Home » Posts tagged 'Shibley Rahman' (Page 5)
Tag Archives: Shibley Rahman

Stigma in dementia poses crucial questions for dementia friendly communities
The literature on stigma is comprehensive.
But Kate Swaffer added to it beautifully in the journal ‘Dementia’, with an article today – on open access – entitled “Dementia: Stigma, language and dementia friendly”.
Kate refers to a blogpost by Ken Clasper, a Dementia Friends Champion, which asks, sensibly, what we are trying to achieve with more ‘awareness’.

And if you scroll down to the end of this tour de force on stigma and dementia, you’ll see exactly why Kate is able to opine with such legitimacy and authority.

I conceded a long time ago – in March 2014, in fact – on this blog that the policy plank of ‘dementia friendly communities’ is an incredibly complex one.
The discussion of stigma seems to be one of perpetuity. We’ve seen numerous attempts at it, including the original work of Goffman (1963) on stigma and ‘spoiled identity’.
It’s been re-incarnated as a Royal College of Psychiatrists campaign on stigma.
This morning there was another bite of the cherry.
The report, New perspectives and approaches to understanding dementia and stigma, published by the think tank International Longevity Centre UK (ILC-UK) is produced by the MRC, Alzheimer’s Research UK, and Alzheimer’s Society; it was also supported by Pfizer.
I’ve thought how I could possibly respond to Kate. And I can’t, as Kate is in every sense of the word an ‘expert’.
But it did get me thinking.
It got me thinking of the happy times I had with Chris and Jayne last week at the Alzheimer Europe conference in the city of my birth in Glasgow.
‘There’s more to the person than the diagnosis” is one of the key five messages of ‘Dementia Friends’, an initiative from the Alzheimer’s Society predominantly (and Public Health England). This is mirrored in a tweet by Chris from this morning.

Chris is also a “Dementia Friends Champion“, and lives well with dementia.
Last week, I attended a brilliant all-day workshop chaired by Karishma Chandaria, Dementia Friendly Communities manager for the Alzheimer’s Society. The progress which has been made on this policy plank is substantial, and I am certain that the next Government will wish to support this policy initiative in the English for 2015-20.

It is stated clearly in Simon Stevens’ “Five Year Plan” for NHS England.

It is a core thread of the Prime Minister’s Dementia Challenge.
And the ‘coalition of the good’ has seen the dementia friendly communities policy plank develop drawing on work from ‘Innovations in dementia’ and the Joseph Rowntree Foundation.
And to give the Alzheimer’s Society credit, where it is certainly due, there has been launched an open consultation for a British Code of Practice (currently ongoing), to which anybody can contribute.
But this code of practice does, again, have the potential to be very divisive. It might be painful to make dementia friendly communities, such as the large one in Torbay, ‘fit into this box’.
Torbay in many ways is a beacon of innovation for integration between NHS and care. There is genuine “community bind”, with citizens, shopkeepers, transport, police, for example, contributing.
The article on the BBC website about Norman McNamara (January 2012) predates the Prime Minister’s Dementia Challenge, (which started in March 2012.)
Any top down way of making bottom-up social groups ‘conform’ will be hugely problematic in the implementation of this approach to dementia-friendly communities, potentially.
The methodology of dementia friendly communities has to be truly inclusive: it is all or nothing.
I agree with Kate, and like her I wish to avoid protracted circular definitions of ‘stigma’. For me, I recognise stigma when you see it, like how the Supreme Court of the US recognises erotica and pornography as per Jacobellis v Ohio [1964].
It is possibly easier to define stigma by its sequelae, such as avoiding wishing to talk about dementia in polite conversation, or not wishing to see your GP about possible symptoms of a dementia in its early stages, or not wanting to socialise with people with dementia who happen to be in your family.
We know these are real phenomena, as demonstrated, for example, by the loneliness of many people on receiving a diagnosis of possible dementia.
And we know stigma can harbour deep-seated irrational prejudice, like the incorrect notion that dementia is somehow contagious like a ‘superbug’.
Stigma can be exhibited in pretty nasty ways in language: such as “snap out of it” or “victim”.
My discussion of whether people living with dementia are ‘sufferers’ tends to go round and round in circles with people who disagree with me.
Suffice to say, I agree it is possible for a person living with dementia, such as a person who has received a diagnosis of Lewy body dementia and who has to put up with terrible “night terrors” and exhaustion the following day.
I think if you live independently, but with full insight into your symptoms, it can be exasperating. I have never been in that position though, and it would be invidious of me to second-guess.
I think if you are close to someone in the latter stages of dementia, you can suffer.
But I’ve written about this all, indeed on this blog, before here.
The only thing that is new is Peanuts’ cartoon (original citation here).

In that workshop, I also sat through Joy and Tone Watson’s brilliant “Dementia Friends” session. Joy lives with dementia. And their session was brilliant.
This was the final ‘exhibit’.

I attended a special group session on stigma with Toby Williamson from the Mental Health Foundation during that day. In that session, it was mentioned that ‘rôle models’ of people living well with dementia might help to break down stigma.
Or maybe guidance for the media might help? One cannot help wondering if an article such as in the Daily Mail today might actually put off people from seeking a diagnosis of dementia (completely unintentionally).
But I did bring up something on my mind.
“Stigmata” literally means signs.
But dementia can be, like other disabilities, quite invisible.
Somebody might have insidious change in personality and behaviour, noticed by somebody closest to him or her, with no obvious changes in cognition (nor indeed in investigations).
I showed this in my paper published in Brain in 1999, currently also in the Oxford Textbook of Medicine.
The condition I refer to is in fact one of the more prevalent causes of dementia in the younger age group, called the “behavioural variant of frontotemporal dementia“.
If the signs are ‘visible’, then you are obliged legally to make reasonable adjustments for any disability. In England, this includes dementia under the guidance to the Equality Act (2010).
As Toby Williamson says, if you’re obliged to build a ramp for somebody in a wheelchair for a place of work, there’s an equal obligation to produce adequate signage for people who have navigation problems as a result of a dementia such as dementia of the Alzheimer’s type.
There are reams and reams of evidence on equality and the built environment (for example the Design Council or Commission for Architecture and the Built Environment).
I personally think it’s brilliant you can go into certain shops, and the customer-facing staff will, potentially, be able to recognise if a person does need time and space to pay for items.
This is also been tackled in the Scottish jurisdiction through Alzheimer Scotland.
Also, corporate lawyers should be advising large employers about the scope for unfair dismissal claims by people dismissed as they are about to arrive at a diagnosis of dementia (particularly young onset dementia).
The timeline is roughly this. Somebody has health problems – he or she is invited to leave and given a pay off – these health problems turn out to be a diagnosis of probable dementia – by this time the dismissal is not unfair.
I feel confident the ‘dementia friendly communities’ policy strand in England, and across other jurisdictions, is here to stay. I share, though, Kate’s concerns that about the relative ease with which this policy has lifted off, say, compared to how one might feel about ‘gay friendly communities’ or ‘black friendly communities’. One has to be extremely careful about any policy plank which alerts people to divisions, “them against us”.
This is what I know best as the “don’t think of elephants phenomenon” and then you think of elephants.
This policy, anyway, currently has huge momentum. Marc Wortmann is currently Executive Director of Alzheimer’s Disease International (ADI), the organisation providing a global voice for dementia and the founder of World Alzheimer’s Month. Wortmann has been instrumental in propelling dementia friendly communities to the foreground of world policy.
But, in firing up ‘dementia friendly communities’ (a term which I think is sub-optimal’), v 2.0, there is plenty of time to get it right.

The 24th Annual Conference for Alzheimer Europe put people with dementia in the driving seat. Deservedly so.
The biggest dementia conference to be taken place in Scotland (“Conference”, attended by 800 professionals, people with dementia and carers) was held in Glasgow last week (20-23 October 2014).
The focus of the conference was Dignity and autonomy in Dementia and the four day event explored in quite some detail how recognising the human rights of people with dementia, their carers, partners and families is key to ensuring dignity and respect, as well as overcoming stigma.
It was the 24th Annual Conference of Alzheimer Europe (@AlzheimerEurope, an umbrella organisation of 36 Alzheimer associations from 31 countries across Europe), supported this year by Alzheimer Scotland, .
The timetable was exacting.
The people there were very special; for example Tommy Whitelaw (@TommyNTour) mentioned in Alex Neil MSP’s speech at the conference. Tommy and Irene Oldfather (@IreneOldfather) happened to be passing through during one of my poster sessions.

And Beth Britton (@BethyB1886).

Well done to the conference organisers for putting it together, especially Gladwys Guillory.

The main conference hall of the venue, the Crowne Plaza in Glasgow, the Argyll Suite, was majestic.
I particularly liked the ‘live Twitter feed’ at the front of the hall, where curiously Kate Swaffer (@KateSwaffer) appeared many times all the way from Australia. Here I am appearing with my ‘selfie’, with somebody well known in the foreground of the photograph.

The relative failure of the medical model in addressing the needs of people with dementia and caregivers was a pervasive theme throughout the whole conference.


I had a nice chat with Marc Wortmann (@marcwort) over one of the lunches. Marc is in charge of all aspects of ADI’s work (ADI = Alzheimer Disease (and associated conditions) International; @AlzDisInt). Collaborating with the Board, Marc implements finance and campaign strategies.
Marc represents ADI at international conferences and in the NCD Alliance and takes part in WHO and UN meetings. I was also able to bump into Jean Georges (@JeanGeorgesAE), the Executive Director of Alzheimer Europe.

Cabinet Secretary for Health, Alex Neil, delivered a clear keynote speech to the conference at the Tuesday morning plenary session, in which he paid tribute to the immense contribution of Tommy Whitelaw.
Key to the event was the signing of the Glasgow Declaration: a commitment to promoting the rights, dignity and autonomy of people living with dementia across Europe, as guaranteed in the European Convention of Human Rights and the Universal Declaration of Human Rights.

Here’s a great slide of @alzscot‘s “PANEL” (pic taken by @LauraMcC86).

The satellite symposium sessions were well put together, and attracted substantial audiences.
There was an amazing moment when Agnes Houston (@Agnes_Houston), Chair Scottish Dementia Working Group, said to Helga Rohra (@ContactHelga), the Chair of the satellite session and Chair of European Persons With Dementia, “All we people with dementia need is a bit of help — AND A BIT OF TIME!”
A quotation from Agnes – from a previous conference – says it all for me.


The audience burst out laughing.
The reason for this is that Agnes had been originally timetabled to have more time for her slot, apparently.
As the conference was themed around the law, including human rights, invariably discrimination against people with dementia came up in various forms.

I asked about the topic several times.
One talk of the entire programme which I thought was truly outstanding was PL1.3. Gráinne McGettrick (Alzheimer’s Society of Ireland): The UN Disability Convention as an instrument for people with dementia and their carers.

In the English jurisdiction, dementia can count as a disability; therefore there are statutory requirements for ensuring dementia-friendly communities from employers. Also, unfair dismissal of a person on account of being newly diagnosed with dementia will clearly be unlawful.
A member of the audience politely pointed out to me afterwards that a person normally gets sacked first, and then gets his or her diagnosis of dementia confirmed much later, so at the point of dismissal the dismissal does not obviously appear unfair legally.
I found this observation incredibly insightful, as there have been thus far no ‘test cases’ of unfair dismissal on grounds of a diagnosis of dementia in the English jurisdiction.

I had brought along my book ‘Living well with dementia’, but I rarely got a chance to read (or refer) to it during the course of the whole week!

I asked several times why there is no representative of persons living with dementia or caregivers on the World Dementia Council (@WorldDementia). The background to this fiasco is explained here.
I had designed that I would be staying in the same competitively-priced hôtel as Jayne Goodrick (@JayneGoodrick) and Chris Roberts in Glasgow for the 24th Alzheimer Europe conference held in Glasgow, the city where I was born.
It was by chance we gave a lift to Dr Ruth Bartlett (@RuthLBartlett) to the conference venue. Ruth was staying, as it turns out, in the same competitively-priced hôtel.
Ruth is of course well known for her well respected contributions about the citizenship of of people living with dementia, and how this has influenced the ‘involvement’ of people with dementia in policy.
This was us just before the opening ceremony – when we were full of energy.

I really enjoyed speaking with Geoff Huggins (@GeoffHuggins), who gave an excellent speech in the opening ceremony.

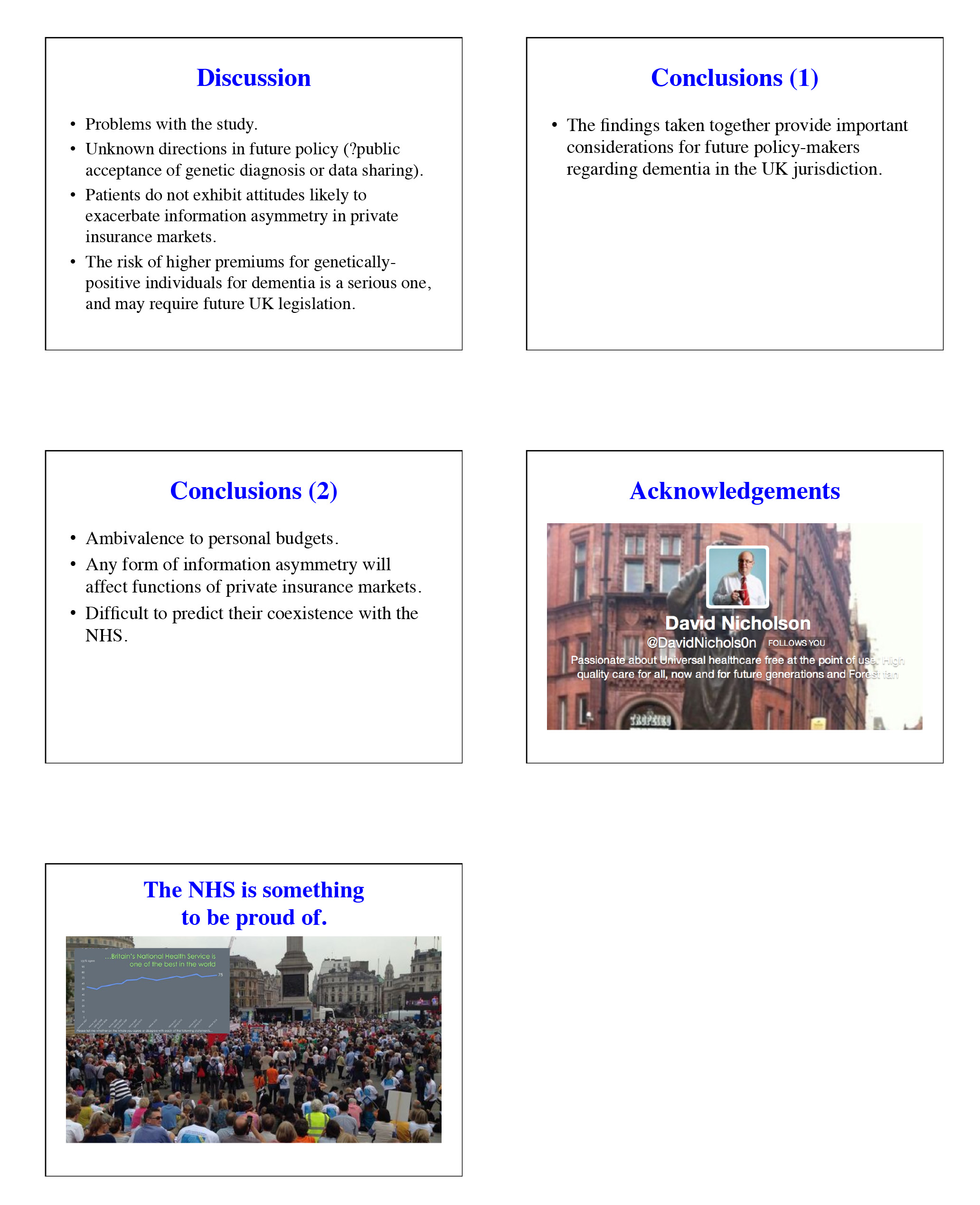
I presented my talk on how dementia healthcare would not be best served by a private insurance system, because of the potential problems of ‘moral hazard’ and genetic discrimination.
This talk was, overall, well received.

I was particularly pleased with the wide-ranging, excellent discussion we had after my talk. Thanks especially to Amy Dalyrymple (@Amy_Dalyrymple), Head of Policy for Alzheimer Scotland, whose contributions in all areas of policy were particularly interesting. The work currently being implemented in Scotland represents a culmination of very high quality inclusive work through a number of different stakeholders.
I was also honoured to present two further research posters, which I had co-authored on the perception and identity of the G8 conference.

And here’s co-author Dr Peter Gordon (@PeterDLROW) proudly in front of our poster too!

Chris Roberts (@mason4233) helped me with the poster session. It was in fact Chris who identified that the phrase “living well with dementia” was not used even once in the top 75 web articles on #G8dementia on Google, in about 44000 words odd.

All around the conference were people whose work is directly relevant to my book: for example Silke Kammer – on the arts and music – and Emma Killick (@RealEmmaKillick) who at the excellent MacIntyre leads on children and adults with learning disabilities and/or autism, but is clearly passionate about people with learning disabilities who later have further unaddressed needs on receiving a diagnosis of dementia.
It was terrific to bump into followers everywhere I went. It was great to meet Julie Christie (@juliechristie1) for the first time, whose work on resilience I am much interested in. It was also lovely to see Anna Tatton (@annatatton1) doing so well.
I am well aware of why the Scottish dementia nursing strategy, some say, has become the ‘envy of the world’. It was a huge privilege to meet in person Janice McAlister (@JaniceMcAlister), who was BJN Nurse of the Year Elderly Care 2013. In addition, I found the presentation by Hugh Masters (@HughCMasters), Associate Chief Nursing Officer for the Scottish Government, interesting for insights as to how England might improve its service too.

I happened to meet in the foyer of the Crowne Plaza on Monday night Ann Pascoe, @A_Carers_Voice, somebody who I have not only liked a lot on Twitter, but whose work on rural ‘dementia-friendly communities’ I have massively respected for some time.


Likewise, it was really nice to catch up with Caroline Bartle (@3SpiritUKNZ), who very kindly once did an infographic of my book ‘Living well with dementia’.

I met in the poster session Prof Mary Marshall to whom the Stirling School in design in dementia owes a huge amount. I owe a huge amount to Prof Marshall too, as the Notting Hill masterclass which I once attended got me first interested in this subject a few years ago (I had a long chat with Prof Marshall there.)

There were not idle tokenistic sops to people living with dementia, and their closest ones, in the whole conference. They were at all times integral to the fabric of the conference.
For example, the seating arrangements in the main Argyll conference suite reflected the special respect given to people with dementia and those closest to them.

The substance of the conference for the most part was of an exceptionally high standard in policy; there was next to no shilling of commercial projects.
The work from Alzheimer Scotland (@alzscot), including, predictably, the work focused on autonomy and dignity, and human rights, was showcased in an impressive way. Their work hangs together as a coherent, forceful narrative of meaningful significance for the Scottish jurisdiction.
It also has clear implications for how England conducts itself south of the border, notably, for example, in a right to timely diagnosis, and a right to timely care and support (including proper coordination of care and support).

In common with Scotland, England is trying to tackle hard the inappropriate use of antipsychotics. Dr Karim Saad (@KarimS3D) gave an excellent talk on this subject, drawing on recent findings from the ALCOVE2 study.

Scotland, in fairness, seems to be having less trouble with its policy than England is.

There was a very good sprinkling of cutting-edge research relevant to all practitioners in the field.

For me, the conference had the feeling of a happy wedding without any of the arguments.
Here are Agnes and Donna.

Whilst originally ‘unkeen’, I ended up having a wonderful time at the “Gala Dinner”. The entertainment – traditional Scottish music and dance – was amazing.



I was able to chat with Agnes and Nancy for some time. What a joy.
Elaine Hunter (@ElaineAHPmh) gave an excellent presentation on the transformative changes which had happened around the workforce in Scotland, including leadership from allied health professionals.

Without doubt, a skilled workforce for the provision of dementia services is essential, not gimmicks.

I consider Helga to be a true friend too. Meeting Helga was akin to being wowed by Lady Gaga.

I had last felt like this when I met Norman McNamara (@norrms) at the Queen Elizabeth II centre in London, Westminster.
I learnt a lot from the all-day workshop on building dementia friendly communities.
Over lunchtime, Joy Watson gave a brilliant ‘Dementia Friends’ (@DementiaFriends) session. I, in fact, was total awe as I am also a ‘Dementia Friends Champion’, and discovered many tips how to run my sessions in future!

This is a brilliant film exhibiting the passion which Joy puts into her Dementia Friends sessions.
Karishma Chandaria (@Karishma1000) chaired this exceptional day’s workshop, called a ‘masterclass’ on dementia friendly communities, which indeed mentioned the code of best practice for dementia friendly communities currently under consultation.

Chris Roberts made time to hand out flyers for membership of the ‘Dementia Alliance International‘, an unique campaigning group run wholly by people living with dementia.

This Conference mapped topics clearly onto people living with dementia and caregivers, for which the organisers of this event must be heavily congratulated.
Next year’s Conference will be in Slovenia. I’ll be there! Bring it on!


Liz McInnes won. Live with it.

The “thrill of the chase” is the layman’s version of a body of marketing research looking at why humans expend a lot of energy in pursuing a goal which they find rewarding, and yet effortful.
Apart from THE major policy, of pulling up the drawbridge on the torrent of immigration we’re apparently experiencing on an industrial scale, many members of the general public are at a loss to identify a single meaningful policy of UKIP. This is particularly the case in UKIP’s submissions on NHS policy, where scattered offerings do not form a coherent picture.
If anything the policy mutterings of UKIP, which do not in any form constitute a policy, go along the lines of a fundamentally corporatist flavour, ‘making the NHS more efficient’ and ‘laying off the excessive staff’, rather than valuing the workforce, for example many nurses who’ve not benefited from a pay rise for many years.
But it could be that the sheer enjoyment of seeking pleasure ultimately from UKIP matters more than what they wish to do on the NHS.
The ‘scattergun’ nature of UKIP decision-making is of course hugely fraudulent. At one moment, UKIP can offer motherhood and apple pie, such as insisting on an exclusion from TTIP, the hated transatlantic trade agreement. It can then do a volte face at any moment, in the hope that potential voters will have selected in their minds the policies most attractive to them even if they subsequently become redacted. UKIP, also, despite wishing to present a united front, can present polar opposite views to voters who have previously voted Labour like Gillian Duffy from those presented to normally Conservative voters in the South West or East of England.
UKIP is an embarrassment politically. All the criticisms have been well rehearsed elsewhere. The criticisms against Liz McInnes, who has spent the last thirty years working in the NHS, have been utter desperation. The BBC, whose credibility is as embarrassing (and some might say offensive) as a Jeremy Clarkson numberplate in Argentina, would much rather focus on how pathetic UKIP insisted on a recount, rather than mentioning what McInnes might offer her constituents in terms of her wealth of experience on valuing staff in the NHS.
But here’s some sanity from James O’Brien.
In a sense we get the media we pay for, but I for one do not wish to pay an enhanced contribution to listen to the bigoted ranting of BBC domestic news commentators as a form of indirect taxation. The output of the Corporation in domestic news has been for some time worse than pathetic.
It has been worse than getting blood out of a stone in trying to get the BBC to cover the diabolical NHS reorganisation which has so far cost a huge amount of waste in terms of redundancy payments and legal fees for competition experts. Labour has next to no hope in getting a fair crack of the whip when it comes to their flagship policy of combining health and care, which many specialists now feel is long overdue in England. There has to be some semblance of fairness in the BBC’s coverage, such that, for example, it can be difficult to incumbents to increase their majority (a meme rapidly disseminated by the CCHQ ably assisting the BBC). Also, the swing away from the current Coalition in the Heywood & Middleton seat was actually more than thirty percent. Labour’s share of the vote did go up in Heywood and Middleton.
The majority for Liz McInnes might constitute a fewer number of people, but overall votes have been declining. The Conservatives which lost both the seats know their leader David Cameron is a dead duck. I do not particularly like Ed Miliband’s leadership style, but I am truly sickened with the way that the Coalition has incessantly lied about how the deficit was caused unilaterally by Gordon Brown. This sheath of lies has given credence to the shambolic lie of economic credibility by the Conservatives – despite a level of debt which is now exploding out of all control.
In a ‘first past the post’ system, Liz McInnes won. Live with it.
For many, the chase of UKIP will be sufficient escapism, until the moment such voters enter a hospital to be treated by an Asian nurse on the minimum wage who will show the patient excellent professionalism anyway. It is impossible to tell the outcome of the general election of 2015, but it might be worth all the political parties not publishing manifestos but statements of their unnegotiable areas.
If it turns out UKIP does not want to negotiate on its flat-tax for the NHS from UKIP manifestos popping through the letterbox, at a time when NHS funding is a national cause for concern, then we know we do not have to buy any extra toilet paper.
On ‘the thrill of the chase':
Labroo A.A. & Nielsen J.H. (2010). Half the thrill is in the chase: Twisted inferences from embodied cognitions and brand evaluation. Journal of Consumer Research. 37(1), 143-158.
My research on #G8dementia and on markets for the @AlzheimerEurope conference 2014
I will be presenting two posters on attitudes amongst the general public towards the ‘G8 dementia’ event as it was then.
I was aghast that out of 75 web articles that the phrase “Living well with dementia” wasn’t used once.
There was a huge bias towards the medical model of dementia. Respondents overwhelmingly felt that the major beneficiaries of that event were large charities, politicians and Pharma, and the people who benefited least were the actual persons living with dementia and caregivers.


I am honoured to give one of the oral presentations.
Information asymmetry between insurance provider and person is a big source of problems. I will showing preliminary data that the two phenomena “moral hazard” and “adverse selection” are likely to be demonstrated in attitudes of people who had received a genetic diagnosis of dementia.
However, I will be raising awareness of the danger of a policy based purely on genetic risk and private insurance; without safeguards against genetic discrimination, such a policy would be likely massively to disadvantage individuals with a higher family-based risk of dementia.


I am hugely grateful to my Twitter followers for taking part in my online surveys.
I am, finally, hugely grateful to the individuals living with dementia and caregivers, as well as other members of the public, who continue to drive the work that I do in dementia.

Developing an enhanced person-centred speech and language service for persons living with PPA dementia
Ravel, composer of ‘Bolero’, who died in 1937, is thought in retrospect to have lived with PPA dementia.
The direction of travel is to develop a person-centred service for people living with dementia and their closest including primary caregivers.
There is still much interest in demonstrating beneficial outcomes, despite the scarcity of resources.
Reports are currently that speech and language input not only can improve communication in people living with PPA, but can improve wellbeing for all involved.
The current NICE guidelines (2011) make it clear that speech and language therapists have a vital role in assessment and management for people with communication difficulties as a result of dementia.
Yesterday, it was very nice to go to the PPA Support Group, this time hosted at UCL off Gower Street.
I was there with my friend Charmaine Hardy whom I had first met on Twitter through Beth Britton.

The “team” is here.

Members of the Queen Square cognitive disorders service are known to me.
Giovanna Mallucci, Jason Warren and Nick Fox were all my Specialist Registrars there – on Prof Martin Rossor’s firm – when I was the equivalent of a FY2 Doctor more than a decade ago. They now are all currently Professors (Jason and Nick at the National Hospital for Neurology and UCL Institute of Neurology).
I had a long chat with Katy Judd, the highly experienced specialist nurse on this firm. I have memories of Katy being completely wonderful. And she was wonderful yesterday. For me, there was a huge deal to catch upon.
The PPA newsletter, containing details of their activities, is here.
Anna Volkmer is a specialist speech and language therapist, from the prestigious South London and the Maudsley NHS Trust.

Anna is on a crusade to go from raising funds for much needed research to developing an innovative, and very much needed, service.
Anna gave a very clear presentation of her research looking at the efficacy of therapy techniques in PPA. A questionnaire survey had revealed that there was much interest in local specialists.
Sessions before the therapy were recorded. Each session was about one hour long.
The aims of therapy for each person and caregiver were different and tailored to the individual.
For example, Anna gave an example of Mr and Mrs G. Mrs G had reported much frustration with her difficulty in communicating, and her perception that Mr G ‘didn’t wish to listen any more’.
Persons with dementia (Frontotemporal Dementia- Primary Progressive Aphasia type) who have been assessed by the St Thomas’ memory clinic team (in the South London and Maudsley NHS Trust) and been referred to a highly specialist speech and language therapist.
The evidence to date had suggested that single word therapies focusing on rehearsal and semantic tasks are most likely to support maintenance of communication for people with PPA (e.g. Jokel, Rochon & Leonard, 2006).
Intervention focused on identifying communication breakdown between the person living with PPA and their communication partner using video-feedback.
One member of the audience described how he had accompanied his wife, living with PPA dementia, to a specialised speech and language unit in Chicago. This unit is apparently world-renowned, known to Anna. The delegate’s experience had been extremely positive.
Anna will be presenting at the British Aphasiology conference later this year, and has a long standing interest in PPA , having written and published on the subject.
Anna’s book on PPA – which she mentioned in the Q&A session – is here.
We then sat around in round table discussions, focused around subtypes of PPA.
Charmaine and I were on the ‘logopenic PPA’ table.
The initial characterisations of a “logopenic” (from Greek, meaning “lack of words”) presentation of PPA described an overall paucity of verbal output, with relative sparing of grammar, phonology, and motor speech,
More specialised information about this type of PPA – meant for a specialist audience – is here.
We discussed various aspects.
One was how it would be a great idea to involve friends or family early on, to help with communication with services from an early stage.
We also discussed how good it was to capture communication intervention techniques on video, so that analysis could also be conducted for non-verbal communication.
We discussed how both hospital and bome settings could be useful for such ‘roll out’ of the service. More research was needed how many sessions there could be, what the time intervals between each session might be, and how early on in the condition the service should take place.
A number of families had had access to speech and language services. The ‘quality’ of such services varied in style and content.
It was observed that speech and language therapists often were keen to administer tests rather than to build up a person-centred or relationships-centred rapport. However, Charmaine Hardy described how her husband had been investigated using an extensive biography approach. Charmaine is on Twitter (@charbhardy), and her profile states indeed her husband, whom she cares for too, lives with PPA dementia.
We talked about how the numbers of people living with PPA dementia were few in number in disparate localities, but how expertise could be pooled for the benefit of persons and families. Our group felt that a coherent PPA information provision, strategy, perhaps organised in both a generic and an individualised person-centred way, could be enormously helpful in service provision.
It was felt that one hour was long, possibly a bit too long provided there was an adequate number of ‘breaks'; but delegates on my table emphasised that each person was different.
References
Jokel, R., Cupit, J., Rochon, E. and Leonard, C. (2009) Relearning lost vocabulary in nonfluent progressive aphasia with MossTalk Words. Aphasiology 23 (2) 175 -191.
National Collaborating Centre for Mental Health commissioned by the Social Care Institute for Excellence National Institute for Health and Clinical Excellence (revised 2011) CG 42.

Is there more to influencing English dementia policy than putting up a poster?
Now is the time to influence the new English dementia strategy. It is critically important that the informed opinions of a diverse group of stakeholders are involved in framing this policy.
As with any strategy document, it will be hard to be in full control of all of the facts and evidence, but I feel it’s very important that the views of people living with dementia are taken into account. This is not just a case of ‘involving’ people living with dementia where possible. It’s a case of allowing people living with dementia to lead in framing the narrative. I am not going to suggest what these topics might be. I think, for people with more advanced dementia, it is going to be important to listen to the views of carers, both unpaid and paid. There is currently a huge policy problem that the needs of carers themselves are unaddressed. Carers need to be better supported in a more structured way.
There has also been a problem rumbling on years: that people who’ve received a diagnosis of dementia are not signposted to appropriate services. While the job description of ‘dementia adviser’ was mooted, I don’t feel this goes nearly enough. The ‘Dementia Challengers’ website, through amazing personal efforts from its one-person designer who has personal experience of this field, offers useful leads on support for making informed choices for living well with dementia. There is no escaping the overwhelming desire, also, to see a system of specialist nurses participating in a care system. Also, we are not making use of the substantial expertise of social work professionals. For issues such as advocacy over capacity and liberty, there are certain people with dementia who need to have equitable access to such resources.
I am a card-carrying signatory that each person living with dementia has an unique experience. I’ve even written a book on it. But it might help people with certain types of dementia to be reassured that there are clinicians with expertise in dementias, and can promote certain support groups (such as the excellent PPA Support Group). We need any diagnosis of dementia to be correct. I too often hear of people being given a diagnosis from somewhere, on the basis of a very scanty work-up. I understand the concerns that too many people are being denied of a correct diagnosis, but we must ensure that this part of the system is adequately resourced. It is possible there will be a breakthrough in drug development for the dementias in the near future. I wish the people working on this well. I am sure that they will not wish resources to be diverted disproportionately into this away from current care, or making it appear that the current living well of people with dementia is less of a priority?
The ‘dementia friendly communities’ policy plank is potentially fruitful. However, I think we should address how we hear a lot from corporates, but not much, in this jurisdiction, from professionals and practitioners who could be useful members of that community. Under the current legislative framework, both in domestic and international law, the rules of equality and human rights apply. These are not issues only for the ivory towers. They have direct relevance to the person with younger onset dementia who finds himself in an unfair dismissal situation. They also have relevance to the person in the badly run care home who feels (s) he is subject to “degrading treatment”. Access to the law has been a real setback for the current Government, as has been access to see your GP. These create the perfect storm for a ‘dementia unfriendly community’.
I am the last person to denigrate the efforts of the vast army of people putting up posters, signing petitions, or handing out leaflets, in the name of ‘dementia awareness’. There is a huge danger that these posters, petitions and leaflets send out a message of ‘mission accomplished’, if there is no follow up? But I am likewise a bit burnt that the fact that #G7dementia and “Prime Minister’s Dementia Challenge” appeared from nowhere, and had the effect of threatening plurality in the dementia third sector. I am concerned about this, and now is the time to make views known to the Baroness Sally Greengross, Chair of the All Party Parliamentary Group, Prof Alistair Burns, the clinical lead for dementia in England, and Prof Martin Rossor, lead for research for dementia for NIHR.
The Tory pitch on the NHS is based on two innocent misrepresentations. They’re huge – like the debt.
A perfect way to annoy nurses is to promise a tax cut for people with the highest incomes ahead of a release from the pay freeze most nurses have endured for the last few years.
I’ve noticed a curious phenomenon when I retweet articles on Twitter. It is not a secret that I am ‘left wing’, whatever that means to the intelligentsia of North London. If I retweet an article from the perspective of how awful this Government, by a left wing ‘seleb’, it won’t be uncommon for people to think ‘nothing to see here, please move on’ . But, if I share something by Fraser Nelson or Isabel Hardman, all hell breaks lose.
Take, for example, the article by Nelson criticising the burgeoning debt burden, published in that well known leftie rag, “The Spectator”. It’s a refreshing honest piece of journalism entitled, “Osborne increases debt more than Labour did over 13 years“. I suspect both Ed Miliband and David Cameron were more prepared for the scenario if Scotland had voted ‘yes’ to independence. Most people I know felt that the story of Ed Miliband’s walk in the park was totally underwhelming. David Cameron, in an outbreak of honesty, meanwhile, let slip that he “resented” the poor. This, for me, represents a clear example the “don’t think of elephants” phenomenon. The harder you try not to think of something, you think of it.
Once, at the Labour Conference held in Liverpool (2011), I asked Jim Naughtie about this famous episode.
Both Naughtie and I burst out laughing. Jim Naughtie is of course not the first person to have dropped a massive clanger. Everyone, including Andrew Neil and Nick Robinson, knows that the pitch by the Tories on tax cuts, when the deficit is being given a second chance to resolve itself, this time by 2018, is a total farce.
I had barely got over the admission that Cameron resented the poor when this suddenly happened.
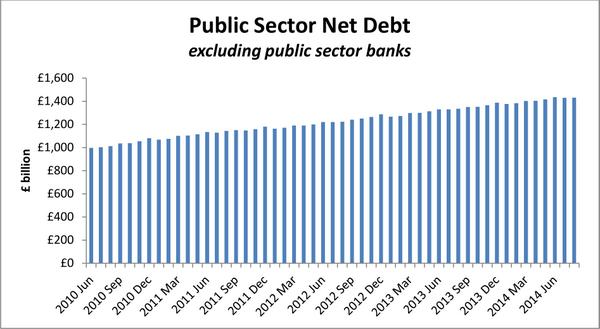
This is a colossal lie, as Sir Andrew Dilnot CBE, Chair of the UK Statistics Authority, has explained to Chris Leslie MP, the Shadow Chief Secretary to the Treasury, in his letter. The critical paragraph of that letter is this.
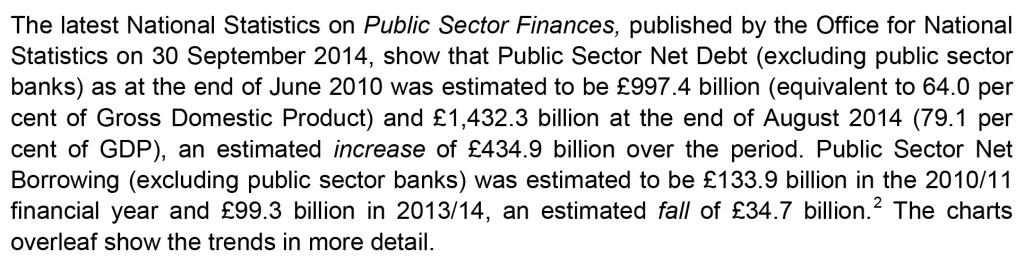
Even a PPE graduate from Oxford can begin to get the gist from this graph helpfully provided by Dilnot.
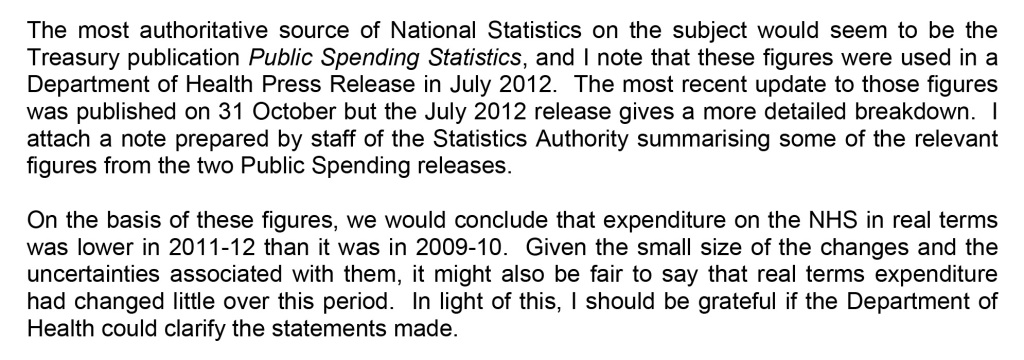
Similarly, because of inflationary pressures – including increasing service demands – on the NHS budget, it is difficult to argue that in real terms there has been an increase in funding of the NHS. That one is also colossal lie, as Sir Andrew Dilnot CBE, Chair of the UK Statistics Authority, has explained to Jeremy Hunt MP, Secretary of State for Health, in his letter here. The critical paragraph of that letter is this.
The Conservative pitch logic is as follows: (1) the Tories are trusted on the economy, (2) Labour is trusted on the NHS, (3) Discredit Labour by repeatedly talking about Mid Staffs despite clearly enduring problems in the lifetime of this period of office, (4) Promise tax cuts in 2018 and ‘more for less’ (by citing examples such as falling crime despite budget cuts). But this logic is based on a surfeit of lies and half truths.
It is a curious phenomenon that crime statistics keep on falling across a number of jurisdictions, fitting very nicely with the argument by libertarians for a smaller state. Furthermore, NHS England has reported on poor recent performance, following the time of the Mid Staffs disaster, in the “Keogh Trusts” during the lifetime of this period of a Conservative-led government. Andy Burnham MP does not repeatedly bring up the example of Harold Shipman, a colossal failure of regulation of general practice which happened instead under the lifetime of a previous Conservative government. It’s been repeatedly reported that Labour ‘do not appear to want to be in power despite being on the brink of power’. But, by that token, the Conservatives are behaving as if they realistically do not expect to be the largest party next May, either. The Conservatives-led Government decided not to take up a golden opportunity of regulating clinical professions, handed on a plate by the English Law Commission, in the last Queen’s Speech of this term. The General Medical Council even signalled their disapproval of this. And, as alluded to above, the debt is exploding while NHS demand continues to increase, leaving a ‘funding gap’ which has been brilliantly discussed by ‘The Health Foundation’. Once again, the patriotic Conservative Party have stuck two fingers up at the best interests of the country by currying favour with their high income (and wealthy) backers, instead. The “jam tomorrow” argument from the Conservatives could be fatal to a frank discussion of the need to integrate health and care from the next Government, whoever it is. But, as my late father often used to remind me, “one lie leads to another”.
Time to turn to the “Black Eyed Peas” for inspiration perhaps.
Sorry, sorry, sorry, sorry
Hey, baby my nose is getting big
I noticed it be growing when I been telling them fibs
Now you say your trust’s getting weaker
Probably coz my lies just started getting deeper
And the reason for my confession is that I learn my lesson.
NHS “credibility gap”
The Conservatives have overtaken Labour for the first time since March 2012 in the latest YouGov/The Sun poll.
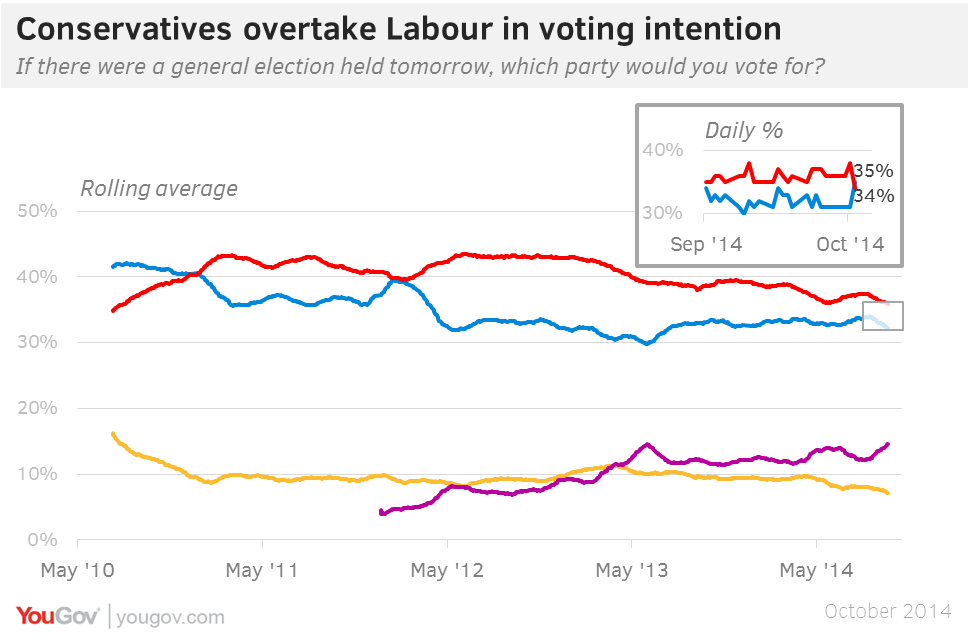
David Cameron has an inherent advantage in the public perception’s of his leadership qualities, in that he is doing the job every day and being seen to do so on the news. Credibility is an important currency. And Labour has already stated ‘the market went too far’ in the NHS. It is not a secret that many parts of the media try to present Ed Miliband in a negative light. Labour is trusted on the NHS, and the Tories are trusted on the economy; so a rationale strategy for the Tories is to make the link between the country’s economy and the NHS. However, real-terms NHS funding has effectively flatlined for a number of years now, not keeping up with the inflation in the system, and debt under this Government has got out of control.
For example, you’re more likely to get a discussion of the ‘bacon butty’ incident than a discussion of how NHS contracts have been aggressively been promoted to the private sector, or how the Health and Social Care Act (2012) locks in the market.

The Prime Minister often blames this lack of coverage on the era of the rolling news, but conversations in the social media have been very productive in exposing events which the BBC would rather not cover. David Cameron’s segment on the NHS was certainly passionate. Cameron must have been distraught at the closure of the Cheyne Centre which he had once fought to keep alive.
But actions speak louder than words. When Cameron claims he will protect the NHS he doesn’t say from whom or what he needs to protect it. He no longer talks about the importance of competition in the NHS and many of the initiatives associated with Andrew Lansley seem to have been quietly forgotten.
If David Cameron had wanted to win the trust of the medical profession, he would not have ambushed them out of nowhere with a ‘top down reorganisation’ which he promised would never happen. The £2.4 bn reorganisation is widely considered to be a tragic waste, when money could have, and should have, been invested in frontline services. The chunk of the speech on the NHS was little consolation to hardworking nurses who’ve witnessed yet another pay freeze, despite the economy’s performance recovering. Nurses, part of the lifeblood of the service, are not immune from the ‘cost of living crisis’, particularly if they are living in London and working in one of the powerhouse teaching hospitals.
A&E targets have been consistently missed during the duration of this period of office by the Conservative Party (and the Liberal Democrat Party).
The current Government need to address what to do about the ‘private finance initiative’. New contracts have been awarded during the lifetime of this Government, and, whilst they were undoubtedly popular under New Labour, their origin is clearly found in the John Major Conservative administration of 1992-1997.
David Cameron, in his conference speech, simply behaved so passionately about the NHS as if the Lewisham debacle had never happened. The current Government even spent money trying to win the case in the Court of Appeal.
GP waiting times have been an unmitigated disaster under this Government. There has been a marked rise in the number of NHS trusts in deficit. Jeremy Hunt is stuck in a time warp. He mentions Mid Staffs at every opportunity. Hunt, completely disingenuously, does not let the failures in culture, quality or management, identified at the CQC, soil his lips. The “Keogh Trusts” were dealt with due to failings which had occurred in the lifetime of and due to this government.
Like the referendum on Europe, promising ‘to protect’ the NHS could be ‘jam tomorrow‘, if the Conservative Party fail to get re-elected. It is either a sign of confidence, or sheer arrogance, that David Cameron and colleagues can hang these uncoated promises in thin air.
The position in an editorial of the Financial Times is clear – and damning:
“But in the bid both to draw a clear dividing line with Labour and reassure the wavering right, they have staked out a fiscal position that is neither sober nor realistic.”
And, hard though it might be to swallow, the Coalition appears to have an ‘edge’ on some key policy areas.
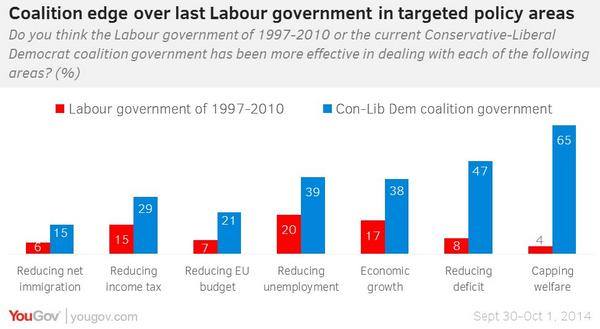
Labour would never have been able to get away with such dodgy promises, with their plans for government being watched like a hawk. With the help of the BBC and other supine media outlets, rather, there will be an inadequate scrutiny of these Conservative plans, which hopefully will be better articulated before the time of the election. As such, it does not matter what Labour promises its voters on the abolition of the purchaser-provider split, whole person care, the private finance initiative, reconfiguration of hospitals, GP waiting times, patient safety, and so on, if voters wish to vote for ‘jam tomorrow’.
The hope is that a Secretary of State for a Labour government would be able to untangle the UK government out of TTIP and CETA trade agreements further giving propulsion to neoliberal forces attacking the NHS. There is a hope that health and care finances will be properly funded in the next Government. All parties have arguably failed to have this conversation with the general public thus far.
Some policies of the current Conservative-led administration are incredibly unpopular with Labour voters: e.g. welfare benefits, NHS privatisation, repeal of the Human Rights Act. The feeling of many, currently, is that, while they do not particularly like this Government, they do not wish to vote for Labour which appears to be offering a diluted form of what the Conservative Party is offering. This is not in any way a indictment of the sterling efforts of the Labour Party Shadow Health Team.
But, before Labour attempts to plug the ‘funding gap’, it will need to resolve any ‘credibility gap’ first.
Whole person care, not misleading campaigning, will be brilliant for dementia

I believe that whole person care, to be introduced by the next Labour government, will be brilliant for bringing together health and care professionals with persons with dementia, and carers and support workers. But we should also be extremely vigilant of dodgy presentation of evidence being used ‘in the name of’ campaigning for my pet subject, dementia, I feel.
We keep on being told that the ageing population is one reason why we can no longer afford the NHS.
The clinical syndrome of dementia, for which advanced age is a risk factor, has therefore taken on a special significance in this context. Health policy gurus and politicians are seemingly having to find increasingly elaborate ways to force their agendas on an unsuspecting public. “The Shock Doctrine: The Rise of Disaster Capitalism” (2007), penned by the Canadian author Naomi Klein, argues that libertarian free market policies have risen to prominence in some developed countries because of a strategy by some political leaders. These leaders deliberately exploit crises to push through controversial exploitative policies while citizens are too emotionally and physically distracted by these crises to mount an effective resistance. Crises are, though, useful instruments for bringing about change.
Within the timescale of this parliamentary term, the Prime Minister’s Dementia Challenge (launched in 2012) has seen a torrent of newspaper headlines with sensational memes. They invariably depict some sort of crisis in projected numbers of people with dementia, and have helped Big Pharma with the task of campaigning for increased funds to find ‘a cure for dementia’. The memes have largely had twangs of crises. For example, ‘dementia is the “next time bomb”‘ was an early news story from 7 May 2012. This messaging has continued consistently since, with the latest popular meme being “soaring numbers diagnosed with dementia“. Indeed, only recently with the arrival of the “Dementia UK (second edition) report” presented in a conference in Central London, a press release was published stating “Alzheimer’s Society calls for action as scale and cost of dementia soars”. But this messaging has caused utter confusion and resentment amongst leading academics and practitioners in dementia. The cumulative effect, instead, of such headlines and articles in public health has been to produce a feeling of ‘moral panic‘. As rightly pointed out by Dr Martin Brunet in “Pulse Magazine”, a well respected commentator on dementia policy in English primary care, recent evidence suggests rather that that the prevalence of dementia in over 65s in 2011 is lower than would have been expected. This “CFAS-II study” from Cambridge, which was published last year in the Lancet, is widely quoted, comprehensively peer-reviewed, and is extremely well known amongst people working in this field.
This is all incredibly self-defeating, as the “Prime Minister Dementia Challenge” was intended to bring greater awareness of the dementias amongst the general public not least to tackle the stigma faced by people living with dementia in their everyday lives. But you have to wonder what the intention of this approach is in the long term? The final report from the Commission on the Future of Health and Social Care in England (“Barker Commission”) was published on 4 September 2014. It discusses “the need for a new settlement for health and social care to provide a simpler pathway through the current maze of entitlements”. Labour intends to introduce ‘whole person care’ in the next parliamentary term, and it could be that this “scorched earth” approach for dementia has served a useful function. “Whole person care” is their new “big idea“. The Barker Commission recommends moving to a single, ring-fenced budget for the NHS and social care, with a single commissioner for local services.
On page 9 of their final report, the ‘ultimate star prize’ is described, the personal budget:
“Personal budgets, and care in hospital and out of it, would be provided from a single, ring-fenced budget. There would be one budget and one commissioner for individuals and their families to deal with, in place of health, social care and, in the case of those aged over 65, the Department for Work and Pensions. Commissioners would be freed to acquire care designed around an individual’s need for support and health care, largely dissolving the current definitions of what is a health need and what is a care requirement.”
And this of course is nothing new: it has been in gestation for quite some time. I myself, in fact, wrote about personal budgets for ‘Our NHS’ in my piece ‘Shop til you drop?’ on 4 September 2013. It is said that Andy Burnham MP, Shadow State of Secretary of Health, “welcomes the Barker Commission“, but one wonders whether he wishes openly to support the more unsavoury parts. Labour is desperately keen to introduce its policy changes on integrated care, without them being seen as another “top down reorganisation”. Any public resistance to their flagship policy will be political dynamite. Labour is instead currently campaigning on an anti-marketisation and anti-privatisation slate, and has pledged to repeal the highly toxic Health and Social Care Act (2012) (“the Act”).
One significant part of this repeal will be the abolition of “section 75″ and its associated regulations, which introduced competitive tendering in commissioning as the default option for NHS procurement. Nevertheless significant faultines in policy, described elegantly by Prof Calum Paton in his pamphlet “At what cost? Paying the price for the market in the English NHS” for the Centre for Health and Policy Interest (February 2013), still exist. They also are at danger of persisting, even if Labour triumphantly repeals the Act. There is a danger that unless these other pro-marketisation strands are addressed first, such as the purchaser-provider split, the “whole person care” policy will become engulfed in an intensely neoliberal direction. The counterfoil to this from Labour would presumably be that whole person care does not require a market in the first place. For this, clearly, Labour must not inflict personal budgets. A further big concern of mine is simple: not only will current scientific research into dementia have been completely misrepresented in the popular press, but also the field of dementia will be used to provide the raison d’être for yet another upheaval in service change.
And that upheaval could witness yet another change from the founding principles of the NHS. It could also be one too many.
The “disastrous” performance of this Tory-led government was not accidental. It was entirely deliberate.

One conversation I once had with Jos Bell (twitter here), an incredibly productive campaigner and chair for the independent Socialist Health Association London division, had much more of a profound impact than I thought at the time.
I simply remarked that the Conservative-led government had been ‘disastrous’.
Jos disagreed. She pointed out that the term of office had gone extremely successfully for the few who’ve made shedloads of money through private equity and hedge funds.
A massive assumption we’re all prone to make, some more than others, is that the political class largely represent us and our interests.
The number of ‘lost votes’ is the reminder to all of us of how disconnected parliamentary politics have become with our needs and concerns.
There are, of course, some truly outstanding MPs, however.
Another realisation for many, almost a right of passage, is the “lightbulb moment” that some leading ‘independent’ health and care think tanks have not been offering useful reliable impartial advice after all.
The performance of some on the issue of competition, a shoo-horn for neoliberal markets, against the wishes of many professionals, is a testament to them.
Dodgy advice was used to prop up the business case for the Health and Social Care Act (2012), and it is going to take a long time to unwind from this.
I know of the misery that the ‘welfare reforms’ have had on the morbidity and mortality of disabled citizens. This does not prevent ATOS from fulfilling a lucrative contract, which was made under the last Government (Labour).
There are accusations and counter-accusations of the effects of injection of private capital, the private finance initiative, which many hope will be addressed properly by the incoming government next year. City financiers and law firms continue to benefit from this sustained policy which has reaped havoc on various ‘local economies’ of the NHS.
The sale of Royal Mail, and various other projects, into the private sector at an undervalue (it is alleged) clearly has not been to the best benefit of the taxpayer. But again many in the City, some alleged to be close to the current Government, have benefited personally (it is alleged).
Through the prism of me and my friends, this Conservative-led Government has been ‘disastrous’. But they’ve actually achieved a lot for themselves in the last few years in the tenuous argument of ‘austerity’.
The buzzword for George Osborne was ‘choice’, and you could hear a pin drop literally at George Osborne’s reassurance in his speech yesterday, “We’re all in it together”.
I simply can’t agree with political commentators who wish to pollute the discussion with their meme that ‘Labour do not wish like a party who wish to govern.”
Many grassroots activists in Labour are desperate to sort out the mess the country finds itself in.
They certainly detest the idea of a Tory-UKIP coalition.
The repeal of the Health and Social Care Act (2012) will be in the first Queen’s Speech of an incoming Labour government.
This Act of parliament turbo-boosted the aggressive pimping of NHS contracts into private sector providers. Correct – another set of beneficiaries from this government, led by the Conservatives but the lifeblood of which is currently provided by the Liberal Democrats.
In many ways, the next period of office is a ‘poisoned chalice’ once again, with debt in the last four years 4 x as much as the debt amassed by Labour in 13 years.
But, to repeat David Cameron, “we can’t go on like this”.
And the goalposts keep on moving.
An identifiable threat still remains having a means-tested social care service bolted onto the ‘universal’ health system, like a badly soldered “lemon car”.
A threat, less visible on the event horizon, is the corporatisation of general practice in the English jurisdiction.
I suspect that, despite the noise produced by UKIP and LibDems, the NHA Party will fail to make inroads in seats in the actual election. This will be of great sadness to me, despite the fact I wish all Labour candidates very well, as they are clearly campaigning on many relevant issues.
I feel that Labour will win the next general election. But I am terrified that, like the aftermath of 1997, it will be another missed opportunity for us.
