Home » Articles posted by shibleyrahman (Page 4)
Author Archives: shibleyrahman

Delirium. Why so little and so late?
My most recent experience of delirium was truly terrifying, to the point that, as a care partner of a close relative with dementia experiencing delirium, I felt I needed counselling about this admission to a London teaching hospital. I have witnessed delirium ‘around the clock’ for half a month so far.
Delirium is not for me a matter of Twitter hashtags, gimmicks or infograms, but a very serious issue I wish to be taken much more seriously. Traditionalists in neurology, for example in the tradition of Gall or Broca, pride themselves on localisation of function – in other words a particular constellation of signs will tell you where the lesion is. But this reason for me is insufficient why academic neurologists and psychiatrists should be disinterested in delirium. Where for example is the research which explains the neural substrates of hypoactive and hyperactive delirium? How long do ‘sleep episodes’ last for? Is it a good idea to wake someone up while he is sleeping? Are there are any neuroprotective agents which prevent long term deterioration after delirium? How much of the delirium will the person experiencing it actually remember?
In a paper by Profs. John Young and Sharon Inouye, the following case scenario is presented:
“An elderly man is recovering from a heart attack and seems to want to lie in bed. He is polite when approached, but sleepy, and he doesn’t seem interested in eating or drinking. Sometimes his speech is incoherent and he doesn’t seem to follow what is said to him.”
Yet this is virtually a carbon copy of the state of my relative when discharged under ‘discharge to assess’. The relative, who also could not mobilise at all (due to the delirium and viral pneumonia), was unmanageable for me at home. I live with her, and unfortunately she had to boomerang bang into the same hospital three days after being discharged ‘medically fit for discharge’. As it happens, for virtually all of the nineteen-day hospital re-admission, many factors conspired to ensure my relative stayed bed-bound, totally unusual for her. It was with a very heavy heart that I decided to call ‘999’, as the hospital environment itself often precipitates or exacerbates episodes of delirium..
The diagnosis at that stage was hypoactive delirium, although the picture became more mixed in the subsequent few days. My relative was admitted, and thought to have a respiratory tract infection, constipation and dehydration. She also lives with frailty and dementia.
It is claimed that, ‘for the family and health-care staff, clear communication, education, and emotional support are vital components to assist with decision making and direct the treatment care plan’, but I felt all three were lacking in this admission. Nobody told me about what to expect in the delirium, or offered me any support for my distress.
If you read the page on “Dementia UK” website about delirium, you are offered the following advice:
“keep calm and reassure the person”
A different HCA in the bay every day and every night is not reassuring.
“observe the person to see if they are in any pain”
The paracetamol was written up prn. My relative could not remember if she was in pain, and none of the nursing staff asked me as her full-time carer if she was in pain.
“avoid too much stimulation”
the ward had a noisy bleeping air mattress which was bleeping all the time, and at night the lights were often bright.
“if possible offer them drinks to maintain hydration”
this simply didn’t happen
Whilst my own regulator, the General Medical Council, takes heavy criticism on a daily basis, I can frankly say that the GMC code on communication (“Communicate effectively” in “Duties of a Doctor”) was flatly ignored in my relative’s admission:
31. You must listen to patients, take account of their views, and respond honestly to their questions.
32. You must give patients he information they want or need to know in a way they can understand. You should make sure that arrangements are made, wherever possible, to meet patients’ language and communication needs.
33. You must be considerate to those close to the patient and be sensitive and responsive in giving them information and support.
34. When you are on duty you must be readily accessible to patients and colleagues seeking information, advice or support.”
John’s Campaign, for me, has to be more than allowing care partners to sit by patients’ beds for longer than a few hours. To make delirium management work, care partners, where available, should be fully involved. I was not asked once by clinician how my relative’s function had dropped off a cliff, nor indeed what she was capable of doing prior to admission.
For me, the initial ‘head rush’ of my relative was astonishing – she was agitated with a blood pressure of 200/110. I subsequently discovered that high levels of cortisol had been suggested to be associated with acute stress in precipitating and/or sustaining delirium. (Neuroimmunomodulation. 2005;12:60–66).
Of course, I agree with letting the treating physicians to ‘get on with it’, but it was staggering how none of the rationalisation of the medications was ever communicated with me (including the discontinuation of the cholinesterase inhibitor). The cholinergic system has a key role in cognition and attention, and it is not surprising, therefore, that there is some evidence to support a role for cholinergic deficiency in delirium. For example, anticholinergic drugs can induce delirium and often contribute substantially to the delirium seen in hospitalized patients, and cholinergic deficiency is commonly implicated in the pathophysiology of delirium.
Bidzan and Bidzan (2012) have described a 62-year-old female diagnosed with Alzheimer’s disease, who on sudden discontinuation of donepezi experienced a worsening of the dementia symptoms, culminating in delirium. When donepezil was re-prescribed, the delirium resolved and the patient’s mental state stabilised. I would also find lorazepam and midazolam prescribed to my relative, without any communication with us, when it is believed by some that these can actively worsen delirium.
None of the following points from ‘Concise guidance to good practice’ from the Royal College of Physicians of London on delirium (2006) were followed in the course of my relative’s hospital admission.
“A history from a relative or carer about the onset and course of the confusion is essential to help distinguish between delirium and dementia
Patients at high risk should be identified at admission and prevention strategies incorporatedinto their care plan
Many patients with delirium are unable to provide an accurate history. Wherever possible, corroboration should be sought from the carer, general practitioner or any source with good knowledge of them.
The patient should be nursed in a good sensory environment and with a reality orientation approach, and with involvement of the multidisciplinary team.Keep the use of sedatives and major tranquillisers to a minimum.
Review all medication at least every 24 hours.
Senior doctors and nurses should ensure that doctors in training and nurses are able torecognise and treat delirium.”
I feel that non-pharmacological strategies are the first-line treatments for all patients with delirium, and yet as a care partner I was offered absolutely no help with this. I was not encouraged over any reorientation and behavioral intervention, or advised on pretty standard advice such as using clear instructions and make frequent eye contact.
The hospital bed itself had a bed rail. But it is advised that, “physical restraints should be avoided because they lead to decreased mobility, increased agitation, greater risk of injury, and prolongation of delirium.”
As the ultimate insult, the hospital in question refused to talk to me about my experience of the admission as part of their ‘Friends and Family’ feedback, only because the relative in question had limited memory of the actual admission itself.
As a medical student, I thought of delirium as a list of causes, and, even as a foundation doctor, I had little experience of it. But I do feel now it should no longer remain in the blindspot of some doctors, particularly as the experience was so distressing for me.

Carers have to be valued, not treated as an inconvenience

I think before a physician comes to the conclusion that his or her patient has had ‘an acute deterioration of dementia’, he or she should make some effort to get a clear history of the time scale of events.
It amazed me how I was not asked at the Royal Free by any of the admitting physicians what the timescale of my mum’s decline in communication, behaviour or mobility had been. This was not a focal problem in the acute assessment and treatment area, but has been throughout the ten day admission so far.
I genuinely do wonder how useful, if at all, junior doctors are in the daily ward round of my mum with delirium, on a background of dementia. A message to you all – it is not a big success to say that my mum’s chest is clear, and proclaim she is medically fit for discharge, when she has been stuck in bed for the whole admission, her food and drink intake has fallen off a cliff, and she occasionally talks complete mumbo jumbo.
The ward round model is totally unsuited for managing delirium. The junior doctors do not involve the carers in any sort of history, and nor do any of the staff on the ward. There is absolutely no discussion of the management, including calming techniques if your mum happens to be agitated, the avoidance of chemical or physical restraints, orientation in time and place, and sleep hygiene, for example. No discussion at all.
It’s almost as if delirium was never taught at medical school to any of the staff in the hospital. To be honest, I have been totally amazed how my mum, who had suddenly fallen asleep during the middle of the day with hypoactive delirium, would have ‘nothing wrong’ in the eyes of the healthcare assistants.
It’s not enough to give carers passports, although that helps a lot. Carers need to be there to be as far as possible on the ward round, to know what medications have been crossed off without the patients’ or family’s knowledge, to know what the rough plan is, and to be able to ask questions.
It’s often the case that healthcare assistants aren’t able to feed patients with dementia. The reason for this is that it’s not just the actual food which counts, although that’s a big part of it, but also the entire mealtime environment, including how comfortable the patient feels about eating the often dire hospital food. And often the food is dumped miles away from the patient.
And if, like mum, her mobility and independence had relatively suddenly dropped off a cliff, the therapists need to know this. I’ve had absolutely no discussion or goals set by the therapists of what they hope to do with mum. Mum is a frail lady who has experienced a number of shocks, viz change of environment, weight loss, delirium, dementia, infection, dehydration, and there’s been no discussion of her frailty despite this apparently being a priority of the NHS.
There has been no discussion of her management of dementia, with her cholinesterase inhibitor having been crossed off, nor her wider needs beyond discharge. The whole thing is entirely pitiful, as if the two long term conditions my mum has been living with in the community are entirely irrelevant to this hospital admission.
And her meds for osteoporosis have been crossed off. And for her high blood pressure.
I have often thought that doctors don’t want to communicate with carers there, often because they don’t want them interfering with their ill-informed medical plans. This is hugely insulting to those of us who are 24/7 trying our best for our loved ones.
It’s not just about having a dementia friendly clock, or reminiscence room. Carers have to be valued, not treated as an inconvenience.

Why might there be a divide between patients and doctors?

The case against Bawa Garba (“Bawa Garba”) has thrown up some fairly strong opinions from people who support Bawa Garba and from those who don’t.
The feelings on the social media seem to have ignited some long-held views about whether the medical profession is working with patients, or simply against.
All opinions lie on a range, and some of the opinions lie at an extreme, such as the notion that doctors regularly lie and cover up.
Much of the discussion on Twitter seems to refer to some power imbalance, but it is the case that all regulated medical professions on Twitter run the danger of being reported to the regulator if their behaviour is called into question. The vast majority of registered doctors, one assumes, does not want to be abusive to any patients, who are not even their own.
The idea that registered doctors regularly cover up their mistakes is a conclusion from the admissions on Twitter that doctors regularly make mistakes and also that doctors are not regularly reporting themselves or others to any regulator about their mistakes.
I feel the question of what actually is a ‘mistake’ or error needs some airing too, however. We accept that there is a range of errors, some which do not cause any substantial harm to decisions which are outright dangerous. The word ‘mistake’ itself is binary, but it does often take a judgment from peers as to whether a pattern of decision-making was clearly abnormal.
No two doctors will always make the same clinical decisions, and even specialists working in exactly the same field might have differing views about the direction in which to take their patients.
But the binary nature of ‘doctor’ and ‘patient’ is at once called out when one realises that many doctors are themselves patients or doctors, so have direct experience of what it’s like on the other side of the fence. Admittedly, most doctors have to switch off emotionally about their patients to protect themselves from going into an emotional meltdown.
This defensive mechanism of not becoming too close to your patients lies in conflict with the democratisation of opinions on Twitter. It would be wrong to feel that all opinions, however, have exactly the same merit. For example, even the most ferocious denial of the Holocaust will fall down.
The information asymmetry between doctors and patients has long existed, and it is probably right that tensions between doctors and patients have resurfaced following Bawa Garba. Some patients will feel strongly that the diagnoses or management plans from their doctors are palpably wrong, given what they might have learnt elsewhere from other sources, and feel powerless to speak out.
The powerlessness to speak out is rife within medicine and nursing anyway, explaining to some extent why ‘whistleblowers’ like Chris Day have such a terrible time. It’s also fair to say that the communication between doctors and patients can be horrific too. I found medications regularly crossed off and added to my mum’s prescription chart without any discussion with anyone.
Whilst it is lovely and fluffy to ‘believe in’ shared decision making and co-production, it is worth considering why it is so widely felt that there is a tense power dynamic between doctors and patients, epitomised by the aloofness of doctors on ward rounds who only see a snapshot of the lives of patients and carers.
I believe that doctors can learn a lot from patients and carers, particularly for frailty, dementia and delirium where the corroborative history is key. This is not just about a sop to visiting hours. This is actually about making the diagnosis and care plans less susceptible to failure.
So whether or not you feel the GMC was too ‘lenient’ with Bawa Garba is neither here nor there compared to the unresolved issues, of a perception of arrogance of some doctors by some patients, or a perception of excess victimhood by some patients in the eyes of some doctors.
The idea of doctors and patients being on opposite sides of the fence is entrenched by the idea of clinicians going into battle ‘on the front line’. Whilst doctors continue to make decisions on their patients albeit in a well meaning and paternalistic way, they will always be accused of playing ‘God’.
What’s the difference between a doctor and God? God doesn’t think he’s God.

Does the GMC believe in patient safety or public confidence?

I am sure that the GMC are interested to a small extent in promoting patient safety or public confidence, but the impression they give out to me is that they see themselves more like the Spanish Inquisition.
For the General Medical Council (GMC), which indeed currently regulates me, to promote patient safety or public confidence it cannot pretend to be apolitical. The wider systemic issues why both safety and confidence are at threat on a daily basis, due to political, economic, and financial issues, simply cannot be ignored any longer.
To some extent, the GMC feels that it can deal with issues without getting its ‘hands messy’ reminiscent to me how the law courts tried to deal with legal issues about welfare payments without making any political or social inquiry. But this is clearly untenable.
If a laboratory is unable to be resourced sufficiently, or there aren’t enough doctors to carry bleeps safety, or there is somehow a wider cultural breakdown in communication between healthcare professionals, it is not reasonable for a ‘just culture’ to fixate on a sanction for a single doctor when much wider issues go simply unaddressed.
I don’t feel it is possible that the public can have confidence in the wider state of the health service if patients with chest pain or an acute asthma attack are queuing up on trolleys in corridors, and the target for assessing acute emergencies is regularly breached nationally.
“Bawa Garba” was clearly a show trial, for the GMC to show to Daily Mail readers that a single mistake of this gravity will not be tolerated. But this does not in itself improve service provision, and, arguably worsens it by throwing in a ‘dead cat’ into the debate.
“Bawa Garba” did not address the central issues of intention to kill or recklessness in medical manslaughter, and, even more worryingly, seemed to signal that the GMC was not only above its own tribunal but potentially above the law in general in wishing to make ‘judge made law’.
I think this is a huge strategic mistake by the GMC, and, if this was a marketing strategy from the GMC, it has gone very badly wrong. Without the legal framework to give some definition of the scope of ‘patient safety’ and ‘public confidence’, the definitions for both are too wooly, and basically issues the GMC a free licence to get rid of anyone it doesn’t like the look of.
You can argue, for example, that a surgeon etching his initials onto a transplanted liver worsens public confidence in the medical profession, as legally there is no implied consent for a surgeon to etch this on property which is not his (a body part). That is common assault and battery in the law, and has been since 1861 in statute law.
Everyone has a bad day at work, and clearly some clinical mistakes are much worse than others. But to pretend that doctors cumulatively in the NHS don’t make thousands of mistakes daily in the NHS is simply complete rubbish, and many medical errors are not made deliberately. To promote both patient safety and public confidence adequately, we do need an approach to the law which is not simply retribution, but potentially rehabilitative too.
After all, it’s not as if we’re not short of doctors in the UK for the demands of the population.
And the GMC does need to operate in the law. It says it does not wish to go behind decisions of the courts, but even the most basic circumspect analysis of the law will tell you the assessment of fitness to practise is a different question is to whether a jury is satisfied criteria are met for a specific offence.
The GMC’s wish not to go behind decisions means that they are in serious danger of running roughshod over double jeopardy in English law, which means you cannot be convicted of the same crime twice.
The GMC really does need, in my opinion, to change tack drastically, as indicated by the disapproval of the Professional Standards Authority at the “Bawa Garba” decision. Otherwise, it will stay as a faceless, self-righteous mass that some of us can really have any faith in.

Everything about the Royal Free management of delirium is completely abnormal

For a start, the Royal Free’s obsession with ‘medically fit for discharge’ does not seem to include whether my mum’s intake of food and drink had fallen off a cliff. She was incoherently rambling, and looked as if she was sedated and half-asleep. This is typical hypoactive delirium, and made my mum’s discharge to assess last week unsurprisingly a complete nightmare for me, her full time carer with whom she lives.
It seems totally unimportant to the therapists on this ward at the Royal Free that she has lucid intervals when she can interact with people. Instead, the therapists are uniquely focused on their task-centered care, performing tasks at their time and convenience, irrespective of which persons are awake or which family is around. As a proponent of person-centred care, I find this totally objectionable, as we now enter two whole weeks of mum deconditioning in bed. For all the attention to ‘end PJ paralysis’, I doubt thanks to the inattention of the therapists at the Royal Free, mum will ever gain her independence again. Her food and drink intake, despite palliation needs, had fallen off a cliff, due to the delirium. She was totally ambulant before. The label of ‘dementia’ rather than opening doors has sent her instead hurtling down a route of ‘terminal’ and ‘end of life’, when she was to all intents and purposes ‘living well’ in the community.
My mum is very light-weight, and is very frail. The diagnosis of dementia, with all drugs crossed of including her cognitive enhancers, never mind rebound of an anticholinergic delirium, has become like a noose round her neck, with the frailty completely ignored. Twice I have had to request the medical team to cross off benzodiazepines, midazolam and lorazepam, off the drug chart, which most people accept can be deliriumogenic. The ward has often been very noisy at night, making it unsurprising many patients are so sleepy during the way, whether or not they have been written up for sedating drugs without any discussion with patient or family. The nurses on the ward, however, are truly outstanding.
Some healthcare assistants are very good. Some overreach themselves with banal phrases such as ‘the blood pressure is PERFECT’ and deliberating facing the electronic blood pressure monitor so that the reading is out of sight. The culture is positively antagonistic, with some threatening to ‘report you for being abusive’, if a cleaner sweeps under your feet while you’re sitting at a chair without any warning, or if you wish to connect Mum on Skype with Kate Swaffer in Australia as a bit of reminiscence. Incidentally, the same healthcare assistant who reported me for that Skype was later sat in the corner with her headphones on chatting on her mobile phone, while patients were calling, and also was feeding my mum at high velocity even when she had not cleared the current mouthful.
I had no choice but to seek my mum to get mum admitted, for dehydration and her falling oxygen saturations, even though the admission itself worsened delirium. There is no attempt to reorient mum in a normal sleep-day cycle, and the regular ‘observations’ have the opposite of a calming effect. The precise diagnosis for mum is a mixed delirium, as she can be agitated. I would never dare to inflict my diagnosis or management on mum, given the code of conduct for registered medical professionals. There seems culturally a reluctance to negotiate with the clear diagnosis of delirium, or a discussion of how function may be recoverable, as the underlying pneumonia is ‘cured’ (or more like delirium does not get coded properly as a diagnosis). There seems to be little appreciation that delirium is worth spotting, and is a significant serious risk itself. When you consider that nobody introduces themselves or what they do, apart from a significant outstanding minority, you have to acknowledge there are good reasons for patients being so confused.
I’ve been really appalled with the ‘acute deterioration of dementia’ being such a prevalent attitude, and no willingness to embrace mum’s function prior to the admission. That is entirely in keeping for the reluctance of everyone to know what mum’s function was like prior to admission. It says on mum’s board that she likes word searches. I can say hand on heart that she has never done a word search in her life.
And whilst medically ‘fit’, she now can’t walk – and that’s new from this admission.
The ‘Frailty Core Capabilities Framework’ is leading not following

I have on occasion wondered what the ‘Frailty Core Capabilities Framework‘ might look like. I have experience of the ‘Dementia Core Skills and Learning Framework‘ also from Skills for Care, having indeed published a book on it.
Unlike dementia, there are very few books on frailty suitable for practitioners and professionals, in health and social care and in housing.
One of the aims of students of frailty according to this new framework is to access up-to-date information about frailty. This is actually quite difficult – there are no large charities concerned with frailty producing factsheets, for example. The new initiative ‘Frailty Focus‘ is a very good website, but this requires service users who are computer savvy.
The Framework seems heavily entrenched in a view of frailty promoted by the British Geriatrics Society, with reference to five frailty syndromes. One is left wondering whether the view of frailty espoused in the framework goes more than a rebadging of the ‘geriatric giants’, for the purposes of making the area attractive to service commissioners.
A big plus of the new frailty framework is that is bang up to date on a view of frailty which I have been espousing, that it is difficult to frame frailty only in terms of the accumulation of deficits. A discussion of frailty must include resilience (and intrinsic capacity).
But I am not alone, in that this brings me directly supporting the approach of the British Geriatrics Society and that of person-centred integrated care in general. That is, health, social care and housing as a whole should be seen as pro-active rather than reactive, so that people who are frail can be ‘offered something’.
And in the absence of robust interventions to reverse frailty, such as nutrition, exercise or multi-component interventions, the new frailty framework is totally in line with current thinking, in promoting assets and community development, resilience, personalised care planning and advance care planning.
The frailty framework also refers to what I feel are enduring themes of frailty, in other words complexity and multi-morbidity.
The framework also emphasises co-production and co-design of services, communication and shared decision-making, ensuring a power dynamic which is far less paternalistic than before. The emphasis on the rights of care partners, and the legal powers of attorney, ensure that the frailty framework reads as a fresh and relevant contribution to post-identification support.
The frailty framework also gets to grips with ways of ensuring independence and quality of life, and I was impressed by the reference to contemporary themes in frailty research, including thermal support, assistive technology and loneliness.
I feel that the frailty framework will do much to get practitioners thinking about what might actually be important to people living with frailty and their care partners. I also reckon it is leading the world literature in frailty, rather than merely following it, and this is no small accomplishment.

Dementia friendly communities are more than the customer experience
For some reason, the terms ‘person experience’, ‘patient experience’ and ‘customer experience’ have become conflated to a rather unhelpful degree.
I would like to be careful how I say this, though, because we do know that bad customer experience does exist for people living with dementia and care partners, and guidance or standards can help.
Corporate marketing can give high street brands a helping hand with adding competitive advantage, by making them more ‘dementia friendly’, and in return these high street brands can give a bit of marketing for the charity in return.
This is, of course, not the time for cynicism. ‘Dementia friendly communities’ have also in a more recent configuration which emphasises a rights-based approach.
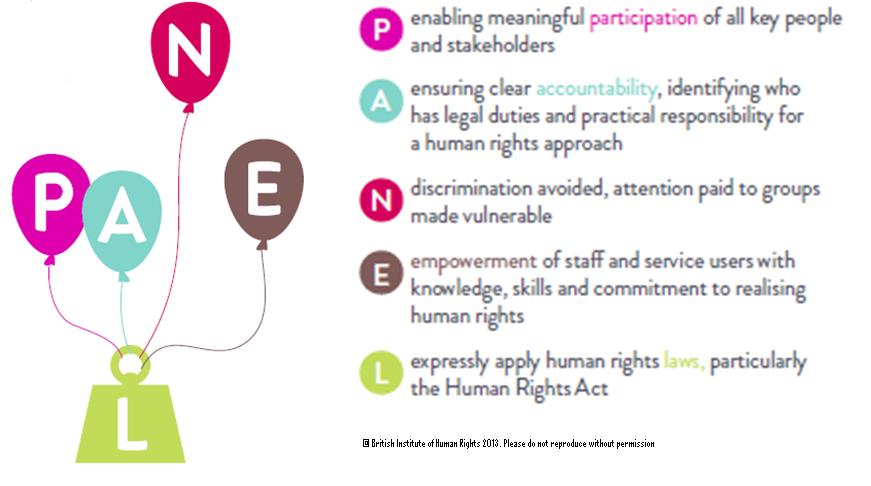
I’ve often felt that the rights-based approach gets confused with party A taking party B to court over matter C, but they are much more of a question of a rights consciousness. The PANEL principles were originally proposed to articulate this rights-based approach, and are summarised here.
PANEL stands for Participation, Accountability, Non-Discrimination and Equality, Empowerment and Legality.
I have seen with my own eyes the subtle, and indeed not-so subtle, discrimination of society towards people with dementia. This is disappointing as the Prime Minister Dementia Challenge was fist introduced five years ago.
I might be standing in a room with my mother, known to have a diagnosis of mixed Alzheimer’s and vascular dementia, and a third person can often completely ignore her because of her diagnosis.
For all the millions of ‘Dementia Friends’ which have been created, the question remains whether a genuine cultural shift in attitudes has existed. Various unknowns exist, including how bad things would have been if there had been no public awareness campaign for dementia.
A significant problem which pervades all the work looking at whether there is merit in the dementia friendly communities approach is knowing how much time to give the dementia friendly communities to ‘take effect’.
Participation is something which can be looked at directly. Democratic inclusion is a matter of principle, and it would be interesting to know how many people with dementia, including in care homes, are actively supported to vote. This might involve making reasonable adjustments for participating in the voting process.
Many of these aspects can be looked at also by looking at how many persons with dementia, now patients of the NHS, are able to secure a GP appointment in the festival of ringing up at 8 am when the GP opens. Many barriers might exist, such as being oriented to the time, remembering the GP number, recalling the purpose of the appointment, and so on.
The scale of ambition is also worth looking at. We could look at how many providers are providing NHS information in an accessible manner, but this is venturing into the area of competitive advantage, especially where providers in dementia services exist in a private market.
But what is interesting, with the problems in legal aid and access to justice aggravated from 2012 especially, is how many persons with dementia on receiving a diagnosis are able to secure a lasting power of attorney.
Again, we would expect a significant difference right now between communities which are ‘dementia friendly’ and those which are not.
So, in summary, I feel that the focus on customer experience in high street shops is a bit of a canard, and wider issues of access to health, access to justice, access to health or participation in the democratic process should have been tangible benefits of ‘dementia friendly communities’ by now.

The perfect storm around #BawaGarba was a long time coming

As a result of my erasure in 2006 from the register of medical professionals in the UK, I had a lot of time to reflect on the events leading up to it. I have from time to time also reflected on this following my restoration in 2014. In the meantime, I had re-trained in law, paradoxically inspired by my experience of the judicial process. This was not a brief Masters in medical law, but both my Bachelor and Masters of Law, as well as the pre-solicitor training course. To do the last bit, I had to be approved as a fit and proper person by the legal regulator, the Solicitors Regulation Authority. I enjoyed my study of the English legal system, and reflect that if I had never studied law I would never have met the late Prof Gary Slapper – a formidable academic with an interest in conspiracy theories and corporate manslaughter.
This is all rather awkward, not least because Charlie Massey and Jeremy Hunt get on well, despite having divergent views on the implications of the #BawaGarba judgment. In a way, the General Medical Council (GMC) does not actually do ‘personal’, although ensuing events do rather appear like a hate campaign. It has become traditional to issue a sop to the ‘victim’ of misfeasance of a Doctor, and I do genuinely feel that there can be few things worse than the mental anguish of a grieving relative. The GMC and Medical Practitioners Tribunal Service maintain separation of powers, and, whilst I feel that the GMC can move in mysterious ways, I feel that the GMC believe that they are doing their very best to maintain public safety and confidence in the medical profession. This blogpost is therefore not an easy one to write, and inevitably will mean that I could accidentally cause offence. I am reflecting on issues to the best of my ability, and, if I fall short, I do apologise.
#BawaGarba found herself in a perfect storm. There are various systemic factors arguably out of direct control of the GMC. These are the exact funding of the NHS, including whether there is a sufficient number of doctors on rotas in individual hospitals. Notwithstanding, the GMC has a statutory duty in education and training, and, from what I know, will intervene in cases where NHS Trusts offer a suboptimal training experience. But there are important other systemic factors. It is quite common for non-white British trainees, once a GMC alert has been triggered, to be ‘thrown to the wolves’ from the regulatory process, but whether this achieves statistical significance is worth exploring. The trend has been for, once these Doctors have been reported, for all positive references to be withdrawn, and, often, although the source of the leaks are never identified, for the Doctors to receive a barrage of unfavourable press prior to any hearing. A media presence seems to defy any traditional notion of contempt of court, or right to a fair trial, as Doctors are subject to a total monstering and humiliation in the media. But it is not uncommon for papers in the English media, and their class of readers, also to subject groups of Doctors, such as EU Doctors, to an utter monstering as well, allowing xenophobia and outright racism to flourish. The scope for moral panic is enormous. But to lay these problems at the foot of the GMC, I feel personally, is unfair.
The GMC indeed also has an important statutory duty for patient safety under section 1 of the Medical Act 1983. The “There but the grace of God go I” used alarmingly frequently by white, English doctors on Twitter might reflect the observation that some Doctors are safer from attacks from institutional racism than others. This is particularly problematic if the NHS Trusts continue on its trend to trigger an official regulatory complaint effectively to cover their own backs rather than a genuine attempt to improve the performance, health and wellbeing of their Doctors employed under employment contracts. This has indeed been witnessed in the enforcement of the junior doctors’ contracts, arguably. Also, the “There but” observation is also problematic from the point of view that it seems to signal an admission that registers an admission that registered Doctors go to work knowingly taking risks and making mistakes. Most Doctors will admit to having taken risks and having made a mistake, and the number of mistakes reported daily in the NHS, a mere fraction of the real number, must urge a need for an open and transparent culture where people can learn from mistakes. But the GMC and the higher courts will tend not to tolerate any mistakes, or catalogues of error, whatever the mitigating factors. This might include an unblemished record for 30 years. The issue is that if the performance is way below a standard, there can be no excuse for it. If somebody has died, the threshold for mitigation has to be high, most reasonable persons might argue. And if a court of law has found someone guilty of manslaughter, whatever the process involved for doing so or the people involved, it is hard to leave no sanction on the Doctor, it is argued, whatever the need for organisational learning. Both the GMC and higher courts have consistently argued that public trust and confidence in the medical profession are more important than any individual doctor’s career.
The argument that ‘We go to work and are caught between a rock and a hard place’ merits scrutiny too. This comes down to the nature of how a crime is satisfied in English law – there can be intention to do the crime, and, although there is some finesse about the jurisprudence, there might be recklessness. The law in this is fairly well settled since R v Adomako. It might seem unfair to blame a Doctor having to cover seven bleeps one morning, but the point in law is that the Doctor by carrying those bleeps has assumed a duty of care to his or her patients, and any breach therefore of this duty of care, given the issues of causation and remoteness, is negligence. It might be argued that in tort the Doctor has assumed this responsibility under duress, but in reality most Doctors pick up the bleep from an office in the Hospital without any altercation. And Doctors are entitled to resign if they feel that there has been a fundamental breach of a contract, including a bilateral feeling of trust and confidence, between employer and employee. In reality, Doctors never do, despite the potential risks for patient safety.
Whilst there might be outrage about the lack of due emphasis on organisational learning, this organisational learning nor indeed any individual duty of candour are operational at any meaningful statutory level, meaning they exist in an Act of parliament or statutory instruments. And nobody is above the law. If there had been no sanction on #GawaBarba, a possible interpretation might have been that mistakes, whatever the reason, are excusable because of the ‘state of the NHS’. It might then be argued that the correct course of action might be for corporate manslaughter against the Secretary of State for health and social care, for ‘avoidable deaths’, but this has to be proven beyond reasonable doubt – an incredibly difficult offence to fulfil, as the late Prof Gary Slapper I am certain would testify.
I doubt, if #BawaGarba finds herself back on the GMC Register, she will find it easy to find employment again, especially with at least a five year gap in training. The GMC, even with its statutory duty for education and training, as well as patient safety, seems pretty indifferent to the professional rehabilitation and retraining of Doctors put back onto their Register. But the observation that no Doctor can ever be professional rehabilitated does concern me, even with the strong emotions that the ‘punishment should fit the crime’, and the need for a scalp can be overwhelming. For example, #BawaGarba has found that her subsequent good performance had become somewhat irrelevant as far as the regulator and higher courts were concerned.
As the old trope provides, there are no winners. There are only losers. It’s said that the GMC ‘doesn’t do personal’ in the same way a sanction is delivered in the same way a parking ticket is issued, and the GMC’s purpose isn’t, it is argued, to do ‘show trials’. The GMC’s position is that they are not in the business of ‘punishing Doctors’, but, I feel, it is of concern that unintended consequences, including a culture of fear, could continue to be dominant in the medical profession. The GMC doesn’t likewise, perhaps reflecting their perceived concerns from the general public, want to allow free rein on Doctors ‘free to make mistakes’, and good doctors will argue that they are all trying to do the job to ‘the best of their abiility’. The problem facing the GMC is whether ‘the best of someone’s ability’ is simply good enough. The general approach is that there is no shortage of doctors, and it is a honour to be a registered doctor. Whether there is a sufficient number of doctors for the demand is a concern the GMC can decide to involve itself with, or not. There is a clause in the code of conduct – Good Medical Practice, 2013 – stating that it is the responsibility of doctors to identify any shortfall of resources. I doubt all the senior Consultants or even STs in training taking to Twitter outraged about the #BawaGarba judgment are writing this morning to the GMC to warn about shortage of resources in their own hospitals, despite concerns about patient safety. It is noteworthy that the GMC in their statement on the case mentioned this only yesterday even. But individual Doctors have also been rather effective at protecting their own backs?

Time to call out dementia friendly cronyism

Whenever there is a restricted number of participants in a crowded market, the quality of the product tends to fall as the participants collude with another.
The botched performance of Carillion is a reminder that it’s often the same people on the same management boards of the same companies supposedly competing with another. And it’s the same for certain charities, with the same workforce with different operating brands, simply faking diversity, but in reality offering zilch thought diversity.
Dementia is not of course political, unless you include the ‘chosen ones’ performing very well in the Queen’s Honours List. I really feel it’s time to call out the nonsense of certain ‘dementia friendly’ brands, such as ‘dementia friendly emergency departments’.
I actually have no ideological objection to an enhanced ‘customer experence’ of a patient in an emergency department, but the hijacking of ‘dementia friendly’ a certain way has led to this construct meaning a better customer experience rather than, say, promoting the health of people with dementia and care partners.
There is a ridiculous secondary gain for charities to award scarce resources to fund research into dementia friendly emergency departments so that a few press releases can go out to comfort us all. Forget people with dementia dying while waiting for hours for an ambulance. Ignore people with dementia waiting for hours on a trolley waiting for a hospotial bed, or waiting for hours for transport to go home.
I am basically appalled by how relaxed some principal investigators in research, who are regulated by professional bodies, appear to be in declaring their financial competing interests when publishing academic papers, particularly in areas where these interests affect diagnosis or treatment of dementias.
I am worried how regulated professionals do not appear comfortable about speaking out about unsafe level of resources for dementia care, particularly if they are worried about their research monies being threatened.
The sheer contempt for specialists in dementia seems to predate the hatred of experts which accompanied the Brexit debate. For example, I don’t feel that the culture is healthy enough for us all to have a meaningful debate without causing offence and outrage about the difference between minimal cognitive impairment and dementia, or the heterogeneity within dementia, when I know of at least two people with dementia who will have published books on living with dementia by the end of next year.
The atmosphere really has become quite threatening for some specialists now afraid to voice opinions, with tropes such as ‘people with dementia and care partners are the real experts’. As it happens, I am a full time carer of someone living with dementia too. But it worries me that in the forthcoming APPG consultation on ‘dementia rights’, something I myself wrote a book chapter on in 2015, it will be exactly the same usual suspects, with exactly the same ‘empowerment and engagement’ causing exactly the same stale predictable narrative.
But we do need people to speak out on important issues, on why certain people find it so difficult to obtain an assessment for legal power of attorney following diagnosis, or how people with dementia might interact with the law if it feels that certain decisions need to be made in their ‘best interests’.
We need to discuss whether people have equitable access to medical and legal opinions. Simply airbrushing these discussions due to convenient pseudo-consultations which don’t ask the right questions from certain people, because of dementia friendly cronyism, is not right.
I think the atmosphere of how dementia care and research are evolving is really not right at the moment, and needs urgent attention. It’s when it’s a case of ‘who you know’ rather than ‘what you can contribute’ then you need to worry.

Jeremy Corbyn and the whole of Labour has become the ultimate nightmare for the Tories

As Emily Thornberry said this morning, “There is nothing stronger than a person of principle…. Thanks to Jeremy Corbyn’s inspirational leadership, and the efforts of all the people in this room, it’s time to put Labour values back into government.” Everything has now in fact changed. This is not merely because the Conservative party, and their bullshit such as £350 million re-invested in the NHS, is a ‘busted flush’. It’s much more than that. I first went to the Labour party conference in 2010 in Manchester. It was in fact a few months before my father was to die. I remember my time there crystal clearly. I remember meeting John Prescott for the first (and only) time in a curry restaurant in the Curry Mile, and various people who were both very young and very energised about being in the Labour movement. David Prescott kindly helped me across the street, avoiding being run over by the trams. I had become newly physically disabled at the time, due to meningitis. In fact, I remember going to a fringe event at breakfast time in Manchester Town Hall on the subject of how to engage ‘missing voters’. Ellie Mae O’Hagan was there. Some brilliant contributions from Matt Zarb Cousin stuck in my mind. I wonder what happened to him.
At the time, I was in the ‘top ten’ Labour blogs. But now is much better. I think this Labour conference in 2017 in Brighton is full of optimism and hope. Labour for the first time in ages, I feel, has a realistic chance of being the party of government. I think we very mostly agree Jeremy Corbyn has turned ‘pro’. He batted away questions on striking from Andrew Marr with amazing ease yesterday morning. The hacks have made it an open secret that they have no conflict to discuss. The observation that Brexit is not one of the motions for debate is the only thing that desperate hacks can cling onto, but you only have to look at the list which has emerged – which includes the NHS, social care, growth and investment and employment issues – to see that there is no existential crisis in the Labour Party. Not at all. It is a party which is prepared to govern for the many, not the few.
The Tories’ economic model of delivering shareholder dividend with rocketing prices, suppressed wages with inflated cost of living, is not appealing to the vast majority. The ‘work til you drop’ approach is terrifying. The way in which disabled citizens have lost their personal independence payment is nothing short of the ultimate in unacceptable morally. Corrupt capitalism has had its day. Grenfell paid testament to that. Outside of the hall, it is very clear that many delegates have been speaking to some of ‘the many’. There has been a strong sense from speakers from the floor to speak out about issues of social justice, in the quest for equalities and fairness. There has been reference to homeless people, which Tony Benn famously used to congratulate market forces for. There has been a clear drive to reset the narrative to appreciate and value migrants and asylum seekers. The Momentum festival has been well received. There is no sense that Polly Toynbee needs to visit it to provide it with external validation. Trade unions defend public services, campaign to prevent abuses of workers and employees, and are no longer a ‘dirty word’.
I voted for Jeremy Corbyn twice as leader of the Labour Party, and, like many, it is tempting not to forget so easily the time which has been wasted in setting out the case for Corbyn again and again and again, the carping and criticism from 170 or so Labour MPs, or the whingeing from senior people in the Labour Party keen to ‘blame’ Corbyn for Brexit. Nor is it quite so easy to forgive and forget the amount of time, effort and money taken by the NEC to stop people voting for Corbyn as leader out of fear that all the new members of Labour were Marxist throwbacks from the 1980s. But the surge in membership of the Labour Party is entirely genuine, making Labour a massive democratic party. This is an especially amazing achievement, given the context of how parties such as ‘Alternative for Deutschland’ with an anti-Muslim and anti-migrant, far right, agenda have garnered support to fill the ‘political space’. True that the Labour Party is not entirely a socialist party, although it has socialists in it. But it is also true that there are many more people are loud and proud to be associated with the socialist ideals and values which have been promoted by the current leadership of the Labour Party.
Whilst the ‘we want a Jobs first Brexit’ is in danger of being a vacuous phrase, there’s no doubt about the dependence of certain sectors, not least the NHS and social care, on EU citizens living in Britain. If it turns out that the Conservatives are simply unable to negotiate a meaningful settlement with the European Union within two years, it is quite possible that the Labour Party will have to do something drastic about deciding upon a post-Brexit future. Jeremy Corbyn openly explained on #Marr yesterday that it was possible that state aid rules had not made it possible to intervene in industries as he would have liked, and actually had helped to privatise certain industries such as rail. It wasn’t that long ago, after all, that there had been concerns about how TTIP might stitch up a trade deal with the US over the NHS, but now the threat to the NHS from Donald Trump and Jeremy Hunt is far greater. Free movement of workers has had problems also with employees, particularly of multi-national corporates, effectively leading to wage suppression, but this fundamentally was always a problem presented by employers. But Labour is well aware that the UK economy could easily tank on Brexit especially on leaving membership of the signatories to the rules of the “single market” or “customs union”, and the devaluation of the pound sterling and exodus of jobs abroad are both already alarming. But if you think to choose who you want driving the car – Boris Johnson, David Davis and Priti Patel or Sir Keir Starmer, I know who I prefer.
Members of the media have consistently been spitting bullets at Corbyn. James O’Brien on LBC spent substantial daily effort into rubbishing Corbyn. The 2017 Labour manifesto was a massive triumph, propelling Labour to its largest vote this century. The Tories claim they even put Jeremy Corbyn on the ballot paper the first time around. Various people sneered at the rallies held by Corbyn across the country, claiming simultaneously that Corbyn had a ‘bunker mentality’ which prevented him from meeting the general public, and saying that there was no such social movement. But it is clear that there is something material and significant happening under the RADAR, as Jess Phillips, Clive Lewis and Laura Pidcock are treated like rock stars rather than members of parliament. Paul Mason, I remember, was often criticised for claiming that “strong and stable” Theresa May would not be returned with a stonking majority, and Paul Mason’s views and opinions, for example, on topics ranging from tuition fees to bellicose nuclear speak from Donald Trump are taken with considerably more gravitas than other commentators. The whole team are pretty awesome now, including Barry Gardiner who is prepared to call out people talking nonsensical crap.
Gains such as Canterbury and London Kensington and Chelsea have been amazing. Amber Rudd’s seat in Hastings is now up for grabs. Nobody can fault how amazing Andy Gwynne has been. Of course, much blood has been spilt and this is to be expected from a broad coalition of sorts. I no longer speak to the Socialist Health Association because of their open support for marketization of the NHS, PFI and Owen Smith. Tom Watson is no longer on Len McCluskey’s Christmas card list. I think critics within Labour have really got the work cut out if they wish not to help Jeremy Corbyn and the Labour party prepare for government. You can tell from the reception to the limp interventions from Ben Bradshaw and Heidi Alexander over the single market that they are not the future now. But supporters of Labour fundamentally know that they did not introduce austerity. Vince Cable, on the other hand, did. The Liberal Democrats cannot be absolved from their blame on the bedroom tax, either. The Fabians, with their star turns, are having trouble trying to reverse the deluge of criticism they have doshed out to Corbyn and colleagues. The Twitter community, with Chunky, Rachael, Steve, Matt, Tom, Peter, Liam, “Scouse Girl”, EL4JC, Michael, WowPetition, Éoin, Matt, Ellie, or Paul, of course going from strength to strength. Labour’s policies speak to the concerns of the many not the few – such as personal debt, only today, being worked up by John McDonnell and Rebecca Long-Bailey. I agree with Jeremy Corbyn that he will need at least two terms of government to get the UK back on course, but there is a real sense of energy, positivity, drive and optimism which means that Labour and its social movement deserve every success.
