Home » Posts tagged 'NHS' (Page 3)
Tag Archives: NHS
The Tory pitch on the NHS is based on two innocent misrepresentations. They’re huge – like the debt.
A perfect way to annoy nurses is to promise a tax cut for people with the highest incomes ahead of a release from the pay freeze most nurses have endured for the last few years.
I’ve noticed a curious phenomenon when I retweet articles on Twitter. It is not a secret that I am ‘left wing’, whatever that means to the intelligentsia of North London. If I retweet an article from the perspective of how awful this Government, by a left wing ‘seleb’, it won’t be uncommon for people to think ‘nothing to see here, please move on’ . But, if I share something by Fraser Nelson or Isabel Hardman, all hell breaks lose.
Take, for example, the article by Nelson criticising the burgeoning debt burden, published in that well known leftie rag, “The Spectator”. It’s a refreshing honest piece of journalism entitled, “Osborne increases debt more than Labour did over 13 years“. I suspect both Ed Miliband and David Cameron were more prepared for the scenario if Scotland had voted ‘yes’ to independence. Most people I know felt that the story of Ed Miliband’s walk in the park was totally underwhelming. David Cameron, in an outbreak of honesty, meanwhile, let slip that he “resented” the poor. This, for me, represents a clear example the “don’t think of elephants” phenomenon. The harder you try not to think of something, you think of it.
Once, at the Labour Conference held in Liverpool (2011), I asked Jim Naughtie about this famous episode.
Both Naughtie and I burst out laughing. Jim Naughtie is of course not the first person to have dropped a massive clanger. Everyone, including Andrew Neil and Nick Robinson, knows that the pitch by the Tories on tax cuts, when the deficit is being given a second chance to resolve itself, this time by 2018, is a total farce.
I had barely got over the admission that Cameron resented the poor when this suddenly happened.
This is a colossal lie, as Sir Andrew Dilnot CBE, Chair of the UK Statistics Authority, has explained to Chris Leslie MP, the Shadow Chief Secretary to the Treasury, in his letter. The critical paragraph of that letter is this.
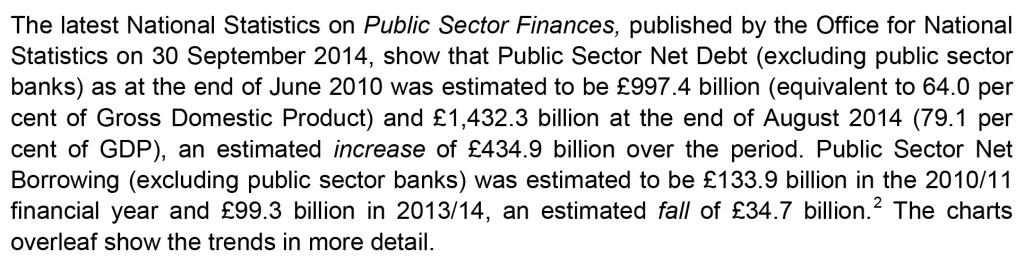
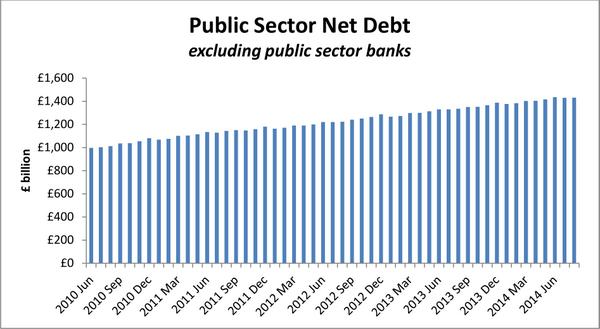
Even a PPE graduate from Oxford can begin to get the gist from this graph helpfully provided by Dilnot.
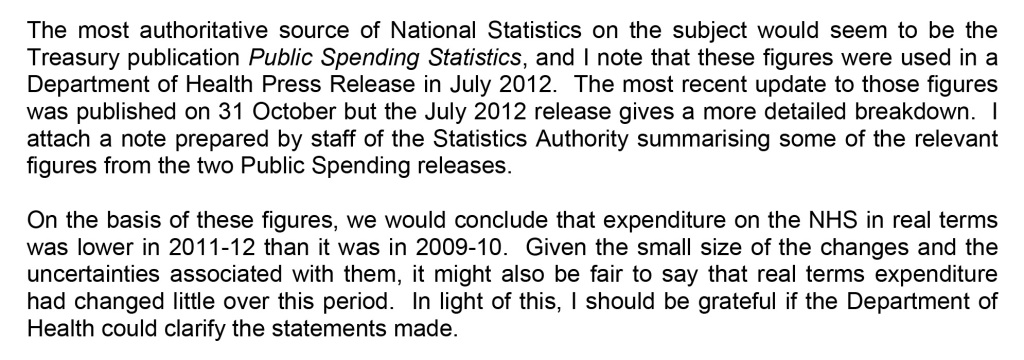
Similarly, because of inflationary pressures – including increasing service demands – on the NHS budget, it is difficult to argue that in real terms there has been an increase in funding of the NHS. That one is also colossal lie, as Sir Andrew Dilnot CBE, Chair of the UK Statistics Authority, has explained to Jeremy Hunt MP, Secretary of State for Health, in his letter here. The critical paragraph of that letter is this.
The Conservative pitch logic is as follows: (1) the Tories are trusted on the economy, (2) Labour is trusted on the NHS, (3) Discredit Labour by repeatedly talking about Mid Staffs despite clearly enduring problems in the lifetime of this period of office, (4) Promise tax cuts in 2018 and ‘more for less’ (by citing examples such as falling crime despite budget cuts). But this logic is based on a surfeit of lies and half truths.
It is a curious phenomenon that crime statistics keep on falling across a number of jurisdictions, fitting very nicely with the argument by libertarians for a smaller state. Furthermore, NHS England has reported on poor recent performance, following the time of the Mid Staffs disaster, in the “Keogh Trusts” during the lifetime of this period of a Conservative-led government. Andy Burnham MP does not repeatedly bring up the example of Harold Shipman, a colossal failure of regulation of general practice which happened instead under the lifetime of a previous Conservative government. It’s been repeatedly reported that Labour ‘do not appear to want to be in power despite being on the brink of power’. But, by that token, the Conservatives are behaving as if they realistically do not expect to be the largest party next May, either. The Conservatives-led Government decided not to take up a golden opportunity of regulating clinical professions, handed on a plate by the English Law Commission, in the last Queen’s Speech of this term. The General Medical Council even signalled their disapproval of this. And, as alluded to above, the debt is exploding while NHS demand continues to increase, leaving a ‘funding gap’ which has been brilliantly discussed by ‘The Health Foundation’. Once again, the patriotic Conservative Party have stuck two fingers up at the best interests of the country by currying favour with their high income (and wealthy) backers, instead. The “jam tomorrow” argument from the Conservatives could be fatal to a frank discussion of the need to integrate health and care from the next Government, whoever it is. But, as my late father often used to remind me, “one lie leads to another”.
Time to turn to the “Black Eyed Peas” for inspiration perhaps.
Sorry, sorry, sorry, sorry
Hey, baby my nose is getting big
I noticed it be growing when I been telling them fibs
Now you say your trust’s getting weaker
Probably coz my lies just started getting deeper
And the reason for my confession is that I learn my lesson.
Burnham announces plans to implement a National Health and Care Service over ten years

The Shadow of Secretary of State for Health, Andy Burnham MP, says that he has tried to produce an answer ‘which people can believe in, and which people can buy into’.
This is particularly timely, as it is well known that Labour intend to make the NHS a major general election issue next year.
The Conservatives and Liberal Democrats are now deeply unpopular over their management of the NHS, as evidenced, for example, by the campaigners who converged on Trafalgar Square recently on behalf of the “Darlo Mums”.
Over successive governments and most recently, the finances of social care have suffered massively.
Speaking at a fringe event for the Fabian Society in Manchester yesterday, Burnham felt that things are not satisfactory as the response to an ageing society has been through a medical model.
Burnham’s problem is that he is about to be bequeathed a fragmented illness service, not a national health service; and that the system is patient-focused on ill people not person-focused on people through health and illness. Burnham feels that focusing on people will enable a greater focus on friends and families too.
Burnham feels that the “ever-increasing hospitalisation” of an ill ageing population will not work, and that hospitals are becoming increasingly dysfunction all the year round due to a social care system which has been malnourished over successive governments.
“This failure piles pressure on the acute system”.
Burnham further adds that people “are battling in caring for people with complex needs”, and that “these silos are not ones which can afford any more”.
This policy is anticipated to bring in housing, education, and leisure strands in due course.
But the urgency for Burnham is to deal with people having to avoid recounting their personal stories repeatedly to different people; and that professionals are often making clinical decisions on the basis of incomplete information.
The intention is, ultimately, to bring together systems for physical health, mental health and care. Sir John Oldham had earlier in the fringe event observed that the general public can have a poor understanding of the word “social” in relation to ‘social care’.
Burnham intends to set out a ten year plan for a whole person care, fully accepting the findings of the Oldham Commission, and which “endorses” the findings of the Barker Commission from the King’s Fund.
Such a plan will be strongly attractive to those vociferous critics, such as Sir David Nicholson the immediate predecessor of Simon Stevens as the CEO of NHS England, that health policy has traditionally been adopted on the basis of the electoral cycle.
This system will be a “National Health and Care Service”, which will realign an activity-based tariff for episodes of illness to produce a single ‘year of care’ budget for each person covering his or her physical, mental or social meeds. This, Burnham feels, will support prevention and wellbeing.
At first the idea was to have a pooled integrated budget across health and care, but, in the subsequent question/answer session, Burnham made extremely clear that he was mindful of the need to move away from privatised fragmented care; and to move away from compulsory personal health budgets which had not been proven to work well.
Burnham, instead, signposted plans to be announced later this week that he would instead advocate a general ‘rights based approach’, where citizens could be given realistic expectations of the development of personal care plans according to their needs.
Burnham emphasised that he remained unconvinced that personal budgets were the sole instrument that could achieve this aim.
He is of course extremely mindful of the public’s overwhelming lack of appetite for the marketisation, outsourcing or privatisation of the NHS.
As an example of ‘market failure’, Burnham cites how councils in their wish to compete to keep council tax bills low end up failing on high quality care.
Interestingly, he also feels that this plan has the potential to be ‘radical’, allowing people can be supported to care, enabling full personalisation.
Such a system will involve a “care coordinator”. This has already been mooted publicly very recently by the Shadow Minister for Care, Liz Kendall MP, as a point of contact for the elderly to navigate themselves through the maze of information including care information.
Such a rôle, it is felt, might not be for general practitioners, but possibly for specialist nurses. The voluntary sector, such as Dementia(UK) which developed the innovative specialist “Admiral” nurses programme, might be well placed to act as these coordinators.
In the alternative, social care practitioners might be particularly well suited for a care coordination rôle for people with dementia, as they command expertise in decision-making and capacity. Social care practitioner leads in this context would help to overcome a barrier to cultural integration, furthermore; this is especially important given the often perceived hierarchies of the professions involved.
“Carers will no longer be peripheral to the system, but central to the development of a care plan.”
This plan would be established over a ten year period to integrate services around the individual, not through a sudden ‘top down reorganisation’.
A potent steer for this would come from the Health and Wellbeing Boards.
It is expected that the Labour Party will also use their party conference this year in Manchester to emphasise its intention to repeal the Health and Social Care Act (2012) in the first Queen’s Speech of an incoming government in 2015.
Jackie Ashley, Sir John Oldham, who chaired the Oldham Commission, and Kate Barker, who chaired the Barker Commission of the King’s Fund, panel members yesterday evening, all agreed that it was unlikely that politicians would openly wish to pledge to raise taxes for health and care. The way in which this had been politically debated in the 2010 UK general election, it is felt, had been unimpressive.
Nonetheless, the general sentiment was that the public would appreciate an open discussion of how sustainable funding for health and care systems could be achieved.
Jackie Ashley, who writes for the Guardian, explained the difficulties in the news media approaching this topic, when headlines consistently remained fixated on crises in the NHS.
The general policy trend has been try to support people who wish to live and to be cared for at home independently.
However, Ashley alluded to the need to avoid a narrative that hospitals are necessarily bad and non-hospitals are necessarily good.
It is felt that when the NHS was originally set up it was not designed to be catering for people in their 90s with their multiple clinical care needs.
Nonetheless, Oldham urged the need for NHS England to move away from the needs of hospitals, and urged, as an example, a greater number of representatives from local authorities (currently involved in commissioning social care) on NHS England.
For a condition such as one of the dementias, citizens have the perception of their care needs being financially punished through the need to pay for care; this is, for example, in contrast to a condition such as one of the cancers, where the NHS appears willing to pay for expensive medications often.
Equity, equality, fairness and justice will therefore be key aims of this new National Health and Care Service.
“These are some silos which we desperately must get rid of”, exhorts Burnham passionately.
Finally, Burnham wishes this to be a plan for the National Health and Care Service fit for purpose for a 21st century, synchronising at last the wishes of the public, professionals and politicians.
The Scottish referendum was, predictably, a disaster for Westminster’s historic view of the NHS

Scotland’s decision on its future, everyone knows, was as much a referendum on the past performance of the Westminster governments to date. In human resources, a guiding principle is that a candidate is likely to behave in future as he or she has down in the past, unless there are exceptional circumstances.
Andy Burnham MP was quoted himself many times as warning against the creeping privatisation of the National Health Service in England. While the ‘No’ campaign consistently explained the Westminster government had protected the NHS budget, it was widely known that the statistical authority has rebuked David Cameron for stating incorrectly that NHS spending has increased in recent years.
The ‘no’ campaign nonetheless did put up a valiant fight, with exceptional campaigners Clare Lally and Johanna Baxter, for example. These campaigners, against some formidable abuse, tried to explain why the leverage of being united with England was especially important for Scotland to withstand future economic pressures resiliently, and why it was in fact intensely patriotic to keep Scotland as part of the United Kingdom.
Whatever Andy Burnham promises as the Shadow Secretary of State for Health, it is a fact that the efficiency savings in the NHS and the private finance initiative loan repayments have put enormous pressure on the operations on the service. Managers, who all too often behave in a divorced way to frontline clinicians, do not appear easily accountable for poor staff shortages impacting on clinical patient safety.
The efficiency savings operate on the assumptions that nobody wants to pay any tax to fund the NHS properly, and that the economy is not growing. Labour, whilst rightly drawing attention to how the ‘cost of living crisis’ is damaging the wellbeing of people, cannot easily claim that people are so unwilling to fund the NHS properly. Nor can they easily dismiss that the GDP of the UK might now be improving.
The resulting democratic deficit which has happened in Scotland is therefore an extreme serious one. Whilst it is the perception that New Labour and the Conservatives, at least, have paid more attention to their friends in the City of London rather than their workforce, there has been a lack of trust between voters and the mainstream parties. Today, UNITE decided it would go on strike. Labour has not yet given a clear indication of what intends to do about the private finance initiative.
In a way, the decision for Scotland was in fact very simple. It was about making a firm decision on separating from England, rather than subjecting Scotland to another eighteen years festering with Devo Max prior to another vote. But of course, we all know it was far from simple. Whatever one’s views about Johanna Lamont or Alex Salmond, the answer of many voters is a response to David Cameron’s original question, “We can’t go on like this.” Gordon Brown’s uttered the famous words yesterday, “And proud that with the powers of the Parliament we can guarantee that the National Health Service will be in public hands, universal, free at the point of need, as long and as ever as the people of Scotland want it.”
But will the general public believe Westminster any more?
It is clear that the Westminster governments totally underestimated the passion and drive of the ‘Yes’ campaign. If Gandhi had been subject to rolling news, one wonders how the Indian independence would have turned out. But the gut feeling of many ‘Yes’ campaigners was a blatant abreaction to lies and misinformation by people who were supposed to be acting in their best interests.
Predictably, Big Business were all mobilised to depict the #iScotApocalypse #ProjectFear scenario. Unfortunately, it had Westminster’s fingerprints all over it. The Westminster delegates, including Danny Alexander, George Osborne and David Cameron, looked utterly unconvincing in raising a populist case. And the media as per usual totally screwed up the reality of the economic contribution to the rest of the UK, which is quite a formidable one albeit not as strong as London and the South East.
When Margaret Thatcher reached Downing Street in 1979, she said, “And I would just like to remember some words of St. Francis of Assisi which I think are really just particularly apt at the moment. ‘Where there is discord, may we bring harmony. Where there is error, may we bring truth. Where there is doubt, may we bring faith. And where there is despair, may we bring hope’ … and to all the British people—howsoever they voted—may I say this. Now that the Election is over, may we get together and strive to serve and strengthen the country of which we’re so proud to be a part.”
England currently is deeply divided, between rich and poor, between employed and unemployed, and, as a result of the ‘welfare reforms’, between able bodied and physically disabled. September 18th was a chance for Scotland to have a ‘clean break’.
The question is, however, will Scotland go Alex Salmond’s way?
What is Clive telling Andy and does Andy need to listen?
I had the pleasure of going to two events at the weekend. On Saturday, I went to the event at Trafalgar Square for the #999CallfortheNHS #DarloMums arriving after their 300 mile-long walk across the country. Thanks to Jos Bell for inviting me, for which I am deeply grateful. The following day, I went to the National Health Action Party for their Annual Conference in Conway Hall, Red Lion Square, London. I enjoyed that afternoon as well.
The National Health Action Party are putting up parliamentary candidates for the General Election 2015, the vast majority of whom are known friends of mine. I am proud of them, and I really do wish them well. They give people a chance to vote for a party which has an established position against privatisation. The party is led by Dr Clive Peedell and Dr Richard Taylor, and they clearly have a strong position against privatisation of the NHS, and various manifestations of the NHS market including the private finance initiative and the EU-US free trade treaty.
They have made substantial progress this year. One of their challenges as a new party is having people recognise what they stand for, and this is clearly going to be hampered if the mainstream media do not give them a fair opportunity. Nonetheless, there have been noteworthy successes, such as appearances on Sky, LBC and “The Evening Standard”. And there is no doubt about the intensity of emotion in support of the National Health Service. A challenge is funding, and, whilst the party is in fact running a healthy surplus, having more funds will allow them to present a greater number of election candidates; an inevitably costly process.
It was very nice to chat with Dr Clive Peedell both before and after the event. I understand the misgivings about previous Labour policy, and indeed whether Labour can be said to be doing enough on abolishing the market. There are clearly strands of Labour policy which made room for private providers, but likewise it is also the case that the Lewisham judgment in the high court clearly stated that legislation under the present Government had been a clear departure from previous law under the last Labour government.
So it is not a surprise that many of the key pledges of the National Health Action Party will also be of concerns of some Labour voters with a keen interest in NHS policy. A slide of these were presented yesterday.

It is easy to underestimate the pernicious effect that the private finance initiative has had. Whilst it may have had good intentions of improving the infrastructure of the health service, one cannot deny how ‘cost savings’ allegedly in places have led to dangerous threats to patient safety, such as hospital infection, or in actual staffing numbers cannot be tolerated, not least by the general public and the clinical regulators. Whilst not all the problems can be held responsible from that desk behind Whitehall, the removal of the Secretary of State’s duty for the NHS is clearly symbolic. And Clive Efford MP perhaps would do well to learn from Peter Roderick, a public interest lawyer by training, and Prof Allyson Pollock, a world respected expert in public health.
Andy Burnham MP undoubtedly has a lot of goodwill too, and it is now likely that Labour will be the largest party of an incoming government at least under the leadership of Ed Miliband; they could win an outright majority, also, if the policy mix is right. Burnham has explicitly stated his desire to repeal the Health and Social Care Act (2012), but it is clear that a huge amount of work will be necessary to clear up the regimes for Trusts in financial distress, and for getting rid of competitive tendering tendering as being the default option.
It is not easy to let the Liberal Democrats ‘off the hook’, though it is clear that there are MPs such as Andrew George who have been strongly critical of the NHS reforms and indeed the “Bedroom Tax”. It is undoubtedly clear that the National Health Action Party will not be the main party forming Government next year, but they have never had aspirations to. They do allow the main political parties to be held to account, and their supporters are enthusiastic and well informed.
One of the critical tests for Labour will be letting go of the more neoliberal twangs to its policy, and to represent those people who had gone on the modern day NHS Jarrow march. It is not simply good enough to riposte every attack with ‘yeah but the NHS is free at the point of need’. There are genuine problems with solidarity, equity, justice, and comprehensiveness in current ethos, and a whole raft of problems which have arisen from indisputable marketisation and privatisation of the National Health Service.
It would be a mistake for Labour to discount the National Health Action Party as an insignificant blot on the landscape, when many of their concerns should be genuine concerns for Labour too. Andy Burnham is a highly skilled politician, but he has a strong vested interest in making a Labour government work properly for the NHS, and that might include for example not holding its staff to ransom yet again on a pay freeze. Andy as critical part of a Labour Government might wish to find a way to fund the NHS properly, especially since the economy is apparently making a recovery?
Whilst the present Coalition Government may seem ‘catastrophic’ to many of us, it has in fact been a blazing success for the Coalition parties. They have been able to do a lot of damage in the name of ‘austerity’. The evidence base for such policies is extremely poor, and indeed there is quite a lot of evidence that the welfare benefit ‘reforms’ have done a lot of damage to the mental health of citizens particularly those with disabilities.
Dr Clive Peedell has much to tell Andy, and – for what it’s worth – I do believe Andy needs to listen. And I have every confidence he will.

Why the ‘999 March of the NHS’ is an important statement of democracy

There is no doubt that one should fight your battles to the hilt, but it is equally true that you should pick the right battles first. Two major battles to be had are whether NHS contracts should be aggressively pimped to the private sector, and whether the NHS should be up for sale to the highest international bidder. That is not to say that other battles are not important, but fighting these battles, I feel, will be able to tell us the future direction of travel of Labour. It’s well known that the political heart of Labour is possibly social democratic, but I feel that the ‘999 March for the NHS’ shows noteworthy twangs of democratic socialism, which has rather disparagingly been referred to as ‘left-wing populism’ previously elsewhere.
Getting Labour embroiled in a turf war over semantics I reckon is an infertile ground. The history of Labour and state ownership has long been a complicated one, as evidenced by previous Labour governments under Hugh Gaitskell and Tony Blair. When it was first established, the NHS was set up on the basis of social solidarity – everyone contributed to the cost of providing the NHS through taxes, and in return healthcare was provided by the state and available for those who needed it, when they needed it. This feeling of solidarity is indeed embed in the ‘999 Call for the NHS’.
The situation in 2014 is that rail fares are rising again, faster than average earnings. Whilst perhaps somewhat over egged, there is a genuine ‘cost of living crisis’ in England, with bills far outstripping real term wages. Employment for some is a very flimsy construct, being held together by a zero term contract. But it is true that, as under previous administrations, inequality is a problem in policy, and taxpayer subsidies are being diverted towards company profits and shareholders. Far from a smaller state, we have ended up with an unaccountable outsourced state. We have had the highest fares in Europe with profits extracted to pay shareholder dividends. In 2012/13 Northern Rail, Transpennine Express and Virgin alone paid almost £100m in dividends to shareholders after receiving over £1bn in public subsidy. Evidence shows that about £1bn per year is wasted due to privatisation, and if saved, this could fund an 18% cut in fares.
Why should the ‘People’s March for the NHS’ become so popular? Is it another example of “left-wing populism”? Left-wing populism is supposed to be a political ideology which combines left-wing politics and populist rhetoric and themes. Such a narrative normally consists of anti-elitist sentiments, opposition to the system and speaking for the “common people”, including themes of anti-capitalism, social justice, pacifism and anti-globalisation, whereas class society ideology or socialist theory is not as important as it is to traditional left-wing parties. The turbo-boosting of the privatisation of the NHS and the decimation of legal aid in England have therefore been good reasons for left-wing populism to gain momentum.
Robert Peston once famously asked, “Who runs Britain?” And looking at the recent elections to the House of Lords, one wonders how certain people get to such elevated heights of power. Meanwhile, Democratic socialists believe that both the economy and society should be run democratically—to meet public needs, not to make profits for a few. For a good such as water, where there is nothing to tell the difference between one brand of water and the next, it is hard to see how a privatised utility system is of benefit other than to corporate shareholders whether here or abroad. Democratic socialists do not want to create an all-powerful government bureaucracy, but likewise they do not want big corporate bureaucracies to control our society either. And some of the private providers in running public services, whether NHS, security, or probation, or otherwise, have been a disaster.
People often criticise Labour of having lost its roots. Indeed, it is hard to see how the most loyal Tony Blair critic should think of the Jarrow March as particularly Blairite? Jarrow is a small industrial town near to the southern mouth of the River Tyne, situated six miles east of the city of Newcastle. Despite the efforts of industrialist and Member of Parliament Sir John Jarvis, by September 1935, Jarrow had lost most of its heavy industry, and unemployment stood at 72.9%. The march was to find jobs to support Jarrow men and their families. It was also a bid for respect and recognition, not only for the people of Jarrow, but for others in a similar situation all over the country. The marchers had no resources other than their own determination, and some good boots supplied by the public. The irony about keeping wages stagnant in the NHS is that this is at a time when the country’s economy is supposedly improving, and when demand for the NHS is outstripping supply.
The People’s March for the NHS will arrive at its destination in London this Saturday, 6 September 2014, when campaigners will be joined by thousands of demonstrators for the final leg from Red Lion Square to Westminster. Started by a group of working mums from Darlington committed to stopping the privatisation of the NHS, the ‘999 Call for the NHS’ march left Jarrow on 16 August and has been winding down the country for the last three weeks following the route of the original Jarrow Crusade. The Chair of the London Socialist Health Association (@SocHealthLondon), Jos Bell (@jos21) has helped with some of the organisation over The final leg of the march, which will start at 2.30pm from Red Lion Square, Holborn, in London, with campaigners gathering from 1.45pm. There will be a rally in Trafalgar Square form 3.30pm with speakers including columnist and author Owen Jones. Further details can be found here.
But I feel that this march is much more than a publicity stunt or an item of ‘left populism’. It for me goes to the heart of a social democracy malaise gone wrong. It is indeed true that many northern European countries enjoy tremendous prosperity and relative economic equality as a result of policies pursued by social democratic parties. Social democratic parties supported strong labor movements that became central players in economic decision-making.
But globalisation of neoliberalism can be seen as a threat as well as an opportunity. With the globalisation of capitalism, the old social democratic model becomes ever harder to maintain. Stiff competition from low-wage labour markets in developing countries and the constant fear that industry will move to avoid taxes and strong labour regulations has diminished (but not eliminated) the ability of nations to launch necessary economic reform on their own. The idea of the NHS participating in this race to the bottom, where radiology opinions are outsourced in a disruptive manner to a foreign jurisdiction which we cannot easily regulate, strikes many people with fear.
Many have long felt that social democratic reform must now happen at the international level. Multinational corporations must be brought under democratic controls, and workers’ organising efforts must reach across borders. The European Commission is currently involved in negotiating a free trade arrangement of unprecedented scale between the US and European Union (EU). This is the Transatlantic Trade and Investment Partnership (or TTIP). The process is also undemocratic as the substance of on-going negotiations is largely kept from our MPs, MEPs, as well as the public. Once the treaty is signed by negotiators, the UK parliament, like other EU member states, will only be able to vote to accept or reject the treaty as a whole: they will not be able to amend it in any way.
Many believe that one of the biggest prizes of the agreement for transnationals will be the NHS. The Health and Social Care Act (2012) and the regulations for implementing it (Section 75) have changed the fundamental nature of the NHS. By fragmenting the NHS, opening it up to competition law and turning the NHS into a market in which private companies can compete for NHS funding for patient services, the Health and Social Care Act contains a toxic tool which can put profit before people, and lead to the piecemeal destruction of the NHS. Labour has pledged to repeal the Health and Social Care Act (2012), which of course they must do to avert the biggest sale of the century.







Politicians need to wipe the blood from their hands from liberalising the NHS

All the main political parties in England have “blood on their hands”, and we’re never going to get anywhere near the Chilcot Inquiry to sort out how it happened. The ‘weapons of mass destruction’ unleashed by corporate agents seeded everywhere in think tanks, media and politics have gone out of the way on a tirade of abuse against workers in the public sector. There are so many nexuses which have become uncoupled, that the NHS and social care systems no longer have anything like a situation approaching credibility.
Top CEOs in the NHS in England can still receive generous renumeration, even if their patient records are worse than the Black Hole of Calcutta. Even if multinational corporates do not perform adequately on a contract, the NHS does not have the legal know-how to ‘performance manage’ these contracts, and will not wish to spend the money. The NHS is scared of imposing any penalties, because of the powerful lawyers of multinational corporates. Above all, in addition to ‘patient safety’, that other secret weapon is used, namely ‘continuity of care’. Continuity of care is another chameleon wheeled out in a guise which suits its purpose at any one time.
Whilst the Blairites continue to espouse that it does not matter who is a Doctor at any one time, corporates are equally happy to use the legal stun gun of saying continuity of care will suffer if contracts are disrupted.One of the lessons from social care should have been that there are pockets of extremely poor social care, fragmented and expensive. As the next Government wishes to integrate care, with or without whole person care, one suspects that merging a means-tested system with one which isn’t will not be “no problem” as some senior health commentators have pretended. The idea that a self-directed budget where you pay for your service is “free at the point of use” is twisting the truth beyond all banality.
And these privatised contracts are neither accidental or insubstantial. One is a 10-year contract worth £1.2 billion for providing cancer services in Staffordshire, and there is also a five-year contract worth £800 million for the care of older people in Cambridge to last for the duration of the next Parliament. Both Labour and the Conservatives set in the present and previous administrations set the mood music for this, and politicians need to wipe the blood from their hands of the stains of neoliberalism. The new Jerusalem offered by private companies fraudulently (but legally) using the NHS logo has clearly run its course. Some in the UK Labour Party should be ashamed of itself for not articulating more clearly their opposition to such obscene onslaughts to the socialist founding principles of the NHS. The public clearly want a properly funded NHS. It is up to a credible party to provide that. Co-payments are a tax on the sick. Even “Pat” Hewitt, the doyenne of a previous Labour administrator, gave a speech to the London School of Economics in 2007 saying it would be madness to go down this route.
And some of the performance of companies to which the NHS has been outsourced is an insult to taxpayers, hardworking or not. Outsourcing giant Serco today announced plans to withdraw from the clinical health services market in a move precipitated by a multimillion pound loss on its NHS contracts. It is possible that Serco’s planned withdrawal could influence significantly how other private firms view the prospect of bidding for contracts involving patient facing services.
The group had already made an early exit from its contracts to provide Cornwall’s out of hours services and clinical services to Braintree Community Hospital.
Introduction of competition into the liberalised market generally has been a policy disaster of totemic proportions, producing sources of corporate fraud and misfeasance, a policy crowbar which can make mergers on the basis of clinical need unlawful, a mechanism for introducing substantial additional transaction costs, and a way of introducing private providers where profit goes into shareholders’ pockets not as surpluses in improving the service. Think tanks which aggressively pimped this have blood on their hands. And they will need to backpedal fast on their prostitution of the purchaser-provider split too.
Earlier this year, it was hailed as a success that the first private sector operator of an NHS hospital has halved its losses in the year to December. AIM-quoted Circle Holdings took over the running of Hinchingbrooke Hospital in Cambridgeshire in 2012 in a controversial part-privatisation. Private companies though wish to have their cake and eat it. They want to hide behind the cloak afforded by the Freedom of Information Act from Tony Blair’s reign. And why should the private providers get protection they haven’t earnt like a welfare claimant so despised by Iain Duncan Smith and Rachel Reeves? Private patients cannot complain to the Public Services Ombudsman for Wales unless they have received treatment commissioned and funded by the NHS. But the Welsh government has now said it has has no plans to bring private health providers within the ombudsman’s remit. Would the private sector like to contribute towards the education and training of the healthcare workforce?
This debacle from Serco, in fact, follows hot on the heels of news from Musgrove Hospital, Taunton, Somerset, where it turns out that dozens of people have been left with significant damage after undergoing operations provided by a private healthcare company at an NHS hospital. The routine cataract operations were carried out by the private provider, Vanguard Healthcare, in May to help to reduce a backlog at Musgrove Park. But the hospital’s contract with Vanguard Healthcare was terminated just a few days after thirty patients, most elderly and some frail, reported complications, including blurred vision and signs of inflammation including pain and swelling.
Laurence Vick, a medical negligence lawyer and the head of the clinical negligence team at Michelmores solicitors in Exeter, had been approached by some of the patients for whom there had clearly been a breakdown of a duty of care. Vick further said the case highlighted the “uneasy relationship” between the NHS and the private sector. He said the question of who paid – when outsourced NHS treatment – failed was of growing importance as more services were handed over to the private sector. This “uneasy relationship” which Vick refers to is likely to get massively worse as one cannot pin down who is legally accountable for failure for performance by subcontractors in “the prime contractor model”, where a main contractor can lead subcontracts for contracts say lasting ten years.
So Tony Blair was blatantly wrong: it does matter who provides NHS care. Blairites have unleashed ideological weapons of mass destruction on the Welfare State, and someone should pay the penalty for this. And it’s worse than that – you don’t know any more who’s in receipt of your taxes when you pay for what you think is the NHS. The Welfare State is being killed softly: and all English neoliberal parties have blood on their hands.
Polling firm ComRes recently found that 49% of people would be prepared to pay more tax to help fund the health service, one in three (33%) people said they would not be ready to do so, and 18% did not know either way. The public’s willingness to pay extra tax to help the NHS has reached its highest level in over a decade amid growing concern about hospitals slipping into the red, waiting lists lengthening and the service becoming unsustainable. The plan always was from the neoliberal advocates to produce a small state with low taxes, but what we have ended up is a moderate state with moderate-high taxes to fund the shareholder dividends of the outsourced companies in a range of sectors, including probation and health.
The Conservatives feel that their voters do not like ‘unfairness’ with one person obtaining an unfair advantage over another, but what we’ve got now is outsourced companies still be paid for unbelievably bad performance, and top CEOs in private providers experiencing a world nothing like their nursing counterparts in the NHS.
Labour will always try to woo the City all it wants, as per
But if disenfranchises hardworking nurses maintaining the fabric of the NHS, and brown nosing the City, it will find it does not get elected. And many socialists in Labour will not want to have blood on their hands in being part of Labour either. This because there is no obvious disinfectant yet.
All a far cry from the Spirit of ’45.
Time for a new regeneration. The New Secretary of State for Dementia.

Ed Miliband looks a bit awkward eating a bacon sarnie, or simply looks a bit “weird”. This man doesn’t look like your next Prime Minister?
But switch back into the reality. A cosmetic reshuffle where the present Coalition had to ditch a Secretary of State more toxic than nuclear waste from Sellafield to transport in a catwalk of tokenistic young hopefuls, “governing for a modern Britain”.
And engage a bit with my reality: where English law centres have been decimated, nobody is feeling particularly “better off” due to the cost of living crisis, GPs have been pilloried for being “coasters”, criminal barristers have gone on strike, or you can’t get your passport on time.
Whisper it quietly, and nobody wants to admit it, that despite all the concerns that Labour will front another set of middle-class neoliberal policies, Labour is in fact going to walk it on May 8th 2015 as the new UK government.
This will obviously be quite a shock to the system, and you can already feel the Civil Service behind the scenes mentally preparing themselves for a change in flavour for the dementia policy.
The current dementia policy had “Nudge” fingerprints all over it. “Customer facing” corporates could become dementia friendly so as to allow market forces to gain competitive advantage for being ‘friendly’ to customers living with dementia.
The Alzheimer’s Society got thrust into the limelight with the Prime Minister’s Dementia Challenge, ably supported by Alzheimer Research UK, to offer the perfect package for raising awareness about dementia and offering hope for treatment through basic research. This private-public partnership was set up for optimal rent seeking behaviour, with the pill sugared with the trite and pathetic slogan, “care for today, and cure for tomorrow.”
Except the problem was that they were unable to become critical lobbying organisations against this Government, as social care cuts hit and dementia care went down the pan. Dementia UK hardly got a change to get a look in, and it looked as if a policy of specialist nurses (such as Admiral nurses) would get consigned to history. They are, after all, not mentioned in the most recent All Party Parliamentary Group report on dementia.
It is widely expected that Labour’s NHS policy will be strongly frontloaded with a promise of equality, which the last Labour government only just managed to get to the statute books. Insiders reckon that this policy will be frontloaded with an election pledge with equality as a strong theme.
In the last few years, it has become recognised that caregivers feel totally unsupported, people get taken from pillar to post in a fragmented, disorganised system for dementia with no overall coordinator, and there are vast chasms between the NHS and social care treatment of dementia.
The next Government therefore is well known to be getting ready for ‘whole person care’, and it now seems likely that the new Secretary of State for Health and Care under a new government will have to deliver this under existing structures. This will clearly require local authorities and national organisations to work to nationally acceptable outcomes for health and wellbeing through empowered Health and Wellbeing Boards. This will help to mitigate against the rather piecemeal patchwork for commissioning of dementia where contracts tend to be given out to your friends rather than the quality of work. Health and Wellbeing Boards are best placed to understand wellbeing as an outcome (which can become missed in research strategies of large corporate-like charities which focus on care, cure and prevention).
And the switch in emphasis from aspirational friendly to a legal equality footing is highly significant. The new policy for dementia under the new Secretary of State will be delivering what people living with dementia have long sought: not “extra favours”, but just to be able to given equal chances as others. Environments will have signage as reasonable adjustments for the cognitive disabilities of people living with dementia in the community under the force of law, rather than leaving up to the whim of a corporate to think about with with the guidance of a fundraising-centred charity to implement.
With the end of the Prime Minister’s Dementia Challenge in March 2015, which has been highly successful in places in delivering ‘dementia friendly communities’, a commitment to improved diagnosis rates and improved research, it is hoped that the next government will be able to take the baton without any problems. It will be quite a public ‘regeneration’ from Hunt to Burnham, but one which many people are looking forward to.
As regards the NHS, Dave Cameron is also being a tad economical with the truth

We keep on being told from the right wing that “money does not grow on trees”, but the Chilcot Inquiry on the Iraq War has so far cost millions (the actual war was costly in many senses too.)
These are #pmqs from my 40th birthday.
Nick Brown MP asks the Prime Minister about the underlying causes of the £2bn forecast deficit for NHS Trusts, and what the remedies might be.
This topic hit the headlines big time yesterday, but it had been copiously discussed by John Appleby by the King’s Fund in one of their documents previously.
The exchange as reported in Hansard went as follows:-
Specifically, the Prime Minister contends that, “money has been ploughed back into better patient care in our NHS.”
This is likely to be true as a half-truth as he does not say “the” before the word “money”.
But where did the money actually go?
It appears it has traditionally gone to HM Treasury, NOT directly to the Department of Health budget.
Everyone knows that the pay settlement for the NHS was tight this year, given the pay freeze discussed at the #RCNCongress this year.
Crispin Dowler reported in the HSJ in October 2012:
“The Department of Health has returned nearly £3bn of its funding to the Treasury over the past two years, despite facing its tightest financial settlement for five decades.
“A Treasury spokesman this week confirmed to HSJ the department had handed back around £1bn of the funding it was allocated for health spending in 2011-12. Just £316m of the £1.4bn that the DH left unspent last financial year has been carried over for it to use in 2012-13.
“The final sum clawed back from last year’s health allocation is double the £500m estimate that was published in chancellor George Osborne’s March Budget.”
Sofia Lind in the Pulse magazine reports a similar story in 2013.
My brief Twitter chat yesterday with @DaveWWest went as follows.
about #NHS ‘efficiency savings’ 12.17 pm PM ‘..that money has been ploughed back into better patient care in the NHS’ true? @DaveWWest
— shibley (@legalaware) June 18, 2014
@legalaware largely paid for increased activity, so yes in a sense but you could point to the annual DH underspends til 13/14, which are not — Dave West (@Davewwest) June 18, 2014
@Davewwest Thanks Dave. I’ve never worked out where in fact the surplus goes – I had thought it goes back into HM Treasury not DoH.
— shibley (@legalaware) June 18, 2014
@legalaware yes you’re right — Dave West (@Davewwest) June 18, 2014
There did seem, however, to be a record number of questions on the NHS in #pmqs?
Dementia care in the whole person care age
The Australian jurisdiction have recently provided some helpful inroads here.
The narrative has changed from one of incessantly referring to people living with dementia as a ‘burden’ on the rest of society. For example, to push a sense of urgency that we have an ‘ageing population timebomb’, the cost of the ageing people with dementia flies completely in the face of other public health campaigns which emphasise, for example, “dementia is not a natural part of ageing”.
“The NHS as a whole and individual hospitals recognise that dementia is a significant, growing and costly problem for them” is the opening gambit of the Alzheimer’s Society “Counting the cost” report.
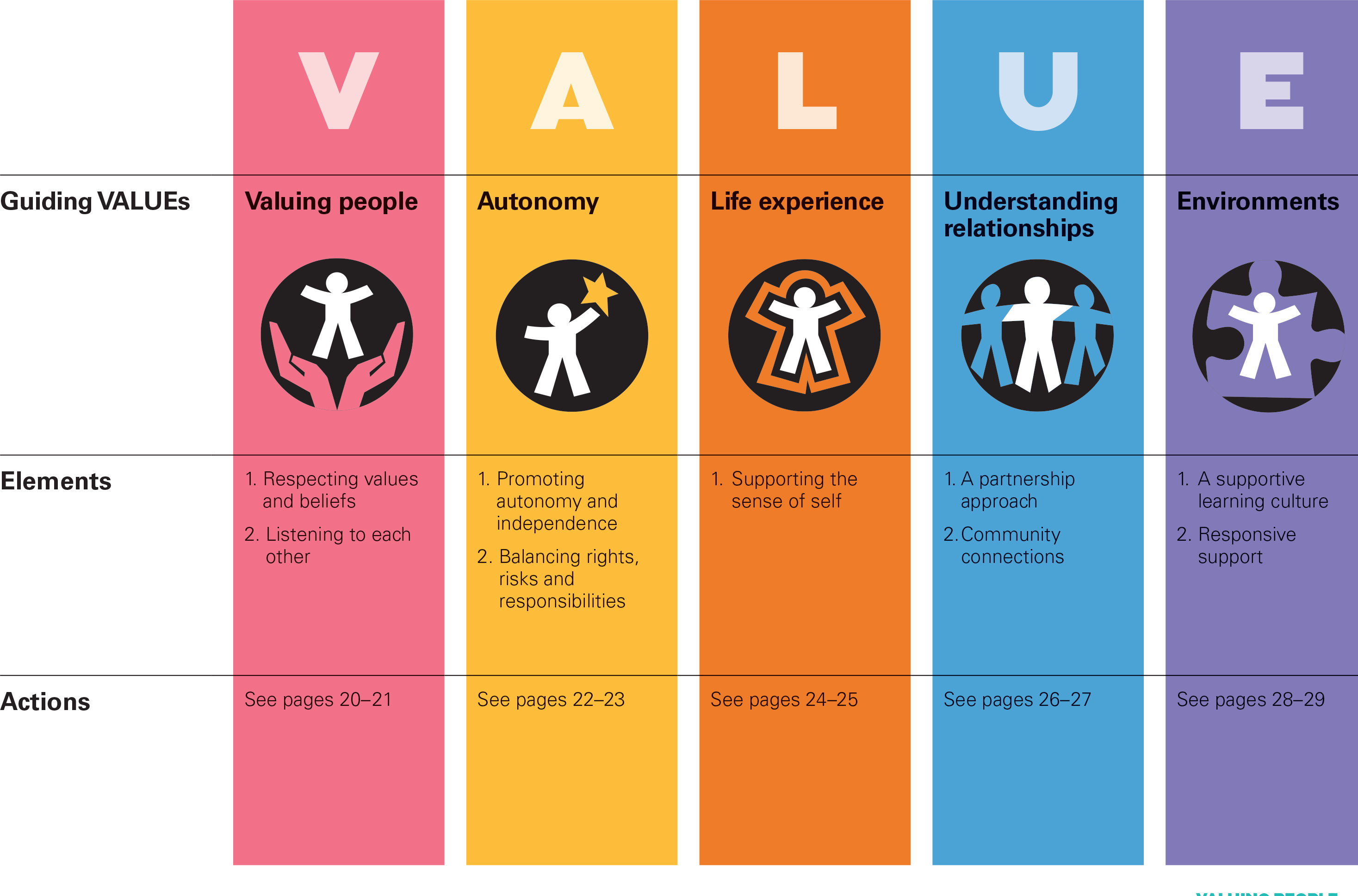
An easy to use online resource, Valuing People from Alzheimer’s Australia has been developed in collaboration with community aged care providers who have helpful in stablishing a person centred approach to service delivery.
Person centred care is a development to provide ervices provided in a way that is respectful of, and responsive to, the preferences, needs and values of people and those in the care and support network.
I cannot recommend this resource highly enough. The main source is here.
In fact, it summarises succinctly the conclusions I came to after my exploration of personhood in my book ‘Living well with dementia’. The late great Prof Tom Kitwood said of personhood, “It is a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being. It implies recognition, respect and trust”.
If a Labour government is elected on May 8th 2015, the first necessary step is to legislate for the repeal of the Health and Social Care Act (2012) and to enact new legislation to allow for integrated packages provided they are justified by clinical outcome. For this to happen, it will be necessary for Labour to undergo a ‘conscious uncoupling’ from all the baggage of EU competition law. For this, it is essential also that the UK government is able to carve out provisions from the investor protection clauses and/or the rest of the EU-US free trade treaty (TTIP).
The “whole person care model” has become attractive to those who wish to break down silos between different physical health, mental health and social care “silos”. It has been worked up in various guises by various parties.
A helpful construct is provided in the document, “Healthcare for complex populations: the power of whole-person care models” originally published by Booz & Company in 2013.
A major problem with dementia care, however it is delivered, is that it is full of divisions: public vs private care, fragmented vs national care, competitive vs integrated models. Operating in silos can’t work because of the nature of the dementias: the mood and cognition of a person with dementia profoundly affects how they might interact with the outside world, for example perform activities in the outside world. And we know that taking part in leisure activities can promote a good quality of life.
Their model is, though, a useful starting point.

Dementia cannot be only addressed by the medical model. In fact, it is my sincere belief that it would be highly dangerous to put all your eggs in the physical health basket, without due attention to mental health or social care. For example, last week in Stockholm, the international conference on Parkinson’s disease, a condition typified by a resting tremor, rigidity and slowness of movement, which can progress to a dementia, often is found to have as heralding symptoms changes in cognition and mood.
So it’s pretty clear to me that we will have to embark on a system of multidisciplinary professionals who could all have a part to play in the wellbeing of a person with dementia, depending on his or her own stage in life, and ability or need to live independently. “Care coordinators” have traditionally been defined incredibly badly, but we do need such an identity to navigate people with dementia, and actors in the care and support network, through the maze.
“Care collaborators” in their construct are very wonkily articulated, like “pre-distribution”, but the concept is not stupid. In fact it is very good. One idea is that people with dementia could act as support as other people with dementia, for people on receiving a diagnosis of dementia. The rationale for this is that people living with long term conditions, such as for example recovery from alcoholism, often draw much support from other people living with other long term conditions, away from a medical model. There needs to be safeguards in the system to safeguard against a lot of unpaid goodwill (which currently exists in the system.)
Informatics would have a really helpful rôle here, being worked up in telecare and assistive technology. But even simple disruptions such as a person living with dementia at risk of falling from problems with spatial depth perception being able to ‘hot email’ a care coordinator about perceived problems could trigger, say, an early warning system. And with various agents in the provision of care being involved in differing extents it will be up to NHS England to work out how best to implement a single accountable tariff. Falls are just the sort of ‘outcome metric’ which could be used to determine whether this policy of ‘whole person care’ for people living with dementia is working. And, even though everyone ‘trots it out’, the performance on avoided hospital admissions could be put into the mixer. It’s already well recognised that people with dementia can become very disoriented in hospital, and, and despite the best efforts of those trying to improve the acute care pathway, people with dementia can often be better off away from hospital in the community. But it’s imperative that care in the community is not a second-rate service compared to secondary care, and proper resourcing of community whole person care is essential for this before any reconfiguration in acute hospital services.
But the private sector has become such a ‘bogey term’ after arguably the current Government overplayed their hand with the £3bn Act of parliament which turbo-boosted a transfer of resource allocation from the public to private sector. Any incoming government will have to be particularly sensitive to this, as this is a risk in strategy for the NHS.
In October 2005, Harold Sirkin, Perry Keenan and Alan Jackson published a highly influential article in the Harvard Business Review entitled “The hard side of change management“. Whilst much play has in fact been made of politicians having to be distant from running the NHS, a completely lubricous line of attack when it is alleged that Jeremy Hunt talks regularly to senior managers and regulators in the NHS, the benefits of clear political leadership from an incoming Labour government are clear.
Andy Burnham MP has already nailed his colours to the mast of ‘whole person care’ on various occasions, and it is clear that the success of this ambitious large scale transformation depends on clear leadership and teamwork from bright managers. Take for example the DICE criteria from Sirkin, Keenan and Jackson:

But this is perfectly possible from an incoming Government. The National Health Service has a chance to lead on something truly innovative, learning from the experience of other jurisdictions such as Australia and the USA.
As alluded to in the new resource from the Alzheimer’s Australia, this cultural change will require substantial ‘unfreezing’ from the current mindset for provision of care for people with dementia. It will require a change in explicit and implicit sources of knowledge and behaviours, and will need to be carefully brought about by learning from the successes and failures of pockets of implementation.
The whole project’s pretty high risk, but the rewards for people living with dementia, and members of the care and support network, are potentially vast. But it does require the implementation of a very clear vision.
[First posted on the 'Living well with dementia' blog]

A large scale cultural national transformation is needed to drive whole person care in dementia
I’ll be blunt. It’s my dream for the #NHS to run a proactive not reactive service, promoting the whole person living well with dementia.
The Australian jurisdiction have recently provided some helpful inroads here.
The narrative has changed from one of incessantly referring to people living with dementia as a ‘burden’ on the rest of society. For example, to push a sense of urgency that we have an ‘ageing population timebomb’, the cost of the ageing people with dementia flies completely in the face of other public health campaigns which emphasise, for example, “dementia is not a natural part of ageing”.
“The NHS as a whole and individual hospitals recognise that dementia is a significant, growing and costly problem for them” is the opening gambit of the Alzheimer’s Society “Counting the cost” report.
An easy to use online resource, Valuing People from Alzheimer’s Australia has been developed in collaboration with community aged care providers who have helpful in stablishing a person centred approach to service delivery.
Person centred care is a development to provide ervices provided in a way that is respectful of, and responsive to, the preferences, needs and values of people and those in the care and support network.
I cannot recommend this resource highly enough. The main source is here.
In fact, it summarises succinctly the conclusions I came to after my exploration of personhood in my book ‘Living well with dementia’. The late great Prof Tom Kitwood said of personhood, “It is a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being. It implies recognition, respect and trust”.
If a Labour government is elected on May 8th 2015, the first necessary step is to legislate for the repeal of the Health and Social Care Act (2012) and to enact new legislation to allow for integrated packages provided they are justified by clinical outcome. For this to happen, it will be necessary for Labour to undergo a ‘conscious uncoupling’ from all the baggage of EU competition law. For this, it is essential also that the UK government is able to carve out provisions from the investor protection clauses and/or the rest of the EU-US free trade treaty (TTIP).
The “whole person care model” has become attractive to those who wish to break down silos between different physical health, mental health and social care “silos”. It has been worked up in various guises by various parties.
A helpful construct is provided in the document, “Healthcare for complex populations: the power of whole-person care models” originally published by Booz & Company in 2013.
A major problem with dementia care, however it is delivered, is that it is full of divisions: public vs private care, fragmented vs national care, competitive vs integrated models. Operating in silos can’t work because of the nature of the dementias: the mood and cognition of a person with dementia profoundly affects how they might interact with the outside world, for example perform activities in the outside world. And we know that taking part in leisure activities can promote a good quality of life.
Their model is, though, a useful starting point.
Dementia cannot be only addressed by the medical model. In fact, it is my sincere belief that it would be highly dangerous to put all your eggs in the physical health basket, without due attention to mental health or social care. For example, last week in Stockholm, the international conference on Parkinson’s disease, a condition typified by a resting tremor, rigidity and slowness of movement, which can progress to a dementia, often is found to have as heralding symptoms changes in cognition and mood.
So it’s pretty clear to me that we will have to embark on a system of multidisciplinary professionals who could all have a part to play in the wellbeing of a person with dementia, depending on his or her own stage in life, and ability or need to live independently. “Care coordinators” have traditionally been defined incredibly badly, but we do need such an identity to navigate people with dementia, and actors in the care and support network, through the maze.
“Care collaborators” in their construct are very wonkily articulated, like “pre-distribution”, but the concept is not stupid. In fact it is very good. One idea is that people with dementia could act as support as other people with dementia, for people on receiving a diagnosis of dementia. The rationale for this is that people living with long term conditions, such as for example recovery from alcoholism, often draw much support from other people living with other long term conditions, away from a medical model. There needs to be safeguards in the system to safeguard against a lot of unpaid goodwill (which currently exists in the system.)
Informatics would have a really helpful rôle here, being worked up in telecare and assistive technology. But even simple disruptions such as a person living with dementia at risk of falling from problems with spatial depth perception being able to ‘hot email’ a care coordinator about perceived problems could trigger, say, an early warning system. And with various agents in the provision of care being involved in differing extents it will be up to NHS England to work out how best to implement a single accountable tariff. Falls are just the sort of ‘outcome metric’ which could be used to determine whether this policy of ‘whole person care’ for people living with dementia is working. And, even though everyone ‘trots it out’, the performance on avoided hospital admissions could be put into the mixer. It’s already well recognised that people with dementia can become very disoriented in hospital, and, and despite the best efforts of those trying to improve the acute care pathway, people with dementia can often be better off away from hospital in the community. But it’s imperative that care in the community is not a second-rate service compared to secondary care, and proper resourcing of community whole person care is essential for this before any reconfiguration in acute hospital services.
But the private sector has become such a ‘bogey term’ after arguably the current Government overplayed their hand with the £3bn Act of parliament which turbo-boosted a transfer of resource allocation from the public to private sector. Any incoming government will have to be particularly sensitive to this, as this is a risk in strategy for the NHS.
In October 2005, Harold Sirkin, Perry Keenan and Alan Jackson published a highly influential article in the Harvard Business Review entitled “The hard side of change management“. Whilst much play has in fact been made of politicians having to be distant from running the NHS, a completely lubricous line of attack when it is alleged that Jeremy Hunt talks regularly to senior managers and regulators in the NHS, the benefits of clear political leadership from an incoming Labour government are clear.
Andy Burnham MP has already nailed his colours to the mast of ‘whole person care’ on various occasions, and it is clear that the success of this ambitious large scale transformation depends on clear leadership and teamwork from bright managers. Take for example the DICE criteria from Sirkin, Keenan and Jackson:
But this is perfectly possible from an incoming Government. The National Health Service has a chance to lead on something truly innovative, learning from the experience of other jurisdictions such as Australia and the USA.
As alluded to in the new resource from the Alzheimer’s Australia, this cultural change will require substantial ‘unfreezing’ from the current mindset for provision of care for people with dementia. It will require a change in explicit and implicit sources of knowledge and behaviours, and will need to be carefully brought about by learning from the successes and failures of pockets of implementation.
The whole project’s pretty high risk, but the rewards for people living with dementia, and members of the care and support network, are potentially vast. But it does require the implementation of a very clear vision.
[First posted on the 'Living well with dementia' blog]
