Home » Posts tagged 'Shibley Rahman' (Page 4)
Tag Archives: Shibley Rahman

Why are some journalists getting snooty over the social media campaign #CameronMustGo?

One of my fondest memories is when the late great Tony Benn used to pronunciate ‘socialism’ as ‘social-ism’.
I remember sitting in countless snooty debates about how the social media will never have any influence on mainstream politics.
And it is complete bollocks.
Andrew Neil’s style of interviewing, in which he blatantly despises the socialist point of view, makes my hair stand on end.
I’ve lost count of where the BBC have parrot-repeated press releases getting rid of the words “Jeremy Hunt said…”
The social media is great as we discuss issues which nobody wants us to talk about. We discuss how it has been observed that the welfare reforms are alleged to have driven some disabled citizens to suicide.
We discuss how the recovery led by the Conservatives and the Liberal Democrats is utter bollocks. The income from the tax receipts is unsurprisingly low due to the sheer number of employment contracts which pay a pittance to staff that they have to be topped up by working tax credits.
Employers are having a laugh.
The debate is utter crap. I don’t give a shit what White Van Man thinks, and that’s got nothing to do with living with North London. I do however care about social care being on its knees so that NHS hospitals can’t discharge patients in a timely prompt fashion.
So do I care about #CameronMustGo?
Too right I do, as I have absolutely zero confidence in the BBC domestic news, which has failed to discuss the legislation of the Health and Social Care Act (2012), nor the annihilation of legal aid in England.
They have refused to mention the flagship policy of Labour of finally integrating at a national level the health and care systems.
More and more people are regarding voting behaviour like customer behaviour. But I liken this to shoppers wanting to base THEIR judgment instead of buying the product that is being continually rammed down their throats.
I don’t give a monkeys about Nigel Farage and his merry band of men alleging that the quality of life of indigenous Brits is suffering due to immigrants. This is an insult to all the hardworking staff in NHS hospitals, including the ones who treat White Van Man.
This is a Government on its last legs. The LibDems may think it’s delivering a strong economy with national debt going through the roof.
I’m not sticking to their long term plan.
In fact, I’m flushing it down the toilet with a bottle of Domestos.

Yes, I am getting totally sick of NHS campaigners too

The tragedy about the context to what I am about to say is that the NHS is THE issue of the next election.
Cameron is not a leader. He’s a manager, and not a very good one.
A couple of days ago, the ‘New Economics Foundation’ published an interesting report on how the NHS reforms had been sold on false pretences.
It was an excellent report.
The story starts in the 1980s with full gusto.
Market-based reforms began in the 1980s, when support services were first contracted out, but, according to the report, continued in the 1990s, with the creation of an internal market for clinical services.
The claim was that increased competition can improve both efficiency and quality of care is a central justification of market-based reforms and the Health and Social Care Act.
The King’s Fund thought it might do too.
But many of us knew this was utter bollocks.
Reams and reams of evidence was published to the contrary, such as on the LSE blogs.
On page 5 of the Report, the experience from Serco makes chilling reading:
“Before pulling out of the Cornwall contract, Serco had replaced clinicians on its out- of-hours service with call-handlers who did not have medical training but followed a computer-generated script. The new system quadrupled ambulances called. Call handlers were then told to make new checks before calling 999 when they received what appeared to be emergency cases, so that managers could cut down the number of referrals they made to the ambulance service. A leaked management email to staff described how they should use their computer system to meet targets set down in the company’s contract on 999 responses.”
Often the NHS discussion goes round and round and round and round and round and round in circles of who started it and who continued it.
On the “private finance initiative” –
“This is a scheme that enables private companies to design, build and operate NHS (and other) facilities, using capital raised through financial markets, and then rent them back under long-term contracts lasting 30 years or more.
First introduced by the Major government, this approach was popular with New Labour, with nearly three-quarters of hospital building schemes funded through PFI between 1997 and 2009.”
And desperate Dan Poulter pulled the same rabbit out of the same that last week.
Labour “started it” with their NHS Competition and Co-operation units. They started it with their “Independent Sector Treatment Centres”.
Except… Labour didn’t start two things in particular.
One – the breach of the “four tests” in reconfiguration, which saw Lewisham win both in the High Court and Court of Appeal.
Second – the legal provision in section 76(7) Health and Social Care Act (2012), from the current Government, of a threat if services do not go to out to competitive tender if there is not a sole bidder.
We saw the same crap last week.
People saying the Clive Efford Bill didn’t go far enough – except nobody said it would abolish the purchaser provider split, PFI, the £2bn funding gap, Foundation Trusts or mutuals, or advance integration of health and care.
NHAP and KONP have gone mute on integrated care and whole person care.
There is absolutely no doubt that the situation where NHS hospitals cannot discharge patients to social care is a situation which cannot carry on.
NHS campaigners seem more concerned about proving how correct they are, than offering constructive thoughts on, say, how to improve wellbeing in long term conditions.
Mid Staffs in some quarters has furthered a toxic atmosphere of malice and retribution, and a culture of fear and nastiness, rather than thinking about how things can improve.
And it has produced a generation of journalists who are the new model jury of the health and care professions.
… except regulation of primary care was not built entirely around Harold Shipman… Harold, under a Tory Government, in case you’re wondering.
No wonder the Staffs area was plunged into a recruitment crisis after all their negative publicity.
GP surgeries are shutting like no tomorrow, and yet Hunt puts pathetic above more pathetic, while some of us are trying to put people before profit.
There will be only one party of Government on May 8th 2015. It might be a temporary Government but we don’t know who it is yet.
UKIP has made utterly contemptible comments about the NHS in the past which are well documented. The idea that Labour can work with UKIP in promoting the NHS is more than disgusting.
So another week and it’s the same old same old tired discussions.
It’s clear to me that some people prefer the foreplay to the actual act.
And it’s entirely all driven by egos. Again.

Who exactly is in denial over the Clive Efford Bill?

The Private Member’s Bill brought forward by backbencher Clive Efford MP passed by 241 votes to 18.
“From crisis to opportunity — putting citizens and companies on the path to prosperity: A better functioning internal market is a key ingredient for European growth” was updated in November 2014.
This publication is part of a series that explains what the EU does in different policy areas, why the EU is involved and what the results are.
It provides that, “The European internal market, also referred to as the single market, allows people and businesses to move and trade freely across the 28-nation group. In practice, it gives individuals the right to earn a living, study or retire in another EU country.”
It further adds that, “It also gives consumers a wider choice of items to buy at competitive prices, allows them to enjoy greater protection when shopping at home, abroad or online and makes it easier and cheaper for companies large and small to do business across borders and to compete globally.”
Not wanting to be part of Europe was of course how the late great Tony Benn used to be in agreement with Enoch Powell, even though they came from totally different political stables.
On 1 January 1973, Britain joined the “Common Market”, the European Economic Community, under a previous Conservative administration.
There has of course been a strident debate as to whether the free movement of capital, so important for capitalism, is inherently compatible with socialism at all.
Being a member of the EU, the UK has to sign up to the rules and regulations of EU law.
The current position of Labour is that the market ideology went too far under previous Labour administrations.
Critics of Labour say that they are still in denial over the “sweetheart deals” to encourage private provision under a previous administration. Labour argues that this private provision was necessary to improve clear a backlog in NHS work which existed at the time, rather than introducing private provision for the sake of it.
Much criticism centres around the “independent sector treatment centres”. John Rentoul unsurprisingly found himself in agreement with the approach Labour took at the time.
Many still within Labour still loathe what happened here. NHS campaigners affiliated to other parties have been critical of Labour in inadvertently contributing to the privatisation of the NHS, and are concerned it will happen again.
Critics point to unconscionable transactions under the private finance initiative, for example.
But historically this strand of policy started under a previous Conservative administration under Lord Major.
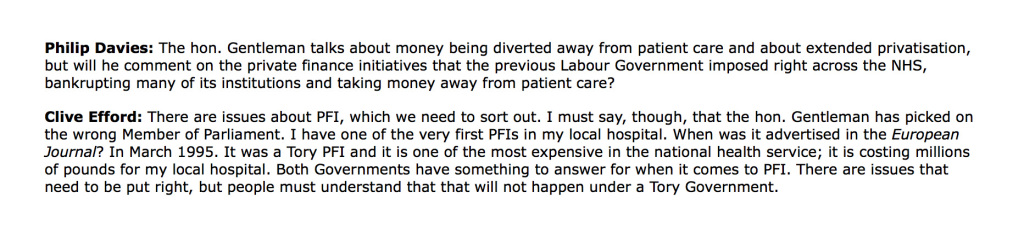
Clive Efford MP even referred to his local hospital in Eltham having been set up as the country’s first PFI hospital in last week’s debate on “The Clive Efford Bill”.
Given that we are under treaty obligations, unless there were a radical renegotiation of an unilateral exemption of the market aspect of the EU, we are stuck with a market in some form.
To argue otherwise would be in denial.
None of the front team of Labour have argued for abolition of the market altogether, to my knowledge.
But that is not to say that the ‘purchaser provider split’ might be abolished internally within England, notwithstanding treaty obligations.
The argument is that the market costs billions as it introduces “transaction costs”. The ‘household analogy’ is often used to explain the diversion of resources needed to monitoring the various transactions within a household at microlevel.
The market has become particularly problematic for the NHS, as was widely predicted before the Health and Social Care Act (2012). I myself wrote an article on the impact that section 75 Health and Social Care Act (2012) would have on the Socialist Health Association blog on 7 January 2013.
And the former CEO of NHS England, Sir David Nicholson, himself drew attention to how it had become a magnet for competition lawyers.
This was entirely to be expected as it was this clause which signalled a marked diversion from previous law under the most recent Labour government (viz section 76 sub 7 Health and Social Care Act 2012).

Elsewhere in the legislation it says that you do not have to put contracts out to competitive tender if there is only one sole bidder, which hardly ever happens.
To deny that the current legislation departs from the previous legislation is, arguably, denial.
So the “Clive Efford Bill” was finally debated last week. You can read it here. The official explanatory notes for the Bill are here.
The guidance given to the legislature is useful.
For example, for clause 6, it is provided: “The clause also enables the NHS to take advantage of exemptions to procurement obligations as set out in the European Union Directive 2014/24/EU.”
The Directive provides the ‘codification of the Teckel exemption‘.
The Teckel Exemption has proved important as an exemption from EU competition law when applied to the NHS.
Clause 1 posits that the NHS is a system based on ‘social solidarity’.
Solidarity is another mechanism of providing an exemption from EU competition law. In fact, the lack of solidarity was one of the criticisms of the Health and Social Care Bill made at the time made by ‘Richard Blogger’.
The Poucet and Pistre Case C-159, 160/91 case sheds light not heat on the ‘social solidarity’ exemption of competition law.
A reasonable concern is whether the ‘Clive Efford Bill’ hangs on by its claws to the notion of the NHS being comprised of ‘units of economic activity’ as per s.1 sub (2)(b):
But here it is the “Clive Efford Bill” which may be in denial.
Scrutiny in the Committee stage will have to be given as to whether the term here should be “general economic interest” or “general interest”.
The Government’s own guidance on this implementation of EU law is here.
If the direction of travel for all mainstream governments is genuinely to keep the proportion of private provision low, “general interest”, arguably, would be more suitable if the majority of health provision is not intended for profit.
It has been a consistent mantra from the Labour front bench “to put people before profit”, for example.
There are other issues about the significance of the words ‘deliver’ and ‘promote’ in the duty of the Secretary of State for Health.
The view of David Lock QC is here. The view of “The Campaign for the NHS 2015 Reinstatement Bill” is here.
Would a rose by any other name smell as sweet? It is a deeply entrenched position of the legal profession that lawyers look at the substance not the form.
As a statutory aid to the wording of this legislation, there is this paragraph lurking on the internet from David Lock QC from June 2013 which lends support to the notion that it is most useful if the ‘Clive Efford Bill’ is a statutory instrument best read as a whole.
Assuming that events do not overtake us, in other words we do not get chucked out of Europe imminently or the UK does not get bound in indefinitely over TTIP, we should in theory have some freedom to legislate for what sort of health service we want.
This is provided for in Article 168(7) TFEU.

It is therefore crucial we draft this legislation correctly.
Taking the position that there must be no criticism of the drafting of the Clive Efford Bill, arguing that it will undermine its implementation at Committee Stage, I think is an unreasonable position to adopt.
Likewise, grandstanding over “who is right” is inappropriate as well. There are possibly as many legal opinions as there are lawyers. We will not know with any certainty unless the Clive Efford Bill, if enacted, is put to the test by the judiciary; and even then, it will not be absolutely certain.
I think the Clive Efford Bill clearly positions itself as exempting itself from the overall gambit of EU competition law.
“It says what it does on the tin”. It is an immediate mechanism, if enacted, for getting rid of the toxic section 75 and baggage. It has been a useful campaigning tool.
But, if there is a Labour government of some sort in May 2015, it is already proposed that there will be regulation of health and care professionals as per the recommendations of the English Law Commission. This should have been in the last Queen’s Speech just gone, but the current Government chose to park this issue. Furthermore, quite drastic changes to the law will still be needed to promote integration of health and care to make whole person care work smoothly and legally. I first wrote about that issue here on this blog in June 2013. Decisions, made on clinical grounds, must be clear of competition obstructions, Enmeshing the NHS with the Enterprise Act over mergers has been a disastrous development in national policy, for example witnessed in the Bournemouth and Poole merger.
So it’s pretty likely that “The Efford Win” is the opening salvo in a war for the soul of the NHS. Time will tell whether UKIP are genuinely against privatisation. I’d bet my life on the fact are far from cuddly socialists. Their policy across a number of areas changes very rapidly, so only time will tell. The more parsimonious explanation is that UKIP are acting completely opportunistically, and wish to win seats off disaffected members across all the mainstream parties. A Labour-UKIP coalition would be very difficult to implement, whatever one thinks of Ed Miliband’s ability to negotiate a bacon butty.
The final conclusion to my book on living better with dementia
Anything can happen to anyone at any time. Despite all the best initiatives in the world, it will be unachievable to extinguish all negative perceptions about dementia. Nobody can deny the imperative for communities and society to be inclusive and accessible for people with dementia, but is no mean feat to rationalise with more individualistic approaches ranging from personal budgets, human rights and equality law responsibilities. It really is not a question of what a person can no longer do. It is an issue of what a person can currently do, and this might include, for example, unleashing of previously unwitnessed artistic and creative talents.
All jurisdictions converge on the right for a timely diagnosis and a right to timely post-diagnostic support, but political grandstanding over cures will be small change to those people currently wanting to live better with dementia. People who have received a diagnosis of dementia are not all consumers, and some do not even interact with health and care services as patients. They are all persons, however, and wish for inalienable dignity and respect. Everyone knows that the diagnosis affects not just the person with dementia,but their whole network of friends and family. There now must be a political will to do something about this, and this is not just a societal issue for the G7. Silos must be abolished; for example, in considering eating better with dementia, the emphasis can no longer be on the design of ‘finger snacks’, but responsible thought has to be put into how certain mealtime environments work (or do not work). It is utterly pointless talking about joining initiatives to encourage ‘dementia friendliness’, while words such as ‘victim’ continue to litter the mainstream press. And “leading” scientists and practitioners can unwittingly perpetuate stigma through somewhat perjorative language such as ‘wanderer’; the willful blindness to this must stop too. Living better with dementia is not just an aspiration; it is in many places legally enforceable.
Bring it on.


An overview of my book ‘Living better with dementia: champions for enhanced communities”.
I hope you find this overview of my book ‘Living better with dementia: champions for enhanced communities’ useful.
It is written by me.
And the Forewords are Prof Alistair Burns, the England clinical lead for dementia, Kate Swaffer (Alzheimer’s Australia, Dementia Alliance International, and University of Wollongong, Australia), Chris Roberts (Dementia Action Alliance Carers Call to Action, Dementia Alliance International), and Dr Peter Gordon (Consultant Psychiatrist in dementia and cognitive disorders, NHS Scotland).
It will primarily assess where we’ve got to, along with other countries, in improving diagnosis and post-diagnostic care, and assess realistically the work still yet to be done.
My thesis will articulate why the ‘reboot’ of the global “dementia friendly communities” must now take account of various issues to be meaningful. It will argue for a difference in emphasis from competitive ‘nudge’ towards universal legal and enforceable human rights promoting dignity and autonomy.
It will also argue that dementia friendly communities are meaningless unless there is a shift in the use of language away from ‘sufferers’ and ‘victims’, while paying tribute to the successful “Dementia Friends” initiative.
It will, further, argue that dementia friendly communities are best served by a large scale service transformation to ‘whole person care’, and provide the rationale for this. A critical factor for enhancing the quality of life of people living better with dementia will be to tackle meaningfully the social determinants of health, such as housing and education.
The thesis will also argue that dementia friendly communities must also value the behaviours, skills and knowledge of caregivers in wider support networks. This is essential for the development of a proactive service, with clinical specialist nursing input deservedly valued, especially given the enormous co-morbidity of dementia.
This title will be published by Jessica Kingsley Publishers, in early 2015.
Chapters overview
Chapter 1 provided an introduction to current policy in England, including a review of the need for a ‘timely diagnosis’ as well as a right to timely post-diagnostic care. This chapter also provided an overview of the current evidence base of the hugely popular “Dementia Friends” campaign run by the Alzheimer’s Society and Public Health England, to raise awareness about five key ‘facts’ about dementia. It was intended that this campaign should help to mitigate against stigma and discrimination that can be experienced by people living with dementia and their caregivers.
Chapter 2 comprised a preliminary analysis of stigma, citizenship and the notion of ‘living better with dementia’. This chapter explained the urgency of the need to “frame the narrative” properly. This chapter also introduced the “Dementia Alliance International” which has fast become a highly influential campaigning force by people living with dementia for people living with dementia.
Chapter 3 looked at the various issues facing the timely diagnosis and post-diagnostic support of people living with dementia from diverse cultural backgrounds, including people from black, Asian and ethnic minority backgrounds, people who are lesbian, bisexual, gay or transsexual, and people with prior learning difficulties.
Chapter 4 looked at the issue of how different jurisdictions around the world have formulated their national dementia strategies. Examples discussed of countries and continents were Africa, Australia, China, Europe, India, Japan, New Zealand, Puerto Rico and Scotland.
Chapter 5 looked at the intense care vs care debate which has now surfaced in young onset dementia, with a potentially problematic schism between resources being allocated into drugs for today and resources being used to fund adequately contemporary care to promote people living better with dementia. An example was discussed of how the policy of ‘Big Data’ had gathered momentum across a number of jurisdictions, offering personalised medicine as a further potential compontent of person-centred care. This chapter also considered the impact of the diagnosis of younger onset dementia on the partner of the person with dementia as well. A candid description was also given about the possible sequelae of the diagnosis of young onset dementia on employment, caregivers, and in social isolation.
Chapter 6 focused on delirium, or the acute confusional state, and dementia. It considered the NICE guidelines for delirium, and the pitfalls in considering the relationship between delirium and dementia in English policy.
Chapter 7 was the largest chapter in this book, and took as its theme care and support networks. An overview of how patient-centred care is different from person-centred care was given, and how person-centred care differs from relationship-centred care. The literature inevitably has thus far focused on the ‘dyadic relationship’ between the person with dementia and caregiver, but a need to enlarge this to a professional in a ‘triangle of care’ and extended social networks was further elaborated and emphasised. Finally, the importance of clinical specialist nurses in ‘dementia friendly communities’ was argued, as well as the Dementia Action Alliance’s “Carers Call to Action”. Different care settings were described, including care homes, hospitals – including acute hospital care, and intermediate care.
Chapter 8 considered eating for living well with dementia. This chapter considered enforceable standards in care homes, including protection against malnutrition or undernutrition. The main focus of the chapter was how people with dementia might present with alternations in their eating behaviour, and how the mealtime environment must be a vital consideration for living better with dementia.
Chapter 9 looked at a particular comorbidity, incontinence. The emphasis was on conservative approaches for living well with dementia and incontinence. Other issues considered were the impact of incontinence on personhood per se, and the possible impact on the move towards an institutional home.
Chapter 10 argued how the needs for people living better with dementia would be best served by a fully integrated health and social care service. This chapter provided the rationale behind this policy instrument in England. The chapter also considered various aspects of what would be likely to make ‘whole person care’ work, including data sharing, collaborative leadership, care-coordinators, responsible and accountable ‘self care’, and the multi-disciplinary team. This chapter also considered how it was impossible to divorce physical health from mental health and social care, and explained the intention of the longstanding drive towards ‘parity of esteem’ in English policy.
Chapter 11 considered the importance of the social determinants of health. A focus of this chapter was on education, and its impact on a person living with dementia. However, the main focus of this chapter was housing, including ‘dementia friendliness, downsizing, and green or public spaces.
Chapter 12 considered whether ‘wandering’ is the most appropriate term. The main emphasis of this chapter were the legal and ethical considerations in the use of ‘global positioning systems’ in enhancing the quality of life of persons with dementia and their closest ones.
Chapter 13 considered a number of important contemporary issues, with a main emphasis on human rights and “rights based approaches”. While there is no universal right to a budget, the implementation of personal budgets was discussed. The chapter progressed to consider a number of legal issues which are arising, including genetic discrimination in the US jurisdiction, dementia as a disability under the equality legislation in England, and the importance of rights-based approaches for autonomy and dignity. Finally, the issue of engagement was considered.
Chapter 14 was primarily concerned with art and creativity. This chapter took as its focus on how living with dementia could lead to art and creativity, and how the cultural needs of people living with dementia could best be furnished through laughter, poetry and art galleries or museums. This focus also looked at the exciting developments in our understanding of the perception of music in people living with dementia, and how music has the potential to enhance the quality of life for a person living well with dementia.
Chapter 15 looked at the triggering of football sporting memories in people living well with dementia. This chapter considered the cognitive neuroscience of the phenomenon of this triggering, and presented a synthesis of how the phenomenon could be best explained through understanding the role of emotional memory in memory retrieval, how autobiographical memories are represented in the human brain usually, the special relevance of faces or even smells such as “Bovril”.
Chapter 16 looked at the impact of various innovations in English dementia policy, giving as examples including service provision (such as the policy on reducing inappropriate use of antipsychotics or the policy in timely diagnosis) and research. This chapter also contemplated the principal factors affecting how innovations can become known, and what ultimately determines their success.
Chapter 17 looked at how leadership could be promoted by people living with dementia. This chapter considered who might lead the change, where and when, and why this change might be necessary to ‘recalibrate’ the current global debate about dementia. This chapter considered how change might be brought about from the edge, how silos might be avoided, the issue of ‘tempered radicals’ in the context of transformative change to wellbeing as an outcome; and finally how ‘Dementia Champions’ are vital for this change to be effected.
Please note that Beth is not endorsing this book – this image is entirely separate and is taken from the main event for G8 dementia – we’re all proud of Beth’s work meanwhile!


How badly does Ed Miliband want the job?

Ed Miliband has often remarked that he views his pitch for being Prime Minister being like a job interview. This is not a bad way of looking at the situation he finds himself in, one feels.
The “elevator pitch” is a construct where you’re supposed to sell yourself in the space of a short journey in an elevator. What would Ed Miliband have to do to convince you that he means business?
This question is not, “Would you like to be stuck in a lift with Ed Miliband?” But that is undoubtedly how the BBC including Andrew Neil, Andrew Marr or David Dimbleby would like to ask it.
On Facebook yesterday, Ed presented his potted ‘here’s what I stand for in four minutes’ pitch.
It’s here in case you missed it.
Presumably advisers have recommended to Ed in interviews that he must look keen to do the job. But presumably there is a limit to looking ‘too keen': i.e. desperate.
Ed being given the job depends on what the other candidates are like: and Nigel Farage, Nick Clegg and David Cameron are not the world’s most capable candidates.
It’s said that most HR recruiters ‘google’ the candidates before shortlisting. Will Ed Miliband survive the stories about him eating a butty? Or being public enemy no. 1?
Does Ed Miliband have issues he wants to bring to the table?
Yes he does: repeal of the loathed Health and Social Care Act (2012), abolition of the despised bedroom tax, a penalty for tax avoidance, and so on.
Will the media give him a fair hearing?
No.
Does Ed Miliband have a suitable background? Well, he got at least a II.1 – this is all anyone seems to care about these days. (I, for the record, think that the acquisition of a II.1 in itself is meaningless, but that’s purely a personal opinion.)
Would Ed take the job if offered it? Yes.
Will he have OK references? Not if you ask Andrew Marr, but if you ask somebody like James Bloodworth, Sunny Hundal, or Dr Éoin Clarke, yes.
Can Ed return something to his stakeholders? Possibly more than David Cameron can return to his. All Ed has to do is to win.
It’s going to be difficult. This general election on May 7th 2015 is incredibly unpredictable. The main factors, apart from Ed Miliband’s two critics, are whether the LibDem vote will collapse, how well UKIP might do, whether Scotland will be a ‘wipeout’, and so on.
But Ed Miliband’s government repealing the Health and Social Care Act (2012) is far more significant than whether he can eat a butty.

Culture and diversity in living well with dementia
This is a very important chapter to me.
Culture and diversity considerations are hugely pervasive in all of English dementia policy: from the point of timely diagnosis and throughout the course of post diagnostic support.
These are the academic journal references I wish to include in my chapter for my book ‘Living better with dementia: champions for enhanced friendly communities”.
Please do let me know of any initiatives, projects, published papers or reports that you should like me to include in this chapter.
What is listed below is only a start. It does include blogposts, which I intend to include too.
This chapter is of course hugely relevant to global dementia policy.

Aminzadeh F, Byszewski A, Molnar FJ, Eisner M. Emotional impact of dementia diagnosis: exploring persons with dementia and caregivers’ perspectives. Aging Ment Health. 2007 May;11(3):281-90.
Botsford J, Clarke CL, Gibb CE. Dementia and relationships: experiences of partners in minority ethnic communities. J Adv Nurs. 2012 Oct;68(10):2207-17. doi: 10.1111/j.1365 2648.2011.05905.x. Epub 2011 Dec 11.
Bowes A, Wilkinson H. ‘We didn’t know it would get that bad': South Asian experiences of dementia and the service response. Health Soc Care Community. 2003 Sep;11(5):387-96.
Burns A, Mittelman M, Cole C, Morris J, Winter J, Page S, Brodaty H. Transcultural influences in dementia care: observations from a psychosocial intervention study. Dement Geriatr Cogn Disord. 2010;30(5):417-23. doi: 10.1159/000314860. Epub 2010 Nov 12.
Chan WC, Ng C, Mok CC, Wong FL, Pang SL, Chiu HF. Lived experience of caregivers of persons with dementia in Hong Kong: a qualitative study. East Asian Arch Psychiatry. 2010 Dec;20(4):163-8.
Connell CM, Gibson GD. Racial, ethnic, and cultural differences in dementia caregiving: review and analysis. Gerontologist. 1997 Jun;37(3):355-64.
Day A, Francisco A. Social and emotional wellbeing in Indigenous Australians: identifying promising interventions. Aust N Z J Public Health. 2013 Aug;37(4):350-5. doi: 10.1111/1753 6405.12083.
Friedman MR, Stall R, Silvestre AJ, Mustanski B, Shoptaw S, Surkan PJ, Rinaldo CR, Plankey MW. Stuck in the middle: longitudinal HIV-related health disparities among men who have sex with men and women. J Acquire Immune Defic Syndr. 2014 Jun 1;66(2):213-20. doi: 10.1097/QAI.0000000000000143.
Johl N, Patterson T, Pearson L. What do we know about the attitudes, experiences and needs of Black and minority ethnic carers of people with dementia in the United Kingdom? A systematic review of empirical research findings. Dementia (London). 2014 May 22. pii: 1471301214534424. [Epub ahead of print]
Khan F, Tadros G. Complexity in cognitive assessment of elderly British minority ethnic groups: Cultural perspective. Dementia (London). 2013 Feb 21;13(4):467-482. [Epub ahead of print]
Kirk LJ Hick R, Laraway A. Assessing dementia in people with learning disabilities: the relationship between two screening measures. J Intellect Disabil. 2006 Dec;10(4):357-64.
La Fontaine J, Ahuja J, Bradbury NM, Phillips S, Oyebode JR. Understanding dementia amongst people in minority ethnic and cultural groups. J Adv Nurs. 2007 Dec;60(6):605-14.
Lim YY, Pietrzak RH, Snyder PJ, Darby D, Maruff P. Preliminary data on the effect of culture on the assessment of Alzheimer’s disease-related verbal memory impairment with the International Shopping List Test. Arch Clin Neuropsychol. 2012 Mar;27(2):136-47. doi: 10.1093/arclin/acr102. Epub 2011 Dec 23.
Llewellyn, P. The needs of people with learning disabilities who develop dementia: A literature review. Dementia 2011 10: 235-247.
Low LF, Anstey KJ, Lackersteen SM, Camit M, Harrison F, Draper B, Brodaty H. Recognition, attitudes and causal beliefs regarding dementia in Italian, Greek and Chinese Australians. Dement Geriatr Cogn Disord. 2010;30(6):499-508. doi: 10.1159/000321667. Epub 2011 Jan 20.
Manthorpe J, Moriarty J. Examining day centre provision for older people in the UK using the Equality Act 2010: findings of a scoping review. Health Soc Care Community. 2014 Jul;22(4):352-60. doi: 10.1111/hsc.12065. Epub 2013 Aug 17.
McCleary L, Persaud M, Hum S, Pimlott NJ, Cohen CA, Koehn S, Leung KK, Dalziel WB, Kozak J, Emerson VF, Silvius JL, Garcia L, Drummond N. Pathways to dementia diagnosis among South Asian Canadians. Dementia (London). 2013 Nov;12(6):769-89. doi: 10.1177/1471301212444806. Epub 2012 Apr 26.
Morhardt D, Pereyra M, Iris M. Seeking a diagnosis for memory problems: the experiences of caregivers and families in 5 limited English proficiency communities. Alzheimer Dis Assoc Disord. 2010 Jul-Sep;24 Suppl:S42-8. doi: 10.1097/WAD.0b013e3181f14ad5.
Nakanishi M, Nakashima T. Features of the Japanese national dementia strategy in comparison with international dementia policies: How should a national dementia policy interact with the public health- and social-care systems? Alzheimers Dement. 2014 Jul;10(4):468-76.e3. doi: 10.1016/j.jalz.2013.06.005. Epub 2013 Aug 15.
Price E. Coming out to care: gay and lesbian carers’ experiences of dementia services. Health Soc Care Community. 2010 Mar;18(2):160-8. doi: 10.1111/j.1365-2524.2009.00884.x. Epub 2009 Aug 25.
Prince M, Acosta D, Chiu H, Scazufca M, Varghese M; 10/66 Dementia Research Group. Dementia diagnosis in developing countries: a cross-cultural validation study. Lancet. 2003 Mar 15;361(9361):909-17.
Regan JL. Ethnic minority, young onset, rare dementia type, depression: A case study of a Muslim male accessing UK dementia health and social care services. Dementia (London). 2014 May 22. pii: 1471301214534423. [Epub ahead of print]
Rovner BW Casten RJ, Harris LF. Cultural diversity and views on Alzheimer disease in older African Americans. Alzheimer Dis Assoc Disord. 2013 Apr-Jun;27(2):133-7. doi: 10.1097/WAD.0b013e3182654794.
Stokes LA, Combes H, Stokes G. Understanding the dementia diagnosis: the impact on the caregiving experience. Dementia (London). 2014 Jan;13(1):59-78. doi: 10.1177/1471301212447157. Epub 2012 Aug 3.
Sun F, Ong R, Burnette D. The influence of ethnicity and culture on dementia caregiving: a review of empirical studies on Chinese Americans. Am J Alzheimers Dis Other Demen. 2012 Feb;27(1):13-22. doi: 10.1177/1533317512438224.
Werner P, Karnieli-Miller O, Eidelman S. Current knowledge and future directions about the disclosure of dementia: a systematic review of the first decade of the 21st century. Alzheimers Dement. 2013 Mar;9(2):e74-88. doi: 10.1016/j.jalz.2012.02.006. Epub 2012 Oct 24.
Wilkinson, H, Kerr, D, Cunningham, C. Equipping staff to support people with an intellectual disability and dementia in care home settings Dementia vol 4(3) 387–400

The GMC will know what is wrong with their fitness to practice procedures for unwell doctors
The GMC are conducting a review into their ‘fitness to practise’ FTP, procedures.
The independent review into deaths of Doctors who have been on their Register, awaiting FTP, is about to be published soon one hopes.
I have decided to write the GMC a last minute contribution to this consultation.
I am on currently on the Medical Register, having been erased from it in 2006/7. It is beyond reasonable doubt that I was severely ill with an alcohol dependence syndrome.
You’ll get fewer people than me wishing the GMC well, still.
I feel that the support for unwell Doctors in the National Health Service, and any hunger for scalps of Doctors will feed into this.
The question is whether the GMC can fit itself into a wider system of learning from mistakes and also supporting Doctors ‘in trouble’.
I have learnt much from my time, not least becoming into recovery from alcoholism, and being physically disabled for the first time.
But I thought it would be incorrect not for me to make some polite views known. As I say, I wish the GMC well. I am also regulated by the Solicitors Regulation Authority, so I will expect the GMC to obey a new Act of Clinical Regulation if it comes into law pursuant to the English Commission’s proposals.

General Medical Council
3 Hardman Street
Manchester
M3 3AW
Dear Sir
Re GMC Consultation over fitness to practice procedures
It is with interest I have been following your consultation over fitness to practice (FTP) procedures for the medical profession.
I have thus far tried to keep out of these discussions. I myself was only restored to the medical register earlier this year pursuant to a full Medical Practitioners Tribunal Service (MPTS) panel hearing. I can say with all honesty that being returned to your Medical Register was the happiest moment of my entire life. I consider a massive honour to be there now, and indeed became quite tearful taking about it at the recent BMA Careers Fair held in North London a few weeks ago.
My regulation with the General Medical Council (GMC) has been simultaneously ‘the best of times and the worst of times’. I had resisted of commenting on it, because I can hardly been said to have been detached from the processes. But I have gone through the full regulatory loop.
I also have, since my erasure in 2006, re-trained in law, having even obtained a Masters of Law. I feel that proportionality runs like letters through a stick of rock in all the work the legal profession does. Balancing competing interests is what lawyers do. It is what the GMC has done since 1858, reflected as well in your current tagline.
I have also, as explanation, successfully completed a MBA. I decided to study an area called ‘performance management’. I don’t feel this term is particularly helpful, but the discipline has a lot to offer both the legal and medical profession. I had become regulated by the Solicitors Regulation Authority back in January 2011, following a full due diligence procedure.
At the outset, I should wish to apologise for this short note. But I was moved by your current Chair, Prof Terence Stephenson, who told an audience of us at the Practitioners Health Programme in Swiss Cottage, London, that change is totally possible; however, it tends to be ineffective through loud criticism from the sidelines.
That is why I wish to address your concerns head on.
I feel personally my erasure was completely correct. In response to the Chairman of my MPTS panel who asked me whether my time had ‘gone badly’, I disagreed; I said “it was a complete disaster”.
Nearly a year after direction to erasure, in 2007 June I was blue lighted into the Royal Free Hospital. I had a cardiac arrest and epileptic seizure, with a rampant acute bacterial meningitis. I was then kept on life support for six weeks. I became physically disabled. The NHS, though, saved my life.
I have now been in recovery for seven years at least. I do not in any way condone the events which led to my erasure, but in law I believe that ‘but for’ my alcoholism these events would not have happened.
The direction of travel seems pretty clear. Despite a temporary stalling in the response to the English Law Commission, I feel it is likely the proposals for a root and branch reform of clinical regulation will take place shortly. I full support Niall Dickson in this.
Patient safety is paramount. But the balancing of competing interests is not the reputation of Doctors or the reputation of the regulator, but rather the needs of the patients compared to Doctors trying to do their professional work.
It is often forgotten that many Doctors feel mortified if they make a mistake. But the sheer volume of medical mistakes made daily, for example in medication errors, makes it untenable that every doctor who has ever made a mistake should face a tough public sanction.
Furthermore, cracking down too heavily on Doctors in the medical profession is completely countercurrent to the drive to learn from mistakes in the NHS. There should be a learning culture, and in the drive for quality complaints should be acted upon as gold-dust.
I have every confidence that a well respected medical profession will be possible through a well respected GMC. Ensuring high standards in medical profession is not only achieved through regulation. It will only be possible if seniors in the medical profession show leadership as to the skills they wish to see flourish in the health and care sectors.
There is no doubt for me that the investigations process is too long. There are clear ways in which the GMC departs from the standard English law (e.g. regards costs, telling you how long investigations will take, ambiguities in the civil standard of proof of applied). During that time, the mental health of certain Doctors appearing before the GMC will markedly deteriorate due to stress. Low self esteem is a massive problem in people like me who have faced alcoholism or, in the case of others, other substance misuse problems. When you add to this the trial by media which is out of the GMC’s control, the perfect storm can be utterly disastrous.
One of the principal ways in which the GMC departs from the law currently is how there is little emphasis to manage disputes at a local level. Mediation and arbitration is very important under the civil procedure rules of English law, prior to litigation. The GMC approach is adversarial.
I should like enforcement of the current code of conduct, with a view to solving problems rather than publicly sanctioning Doctors as the key priority, to be important. The enforcement of the national minimum wage, for example, has proved problematic, despite it being a very good piece of legislation. Likewise, one can easily argue that requirements for Doctors to express concerns about inadequate resources, or a duty of candour, are already enshrined in the code of conduct, and have been so for many years now.
I mean my short note with complete goodwill. The GMC has an incredibly important function to perform. I am currently under two professional regulators. Since my erasure, I have spent 7 years in recovery, nearly finished five books and graduated in three degrees and one diploma, so rehabilitation is perfectly possible in my view.
As such it’s going to be impossible for the GMC to ‘do outreach’ as regards the health of Doctors. I openly admitted to your MPTS panel that I failed in not putting myself under a GP. I worry about junior Doctors who are worried to seek help over medical issues, because of concerns about their careers. Patient safety is paramount. During time of a lengthy investigation by the GMC, with mental illness not under control, a Doctor due to be appearing in front of you can go from poor health to catastrophic health. They can become in total denial and lack insight.
Whilst I will note why you may not wish to ask about health issues because of various statutory instruments in the English law, one might consider whether it might be proportionate for there to be a ‘middle man’ overseeing sick Doctors. This is essential for separation of powers between the regulator and the regulated. The Practitioners Health Programme and Doctors Benevolent Fund deserve national resourcing. This is not solely an economic case; it is a moral one, I strongly feel.
I trust the GMC will act impressively in response to these demanding issues in due course. Please do not hesitate to contact me should you need to.
Kind regards.
Yours faithfully,
Dr Shibley Rahman
cc [REDACTED]

Journal references for my chapter on living well with dementia and urinary incontinence
I am yet to include influential blogposts, such as this one by Beth Britton (@BethyB1886).
But there is the core of my journal references which I intend to cite in my book chapter on living well with dementia and incontinence.
Please do let me know of any work, in whichever one of the media, you should like me to include. Very many thanks.

Abrams P, Blaivas J, Stanton S, Anderson J. The standardization of terminology of lower urinary tract function.Scand J Urol Nephrol 1988;(Suppl 1)14:5–10.
Afram B, Stephan A, Verbeek H, Bleijlevens MH, Suhonen R, Sutcliffe C, Raamat K, Cabrera E, Soto ME, Hallberg IR, Meyer G, Hamers JP; RightTimePlaceCare Consortium. Reasons for institutionalization of people with dementia: informal caregiver reports from 8 European countries. J Am Med Dir Assoc. 2014 Feb;15(2):108-16. doi: 10.1016/j.jamda.2013.09.012. Epub 2013 Nov 12.
Allan L, McKeith I, Ballard C, Kenny RA. The prevalence of autonomic symptoms in dementia and their association with physical activity, activities of daily living and quality of life. Dement Geriatr Cogn Disord. 2006;22(3):230-7. Epub 2006 Aug 10.
Allen J, Oyebode JR, Allen J (2009) Having a father with young onset dementia: The impact on well-being of young people. Dementia. 8: 455-480.
Berrios G. Urinary incontinence and the psychopathology of the elderly with cognitive failure. Gerontology 1986;32:119–24.
Boustani MA, Sachs GA, Alder CA, Munger S, Schubert CC, Guerriero Austrom M, Hake AM, Unverzagt FW, Farlow M, Matthews BR, Perkins AJ, Beck RA, Callahan CM. Implementing innovative models of dementia care: The Healthy Aging Brain Center. Aging Ment Health. 2011 Jan;15(1):13-22. doi: 10.1080/13607863.2010.496445.
Brandeis GH, Baumann MM, Hossain M, Morris JN, Resnick NM. The prevalence of potentially remediable urinary incontinence in frail older people: a study using the Minimum Data Set. J Am Geriatr Soc. 1997 Feb;45(2):179-84.
Brocklehurst J, Dillane J. Studies of the female bladder in old age II: cystometrograms in 100 incontinent women. Gerontol Clin 1966;8:306–19.
Campbell A, Reinken J, McCosh L. Incontinence in the elderly: prevalence and prognosis. Age Ageing 1985;14:65–70.
Clarkson, P, Abendstern, M, Sutcliffe, C, Hughes, J, Challis, D. (2012) The identification and detection of dementia and its correlates in a social services setting: Impact of a national policy in England Dementia September 2012 vol. 11 no. 5 617-632
Downs M. Embodiment: the implications for living well with dementia. Dementia (London). 2013 May;12(3):368-74. doi: 10.1177/1471301213487465.
Drennan VM, Norrie C, Cole L, Donovan S. Addressing incontinence for people with dementia living at home: a documentary analysis of local English community nursing service continence policies and clinical guidance. J Clin Nurs. 2013 Feb;22(3-4):339-46. doi: 10.1111/j.1365
2702.2012.04125.x. Epub 2012 Jul 13.
Drennan, VM, Cole, L, Iliffe . A taboo within a stigma? a qualitative study of managing incontinence with people with dementia living at home, BMC Geriatrics 2011, 11:75
Drennan, VM, Greenwood, N, Cole, L, Fader, M, Grant, R, Rait, G, Iliffe, S. Conservative interventions for incontinence in people with dementia or cognitive impairment, living at home: a systematic review BMC Geriatrics 2012, 12:77 doi:10.1186/1471-2318-12-77
Ebly EM, Hogan DB, Rockwood K. Living alone with dementia. Dement Geriatr Cogn Disord. 1999 Nov-Dec;10(6):541-8.
Eggermont L H, Scherder E J. Physical activity and behaviour in dementia: a review of the literature and implications for psychosocial intervention in primary care. Dementia 2006; 5(3): 4 1-428.
Ekelund P, Rundgren A. Urinary incontinence in the elderly with implications for hospital care consumption and social disability. Arch Gerontol Geriatr. 1987 Apr;6(1):11-8.
Evans D, Lee E. Impact of dementia on marriage: a qualitative systematic review. Dementia (London). 2014 May;13(3):330-49. doi: 10.1177/1471301212473882. Epub 2013 Jan 25.
Flint A, Skelly J. The management of urinary incontinence in dementia. Int J Geriatr Psychiatry 1994;9:245–6.
Hägglund D. A systematic literature review of incontinence care for persons with dementia: the research evidence. J Clin Nurs. 2010 Feb;19(3-4):303-12. doi: 10.1111/j.1365 2702.2009.02958.x.
Hasegawa J, Kuzuya M, Iguchi A. Urinary incontinence and behavioral symptoms are independent risk factors for recurrent and injurious falls, respectively, among residents in long term care facilities. Arch Gerontol Geriatr. 2010 Jan-Feb;50(1):77-81. doi: 10.1016/j.archger.2009.02.001. Epub 2009 Mar 17.
Hellström L, Ekelund P, Milsom I, Skoog I. The influence of dementia on the prevalence of urinary and faecal incontinence in 85-year-old men and women. Arch Gerontol Geriatr. 1994 Jul-Aug;19(1):11-20.
Hirasawa, Y, Masuda, Y, Kuzuya, M, Kimata, T, Iguchi, A, Uemura, K. End-o life experience of demented elderly patients at home: findings from DEATH project. Psychogeriatrics, Volume 6, Issue 2, pages 60–67, June 2006
Hirsh D, Fainstein C, Musher D. Do condom catheter collecting systems cause urinary tract infection? JAMA 1979;242:340.
Idiaquez J, Roman GC. Autonomic dysfunction in neurodegenerative dementias. J Neurol Sci. 2011 Jun 15;305(1-2):22-7. doi: 10.1016/j.jns.2011.02.033. Epub 2011 Mar 25. Review.
Iltanen-Tähkävuori, S. Design and dementia: A case of garments designed to prevent undressing. Dementia January 2012 vol. 11 no. 1 49-59
Jirovec M. Urine control in patients with chronic degenerative brain disease. In: Altman H ed. Alzheimer’s disease problems: prospects and perspectives. New York: Plenium Press, 1986.
Jirovec MM, Wells TJ. Urinary incontinence in nursing home residents with dementia: the mobility-cognition paradigm. Appl Nurs Res. 1990 Aug;3(3):112-7.
Kraemer HC, Taylor JL, Tinklenberg JR, Yesavage JA.The stages of Alzheimer’s disease: a reappraisal. Dement Geriatr Cogn Disord. 1998 Nov-Dec;9(6):299-308.
Kraijo, H, Brouwer, W, de Leeuw, R, Schrijvers, G.Coping with caring: Profiles of caregiving by informal carers living with a loved one who has dementia. Dementia November 7, 2011 1471301211421261
Leung FW, Schnelle JF. Urinary and fecal incontinence in nursing home residents. Gastroenterol Clin North Am. 2008 Sep;37(3):697-707, x. doi: 10.1016/j.gtc.2008.06.005. Review
Lussier M, Renaud M, Chiva-Razavi S, Bherer L, Dumoulin C. Are stress and mixed urinary incontinence associated with impaired executive control in community-dwelling older women? J Clin Exp Neuropsychol. 2013;35(5):445-54. doi: 10.1080/13803395.2013.789483. Epub 2013 May 8.
Måvall, L, Malmberg, B. Day care for persons with dementia. An alternative for whom? Dementia February 2007 vol. 6 no. 1 27-43
Mo F, Choi BC, Li FC, Merrick J. Using Health Utility Index (HUI) for measuring the impact on health-related quality of Life (HRQL) among individuals with chronic diseases. ScientificWorldJournal. 2004 Aug 27;4:746-57.
O’Donnell BF, Drachman DA, Barnes HJ, Peterson KE, Swearer JM, Lew RA. Incontinence and troublesome behaviors predict institutionalization in dementia. J Geriatr Psychiatry Neurol. 1992 Jan-Mar;5(1):45-52.
Orrell M, Hancock GA, Liyanage KC, Woods B, Challis D, Hoe J. The needs of people with dementia in care homes: the perspectives of users, staff and family caregivers. Int Psychogeriatr. 2008 Oct;20(5):941-51. doi: 10.1017/S1041610208007266. Epub 2008 Apr 17.
Ouslander J, Leach G, Staskin D, Abelson S, Blaustein J, Morishita L, Raz S. Prospective evaluation of an assessment strategy for geriatric urinary incontinence. J Am Geriatr Soc. 1989 Aug;37(8):715-24.
Rabins P, Mace N, Lucas M. The impact of dementia on the family. JAMA 1982;248:333–5.
Rai, J, Parkinson, R. Urinary incontinence in adults/ Surgery Volume 32, Issue 6, p286–291
Resnick, NM: “Urinary incontinence in the elderly.” Medical Grand Rounds 3:281-290, 1984.
Sakakibara R, Uchiyama T, Yamanishi T, Kishi M. Dementia and lower urinary dysfunction: with a reference to anticholinergic use in elderly population. Int J Urol. 2008 Sep;15(9):778-88. doi: 10.1111/j.1442-2042.2008.02109.x. Epub 2008 Jul 14.
Skelly J, Flint A. Urinary incontinence associated with dementia. J Am Geriatr Soc 1995;43:286–94.
Tadros G, Ormerod S, Dobson-Smyth P, Gallon M, Doherty D, Carryer A, Oyebode J, Kingston P. The management of behavioural and psychological symptoms of dementia in residential homes: does Tai Chi have any role for people with dementia? Dementia (London). 2013 Mar;12(2):268-79. doi: 10.1177/1471301211422769. Epub 2011 Nov 20. Review.
Teri L, Borson S, Kiyak HA, Yamagishi M. Behavioral disturbance, cognitive dysfunction, and functional skill. Prevalence and relationship in Alzheimer’s disease. J Am Geriatr Soc. 1989 Feb;37(2):109-16.
Tilvis RS, Hakala SM, Valvanne J, Erkinjuntti T. Urinary incontinence as a predictor of death and institutionalization in a general aged population. Arch Gerontol Geriatr. 1995 Nov Dec;21(3):307-15.
Toot S, Hoe J, Ledgerd R, Burnell K, Devine M, Orrell M. Causes of crises and appropriate interventions: the views of people with dementia, carers and healthcare professionals. Aging Ment Health. 2013;17(3):328-35. doi: 10.1080/13607863.2012.732037. Epub 2012 Nov 16.
Ward R, Campbell S. Mixing methods to explore appearance in dementia care. Dementia (London). 2013 May;12(3):337-47. doi: 10.1177/1471301213477412. Epub 2013 Feb 26.
Yap P, Tan D. (2006) Urinary incontinence in dementia – a practical approach, Aust Fam Physician, 35(4), pp. 237-41.
Yokoi T, Okamura H. Why do dementia patients become unable to lead a daily life with decreasing cognitive function? Dementia (London). 2013 Sep;12(5):551-68. doi: 10.1177/1471301211435193. Epub 2012 Mar 16.

The chapter on art, music and creativity for my new book on living better with dementia
The following are the journal references for my chapter on art, music and creativity for my book “Living better with dementia: champions for enhanced friendly communities”. Please do let me know if you wish to have any further academic papers cited. And also please do let me know if you wish local initiatives or innovations to be featured in my chapter, and I will do my best to include them if appropriate.
Very many thanks.

Amaducci L, Grassi E, Boller F. Maurice Ravel and right-hemisphere musical creativity: influence of disease on his last musical works? Eur J Neurol. 2002 Jan;9(1):75-82.
Basaglia-Pappas S, Laterza M, Borg C, Richard-Mornas A, Favre E, Thomas-Antérion C. Exploration of verbal and non-verbal semantic knowledge and autobiographical memories starting from popular songs in Alzheimer’s disease. Int Psychogeriatr. 2013 May;25(5):785-95. doi: 10.1017/S1041610212002359. Epub 2013 Feb 7.
Beard, R.L. Art therapies and dementia care: A systematic review 2012 11: 633-656.
Bisiani L, Angus J. Doll therapy: a therapeutic means to meet past attachment needs and diminish behaviours of concern in a person living with dementia–a case study approach. Dementia (London). 2013 Jul;12(4):447-62. doi: 10.1177/1471301211431362. Epub 2012 Feb 15.
Blood AJ, Zatorre RJ. Intensely pleasurable responses to music correlate with activity in brain regions implicated in reward and emotion. Proc Natl Acad Sci U S A. 2001 Sep 25;98(20):11818-23.
Budrys V, Skullerud K, Petroska D, Lengveniene J, Kaubrys G. Dementia and art: neuronal intermediate filament inclusion disease and dissolution of artistic creativity. Eur Neurol. 2007;57(3):137-44. Epub 2007 Jan 10.
Camic PM, Chatterjee HJ. Museums and art galleries as partners for public health interventions. Perspect Public Health. 2013 Jan;133(1):66-71. doi: 10.1177/1757913912468523.
Camic PM, Tischler V, Pearman CH. Viewing and making art together: a multi-session art gallery-based intervention for people with dementia and their carers. Aging Ment Health. 2014 Mar;18(2):161-8. doi: 10.1080/13607863.2013.818101. Epub 2013 Jul 22.
Camic PM, Williams CM, Meeten F. Does a ‘Singing Together Group’ improve the quality of life of people with a dementia and their carers? A pilot evaluation study. Dementia (London). 2013 Mar;12(2):157-76. doi: 10.1177/1471301211422761. Epub 2011 Oct 31.
Chakravarty A. De novo development of artistic creativity in Alzheimer’s disease. Ann Indian Acad Neurol. 2011 Oct;14(4):291-4. doi: 10.4103/0972-2327.91953.
Crutch SJ, Isaacs R, Rossor MN. Some workmen can blame their tools: artistic change in an individual with Alzheimer’s disease. Lancet. 2001 Jun 30;357(9274):2129-33.
Eekelaar, C., Camic, P. M., Springham, N. Art galleries, episodic memory and verbal fluency in dementia: An exploratory study. Psychology of Aesthetics, Creativity, and the Arts, Vol 6(3), Aug 2012, 262-272.
Fletcher PD, Clark CN, Warren JD. Music, reward and frontotemporal dementia. Brain. 2014 Oct;137(Pt 10):e300. doi: 10.1093/brain/awu145. Epub 2014 Jun 11.
Fletcher PD, Downey LE, Witoonpanich P, Warren JD. The brain basis of musicophilia: evidence from frontotemporal lobar degeneration. Front Psychol. 2013 Jun 21;4:347. doi: 10.3389/fpsyg.2013.00347. eCollection 2013.
Fornazzari LR. Preserved painting creativity in an artist with Alzheimer’s disease. Eur J Neurol. 2005 Jun;12(6):419-24.
Gjengedal E, Lykkeslet E, Sørbø JI, Sæther WH. ‘Brightness in dark places': theatre as an arena for communicating life with dementia. Dementia (London). 2014 Sep;13(5):598-612. doi: 10.1177/1471301213480157. Epub 2013 Mar 13.
Gold K. But does it do any good? Measuring the impact of music therapy on people with advanced dementia: (Innovative practice). Dementia (London). 2014 Mar 1;13(2):258-64. doi: 10.1177/1471301213494512. Epub 2013 Jul 26.
Gordon N. Unexpected development of artistic talents. Postgrad Med J. 2005 Dec;81(962):753-5.
Gross SM, Danilova D, Vandehey MA, Diekhoff GM. Creativity and dementia: Does artistic activity affect well-being beyond the art class? Dementia (London). 2013 May 22. [Epub ahead of print]
Guétin S, Portet F, Picot MC, Pommié C, Messaoudi M, Djabelkir L, Olsen AL, Cano MM, Lecourt E, Touchon J. Effect of music therapy on anxiety and depression in patients with Alzheimer’s type dementia: randomised, controlled study. Dement Geriatr Cogn Disord. 2009;28(1):36-46. doi: 10.1159/000229024. Epub 2009 Jul 23.
Hafford-Letchfield T. Funny things happen at the Grange: introducing comedy activities in day services to older people with dementia–innovative practice. Dementia (London). 2013 Nov;12(6):840-52. doi: 10.1177/1471301212454357. Epub 2012 Jul 9.
Holland AC, Kensinger EA. Emotion and autobiographical memory. Phys Life Rev. 2010 Mar;7(1):88-131. doi: 10.1016/j.plrev.2010.01.006. Epub 2010 Jan 11. Review.
Hsieh S, Hornberger M, Piguet O, Hodges JR. Neural basis of music knowledge: evidence from the dementias. Brain. 2011 Sep;134(Pt 9):2523-34. doi: 10.1093/brain/awr190. Epub 2011 Aug 21.
James IA, Mackenzie L, Mukaetova-Ladinska E. Doll use in care homes for people with dementia. Int J Geriatr Psychiatry. 2006 Nov;21(11):1093-8.
Janata P. The neural architecture of music-evoked autobiographical memories. Cereb Cortex. 2009 Nov;19(11):2579-94. doi: 10.1093/cercor/bhp008. Epub 2009 Feb 24.
LaBar KS, Cabeza R. Cognitive neuroscience of emotional memory. Nat Rev Neurosci. 2006 Jan;7(1):54-64. Review.
Lazar A, Thompson H, Demiris G. A systematic review of the use of technology for reminiscence therapy. Health Educ Behav. 2014 Oct;41(1 Suppl):51S-61S. doi: 10.1177/1090198114537067.
Mezirow J. (2000) Learning to think like an adult. In J. Mezirow and Associates, Learning as transformation: Critical perspectives on a theory in process. (pp. 3-33). San Francisco: Jossey Bass.
Miller BL, Boone K, Cummings JL, Read SL, Mishkin F. Functional correlates of musical and visual ability in frontotemporal dementia. Br J Psychiatry. 2000 May;176:458-63.
Miller BL, Cummings J, Mishkin F, Boone K, Prince F, Ponton M, Cotman C. Emergence of artistic talent in frontotemporal dementia. Neurology. 1998 Oct;51(4):978-82.
Miller, B.L., Yener, G, Akdal, G. (2005) Artistic patterns in dementia, Journal of Neurological Sciences (Turkish), vol. 22(3), pp. 245-249.
Mitchell G, McCormack B, McCance T. Therapeutic use of dolls for people living with dementia: A critical review of the literature. Dementia August 25, 2014 1471301214548522.
Mitchell G, McCormack B, McCance T. Therapeutic use of dolls for people living with dementia: A critical review of the literature. Dementia (London). 2014 Aug 25. pii: 1471301214548522. [Epub ahead of print]
Mitchell G, Templeton M. Ethical considerations of doll therapy for people with dementia. Nurs Ethics. 2014 Sep;21(6):720-30. doi: 10.1177/0969733013518447. Epub 2014 Feb 3.
Omar R, Hailstone JC, Warren JE, Crutch SJ, Warren JD. The cognitive organization of music knowledge: a clinical analysis. Brain. 2010 Apr;133(Pt 4):1200-13. doi: 10.1093/brain/awp345. Epub 2010 Feb 8.
Pezzati R, Molteni V, Bani M, Settanta C, Di Maggio MG, Villa I, Poletti B, Ardito RB. Can Doll therapy preserve or promote attachment in people with cognitive, behavioral, and emotional problems? A pilot study in institutionalized patients with dementia. Front Psychol. 2014 Apr 21;5:342. doi: 10.3389/fpsyg.2014.00342. eCollection 2014.
Ramachandran, VS, Hirstein, (1999) The science of art: a neurological theory of aesthetic experience. Journal of Consciousness Studies (6), no.6-7, pp.15-51.
Rankin KP, Liu AA, Howard S, Slama H, Hou CE, Shuster K, Miller BL. A case-controlled study of altered visual art production in Alzheimer’s and FTLD. Cogn Behav Neurol. 2007 Mar;20(1):48 61.
Roe B, McCormick S, Lucas T, Gallagher W, Winn A, Elkin S. Coffee, Cake & Culture: Evaluation of an art for health programme for older people in the community. Dementia (London). 2014 Mar 31. [Epub ahead of print]
Salimpoor VN, Benovoy M, Longo G, Cooperstock JR, Zatorre RJ. The rewarding aspects of music listening are related to degree of emotional arousal. PLoS One. 2009 Oct 16;4(10):e7487. doi: 10.1371/journal.pone.0007487.
Seeley WW, Matthews BR, Crawford RK, Gorno-Tempini ML, Foti D, Mackenzie IR, Miller BL. Unravelling Boléro: progressive aphasia, transmodal creativity and the right posterior neocortex. Brain. 2008 Jan;131(Pt 1):39-49. Epub 2007 Dec 5.
Stevens, J 2012, ‘Stand up for dementia: performance, improvisation and stand up comedy as therapy for people with dementia; a qualitative study’, Dementia, vol. 11, no. 1, pp. 61-73.
Takahata K, Saito F, Muramatsu T, Yamada M, Shirahase J, Tabuchi H, Suhara T, Mimura M, Kato M. Emergence of realism: Enhanced visual artistry and high accuracy of visual numerosity representation after left prefrontal damage. Neuropsychologia. 2014 May;57:38-49. doi: 10.1016/j.neuropsychologia.2014.02.022. Epub 2014 Mar 11.
Takeda M, Hashimoto R, Kudo T, Okochi M, Tagami S, Morihara T, Sadick G, Tanaka T. Laughter and humor as complementary and alternative medicines for dementia patients. BMC Complement Altern Med. 2010 Jun 18;10:28. doi: 10.1186/1472-6882-10-28.
Tanaka, Y, Nogawa, H, Tanaka, H. (2012) Music Therapy with Ethnic Music for Dementia Patients, International Journal of Gerontology Volume 6, Issue 4, December 2012, Pages 247 257.
Topo, P, Mäki,O, Saarikalle, K, Clarke, N, Begley, E, Cahill, S, Arenlind, J, Holthe, T, Morbey, H, Hayes, K, Gilliard, J. Dementia October 2004 Assessment of a Music-Based Multimedia Program for People with Dementia vol. 3 no. 3 331-350
Woods RT, Bruce E, Edwards RT, Elvish R, Hoare Z, Hounsome B, Keady J, Moniz-Cook ED, Orgeta V, Orrell M, Rees J, Russell IT. REMCARE: reminiscence groups for people with dementia and their family caregivers – effectiveness and cost-effectiveness pragmatic multicenter randomised trial. Health Technol Assess. 2012;16(48):v-xv, 1-116. doi: 10.3310/hta16480.
Zeilig H. Gaps and spaces: representations of dementia in contemporary British poetry. Dementia (London). 2014 Mar 1;13(2):160-75. doi: 10.1177/1471301212456276. Epub 2012 Aug 17.
