal from the 2009 English dementia strategy, entitled ‘Living well with dementia’.
The anonymous feedback we received from our December session was very positive.
The questions I regularly receive at my sessions are much harder than the ones I receive at international conferences on dementia. Such questions have included, “How can we promote the dignity of a person living with dementia?”
I think though, overall, the “Dementia Friends” initiative has succeeded.
Detailed analysis will see whether it has indeed been successful in turning ‘understanding’ into ‘action’. But I think there are currently about 600000 Dementia Friends at the time of writing is a major triumph.
Please book yourself into a Dementia Friends information session to decide for yourself. My next session is at BPP Law School in Holborn, London, on January 15th 2015. Details are here.

The importance of the ‘lived experience’ at the Alzheimer’s Disease International conference in 2015
This year, the Alzheimer’s Disease International under Marc Wortmann has done outstanding work.
It is known for its huge impact in allowing nation states to flourish with dementia strategies
Its output is phenomenal (see for example this latest paper). I have no doubt whatsoever ADI will continue to flourish under Glenn Rees, the incoming Chair (currently Chair Elect).
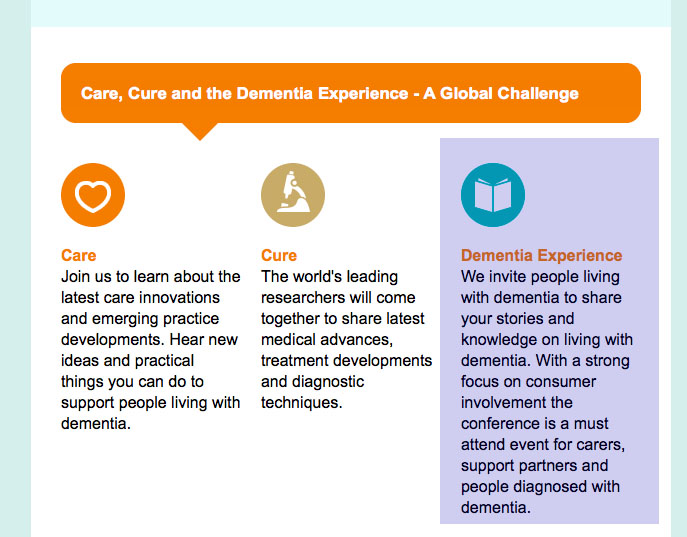
I’m still very excited about the 30th International Conference of Alzheimer’s Disease International “Care, Cure and the Dementia Experience – A Global Challenge” 15-18 April, Perth, Australia, next year.
People who are very close to me will be there.
It is, also, a lovely city.

The conference website is here.
It was always emphasised that this conference would showcase the lived experiences of people with dementia. People living with dementia and caregivers were indeed encouraged to attend.
This is a part of the list of posters to be presented on Thursday 16 April 2014.
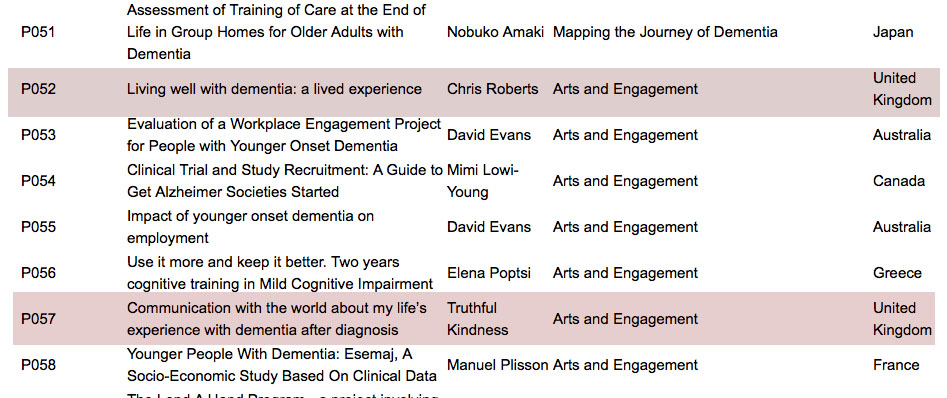
The two submitted by Chris Roberts and Truthful Kindness are shaded in a dark red.
The titles most clearly say ‘lived experience’ in the titles.
They were submitted as oral presentations, as the two people involved did not want them as poster presentations.
Indeed they did not opt for the ‘poster/oral’ option specifically for that reason.
P057
Communication with the world about my life’s experience with dementia after diagnosis
Truthful Kindness
Arts and Engagement
United Kingdom
P052
Living well with dementia: a lived experience
Chris Roberts
Arts and Engagement
United Kingdom
Truthful Kindness’ affiliation is Dementia Alliance International, Iowa; it was never submitted as United Kingdom. The irony about Truthful’s intended oral presentation is that she wished to explain how people with dementia can use all sorts of media to express themselves artistically and creatively. Arts and creativity is a huge policy plank in living well with dementia internationally.
It would have been clear to any diligent reviewer of these abstracts, from their submitted biographies, that both Chris and Truthful were genuinely living well with dementia.
Here’s Chris even holding the flyer of the Dementia Alliance International group, at Glasgow earlier this year in the Alzheimer’s Europe conference on dignity and autonomy in dementia.
Chris is currently a Board member of the Dementia Alliance International.
I understand, from having spoken to one of the juniors at the Alzheimer’s Disease International, that there may even be a chance for poster presenters to give short oral presentations of their work. But I think this possibly may be worse.
It has been explained to me that the environment for the poster sessions is very off putting. It is a crowded room, with not much space for the poster itself. It is a very noisy environment, which is very distracting. In other words, this can be an environment which is potentially disadvantageous to people with early dementia who wish to present.
I am, of course, pleased that the keynote speakers for this conference include two friends of mine, and whom I admire massively, and who are living well with dementia, Kate Swaffer and Helga Rohra.
As is known, I consider Kate to be exceptional in every way.
These are two symposia from the scientific programme in which they might have appeared: “younger onset dementia” and “engaging people living with dementia”. From eyeballing the titles of these talks, I don’t see many speakers talking about their own personal lived experiences.
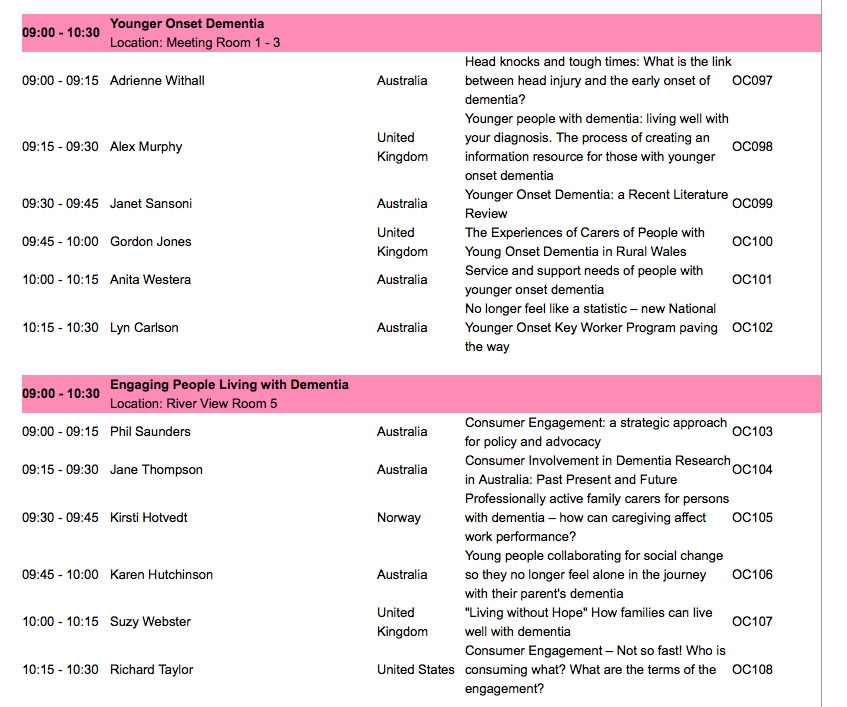
The only parts of the conference yet to be revealed are the ‘workshops’.
The details of the workshops are given as follows:
Day 2 Dementia Friendly Communities
Day 2 “How to” topic to be confirmed
Day 3 Clinical trials
Day 3 “How to” topic to be confirmed
Day 3 Arts and dementia
Day 4 World Alzheimer’s month
Day 4 “How to” topic to be confirmed
I am extremely honoured to be on the international advisory board for the 2015 conference. I should therefore not want to criticise the organising committees in any way for their hard work.
But I cannot be a silent bystander to this either. The whole point about viewing dementia as a cognitive or behavioural disability secondary to a brain disease is that it then comes under international and domestic laws (for example, for UN Convention for people with disabilities and the Equality Act).
Ignoring two people’s wishes to have an oral presentation, as they cannot do poster presentations, is not making reasonable adjustments for their disability, one could easily argue.
I understand that the number of people with dementia fluctuates year on year, so it can be difficult to predict the number of people with dementia who wish to present. But, even with the limited number of places for the two symposia I have cited above, there doesn’t appear to me a big representation of people living well with dementia amongst the speakers, but I could be wrong. This also seems to be the case for other symposia, notably the one on “dementia friendly communities”?
I think the Alzheimer’s Disease International conference 2015 will turn out to be a brilliant opportunity for us to meet up; and we will also get a chance to discuss ‘cure’, ‘care’ and ‘living well’.
But Richard Taylor, living himself with a dementia, is right in his presentation from last year – where is the representation of evidence of psychosocial techniques?
I’d like to ask where is the evidence looking at ‘living well’, such as GPS trackers, design of wards, design of houses, the wider built environment, incontinence, eating well, assistive technology, ambient assisted living, advocacy, and so on?
On that note, I do strongly applaud the work of ‘Dementia Alliance International‘, which is truly representing the community of people living with dementia.
We hear words such as ‘challenge’ being used all the time in relation to dementia.
Hopefully the organisers will rise to the ‘challenge’ of living up to the reasonable expectations of those people with lived experiences wanting to take part fully in the ADI conference 2015 in a format they feel most comfortable with (and which makes reasonable adjustments if required).

A wellbeing economics prism to ‘dementia friendly communities’

There has been some startling consensus over the national political settlement, including as it applies to English dementia policy.
There has generally been cross-party agreement about personal budgets, even though the ‘direction of travel’ from the UK Labour Party is to favour a ‘rights based approach’ to advance choice and control rather than merely though a financial budget.
There are good reasons not to put many eggs into the personal budget basket for dementia; these include how the range of ‘products and services’ for dementia can be in places rather underdeveloped, and the formidable potential safeguarding issues for certain vulnerable individuals living with dementia.
Another consensus is to be found in wellbeing, or living well.
I was struck by a recent recommendation from the first ever report by the All Party Parliamentary Group on Wellbeing Economics, entitled “Wellbeing in four policy areas” (published September 2014):
“Health and Wellbeing Boards should bring together public health professionals, Clinical Commissioning Groups, GPs, and other stakeholders to develop strategies for ‘whole person care’ which effectively integrate mental and physical health.”
Unknown to me, they had been doing great work even prior to the last UK election. Their ultimate aim, unsurprisingly, is to make wellbeing into a pervasive policy strand that straddles across all areas of life.
This ‘wellbeing prism‘ has impacted on various areas of policy, I suspect, in the past, like ‘The Big Society’. I have always felt that the ‘dementia friendly communities’ policy in England, heralded in the Prime Minister Dementia Challenge, although clearly having some roots in the Japanese ‘caravans’ ‘befriending’, fits well into the ‘Big Society’ ethos.
One of the problems with both ‘dementia friendly communities’ and the ‘Big Society’ has been whether the civic sense of solidarity might diminish statutory obligations.
I have witnessed the problems with this, first hand, in writing my book ‘Living better with dementia: champions for enhanced communities’ which I hope to publish next year. The same tensions exist in statutory obligations in the form of equality and human rights law, and statutory entities, and non-statutory community-driven ones there too.
As the O’Donnell Report puts it, wellbeing:
‘leads us to place greater weight on the human factors that explain the big differences in wellbeing, but that tend to be pushed to the margins in traditional policy making’.
There has been some focus on how we need an ‘alternative measure to GDP’. Cynics unsurprisingly argued that such a measure might inevitably gather political momentum given the problems we have had with economic growth in the last few years.
But the general arguments from the APPG on wellbeing economics make an enormous amount of sense to me. Julian Huppert is the current MP for Cambridge, and I dedicated my current book to his mother Prof Felicia Huppert, Professor of Wellbeing at Cambridge. Julian is, to my knowledge, on the APPG on wellbeing economics.
The next parliament, I hope, will see a continuation of a focus on wellbeing in policy. As pointed out in their first report, there is considerable overlap with the wellbeing field and that of the ‘social determinants of health’.
In my next book, I continue with analysing this overlap, using housing as an example. Housing is clearly an area which impacts upon the quality of life of people living well with dementia, not just from architectural perspectives of design, but also how spaces are organised to facilitate personal interaction.
Similarly, planning in the built environment is important, with considerations of inclusivity and accessibility.
These are all ‘desirable’ (or even ‘essential’?) attributes of the ‘dementia friendly communities’.
Unpaid caregivers and paid carers, like professionals, are vital in the social capital of these communities too.
It is said elsewhere that while there has been a strong focus on GDP-style economics the lack of focus on wellbeing means that we do not touch upon many policy areas, such as strife caused by marital breakdown.
I feel that this touches upon another tension of dementia policy, this time at a global level.
We know, for example, loneliness is an important source of emotional morbidity for people who have received a probable diagnosis of dementia all around the world.
Also, jurisdictions have been encouraging the aspiration of people living with dementia to live independently; in other words, not institutionalised in some form, as long as possible. This, I think, is intuitively right, so long as it is not perceived as a ‘failure’ if somebody does need the support and care provided from an institution.
There are some people who believe that the ‘successful ageing’ and ‘ageing in place’ movements have overplayed their hand; with cynics pointing out they fit nicely into the ‘small state’ narrative, a rather individualistic narrative, which takes little account of our cohesion as a society.
But this I genuinely think would be to analyse the issue too much but with one important proviso.
That proviso is that I don’t think you can value people simply in terms of their economic productivity.
I refer to this ‘equality of wellbeing’ even in my Introduction to my new book. Such equality of wellbeing throws a different light on equality driven by a purely economic sense.
In summary, in reference to the first ever report from the APPG in wellbeing economics, as the next Government and the Civil Service turn their minds into thinking about wellbeing and health policy, it will be forefront in their minds that we are about to embark on a huge behavioural change bringing together the NHS and social care.
This transformative change to ‘whole person care’ will bring great opportunities, I feel, as well as formidable challenges, not least funding considerations at a local and national level.
But I feel like the current Government, and like future ones hopefully, that a focus on wellbeing is desirable. O’Donnell is reported to have said, “If you can measure it, cherish it!”
Ideally, it would be nice to have some form of metric to see whether wellbeing interventions have any effect. I am mindful of the excellent work by Prof Sube Banerjee and colleagues on DemQoL, but others exist. And of course we should not want to end up where we started: in a target driven culture which hits targets but misses the point (as famously phrased by Sir David Nicholson).
There might be desirable effects of such metrics, though. They could be formally put into grants for research for living well with dementia; to see whether some activities are more beneficial in care homes, where there is a high proportion of people living with dementia often, than others.
The Baroness Sally Greengross asked me to put in a chapter on arts, music and creativity in my current book; so I did.
But, as the new APPG report on dementia this year rightly discusses, such a metric could be used to incentivise the use of the arts and creativity to improve the quality of life of individuals in society. And I have no doubt whatsoever that arts and creativity are a linchpin of dementia friendly communities too.
The APPG in dementia earlier this year, under Sally’s leadership, urged the importance of high quality commissioning in post-diagnostic support for dementia.
If we have more a ‘joined up’ approach to commissioning and policy, in parallel with the breaking down of silos needed for ‘whole person care’, I think England can consolidate its formidable lead in the ‘dementia friendly communities’ policy in the world.
Other jurisdictions might even follow suit.
Recommended reading:
Gus O’Donnell (Chair) – and Angus Deaton, Martine Durand, David Halpern and Lord Richard Layard(2014). Wellbeing and Policy. London: Legatum Institute. Accessible at: http://www.li.com/docs/default-source/commission-on-wellbeing-and-policy/commission-on-wellbeing-and-policy-report—march-2014-pdf.pdf?sfvrsn=2
Wellbeing in four policy areas: Report by the All-Party Parliamentary Group on Wellbeing Economics (September 2014). Accessible at: http://b.3cdn.net/nefoundation/ccdf9782b6d8700f7c_lcm6i2ed7.pdf
All-Party Parliamentary Group on Dementia assesses progress of the National Dementia Strategy for England
2014 report: The National Dementia Strategy: Change, progress and priorities
Accessible at: http://www.alzheimers.org.uk/site/scripts/download_info.php?downloadID=1447
