Home » 2014
Yearly Archives: 2014

Change

Somebody once advised me in my 20s that destiny is when luck meets preparation.
When I was younger, I used to think that you could prepare yourself out of any situation. But wisdom and events proved me wrong. I soon discovered that what you did yesterday though can affect today, and what can affect today can affect tomorrow. The only thing you can predict pretty comfortably, apart from death and taxes, is change. When I was younger, I used to think I could live forever. All this changed when I woke up newly physically disabled, after a six week coma on a life support machine on the Royal Free Hampstead. The National Health Service saved my life. Indeed, the on call Doctor who led the crash team the day of my admission, when I had a cardiac arrest and epileptic seizure was in fact a senior house officer with me at a different NHS trust in London.
This feeling of solidarity has never left me. I do also happen to believe that anything can happen to anybody at any time. I studied change academically in my MBA in the usual context of change management and change leadership. It’s how I came to know of Helen Bevan’s work. I’ve thought a lot about that and the highly influential Sirkin paper. But I don’t think I honestly ‘got‘ change until this year. In 2007, I was forced to change, giving up alcohol for life. I realised that if I were to have another drink ever I would never press the off switch; I would either end up in a police cell or A&E, and die. This is no time for hyperbole. It was this forced change, knowing that I had an intolerance of alcohol as serious as a serious anaphylactic shock on eating peanuts, that heralded my life in recovery. I later came to describe this to both the legal regulator and the medical regulator as the powerful driver of my abstinence and recovery, rather than a ‘fear based recovery‘ from either professional regulator.
But I feel in retrospect my interpretation of this change, as due totally to an externality, is incorrect. As I used to attend my weekly ‘after care’ sessions with other people newly in abstinence from alcohol or other toxins, or from gambling, or sex, I discovered that the only person who can overcome the addiction is THAT person; and yet it is impossible to read about this path of recovery from a book, i.e. you can’t do it on your own. So ‘command and control’ is not the answer after all. Becoming physically disabled, and a forced change of career and professional discipline, and a personal life which had become obsessed by alcohol, meant I had no other choice. I had to ‘unclutch’ myself gear-wise from the gear that I was in, and move into a different gear. But I did find my new life, living with mum, and just getting on with my academic and practitioner legal and business management training intensely rewarding.
In 2014, I attended a day in a hotel close to where I live, in Swiss Cottage. One of the speakers was Prof Terence Stephenson. After his speech, I went up to thank him. I found his talk very moving. He was later to become the Chair of the General Medical Council (GMC). I was later to become regulated once again by the GMC. Two lines of his has kept going through my mind repeatedly since then. The subject of the day was how sick doctors might get salvation despite the necessary professional regulation process. Stephenson claimed: “If you’re not happy about things, I strongly urge you to be part of the change. You being part of the change will be much more effective than hectoring on the sidelines.” This was not meant as any threat. And as I came to think more and more about this I came to think of how much distress my behaviour had caused from my illness, how I wish I had got help sooner, and how looking for someone to something to blame was no longer a useful use of my energies. I am now physically disabled. I get on with pursuing a passion of mine, which is promoting living better with dementia. But if there are any people who are worthy of retribution I later decided then their karma might see them implode with time. Not my problem anyway.
I now try to encourage others where possible if they feel that they have hit rock bottom; I strongly believe that it’s never too late for an addict to break out of the nasty cycle. If you think life is bad, it unbelievably could be much worse. I think businesses like persons get comfortable with their own existence and their own culture, but need to adapt if their environment needs it. I think no-one would wish to encourage actively social care on its knees such that NHS patients cannot be discharged to care, if necessary, in a timely fashion. I don’t think anyone designing the health and care systems would like them to be so far apart deliberately, with such bad communication between patients, persons and professionals. Above all, I feel any change has to be authentic, and driven by people who really desperately want that change. I think change is like producing a work of cuisine; you can follow the recipe religiously in the right order, but you can recognise whether the end result has had any passion put behind it. For me, I don’t need to ‘work hard’ at my recovery, any more. I haven’t hit the ‘pink cloud‘ of nirvana, but I am not complacent either. Change was about getting from A to B such that I didn’t miss A, I was in a better place, and I didn’t notice the journey. If I had super-analysed the change which was required to see my recovery hit the seven year mark this year, I doubt I would have achieved it.

How do we interpret the significance of living well with dementia?
Strange through it may seem, I have been most influenced in my philosophy of living better with dementia by the late Prof Ronald Dworkin who died in 2013 at the age of 81 (obituary here).

One recent campaign has the tagline ‘Right to know’ from the UK Alzheimer’s Society – about the right for you to know if you have dementia as a diagnosis, a right to treatment, and right to plan for the future.
I feel that people newly diagnosed with dementia have other rights too. I would say that, wouldn’t I. Above all, I feel that people who have received a diagnosis of dementia have a right to live well. This is truly a legal right, as this is not negotiable under the Universal Declaration of Human Rights. Recent case law, in the judgment from Lady Hale in R v Cheshire West and Chester Council (et al), re-emphasises that human rights are inalienable. And given that dementia is a disability under law, the right of that person with dementia is a right to dignity, reinforced by our universal human rights.
Focusing on a right to treatment further consolidates the biomedical model which I think is utterly unjustified. We have just seen the peak of one of the most successful campaigns ever mounted by Pharma and large charities for dementia to raise funds for pharmaceutical approaches to dementia. But at the expense of offering jam tomorrow there was very little on offer for people currently living well with dementia. The answer given to Helga Rohra by the World Dementia Envoy gave little in the way of concrete help for people currently trying to live well with dementia. And the ignorance of this is not benign – for the millions of dollars or pounds sterling spent on molecular biology and orphan drugs for dementia to meet the deadline of 2020, this amount of money is being taken out of the pot for developing the evidence base for and for strategies for living better with dementia in a non-pharmacological way.
Just a minute. Look at the evidence. The medications known as cholinesterase inhibitors are generally thought not to slow down the progression of Alzheimer’s disease in humans, even if they have a short valuable time window of use for symptomatic treatment In the UK, and across the world, there has been a drive for reducing the number of inappropriate prescriptions of antipsychotics for people living with dementia; there is now a growing consensus that where symptoms exist they often are due to a fundamental failure in communication with that person living with dementia, and often other therapeutic routes are much more suitable (such as psychological therapies).
The great FR Leavis, intensely under promoted at Cambridge, reminded us that criticism had to be free and flexible: and hence the famous description of the ideal critical debate as an ongoing process with no final answer: “This is so, isn’t it?” “Yes, but …”
Criticism of the English dementia policy may seem like criticism of senior clinicians, senior personnel in charities or senior politicians, but Leavis gives us a powerful reminder to stand up for what it is right. Surely, people living well with dementia have a right to comprehensive high quality dementia care and support? The evidence in support of multidisciplinary teams, including social work practitioners, speech therapists, doctors, cognitive neuropsychologists, occupational therapists, speech and language therapists, working to produce pro-active plans is now overwhelming. There is now increasing evidence that specialist nursing could prevent many acute admissions to secondary care.
As the late Ronald Dworkin asked us to consider, we might think about what makes an “interpretation” true. As Dworkin notes, psychoanalysts interpret dreams, and lawyers interpret contracts. I would go as far as to say clinicians, of various backgrounds, interpret whether a person presenting with a particular cluster of mainly psychological symptoms is presenting with a dementia. I don’t think the diagnosis of dementia is necessarily easy to make. Given that you’re giving a diagnosis of dementia not just to a person with possible dementia but also to his friends and family it is essential to get right; not to misdiagnose depression as dementia for example. My gut instinct is that doctors of all variety do their utmost to get this diagnosis correct. I think there is also a degree of interpretation in how much a person will successfully adapt to their diagnosis in taking an attitude of ‘living well’, or how they will put their faith in pharmacological treatments. The drugs do work for some people for part of the time after diagnosis, so their importance must not be diminished either. I think there is also a degree of interpretation of how disruptive a diagnosis of dementia might be for that person and his or her community.
Dworkin also notes you would be prone to sack a Judge who said, “I am not sure if this person is guilty or not guilty. I think he’s guilty, but you could probably find great many judges who finds the person not guilty.” It is possible that in the more complicated cases a Doctor might find a person living with dementia, another one not living with dementia. Dementia is presented as a definite diagnosis, a binary decision; but this would be to ignore that even the diagnostic criteria, such as the critical importance of memory (or not), has changed with time. Likewise, there has been a growing conflation of whether you fail a series of tests is the same thing as having a diagnostic label; see for example how some people recorded as having ‘delirium’ in the medical notes have in fact, strictly speaking, failed a specific set of screening tools.
But we can say that there are non-medical routes which are not an idle exercise but are of a person flowing from the diagnosis of probable dementia. This is there is much which can do to enhance the living environment of a person, whether a hospital ward, home or town. Or somebody can be directed towards advocates who can help persons with dementia communicate decisions. Or a person can be directed to inexpensive assistive technologies or lifestyle adjustments that can allow a person to live with dementia just like any other disability. This is framing long term care as living with a condition, rather than the single hit treatment.
Dignity, independence and a vast array of other values will, I feel, are a very necessary outcome of this more helpful approach to dementia. The person who has received a diagnosis of dementia is as much of a need of an acknowledgement of uncertainty as a water-tight explanation. The person who has received a diagnosis of dementia needs to be partnership with the people who wish to share that diagnosis with him or her.
I feel it is now time to unmask the medical professional who may simply be not be able to cope with this cultural shift. The medical profession does not know all the answers, nor indeed do all the people who’ve signed up to the Pharma script.
People who want to live better with dementia can be secure in the knowledge that that is their human right. They have a right to this solution, wherever it comes from.
Reference
Is there truth in interpretation? Prof Ronald Dworkin
Assessment in Business Law and Practice for the Legal Practice Course
This blogpost is to provide with some clues about what you might expect for the BLP assessment for the Legal Practice Course. They are unofficial observations on the main three hour paper for BLP (the second paper is a multiple choice paper which is much shorter).
The aim of the main three hour paper is to offer you a series of fact patterns; and the aim is for you to make diligent assessments of the documents provided, for example, budget sheets or articles of association, to provide accurate advice for your client. A typical paper might consist of about seven questions, varying in length and contribution to the overall quantum of the paper. But there are certain favourite topics, which you would do well to be aware of. Please note that this blogpost should not be used as indication of what will be in your examination. The coverage of the entire syllabus has been pretty complete. For example, one of the questions not listed below is on business accounts, but you could find yourself discussing the impact of various commercial decisions on parts of the budget sheet. Any of the calculations you covered in the business accounts SGS could appear too. Please note that there can be variants of questions; for example the procedure plan might be focused on redemption or buy back of shares following some need to remove a director, for example, or the lead examiner might be much more interested in questions on setting up the original private limited company (exploring topics such as choice of business medium, or relative advantages or disadvantages of debt and equity finance). The main intention of the BLP exam is to ensure competence for aspiring solicitors to be regulated by the Solicitors Regulation Authority, though the assessment will also provide ample scope for working out who the distinction level candidates might be. It might be that the lead examiner might feel that certain topics, such as private acquisitions or employment, are best reserved examining in detail in some later point for elective options.
I am not a BLP tutor, so please don’t take any of the below as other than well meant hints and tips. Thanks.
1. Corporate insolvency
The question on corporate insolvency could carry as much as about 15 marks.
In this question, for example, you might be informed that a company is in financial difficulties with a particular ‘fact pattern’. You might be told of a specific scenario, such as the company had recently disposed of an unused storage unit to an unconnected third party at a discount to its current market value.
You might be asked to advise what the implications were for the company (or its creditors) and for the directors of the company, for example. You might be expected to apply the “every step” defence preventing disqualification of a director, for example:
- undertaking regular financial checks;
- calling regular board meetings and raising concerns there;
- taking independent advice from an insolvency practitioner;
- speaking to the shareholders; and
- suggesting savings to be made in the running of the business.
You will need to apply carefully the statutory law, and include if relevant possible defence steps.
More than offence could of course satisfy the fact pattern. You should however be very careful about considering other issues which on the facts are not relevant to the question being asked. This is not only a waste of time, but also does not produce any marks.
The candidates who do well on this type of question will methodically apply the relevant statutory provisions concerning such transactions to the factual scenario, giving precise and accurate statutory references. They analysed the proposed transaction, with frequent reference to the statute, and outlined the potential consequences for the client if the creditor went into liquidation or administration (namely that the court could order the transaction granting the preference to be set aside), in the same manner as they had considered such issues in the SGS.
2. Removal of a director
This might be quite a quick scenario for about 10 marks.
You might directed to consider some Proposed Articles, and, for each of three proposed articles, explain (i) whether that article was legally permissible, and (ii) whether it was commercially and practically suitable for a proposed limited company.
You might be given a fairly typical scenario of documents that had been served on the board of a company seeking the removal of a particular as a director and advise the board on the steps it should now take and the likely sequence and timing of events.
The question normally students to advise on the procedure to remove a director under s.168 and ss. 303-305 CA 2006. You might also be presented with the perspective of how a director could protect himself or herself from such an action.
Most students answer this type of question very well, but weaker students tend to give vague, generic answers on the commercial points rather than applying the given facts to the details of the question.
3. Procedure plan
Such a question might expect candidates to prepare a procedure plan to implement the appointment of director A, the resignation of director B, the entry into the service contract of director A and the issue and allotment of shares to director A.
This is quite often the most significant question in the main BLP paper, attracting about twenty marks out of 80, i.e. one quarter of the total marks available for the overall BLP examination. The question also asked students to consider all post-meeting matters, to specify the order in which the steps must be taken and who needs to take each step. Students are told normally not to consider the written resolution procedure.
The majority of students will manage to achieve the marks available for basic points by setting out and explaining the board meeting, general meeting, board meeting sequence and standard resolutions required (e.g. board resolution to approve notice of and board resolution to call the general meeting). The question also asks students to consider who would take each step and to list the requisite filings and other post-meeting matters. Students are normally told not to consider the written resolution procedure.
However, there are often several distinct areas where weaker answers do not provide any or sufficient analysis, particularly if the procedure plan involves issuing shares; for example the detail of the procedure for issuing shares can be lacking in answers. Students need to focus on the five-step process for issuing shares in order to establish which resolutions, if any, would be required to score highly. Some students will lose marks by not giving full statutory references, e.g. MA 17(1)(b) to appoint a director, and MA 9(1) in relation to calling a board meeting. Some answers did not show sufficient attention to detail, for example by failing to state what would happen, in the correct order. Some students said that the existing directors would resign before the replacement directors had been appointed.
There are various ways in which distinction answers might excel themselves. For example, distinction answers might describe how the issue of ordinary shares would affect the voting rights of the existing shareholders and would enable individuals to block special resolutions whereas the preference shares did not carry any voting rights.
4. Drafting
This could be asked about in a number of ways.
Students might be asked to identify any typographical, grammatical or formatting errors or inconsistencies and any incorrect or inconsistent use of defined terms. This part of the question tested students’ attention to detail and their knowledge of the conventions of good drafting.
Most students made a fair attempt at this part of the question. Students who scored poorly on this part of the question did not take sufficient care in spotting some obvious errors (which included spelling errors, naccurate cross–referencing and use of singular vs. plural terms, inconsistent use of the definitions, inconsistent punctuation within the sub-clauses of clauses, inconsistent numbering of clauses and errors in the cross references to clauses).
Students who earn good marks on this part of the question were those who paid close attention to detail and were therefore able to spot a wide range of errors. Weaker students will not pay sufficient attention to detail and fail to spot basic grammatical errors and other inconsistencies such as incorrect use of definitions, inaccurate cross–referencing and use of singular vs. plural terms.
A few students will fail to read the question properly and either re-drafted the clause or commented on the substantive drafting rather than identifying typographical, grammatical or formatting errors.
A student might also, for example, be provided with a “blue pencil” clause, to examine whether a student can assess a clause is likely to be too onerous or unlawful.
5. Substantial property transaction
This question might carry 10-15 marks, and might typically be in two parts.
A first part of the question might ask students to identify any statutory provisions that should be considered by a company, in connection with a proposed substantial property transaction, and state how the statutory provisions should be complied with
The facts might, for example, point to a substantial property transaction (applying ss. 190(1)(b) and 191(2)(b)) between a company and a person connected to one of its directors, the director’s father (ss. 242(2)(a) and 253(2)(e). High-performing students made specific reference both to the elements of the relevant sections and the facts provided in the scenario, to back up this conclusion.
A second part of the question asked students to explain the consequences for the company and its board, if the relevant provisions were not complied with. For example, most students would correctly cite relevant subsections of ss. 195 and 196: credit was awarded both for stating that the transaction would be voidable (not ‘void’) and for identifying individuals who, in this scenario, could face personal liability.
6. Taxation
Students are given information about an individual’s financial affairs and told that the client is seeking advice about her income tax and capital gains tax liability.
In the aternative, Corporation tax can be asked in a number of ways, such as how anticipated losses could affect corporation tax liability, or how “straddling” comes about, when a company’s accounting period does not match the financial year.
You may also be asked about the specific scenario of the tax condideration of a ‘close company’ covered in SGS.
7. Conduct
Your client, for example, has requested advice as to whether or not it should invest as it had been told it was a “very good bet‟.
This has not only been covered in the BLP SGS but also in considerable detail in the ‘decision tree’ worked examples for the PCR SGS.
8. Acquisitions
You might be asked a question related to the proposed acquisition of A by B and asked, students to consider the advantages and disadvantages of structuring the transaction as a share sale, from say B’s perspective. Students will generally given credit for sensible points, including the following:
This question might alternatively ask candidates to consider whether a company could pursue a claim against the Seller in respect of problems with vehicles it had indirectly acquired following its purchase of shares. Most candidates , foe example, would therefore be expected to suggest that the company should review:
- the due diligence information it had received (for example any responses to any due diligence questions regarding the condition of the vehicles);
- the share purchase agreement (to identify any warranties or indemnities the Seller had made with respect to the vehicles and any vendor protection clauses the Seller had included to limit its liability); and
- any disclosure letter (to identify any issues disclosed with respect to the vehicles which might preclude a warranty claim).

The Liberal Democrats and UKIP should pledge to repeal the Health and Social Care Act
Ed Miliband, Andy Burnham, and the whole of Labour have pledged robustly that a direction to repeal the Health and Social Care Act (2012) will be made in the first Queen’s Speech of a new Labour Government.
It is said that David Cameron and Nigel Farage are to be issued with a joint challenge to declare that they will rule out any attempt to repeal the ban on foxhunting if they form a pact in the event of a hung parliament.
Evan Harris on 6 March 2012 identified the impact that the Lansley legislation would have to turbo-boost marketisation and privatisation of the NHS.
He warned Liberal Democrat colleagues not to touch it with a bargepole:
“It has no friends among even the non-party-political royal colleges, and has no mandate in those areas where it goes beyond the coalition agreement. The political impact will be to retoxify the Tory brand – which they are welcome to do, of course –, but also, by association, to damage the Lib Dems.”
The assurances given by Lord Clement Jones have turned out to be hollow:
“In putting down amendments, we have no hostility to competition as such, merely a desire to make use of the opportunities that the TFEU and European competition law offer member states to avoid the NHS being treated like a utility, such as gas and electricity.
Under the EU treaties, Article 106 of the Treaty on the Functioning of the European Union states:
“Undertakings entrusted with the operation of services of general economic interest … shall be subject to the rules contained in this Treaty, in particular to the rules on competition, insofar as the application of such rules does not obstruct the performance, in law or in fact, of the particular tasks assigned to them”.
Member states have certain discretion as to which services are services of general economic interest. By ensuring healthcare services for the purposes of the NHS are services of general economic interest and that the “task” of co-operation between services is “assigned” to the healthcare providers, it should be possible to provide some protection from less desirable aspects of competition law.”
This year saw Cambridgeshire and Peterborough NHS Foundation Trust awarding G4S Integrated Services a £3.9 million contract to provide domestic cleaning, portering and catering support across its property portfolio. The three year agreement, with the option to extend for a further year, will see G4S initially delivering services to 34 sites across Peterborough and Cambridgeshire, with further locations likely to be added in the future. Cleaning will be provided across the contract, with additional portering services and catering support at some specific sites.
Privatisation does not require a complicated definition. It’s simply the transfer of public sector resources into the private sector. Even the late Sir Keith Joseph, widely thought to be “brilliant” by the late Margaret Thatcher herself, and who was thought to be the principal “architect” of Thatcherism, ended up trying to keep afloat businesses in the public sector rather than privatise them. This was during his time as Secretary of State for Trade and Industry.
There is generally a feeling that the Coalition government, a joint enterprise between the Conservatives and the Liberal Democrats, went much further in privatising the NHS than the Thatcher government even dared to. And the worst aspect of this was there was absolutely no inkling that this would happen. There was no mention of this even in the Coalition Agreement of 2010.
There is no official policy by UKIP on the NHS yet.
This is absolutely staggering. The late Tony Benn used himself to warn people against voting for people who are ‘false prophets’. UKIP seem alarmingly reluctant to acknowledge the number of people from black asian minority ethic background who actually work for the NHS and bring value to it everyday.
It is now felt that there is quite a high chance of a ‘hung parliament’, although Labour activists are desperate to fight for a Labour government at Westminster with a healthy majority. It appears that the mainstream right-wing press have given up the ghost, in the form of David Cameron.
It is curious why the Conservative Party haven’t ditched their leader, like they did famously in 2010, but the most parsimonious explanation is that it would make sense to find a new leader after the expected catastrophe of the 2015 election. Ditching Cameron now might mean that they would have to ditch a new leader further in 2015. Besides, the Conservatives and Liberal Democrats have become a tried and tested product as far as the City are concerned.
The current Government, and people who sail with her such as BoJo, have fiercely defending the City’s interests in Europe as far as banker bonuses are concerned. They have resisted the ‘Mansion Tax’, which is widely thought to be introduced by Ed Balls as Chancellor in the first Budget of a Labour Government, as a windfall tax to produce a cash injection into the NHS. Furthermore, the City still has lucrative contracts in the form of the private finance initiative which have yet to be renegotiated properly from this Government; and also they have been very successful in promoting social impact bonds, the PFI equivalent for social enterprises, with the current Government which has used mutualisation to Trojan horse rent seeking in response to Mid Staffs.
Certain dividing lines have now got to be laid for the sake of the public good.
I feel that it is essential that David Cameron, Nick Clegg, and Nigel Farage are to be issued with a joint challenge to declare that they will rule out any attempt to resist the repeal of the Health and Social Care Act (2012).
Nigel Farage, for all his faux socialist credentials, seems unseen to resist formally the privatisation of the NHS; in fact his henchmen over the years have prided themselves on the ‘efficiency’ of the private sector, despite the growing allegations of fraud and inefficiency from the outsourcing companies used by the current government to deliver the smaller State.
Nick Clegg not only has a PR problem; he has a major issue with the content of what the Liberal Democrats stand for. It is widely known that there is discontent about his party’s ‘differentiation’ policy, which has seen the Tories and the Liberal Democrats telling the voters why each other party is clearly unfit for government. The charge sheet against the Liberal Democrats, including a weak economy (not enough till receipts from income tax to fund public services), demolition of legal aid, privatisation of NHS, misery for a mass of disabled citizens through botched welfare reforms, is substantial.
As a minority party, the Liberal Democrats would be asked to repeal the Health and Social Care Act (2012) which is possible but simply weird. It is clear that the Liberal Democrats, Conservatives and UKIP are clearly capable of running the NHS into the ground.
A lot of energy was put into fighting the Liberal Democrats on the toxic firestorm hospital closure clause, clause 119, which the Liberal Democrats were instrumental in protecting. Norman Lamb, for all his soothing words, has been the Minister of State in office while social care has imploded; the social care budget has not been ring fenced, coincidentally, since 2010.
There was a popular joke on Twitter this year that turkeys joked, “It’s like humans voting for UKIP”.
David Cameron, if he is still leader in 2015, or whoever is in charge of that toxic brand, will clearly be in no position to repeal the Health and Social Care Act (2012). The least worst option is that the Liberal Democrats and UKIP should pledge not to resist the repeal of the Health and Social Care Act (“Act”), but the hope is that a strong Labour government will have renewed vigour in assessing the political weather. Even better, they should pledge to repeal the Act.
That is, the component of the private sector in the mixed health and care economy has gone way too far. The health and care sectors should never be run anywhere for the benefit for shareholders offering care in 15 minute slots or below the minimum wage. The health and care sectors should not be so fragmented as they are now. People should be collaborating with each other to offer excellent clinical care, not competing with each other.
The vote is the most critical weapon of influence any of us has. Even more than ever, it is vital that it is used wisely.

Can you have ‘half believe’ in dementia friendliness?

There have been numerous examples of refusal of handshakes over the years. In 2012, Luis Suarez refused a Patrice Evra handshake. On the other hand, a handshake can be extremely symbolic. In 2013, it was reported that there had been a brief, but important handshake, between Obama and Castro.
Indeed, using the “Handshake” app, sales reps can take orders on the company’s tablet application while in a store or at trade shows, with the latest data on inventory and previous sales histories at their fingertips. It is now reported that app developer Handshake has raised $8 million in new funding to grow its business selling a mobile wholesale sales ordering and fulfillment application.
There has been much media coverage about a leaked memorandum from the UK Labour Party about ‘changing the subject’ when immigration comes up on the doorstep in campaigning. But, it turns out on closer inspection, such a tactic is advised if a potential voter shows unwillingness to discuss the topic of immigration in a constructive way.
The handshake is the symbol of bilateral goodwill. In other words, for a handshake to work, it cannot be refused by one party. The concept of ‘dementia friendly communities’ critically depends on rational members of the public wanting to show goodwill to people living with dementia. There may be all sorts of reasons why a member of the public might be unwilling to have that conversation. Possibly, a person might demonstrate prejudice towards, and discrimination, against a person living with dementia out of sheer ignorance; or because of powerful preconceptions from media imagery.
It is inevitable that combating such imagery is only possible if the media play out their side of their bargain. In other words, they avoid words such as ‘battle’, ‘fight’, ‘war’, or ‘robbed of his mind’. But this is not always the case. It is possible that if you know absolutely nothing about what dementia is you might have formed very crystallised opinions. Such views are ‘bigoted’ in the sense that it will be difficult for any amount of campaigning to change one’s perception of dementia.
It is now possible that creativity could be one of the best tools in shifting cultural prejudices. The latest ‘illridewithyou’ trend is a testament to that. Many Australians are still showing their support for Muslims using the hashtag #illridewithyou.
The trend started even as the siege in Sydney was ongoing on Monday. But, perhaps inevitably, a backlash has hit Twitter: #iwontridewithyou has been tweeted more than 3,000 times. On a train, one passenger reportedly spotted a Muslim woman removing her hijab, ostensibly out of fear of being targeted. The passenger told her to put it back on and offered to walk with her in solidarity. And so began #IllRideWithYou. The hashtag went viral and is currently still trending worldwide, days after the end of the hostage crisis.
It is very hard to think you can half believe in ‘dementia friendliness’, however defined, in that you can’t be ‘half pregnant’. One would think you might either sign up to the notion of wanting to learn more about the dementias, inclusivity, or accessibility, in other words making a community welcoming to a person living with dementia – or not. But the unpalatable truth is, possibly, that we all have different degrees to which we should want to prioritise this. I have often heard at meetings ‘what makes people living with dementia so special?, albeit asked politely; a person who asks this might be a commissioner in mental health services who is genuinely asking what makes a person living with dementia a higher commissioning priority than, say, a person with first episode psychosis?
These are difficult questions. The current ‘Dementia Friends’ initiative, implemented by the Alzheimer’s Society, with Public Health England in support, officially runs next year too in 2015. But at the end of this time, whatever the exact number of new ‘Dementia Friends’, serious questions will need to be asked about the wellbeing for a person newly diagnosed with dementia is any better. The annual funding of social care is reported to have dropped in recent years, from official figures, with social care not having been ring fenced since 2010.
There has never been a campaign for dementia friendliness to match the vigour of ‘illridewithyou’. Admittedly, there are key differences between stigma and prejudice against a person living with dementia, and, say, that towards a Muslim lady wearing a burkha. But this relates to another aspect of the ‘dementia friendly communities’ policy strand I have been concerned about for a very long time. Proponents of ‘dementia friendly communities’ have often argued that you might be able to spot someone with dementia in a shopping queue by virtue of the fact he or she is having trouble with monetary change. But this is a difficult path to tread down.
Somebody having difficulty with change could be exhibiting such behaviour as he or she is thinking about his partner having just died. The screening test is not particularly sensitive or selective. More basically, many dementias are ‘invisible’ to the outward observer. It might not be obvious to a stranger that someone is living with a dementia, or he or she never talks about the night terrors, the changes in semantic language, or the change in complex visual perception.
More fundamentally, we might get to the end of 2015, and we find that nothing has particularly changed in public attitudes. People living well with dementia might not find that members of society want to ‘ride with them’, but I feel the ‘Dementia Friends’ initiative has been influential in changing around a culture of indifference. Lazy commissioners will have to find another initiative to hand their anti-stigma credentials upon. My gut instinct that we will get to know whether as a society we know whether it’s possible to ‘half believe’ in dementia friendliness by the actual behaviour of us as a society. This will be very difficult to ascertain, but we will need to look into this. One thing’s for sure, it won’t be easily determined by the abundance of stickers in shop windows promoting ‘awareness’.

Ever tried. Ever failed. No matter. Try again. Fail again. Fail better.

Now here’s a question: how are we to ascertain the ‘success’ of the World Dementia Council?
The work of the World Dementia Council is wide-ranging; it’s not just the aggressive pimping of innovations for dementia.
The four main areas of work are to be as follows.
Four main areas are being pursued in order to tackle the lack of effective treatment and sufficient funding to find a cure:
- Integrated development – Optimising the path of medicines from research through to market by reducing barriers & encouraging regulatory flexibility.
- Finance and incentives – Looking at ways to increase the relatively low investment in funding dementia innovation by exploring new types of funding product.
- Open science – Unleashing the potential of open science for sharing information and knowledge to accelerate progress in developing new treatments and care approaches, and avoiding wasteful duplication of effort.
- Public health/prevention – The Council is also beginning an evidence review into existing research on how risk factors such as diabetes and heart disease relate to dementia, as well as looking into public health messaging on lifestyle and prevention.
There are some occasions when it is blatantly unwise to reward failure. For example, one could argue that senior management of the NHS should not automatically command high salaries, if they are not doing the basic things well, such as listening to their junior staff in their decision making.
But the operational failures of the NHS have been eye watering. Data showed just under 90% of patients were seen within four hours in the seven days up to December 14 2014. Pressures in England’s A&E units have hit record levels, with the lowest percentage of patients seen within four hours since monitoring began in 2010. Major units particularly struggled, with just six out of 140 meeting the target to see 95% within four hours.
Earlier this year, it was reported that NHS organisations have run up a total deficit of nearly £500m in the first three months of this financial year, according to two reports from health sector watchdogs Monitor and the Trust Development Authority. Monitor reported that the NHS had come under “unprecedented pressure” from increased patient demand, at a time when they are still trying to make savings in response to the biggest squeeze on Government health spending in the health service’s history. The Foundation Trust sector, made up of 147 NHS organisations, including 83 acute hospitals, which have historically been more financially stable than the rest of the NHS, has gone into overall deficit for the first time.
One of the phenomena which the NHS seems to be learning from big business is the immorality of high executive pay. The High Pay Centre, a think tank, said shareholders were still backing high executive pay deals despite new powers to vote them down at annual meetings. The pay of the average FTSE 100 chief executive increased from £4.1m to £4.7m last year, said the report. The High Pay Centre’s report says that, without further action, trust in business will be damaged by the perception that an executive “elite” is reaping all the rewards from economic growth.
The famous Samuel Beckett adage is, “Ever tried. Ever failed. No matter. Try again. Fail again. Fail better.” But if the current Government were to fail better over the NHS, they would be presiding over an unfathomable epidemic of A&E trolley queues. The adage also draws into sharp focus what ‘failure’ is for the NHS. Failure for an individual Doctor or nurse might be easier to define, in terms of patient safety. One could argue that the metric of overall whether the NHS and care are safe is too blunt, but a necessary component.
Success in health and care, one can broadly define, should not be measured clinically through the lens of shareholder dividend. And yet this is precisely what we appear to do for private providers of care homes. It has long been felt that the 1945 Attlee ‘post war settlement’ failed both the left and right. It failed the left as it led to growing marketisation and privatisation of public services, and it failed the right as true socialism planning and shared resources went flying out of the window.
Numerous recent governments have tried to triangulate their way out of this problem. But it is clear that this has introduced more new problems than the old problems it purported to solve. Take for example financial failure for failed market entities. In a health service that pretended to be safe, otherwise you would not de-prioritise clinical emergencies, you would be taking out of scope life or death situations. And yet successive recent governments have allowed a situation where a NHS hospital might be acting unlawfully if it received ‘state aid’.
There are also strata of how failure is ‘hidden’ in the modern health and care system. The cuts in social care have been staggering, with the current Government coming up with increasingly convoluted explanations of their vanity project ‘The Better Care Fund’ to explain away a social care system on its knees. A fundamental problem, for example, with not being entirely truthful about the quality of care, running it entirely under market forces, is that you cannot easily tell if a patient with mental health problems gets a ‘bum deal’ in clinical care? Even measuring suicides has not become an uncontroversial measure of lack of success of policy; even though reports of suicides of disabled citizens allegedly brought about in welfare reforms continue to emerge.
It is possibly true that the phrase is better suited to long term conditions in service provision.
Let’s think again about, “Ever tried. Ever failed. No matter. Try again. Fail again. Fail better.”
Innovation, doing traditional things differently to achieve the same or better outcome, should not be the territory necessarily of any political ideology. And it is certainly true that you have to crack a few eggs to make an omelette; in other words, an innovator has to be prepared to put up with a few dead ducks before hitting upon a great idea.
So how do you measure the success of an innovator? This question does merit some scrutiny, as one might then consider whether the performance of a successful innovator ought to be ‘sustainable’. Or whether we should make do with an innovator who has ‘hit it lucky’? But here I feel that there are some fundamental misunderstandings about what innovations are. Innovations aren’t simply inventions. A lot of work has to be put into discovering whether an intended target audience can actually adopt an innovation or not; hence the absurdity of not having a person living well with dementia on the World Dementia Council.
How are we to tell whether the World Dementia Council is any good? For me, one measure is whether they include people they purport to be interested in. By this, I don’t include having a person living with dementia in attendance at a meeting, but a person living with dementia with a portfolio and programme to influence their work. Inevitably one person living well with dementia to represent the millions globally in the world will appear tokenistic, but we’re shockingly not even at that stage. There is no person living well with dementia who has been appointed yet as a regular member of the World Dementia Council, and I certainly don’t want to see this to be situation when Kate Swaffer and Dennis Gillings participate in the same session of the Alzheimer’s Disease International Conference next year.
You can see whether a health system is truly embracing integrated care by certain proxy phenomena arguably, such as whether there is a whole person care tariff incentive in place, whether data are shared, whether there is care coordination, whether there is an ethos of multidisciplinary teams, whether stakeholders embrace shared or distributed leadership, and so on.
You can see the extent to which science is ‘open’ by the degree to which results are shared, including those from drug trials which have been dead ducks; the question is whether Pharma will wish to share this information with the market, as this form of market signalling could be to the detriment of shareholder dividends, even if for the market good. Market forces again. Whenever I see somebody sleeping rough under Waterloo Bridge in London, like the late and great Tony Benn, I think of market forces.
But the one domain which is the most vague is measuring the efficacy of prevention strategies. This, however, could be clearer than the ‘target’ of having a drug cure for dementia by 2025. Forget the usual question about which of the hundred dementias they’re finding and funding a cure for? Nobody’s listening. La la la la la. How will be able to tell the actual prevention strategies are working? This is not asking the same question as whether Governments have in place got operations in place to promote prevention; such as Mediterannean diets or fitness clubs.
For those of certain political spectrum, the development of an illness or disease is due to a failure in responsibility by an individual. We have seen this argument reach torrential proportions in the backlash against the effects of obesity being construed as a disability. Some people are medically morbidly obese, so should they be tarred with same brush over criticism of ‘those fatties who eat too many cream cakes’? The current evidence that the non-modifiable risk factors for Alzheimer’s disease are quite substantial, so even if we somehow eradicated all risk certain individuals would still develop that type of dementia. However, it could well be that some forms of dementia are amenable to healthy living. And if so are those people who are developing certain types of dementia, e.g. vascular dementia, guilty of not trying harder?
2014 has seen the growth of the meme ‘healthy body healthy mind’ as the beneficial effects of diet (including cholesterol), blood pressure control or physical exercise have come to the fore in considering the vascular dementias. This whole discussion, though, potentially poses questions about what sort of health system we want. Parking aside the issue of whether we want a health system which views illness as a punishment for personal indiscretions, and therefore your access to treatment fundamentally dependent on society’s view of retribution, we could consider whether we want a health system where we pool our risk, or whether you are sealed to your insurance premium fate by your particular genetic make up? We keep on being told that the future of medicine in the NHS is through advances in DNA technology. We’ll all one day be able to access details of our genome, even if our local care home for Granny is up shit creek.
So where now for, “Ever tried. Ever failed. No matter. Try again. Fail again. Fail better.”
Lessons do have to be learnt from catastrophes, whichever political term they happen to fall under, whether Harold Shipman or Mid Staffs. But there is a danger of making good policy out of extreme disasters (even if extreme disasters turn out to be ‘isolated events’). Likewise, the risks we take in developing innovations may be utterly dissonant with the need to minimise risk in the acute part of the service. But considering this question enables us to think about what sort of society we want? In the case of my interest, dementia, whether we want to have a World Dementia Council without a sitting member living well with dementia or whether we want to ‘blame’ people for developing dementia?

Reasons to be cheerful – my review of 2014
There were many reasons to be cheerful this year for me. One of them was going down at the invitation of Lisa Rodrigues (@lisasaysthis) for Prof Sube Banerjee’s inaugural lecture as Chair of Dementia at Brighton and Sussex Medical School.
Reasons to be cheerful
Sube called his lecture, a timely view on where we’ve got up to in English dementia policy, “reasons to be cheerful”.
Kate
Kate (@KateSwaffer) is a world class advocate for people living with dementia.
I have found Kate’s work on stigma and language particularly interesting. Kate is Chair Elect of Dementia Alliance International (@DementiaAllianc), and I expect this group, consisting in the vast majority of people living well with dementia, to be extremely influential in 2015. As this group becomes more influential, I am sure it will attract more scrutiny, and it will be necessary both to manage people’s expectations and not be unduly swayed by externalities.

The University of Wollongong (@UOW) is where Kate did her Masters of Science degree in dementia care. I only received a Commendation for my Master of Law, but that was in commercial and corporate law, and not really my strongest love. For Kate to receive a Distinction is no less than Kate deserves, and I was genuinely utterly thrilled for her.
Chris and Jayne
I tried to get out more this year, fuelled by seeing friends Chris Roberts (@mason4233) and Jayne Goodrick (@JayneGoodrick). Louise and Rachel from the Dementia Action Alliance Carers Call to Action (@DAACarers) have worked amazingly hard, and I have nothing but the utmost respect for this arm of English policy. Here’s a picture of me, Chris, Sally (@nursemaiden) and Ken Clasper (@ken_kenc) at the Methodist Central Hall in Westminster.

I do strongly believe that ‘experts’ are a potentially false concept in dementia. I certainly don’t believe in experts by longevity – people who’ve professionally been studying dementias for ages. I do agree with Chris though – people living with dementia do become experts in their own experiences at their particular times. We all can learn from this.

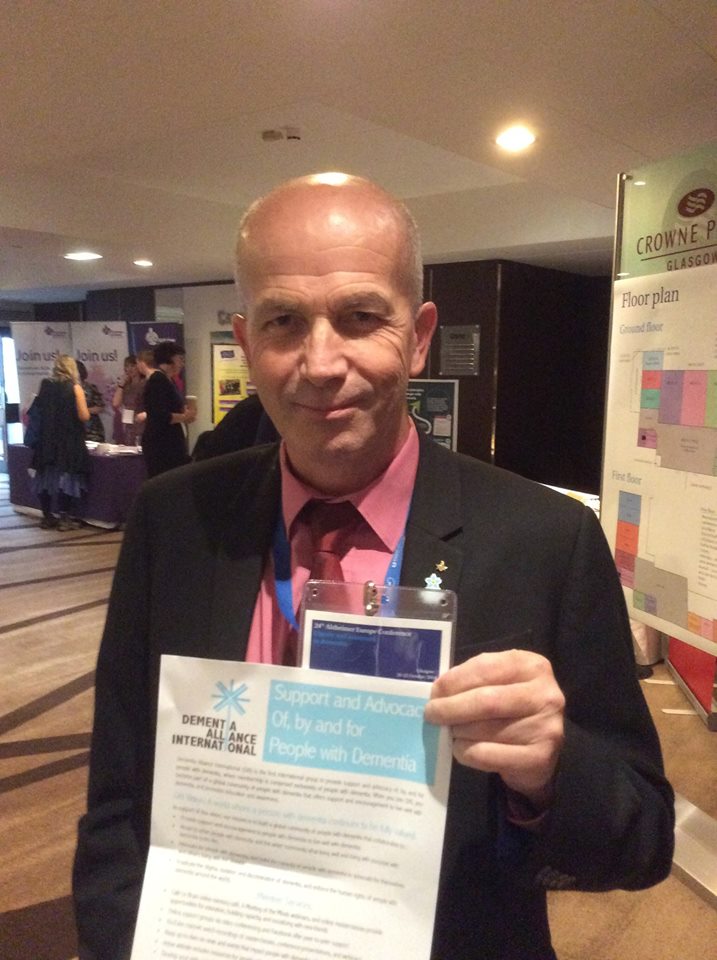
Here’s Chris holding the Dementia Alliance International flyer. This was in a crowded foyer during the conference. I am not sure what we were doing at that precise second. I reckon I might have been panicking about the poster session on my findings of the use of language in the G8 summit. That poster session was very enjoyable for me, as I got a chance to chat with Prof Mary Marshall whose influence on design and dementia has been enormous at Stirling. Mary remembered me from a workshop I attended in Notting Hill once. And I remember her. She spoke with me for ages, when she had no need to at all.
Dementia policy in England and Scotland
I thought this was a parody of a Monty Python sketch until one of my bright Twitter followers advised me it was a parody of the Two Ronnies sketch. That’ll learn me. Anyway, here I am with Chris and Tim Lloyd Yeates (@alivetim) whom I am confident to report is one of the most polite and well mannered persons I have ever met in my life.

Ultimately, I have limits to my understanding of dementia, having not lived with dementia myself to my knowledge, and definitely not been involved in a family caregiving way. I am all the time mindful there is close to a million unpaid family caregivers in the UK, who are the backbone of dementia policy. They are central to care and support. Sally Marciano is a very experienced nurse, but also knows from the closest of family connections how dementia can affect someone. Prof Alistair Burns (@ABurns1907), the national clinical lead for dementia, often remarks that when a diagnosis of dementia is disclosed, it’s not only given to the person with dementia, but to his or her friends and family. This, I feel, is absolutely true.

I first met Toby Williamson from the Mental Health Foundation (@MHF_tweets) when he chaired a groupthink session in one of the fringe meetings of the Alzheimer’s Europe conference in Glasgow. We were discussing stigma in dementia, and thinking of possible strategies for overcoming stigma. Toby is at the Mental Health Foundation, and I find him extremely interesting to talk with. He shares a number of policy interests with me, namely human rights, equality and personal budgets. I name dropped Toby in a comment on Prof Julian Hughes’ excellent presentation on ethics at the annual meeting of the Dementia Action Alliance.

Thanks to Sam (@yeweestoater) for her unending support. I really value this – and I had a great time when I met Sam for the first time at the Beardmore Hotel in Glasgow earlier this year, for the clinical research network day hosted by Scotland.

I was invited by Norman Macnamara (@norrms) to a talk on global positioning systems and people living well with dementia. As it happened, I got lost on the way back to the lift of the Queen Elizabeth II conference centre, and Norman was very helpful! The Purple Angels continue to be an enthusiastic force of people raising awareness of issues to do with dementia.

I have decided I am no longer going to take photos on my digital SLR camera, as something always go wrong on them. Here’s a photo of Suzy (@suzysopenheart) and Jayne not taken on my iPad as it should’ve been (like Tommy Dunne (@tommytommytee18), I adore my iPad).

I was really pleased that Lucy Jane Masters (@lucyjmarsters) was able to make it to my book launch of ‘Living well with dementia’ earlier this year.
It was great to see Marian there (@mariannaidoo). Also, I really appreciate Beth (@BethyB1886), Dr Peter Gordon (@peterDRLOW) and Margaret Kilby (@mkilll) making it too.
Lucy is a specialist nurse in dementia, and also studying at the Brighton and Sussex Medical School. Like me, Lucy shares a passion for the positive rôle specialist nurses can play in proactive case management in dementia, which I anticipate will be an important service provision change innovation shortly.

Travelling back to Glasgow was highly emotional for me; so was meeting people who’ve become a big part of life through Twitter. You certainly can’t fault Tommy Whitelaw (@tommyNTour) for the sheer dedication he has shown to raising awareness of lending a hand of support for caregivers. Besides, he’s a Glaswegian, and given that I was born in Glasgow in 1974, Glasgow is a special part of my own personal life.

There are people I met in 2014 – and I wish they’d come into my life earlier, really. I was always aware of the huge amount of work Agnes Houston in the Scottish Dementia Working Group was doing as well as Donna. It was only until I saw Agnes (@Agnes_Houston) and Donna whizzing around in the Alzheimer’s Europe (@AlzheimerEurope) conference in Glasgow that the penny finally dropped.

I don’t think I ever met Tommy Dunne until this year. Meeting Tommy and Joyce were definitely highlights of my year – and I think Suzy Webster is genuinely fantastic too. With them, there’s no bullshit at all. They exhibit kindness. They are not distracted by others – their focus and attention is a clear indication of their dignity and the amount of respect they command. I think some of the happiest times I had in total in 2014 were through the Dementia Action Alliance Carers Call to Action (@Dementia_Action; @DAACarers). They’re the sort of occasions where you do genuinely feel you’ve known people for ages – like weddings without any of the family traumas!

Twitter can bring with it some degree of mystique. But a general enduring trend of mine was that the people I met in real life were invariably even more impressive than how I knew them from Twitter. One clear example of this was Darren (@mrdarrengormley). I think I share attitudes and values with Darren. Darren really ‘gets it’. A real privilege to know – I’ve got a lot of time for Darren.
Charmaine
To say Charmaine (@charbhardy) is ‘strong’ would be to do Charmaine a disservice. I am completely in awe of how Charmaine doesn’t ‘complain’. Charmaine thinks she’s doing her best, but she’s doing infinitely more than that. I am extremely grateful for the time I had this year in going to Robertsbridge and seeing for my own eyes the garden that Charmaine works so hard on. And I am proud of everything Charmaine does. I am proud of her community. Her friends adore her (look at the bunch I met for example at the Ostrich and Tony especially). I loved meeting G who spontaneously showed me his PhD thesis from around the time when I was born (I was born in 1974). This photo of Charmaine and me was taken at University College London, where completely thanks to Charmaine I was able to attend a support group for carers of people with frontotemporal dementia. There, I had a long chat with Katy Judd. It was great to catch up with Katy, whom I remember working with at the National Hospital for Neurology and Neurology, at Queen Square, more than a decade ago. Prof Martin Rossor (@martinrossor), whom I think is wonderful, was the head of the clinical firm.

I’ve learnt a huge amount from the support groups this year. It also reminds me what an enormous privilege it is to know something about dementias in a professional and academic capacity, and what an honour it is to use this knowledge for the public good.
I’d love to go to the Ostrich in Robertsbridge some time in 2015 for a holiday; not least as it will give me an excuse to see Charmaine G and family.

The international forum
Before I got a chance to finish my sentence, ‘My name is…‘, Marc Wortmann (@marcwort), CEO of Alzheimer’s Disease International (@AlzDisInt), explained to me that he knew ‘exactly who (I am)’. I had a chance to thank Marc twice this year for the work of the ADI – once for the work on national strategies in dementia, and one for his report in which the ADI recommended avoidance of the word “institutionalisation”.

Helga in many ways is larger than life. Helga Rohra (@ContactHelga) just beams encouragement, drive, wisdom, leadership, principles, justice, realism, and charisma. A real joy to spend any time with. Here’s us in Glasgow.

Prof Facundo Manes (@manesf) was in the same research lab as me at Cambridge. He is one of the world experts in frontotemporal dementia now. I have extremely fond memories of his friendship at Cambridge, and he has become a lifelong friend. He is a ‘proper neurologst’, and has a huge amount of common sense as well as a real talent for research. I love his attitude to life, and the fact that he is so clearly very bright. He has taken the field of decision making in dementia into parts I could have only dreamt of, and of course I am eternally grateful for that. Facundo, as well as being a Professor at the University of Favorolo in Buenos Aires, leads at INECO – a huge tour de force in cognitive neurology and cognitive neuroscience in South America; and he is Co Chair of the research division of dementia, aphasia and other cognitive disorders for the World Federation of Neurology.
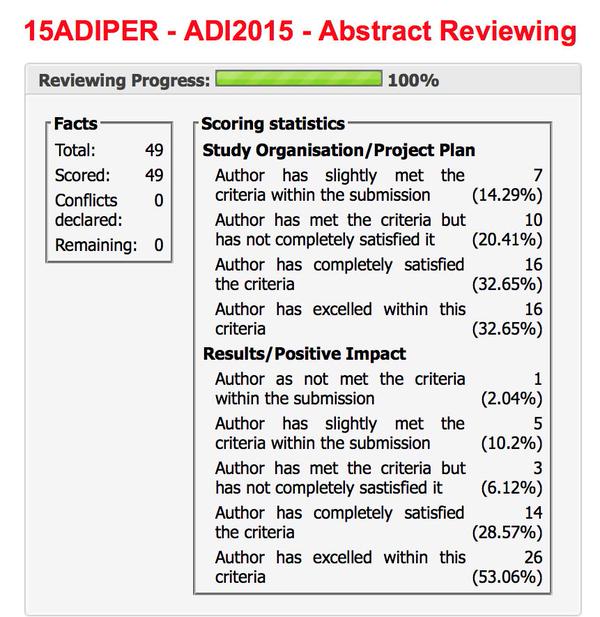
This year, I got put onto the International Advisory Board of the ADI conference to be held in Perth, Australia, this year. I really enjoyed reviewing about fifty abstracts mainly on stigma, younger onset dementia and dementia friendly communities. I look forward to these being presented, when I attend in person next year.
The law
One of the biggest honours I had this year was being asked onto the Board of Governors of the BPP Students’ Association. Prof Carl Lygo (@carllygo), Professor of Law, and CEO of BPP, has been of massive support to me personally. He’s supported me through the stormiest of weather. Also, Shahban Aziz (@ShahbanAziz), CEO of the BPP Students Association, has become a true friend of mine. I get enormously proud of them both whenever I see them in real life, or on Twitter.

In one part of my life, I thank enormously for the happy times I’ve had at BPP Law School. I not only studied for my ‘graduate diploma in law’ (and bachelor of law), but I also did my legal practice course there. This was via brief detour of doing my MBA at BPP Business School and my Master of Law at the University of Law. BPP has been a massive part of my professional and personal rehabilitation. Now, my understanding of business strategy and law make complete sense.
Here I am with Shaun (@DiasShaun) and Shahban.

I had the pleasure of talking to Gary at great length this year twice. Our conversations ranged from conflicts of interest to conspiracy theories. I think it’s fair to say I have met few people as thoughtful or as intellectually versatile as Gary Slapper (@garyslapper). We share very similar values. I am looking forward enormously to his new edition of ‘English legal system’, which reminds me of the second love of my life – the legal profession.

NHS
I have enormous respect for Prof Wendy Savage (@wdsavage). Wendy Savage and I share not only a passion for the NHS, although Wendy’s campaigning is in altogether different level to mine (being far superior). And Wendy, I suspect, shares similar feelings about the medical regulator, the General Medical Council, as me.

This year saw me trying to get out and about a bit more. I met Sharon (@SharonAvraham) outside the Harold Wilson room for a meeting which Jos Bell (@jos21) had brilliantly organised. Jos has worked so hard as Chair for the independent Socialist Health Association London division this year. Jos has also been a real rock of support this year, which has been tough for me. I am inevitably eternally grateful for this.

I saw Andy Slaughter (@hammersmithandy) speak for the first time in Portcullis House. I am of course fully aware of the West London hospital reconfiguration, and I thank Andy enormously for campaigning on this issue. I am also grateful for Andy’s lead against that nasty Legal Aid and Sentencing and Punishment of Offenders Act (2012) which saw legal aid being throttled. I am a firm believer in access to law and justice, as well as access to medicine. Of course I am mindful that Sadiq Khan, currently the Shadow Justice Secretary (@sadiqkhan), will have a difficult year ahead.

For the first and only time this year, I had an amazing smoothie and cheeseboard selection in the restaurant of the National Gallery. Like the late Baroness Thatcher, I have developed a habit of turning up to everything early. I turned up to the event in Trafalgar Square to support the NHS early. Jos knew I would. I had a great time, though.

A poor start
The very beginning of my life I don’t feel was a poor start.
I am Scottish. I went back to Glasgow twice this year in fact.
Glasgow is where I was born in June 1974.

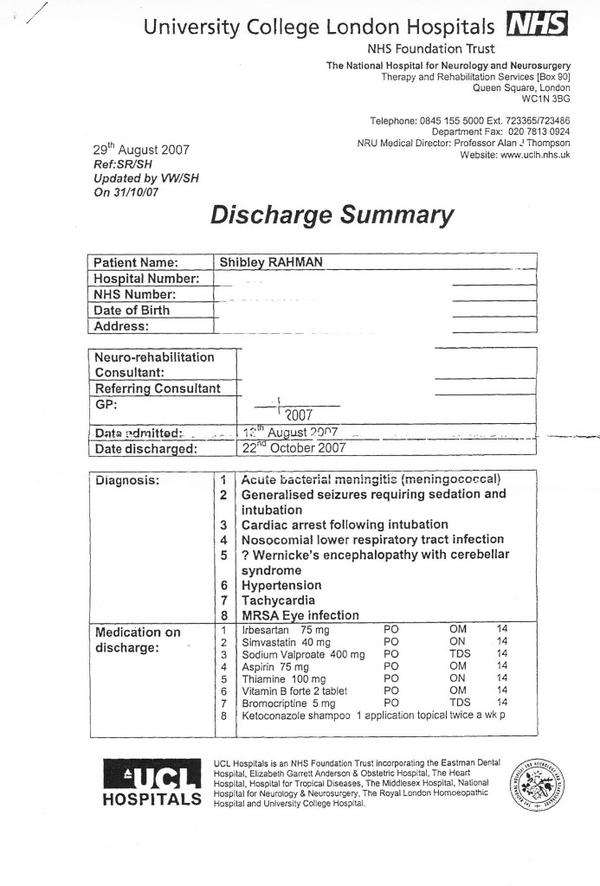
Undeniably I feel I’ve come a long way since that I day I had an epileptic seizure at the Royal Free Hospital due to bacterial meningitis in 2007. Things got worse when I had a cardiac arrest, and then had six weeks in a coma. While I am physically disabled now, I am happy of course that I have been in recovery from severe alcoholism for about seven and a half years now. I feel strongly that anything can happen to anyone at any time.
GMC
I went up to Manchester several times in 2014 to see the GMC – my meeting with them was adjourned the first time around.
I ended up, therefore, contemplating in Starbucks.
With the free Wifi, it was like being on holiday.
It was amazing to meet @kyrakee who found me there. Kylie had just hopped off a tram, perhaps having worked out the clues from my cryptic Twitter clues?

I know this Starbucks now, like the Arnedale Centre, like the back of my hand

2014 was an opportunity to apologise to the medical profession which I strongly feel that I had let down previously. My late father amongst many others would have wanted me to have made this apology to the GMC (@GMCUK).
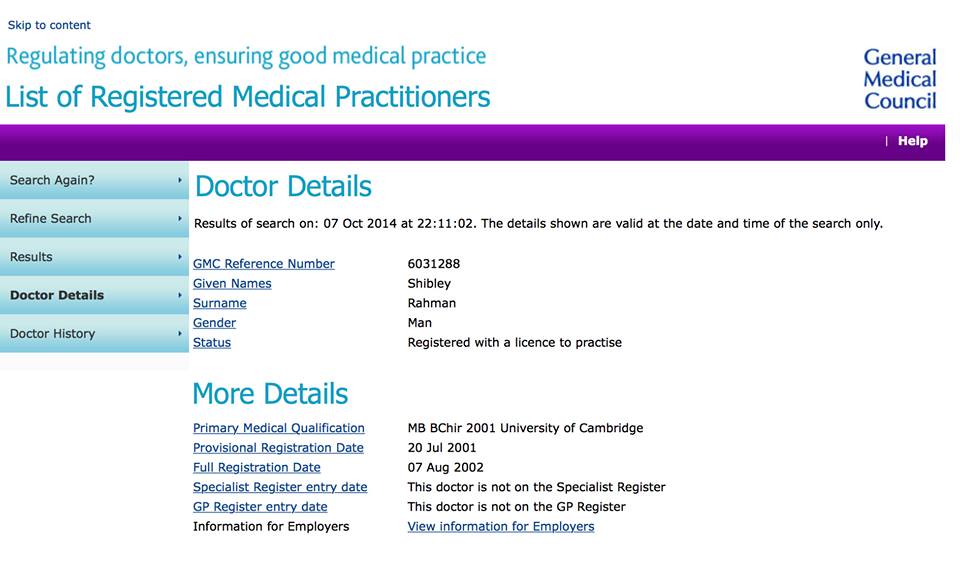
It was a massive honour to be put back onto the GMC register. I don’t think I have ever been happier. To be put on the UK register having lost the opportunity to be there is a massive deal. The GMC oppose all restoration requests not because they’re fundamentally difficult; but because the burden of proof must be on the applicant to prove that they can fulfil their duty of patient safety. There is therefore a necessarily high threshold for this, and now that I am in recovery, I don’t underestimate the enormous privilege to be regulated by both the medical and legal professions.

Martin Rathfelder (@SocialistHealth) took great care of me in my numerous visits to the GMC in Manchester this year. I have very happy memories of the numerous Chinese restaurants we frequented too. Martin was a crucial component in me trying to think positively about the whole experience. Manchester, after all, had been a very sad place for me and my father back in 2006. On a different note, I currently enjoy being on the ‘central council’ of the Socialist Health Association.

I am completely in awe of the GMC. I would say that, wouldn’t I?
Happiness at last
All these life experiences encourage me to try to take life easy when I can. Like a Koala, I can present #KoalaKlaws. I can even, if pushed, go for the #KoalaKill. I therefore have natural affinity to the Koala.

The man on the right of course needs absolutely no introduction. I think it’d be impossible for the English dementia policy to be universally liked by everyone. That I say not as means of an excuse, but because I am genuinely in admiration of how Prof Alistair Burns has served as the clinical lead for England. I met for the first time this year Alistair (here at the DAA Carers meeting at Smith Square, Westminster). I also met Sally Greengross (the Baroness Sally Greengross) for the first time this year. Sally’s the Chair of the All Party Parliamentary Group for dementia. I promised Sally in fact that I would include a chapter on arts, music and creativity in my next book. I like Sally would like to include some of the positives too in the narrative, and looking into this for Sally was a huge delight.

Next year will be a gruelling one. The last few years have not adequately safeguarded against causing misery for disabled citizens. Legal aid was murdered. Criminal barristers were in uproar. The NHS saw a piece of legislation which imposed a heavy penalty for the first time for NHS contracts not put out to competitive tender in all cases other than a sole bidder. The record waits for A&E were a disgrace for the operational management of the NHS in England. We now have a situation where it is difficult sometimes to discharge people in a timely fashion to social care. Bringing together health and care next year, if there is a majority Labour government in the UK, as “whole person care”. The repeal of the Health and Social Care Act (2012) which turbo-boosted the privatisation of the NHS, defined as the transfer of resources from the public to private sector, is now desperately needed. I wish Andy Burnham MP (@andyburnhammp) well. I sincerely hope he can start work as Secretary of State for Health and Care in 2015.
Conferences: a necessary evil?
I really didn’t know what to expect in the Alzheimer Europe conference in Glasgow. I must say that people with dementia and carers were certainly not involved in any tokenistic way. I was happy to be there. Thanks to all at Alzheimer Europe for such a brilliantly run conference; including the work done by Gladwys and Jean (@JeanGeorgeAE).

The conference brought me back to my academic roots – which is no bad thing.
As I grew in confidence this year, not just personally, but also in my opinion of the national train service providers and the London termini, I wanted to travel to conferences about dementia more. As the year progressed, my attitude changed from conferences wanting to sell you something, to conferences being happy places where you shared knowledge and experiences. Besides, they for me became happy places for me. Here’s James Murray-White (@sky_larking) and Chris at the Future Inn, Bristol, just shortly before our day hosted by Alzheimer’s BRACE (@AlzheimersBRACE).

Tommy Dunne and Chris Roberts were sat right at the front of my talk in Manchester. The turnout wasn’t massive, but it meant a lot to me that they were there. There was also somebody in the front row who was very nice to me; his mother had just been diagnosed with a dementia. To make a small difference to just one person means a lot to me. I’ve also felt this about ‘Dementia Friends’ (@DementiaFriends) – it’s not the quantity of the actions, it’s the quality.

Getting a chance to fill a void in print about living well with dementia meant a lot to me this year.
I straddle currently two professions, but I’ve been attending out of support (but not participating in, due to my disability) the legal aid walk for the last few years. Thanks so much to Bob and Natalia who invite me every year. I volunteered once pro bono in the North Kensington Law Centre, the oldest law centre in England, in welfare benefits. I had a brilliant time, and I would strongly recommend this type of work to any law student.

My books
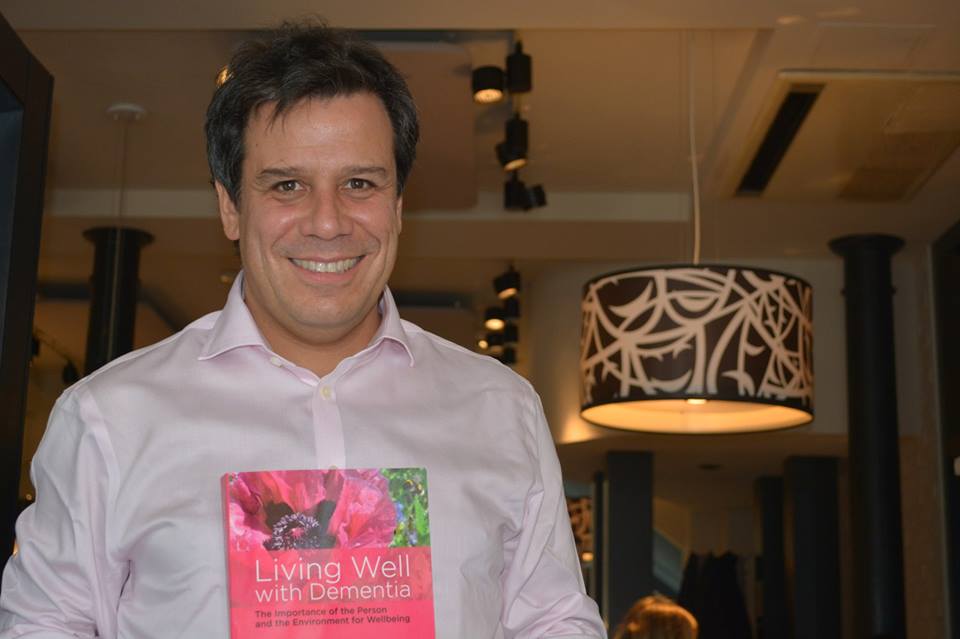
This was a bit of sneaky product placement for my book, of course.
I was totally amazed to see my book in print. I dedicated my book ‘Living well with dementia’ to my late father, but of course without both of my parents this book would’ve been impossible.
Thanks to Prof John Hodges in NeuRA, previously Chair of Behavioural Neurology at the University of Cambridge, for the support he’s given me for my first book ‘Living well with dementia’ (where he indeed kindly wrote a Foreword), and also for my second book ‘Living better with dementia’.

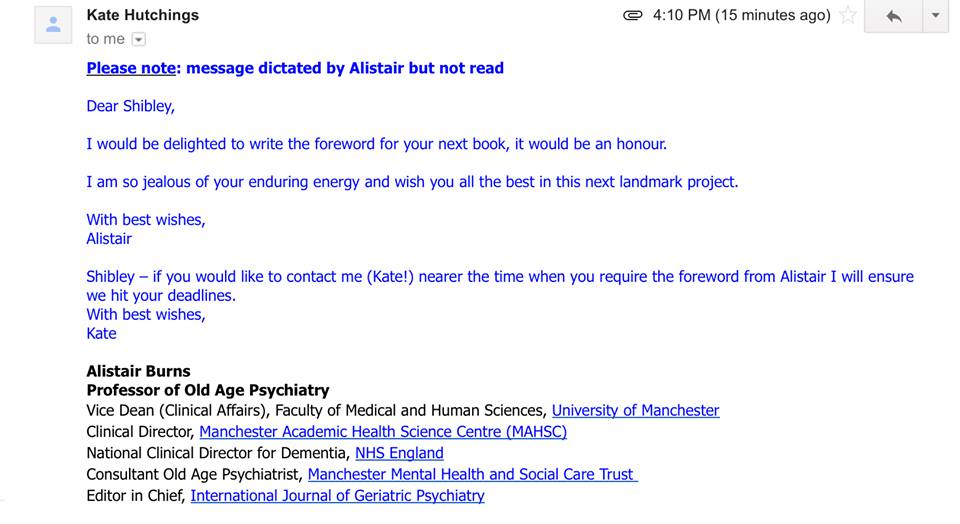
I admire Alistair’s energy, so it was extremely nice to receive this from Prof Burns earlier this year.
Serenity
Above all, I was reminded from Truthful Kindness (@truthfulkindnes) this year not to worry about things which were clearly out of my control. This mantra, the “Serenity Prayer”, is how we conclude each meeting for people who’ve had alcohol problems. There comes a time when some people, having successfully survived a period of abstinence, go into a period of recovery. That’s when you get used to life in the absence of alcohol, and it’s normal. You don’t get cravings – you don’t notice alcohol – you can go into pubs without it even being an issue. So if things don’t go my way, invariably out of my control, I don’t fret about it any more.
Thank you for making my year such a happy one.

Why I do “Dementia Friends”
Let me introduce to you to “Dementia Friends” (details here).
The aim is for you to learn some fundamental information about what dementia is, so you understand it better than you would’ve done otherwise.
Dementia is caused by diseases of the brain; it can affect any thinking depending on what part of the brain is affected.
It’s not a normal part of ageing; it’s important to live well with dementia.
There’s much more to a person that the dementia.
I’d like to say something which may surprise you, depending on how well you know me.
I don’t really like the term ‘dementia friendly communities’. I totally ‘get’ it is well meant, embracing the concept that people living with dementia can go out in their communities at large, talk to people, go shopping, and lead a happy life.
But there are problems with the concept. I think it ignores the fact there are so many different causes of dementia, each with different ways in which they affect a person’s life. These dementias can progress at different speeds too.
I’m also worried about inadvertently creating division. There are enough divisions in society, e.g. rich vs poor, disabled vs non disabled, sick v well, for example.
I worry about the issue that to be dementia friendly you can immediately recognise disability. I’ve always had to bite my touch when people claim you can easily spot dementia in the community, so much so young schoolchildren can spot dementia even when experienced GPs cannot.
Dementia, like all other disabilities, can be invisible.
The term ‘dementia friendly community’ poses the same issues in principle as ‘gay friendly community’, therefore, one could argue.
Nonetheless, I feel the starting point policy-wise is that there is a huge amount of public ignorance about the dementias. The media have been notorious at misrepresenting dementia; even the term ‘epidemic’ is problematic, whatever the exact truth about numbers and definition, given that there are some people who believe that the dementias are essentially contagious.
I regularly ask London cab drivers if they’ve heard of dementia. Invariably, after saying ‘yes’, those cab drivers then can’t tell me much about dementia. These are generally well informed individuals, however. They readily admit they wish they knew more.
For me, it’s easy to underestimate what people know about dementia. I did a medical junior job at the National Hospital for Neurology and Neurosurgery in it. I also did my Ph.D. in it.
But I am in no way an expert.
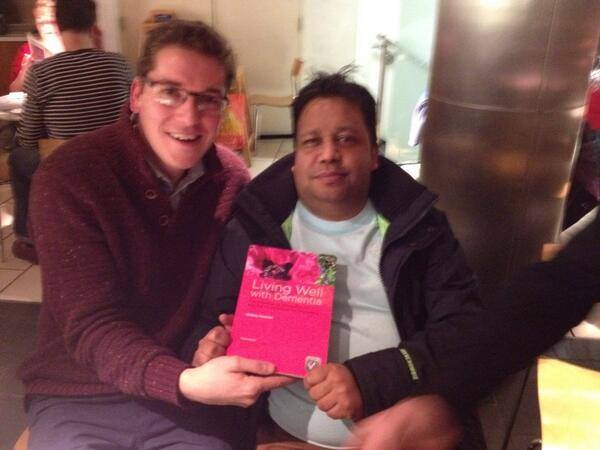
One of my best friends, Chris Roberts, living with a mixed dementia of Alzheimer’s disease and vascular dementia, is a Dementia Friends Champion. He says, if he is an expert, he is an expert in his own dementia at this particular time.

Chris is on the left of the picture above; Jayne on the right. The “thing” in the middle, by the way, is a “selfie stick”, currently all the rage in England.
Thanks to the audio visual unit at BPP Law School for their helping me for my Dementia Friends sessions.
Here’s a short excerpt of the Dementia Friends information session we gave on 4 December 2014, together with Jayne Goodrick.
Our details are here.

It shouldn’t be the case that people who’ve been given a diagnosis of dementia feel somewhat frightened to tell their friends or family. We know loneliness is a big problem for many who’ve received a diagnosis of dementia in England.
I love doing ‘Dementia Friends’.
We never ‘force’ our Dementia Friends infocards and badges onto people!

I came to the programme with the same cynicism as many, wondering what was ‘in it’ for the charity involved in implementing it. I am genuinely worried about lack of diversity in the dementia charity sector, and potential abuse by one or two key providers of ‘dementia services’.
I also came to the programme with concerns about whether the messages or activities of Dementia Friends would be accurate.
I am generally very happy with the messages which Dementia Friends gives out, and the feedback has been overall very positive. No initiative is perfect by any means, and I think ‘Dementia Friends’ is as good a national programme, for what it does, as it could be. It was a major proposal from the 2009 English dementia strategy, entitled ‘Living well with dementia’.
The anonymous feedback we received from our December session was very positive.
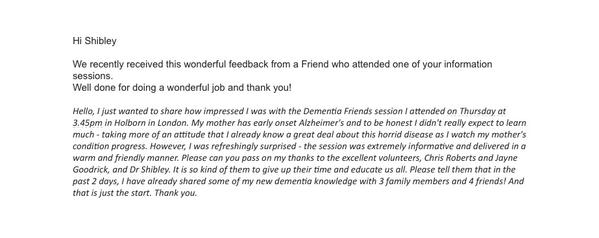
The questions I regularly receive at my sessions are much harder than the ones I receive at international conferences on dementia. Such questions have included, “How can we promote the dignity of a person living with dementia?”
I think though, overall, the “Dementia Friends” initiative has succeeded.
Detailed analysis will see whether it has indeed been successful in turning ‘understanding’ into ‘action’. But I think there are currently about 600000 Dementia Friends at the time of writing is a major triumph.
Please book yourself into a Dementia Friends information session to decide for yourself. My next session is at BPP Law School in Holborn, London, on January 15th 2015. Details are here.

Another 5 years of David Cameron? I really hope not.

What is most intriguing in the in-depth analysis of Ed Miliband as Prime Minister is that most people I know would rather emigrate from the UK rather than to face another five years of David Cameron.
David Cameron has presided over an unbelievable mess in welfare benefits. I’ve lost count of people including myself who suddenly had their welfare benefits stopped (in my case disability living allowance due to physical disability), who just ‘fell off’ the benefits register. I had to have two appeals, and then go to a tribunal, before I was restored to the benefit I had received previously. And in the meantime there had been absolutely no improvement in my disability symptoms.
David Cameron has presided over an economy which works well for the very wealthy – but this is a dangerous time to be vulnerable. It is sheer bare faced cheek to claim the economy is healthy when it can’t muster enough tax receipts to keep public services going. A record number of people in employment, with a growing population in the UK, is short shrift for a society which cannot pay benefits in a timely manner such that a record number of people has to go to food banks. This is precisely what you get when you a bargain basement low wage economy, fuelled by zero hour contracts, with slashing of employment rights.
The Conservative narrative is a highly fraudulent one. Shortly before Lehman Brothers crashed, George Osborne had been boasting about how he would match Labour on spending commitments. So far from giving keys back to the driver who crashed the car, Osborne was the co-driver. Osborne wrote in ebullient terms about the deregulated Iceland – the one which crashed big time. It’s simply a pack of lies, needed to produce a malnourished State of public services, whereas corporates still get their cushy state handouts – such as proceeds from the privatisation of Royal Mail. This time, the Liberal Democrats, under Nick Clegg and Danny Alexander, have been first in the queue chanting repetitively their pack of lies.
David Cameron’s cardinal sin was never to mention the devastating £3 billion reorganisation of the NHS. This four hundred page piece of law, only made possible with the Liberal Democrats on the accelerator pedal not the brake, did not have a single clause on patient safety (apart from abolition of the National Patient Safety Agency). It was the wrong piece of law at the wrong time. With social care on its knees, it did nothing to make the health and care systems fit for purpose. Hospitals simply cannot discharge NHS patients in a timely fashion to social care currently. Add on top of this the chaos in A&E waits, it’s now a case that individuals cannot both enter hospital and cannot leave hospital. The NHS simply could not cope with another five months of this utter mess, let alone another five years under David Cameron.
Cameron and Hunt have presided over a disastrous NHS. How dare they.
But the legislation was not a waste of time for the people who have been behind this Government every step of the way. Lurking in the shadows of ‘The Big Society’ are the big private equity backers. They’re the ones who have controlling stakes in private finance initiative hospitals which they can slept a profit. Eye watering contracts of NHS services are being flogged off to the private sector. Even the late Harold Macmillan, a previous Tory prime minister, resented the selling off of the ‘nation’s silver’ under the prime successor, Margaret Thatcher. Privatisation is simply transfer of resources from the public sector to the private sector. You’d have to be an idiot not to understand that.
Somebody who is far from an idiot, Oliver Letwin, has explained the critical rôle of outsourcing of services (source here).
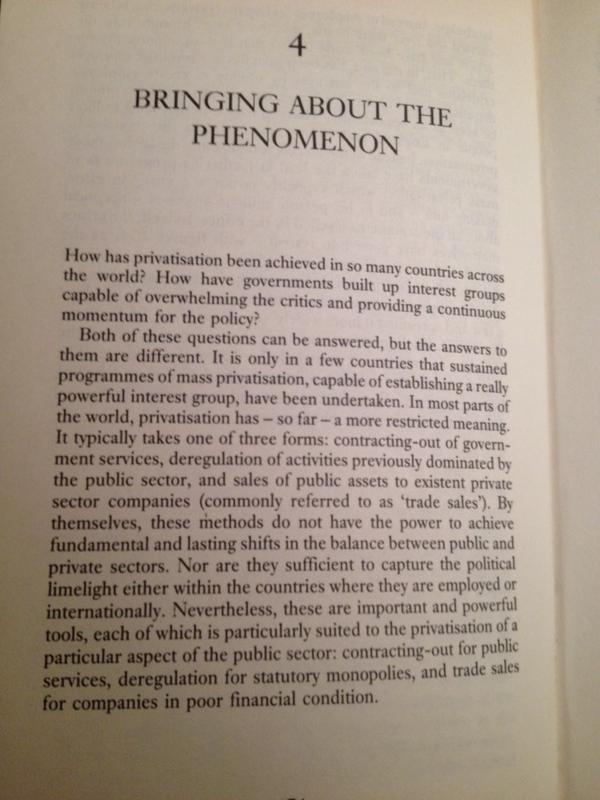
Just in case there is a hung parliament it’s become vital to think who could prop up another failed Tory administration. Vote for Alex Salmond or Nick Clegg at your peril.

Is it too little too late?

We found out this morning from Dave West from an article in the HSJ that HM Treasury has agreed an unannounced £740m increase to the health revenue budget for the current financial year.
Since mainstream parties agreed to sign up to ‘efficiency savings’, a euphemism for making cuts in budgets, NHS Trusts all over the land have been trying to reconcile PFI debt with running a bargain basement staff. The current Government and key political stakeholders have resisted at all costs a national minimum staffing level, arguing primarily that this is not the overall number of nursing staff which matters but their suitability of skill sets in nursing environments.
These efficiency savings, nonetheless, have been made by NHS hospitals. Some hospitals have been more successful than others. The idiotic nature of the NHS drifting towards a market, being ensnared by the EU competition laws, that such financial assistance of hospitals come dangerously close to “state aid” which is deemed unlawful.
In England, “state aid” already exists in the form of foodbanks which have exploded in number under this Government. The consensus is that they have primarily supplied a need demanded from deserving members of the public, many of whom have been waiting for unreasonable time for benefits. This is a direct effect of the crass incompetence of operations in handling of benefits under this Government. This incompetence has seen emotional distress from people who are disabled. Some, it is alleged, have even taken their own lives.
The problem with running the country’s “safety net” in such a ‘lean matter’, means that there is no reserve in the system. If a nurse or Doctor goes off sick, the entire rota is thrown into chaos. The NHS ends up chasing its own tail, for example by employing expensive locum staff when it has not had the competence to employ the correct number of staff in the first place.
The mainstream political parties are still, overall, committed to the ‘private finance initiative’, although there have been some noises about how little value for money it represents. Despite the successful campaigning by some on the NHS, the political motivation for providing a solution to this problem appears lacking. There is an issue not only about the exorbitant demands of loan repayments, akin to a corporate ‘Wonga’ strangehold on the State’s finances, but also how private equity firms seemed to have got an amazingly good deal out of it effecting having a level of control and ownership on NHS hospitals which the general public, if they know, would balk it.
The next Labour Government is expected to introduce ‘whole person care’. Everyone agrees that social care is on its knees, but invariably most people agree that this situation has not come about suddenly in the last few years. There has been an insidious promotion of marketisation in the social care sector, which Labour had much to do with. Anyway, living in the now, the social care sector is in utter chaos. NHS hospitals are not able to discharge, often, their patients into social care in a timely fashion. Health and care sectors are intimately dependent on one other.
There is a growing feeling now that the drift in health and care policy across several governments, with a feeling of ungenerous funding, PFI, personal budgets, etc., albeit catapulted with the chaos over competitive tendering over the Health and Social Care Act (2012), has somehow resulted in an almighty mess. Like Lord Sugar, people are scrabbling around for a quick fix, but this is not going to be easy. Some of the strategies are clearly ‘science fiction’, unmarketable, or incapable of any teamwork. There appears to be too many Chiefs and not enough Indians. To coin the phrase by David Cameron, “We can’t go on like this?”
But in the meantime – the first management step must to be to say to Mr. Jeremy Hunt those immortal words…
“You’re fired”
