Home » Posts tagged 'section 75'
Tag Archives: section 75
Campaigners – your NHS needs you!
Andy Burnham MP recently commented,
“David Cameron used to say that his priority could be summed up in three letters: NHS. Now, it seems, he prefers not to talk about it. The word in Westminster is that, on the advice of Lynton Crosby, the Prime Minister has asked his ministers for a period of pre-election silence on the NHS. So the Queen’s Speech came and went without even a mention of Mr Cameron’s erstwhile priority.”
The NHS says 299,031 patients arrived at A&E departments last week – the highest number on record.
The NHS is set to be a key battleground at the general election and Labour intends to keep it at the forefront of the public mind in the coming months. The plan is now it will use a private member’s bill to lay out how it would repeal the coalition government’s controversial Health and Social Care Act (2012), which had a number of after shocks.
The bill, proposed by Clive Efford MP, would rewrite the rules that put competitive market tendering of services as the default option until proven otherwise. It will be debated in the Commons in November and Labour candidates in marginal seats will call on Tory and Lib Dem incumbents to back the bill, while highlighting examples of how current rules waste money and fragment care.
In fact, this legislative manoeuvre is necessary whichever party comes to power on May 8th 2015. The current legislative framework makes it very difficult for services to be commissioned which promote integration, for fear of breaching competition regulation.
The Shadow health secretary claimed the vote on the bill would “without doubt be the defining moment of what remains of this parliament”.
This private member’s bill is designed, presumably, to keep the NHS on the political and news agenda. Given the blanket reluctance of the BBC to discuss this £3bn re-disorganisation, campaigners will mainly have to resort to the social media to get their message across.
The bill is also designed to drive a wedge between the Conservatives and the Liberal Democrats. At some stage before the general election on May 7th 2015, the Liberal Democrats might wish to distance themselves from the current Conservative policy. It is nonetheless noteworthy that Paul Burstow remains adamant that opposition to hospitals suddenly closing from Labour will not work in the long run.
The Liberal Democrats, to put it simply, need this ‘differentiation strategy’ to survive. Otherwise, it will be completely annihilated as a political force. The Liberal Democrats were instrumental in getting the Lansley Act onto the statute books in both the lower and upper houses. The concept of them repealing their own legislation in a coalition after 2015 is completely unacceptable for many in the Labour Party.
And there is plenty that all NHS campaigners can unite upon, whatever political creed.
First and foremost, it would be motherhood and apple pie for the duty of the Secretary of State for Health for the National Health Service to be restored.
Secondly, it is likely that Labour will wish to see the increase in the ‘private patient income cap’ abolished. I have written about it in great detail here.
The current situation regarding the “private patient income cap” (more correctly an “income cap for non-NHS work“) in the Health and Social Care Act, through s. 164(1)(2A), is described as follows:
An NHS foundation trust does not fulfil its principal purpose unless, in each financial year, its total income from the provision of goods and services for the purposes of the health service in England is greater than its total income from the provision of goods and services for any other purposes.
In an interesting development reported this morning, hospitals are to be banned from charging patients up to £72 a day to park their cars under plans being drawn up by ministers. It is reported that some hospitals charge up to £4 an hour – and in some areas £72 per day – for parking spaces, with costs running to hundreds of pounds for those who make repeated visits for treatment.
It is also claimed that the worse-affected include cancer patients who cannot take public transport because they have reduced levels of immunity, and the parents of premature babies, whose children are often kept in hospital for several weeks.
The abolition of this lifting of the income cap for non-NHS work would go far wider than the Coalition’s targeted strike on car park charges.
A grave concern has been that competition rules ‘hold back quality‘. I first wrote about this at the beginning of January 2013 on this blog. The provision (“section 75″) puts rocket boosters into aggressive pimping of NHS services in the private sector, and the rest as they say was history.
In October 2013, it was reported that two NHS hospital trusts in Dorset would not merge on the basis of clinical need, according to the Competition Commission, an economic regulator overseeing the implementation of competition law applying to this country.
Whilst Jeremy Hunt never mentions the Lansley Act, there’s no doubt that Labour will wish to repeal it in the first Queen’s Speech of a Labour government. It appears to have appeared to have come from nowhere, though a very good description of how it came about comes from Matthew d’Ancona’s outstanding “In it together” and Nick Timmins’ outstanding “Never again”.
It’s undoubtedly a turgid piece of law, which reads like a patchwork quilt of commercial and corporate law relating to competition, regulation and insolvency. There’s only clause on patient safety, and that enables the abolition of the National Patient Safety Agency. In fact, the Draft Bill on regulation of clinical professionals, proposed by the English Law Commission, thought to be a landmark piece of legislation to promote patient safety, has been bounced into the lifetime of the next parliament.
Despite its length, the Lansley Act has three clear aims: firstly, to outsource NHS services into the private sector as easily as possibly, to bolster the functions of an economic regulator (“Monitor”), and to accelerate the managed decline of NHS units which run into financial trouble. It is indeed a result of a need to ‘liberalise the NHS market’, but as Iceland found out in their large experiment of deregulating the banks, the Lansley Act experiment may be just about to go horribly wrong. NHS campaigners, if they unite, can help to seal its fate.
Anybody who expects the Liberal Democrats to ‘save the day’ over the hospital closure clause is frankly deluding himself

Some people believe optimistically that the Liberal Democrats will suddenly have a change of heart.
The chances though of the Liberal Democrats joining Andy Burnham MP (see tweet) in the opposition lobby is about as likely as an ostrich landing on the moon.
The construct of ‘collective responsibility’ means that Liberal Democrats in Government vote with major Coalition party. It was Nick Clegg who predetermined that the Liberal Democrats would go into office with the party with the most number of seats. That was a fairly safe prediction at the time.
It’s widely predicted that irrespective of whether there is a hung parliament on the morning of May 8th 2015 that Labour will have the most number of seats. This is particularly more likely given the boundary reforms which the Conservative Party failed to achieve. That being the case, it raises the possibility of Nick Clegg being the Deputy Prime Minister, and the Liberal Democrats in office, for about a decade despite having never ‘won’ two elections.
It also raises the possibility of Liberal Democrat votes being used to repeal legislation from the lifetime of this parliament, albeit that no party can legislate to bind its successors. But the idea of the LibDems suddenly having a change of heart, to differentiate themselves as per the “differentiation strategy”, is scuppered by three prominent issues.
Firstly, the major thrust of any Government is its economic policies, and the LibDems have already indicated that they can only sign up to aggressive deficit reduction. This could be fine of course if Ed Balls offers the same meat but with slightly different gravy.
Secondly, the recent history of the Liberal Democrats is more than clear. They have got rid of the “social” bit in “The Social and Liberal Democrat Party”. Nick Clegg, having trained under Leon Brittan in the EU, has a competitive neoliberal philosophy, and he mixes in the company with people who share his zest for that sort of thing. Like David Laws. He would with Chris Huhne. A neoliberal firestorm in closing hospitals down due to failure régimes, of the type seen to by clause 118 is entirely in keeping with this neoliberal philosophy, not a social democrat one based on local democratic power.
Thirdly, there is no basis for believing that the Liberal Democrats will suddenly ‘come good’ as the term of this parliament comes to an end.
On 20th March 2012, the Commons voted the Health and Social Care Bill through at 10.15pm, spending less than 6 hours debating the 357 amendments made in the Lords. The Labour motion on disclosure of the risk register was lost by 328 to 246 votes. Two LibDems voted with Labour, Greg Mulholland and Adrian Sanders and three abstained. Most of the Lords amendments passed and the government won most by about 80-90 votes as the bulk of the Lib Dems voted with the government. The unpopular Health and Social Care Act came into law under this Government, though.
Also, despite near universal professional opposition and strong political pressure, the Section 75 regulations that explicitly open up the NHS to competition law were approved in the House of Lords A three-line whip on Liberal Democrat peers ensured a majority of over a hundred, with Baroness Shirley Williams speaking warmly of “an exciting new direction” for the NHS. This is the same Baroness Williams whom Tony Benn alleges in his diaries wished to tax benefits in the Callaghan government of the 1970s. The unpopular Section 75 Regulations came into law under this Government, though.
In January 2012, the government fought off a fresh challenge to its controversial welfare reform bill, when peers rejected a proposal to delay the full introduction of slashed new disability payments after ministers offered concessions. The unpopular Welfare Reform Act came into law under this Government, though.
As the cabinet hardened its tactics by agreeing to overturn a series of defeats in the House of Lords, a cross-party group of peers failed to introduce a pilot scheme before a new regime for disability allowances can be fully introduced. But Lib Dem cabinet ministers agreed with their Tory colleagues to overturn the amendments when the bill returns to the Commons.
Whilst it might suit some with social democrat ‘roots’ to wish the Liberal Democrat Party to ‘come good’, there is no evidence at all that would happen. Attempts to bring out this simple fact tends to become squashed with the attack that ‘Liberal Democrat’ votes are all to play for, and that LibDem MPs reading a fair discussion of this might change their mind from the party line.
LibDem MPs don’t work like that. Their motto, ‘fair society, strong economy’, is reflected in the UK only having performed very badly for three years and with the decimation of legal aid and law centres.
The hospital closure clause gives Trust Special Administrators greater powers including the power to make changes in neighbouring trusts without consultation. It was added to the Care Bill just as the government was being defeated by Lewisham Hospital campaigners, in an attempt to ensure that campaigners could not challenge such closure plans in the future. But the new Bill could be applied anywhere in the country.
Writing in the British Medical Journal, Professor Allyson Pollock said that that the clause would “undermine equal access to care in England” and removes “checks and balances designed to ensure that changes are in the interests of the communities affected” with Trust Special Administrators only having to consider market money.
Neoliberal means neoliberal. It means free movement of capital such that multinationals can buy parts of the NHS. It means everything is put out for competitive tendering. A social movement to pull on LibDems heart strings, with the unflappable Baroness Williams, will be a waste of time, but I suppose one should have dreams.
But dreams ought to be realistic. The Care Act, with its ‘closure clause’, will come into law, again only made possible through help of the Liberal Democrats.
We've just had a huge debate about the NHS. It's just a pity that it's been the wrong one.

Think of how much time we’ve just all spent, in thinking about the way in which services will be mostly put out for competitive tendering in the National Health Service. One of the first rules in law is that you fight your battles to the hilt, but, at first, you pick the right battles first. This is precisely what Labour appears not to have done. When Harriet Harman recently said on Question Time that the Conservatives are definitely not ‘to be trusted with the NHS’, Harriet curiously did not refer to the battle and war just won by the Conservatives (and Liberal Democrats) over NHS procurement. And yet the public desperately want Labour to stand up for the NHS. One member even suggested that, if Labour gave its unequivocal backing for restoring the NHS, Labour could even find itself with a massive vote winner.
Labour is clearly going through policy strands with a fine tooth comb, looking at, for example, the way in which multinational companies might employ workers at below the national minimum wage; effectively, controlling immigration through a wage policy. It does not appear to have worked out unequivocally whether it would reduce the rate of VAT, meaning possibly that the state borrowing requirement would temporarily increase. But do you see what they all did there? For days, weeks, or even months, we have been subjected to a relentless debate about EU immigration, when most surveys probably place the issue at number ten on the list of voters’ concerns. Unsurprisingly, the economy remains in ‘pole position’, but the ability of Labour to turn the opinion of the public, particularly in the South of England, away from the idea that Labour is ‘fiscally incontinent’ remains unconvincing. Labour is still considered to be the “tax and spend” party, for example, and Miliband appears painfully aware of that. So, when it comes to policy, there seems to be an odd combination of Labour shooting itself in the foot, or completely picking the wrong battles. And then you add in a complete inability to look at elephants in the room. Labour, to state the obvious, has no ability to implement any of its policies, if it is unable to win a General Election, and the confidence of Labour to win an election on its own is reflected accurately in Lord Adonis promoting his book that ‘if he were to form a new Lib-Lab pact, he wouldn’t start from here.‘
The NHS remains pivotal in Labour’s electoral chances, and Labour has been unable to use the resentment over the section 75 NHS regulations to maximise political capital. Why this should have happened in itself is interesting, as Andy Burnham, MP for Leigh, is a more than capable Shadow Secretary of State for Health. One of the issues is an ability to choose the right battle, possibly. Burnham, with some support from the right-wing media and thinktanks, has been banging on about integrated and whole-person care. Whether through conspiracy or cock-up, there will be short-term interest in how integrated care might be delivered. Think about a justification for State spending in the ‘mission impossible’ of implementing a NHS IT system. Why on earth would a right-wing libertarian government promote something which is national? Why on earth should you abort an ethos of ‘bonfire of the QUANGOs’ to introduce the biggest QUANGO in the country, viz NHS England? Whether you’re into conspiracy or cock-up, the integration of financial and medical information (including mental, physical and social care systems) allows for the perfect infrastructure for an insurance-based system. Insurance works on the basis of misrepresentation or non-disclosure to invalidate claims, so ‘big data’ serve a perfect storm for this. It won’t have escaped anybody’s attention that Labour (as indeed the Conservative Party) has been heading towards an insurance-based system for social care, so it does not require a massive ideological leap to think how this could be extended for all care with time. This does not involve any degree of paranoia, please note.
There is overwhelmingly an intellectual depravity in the bereft notion of producing policy through poll results and focus groups. New Labour clearly loved focus groups, with Philip Gould in ‘The Unfinished Revolution’ having devoted much airspace to developing a product in line with customers’ wishes. Of course, the Conservatives have a special affinity for polling organisations themselves, Nadhim Zadawi, in 2000 he co-founded YouGov and on its flotation became its CEO. YouGov is now one of the world leaders in political and business information gathering, polling and analysis. It employs over 400 staff on three continents and is listed on the London Stock Exchange. Again – it begs the question on why should Labour should wish to outdo the Conservatives on its own ability to use polling data? One of the polls which has become a toxic meme is how a high proportion of all voters would not mind who provides the NHS services, as long as it’s free at the point of use. However, this is intrinsically linked to other questions. Would you be prepared more in national insurance if it meant the NHS were able to provide a more comprehensive (universal) service?
It is indeed correct to state that the costs of renationalising the NHS might be overwhelming, although no accurate costings of this have ever been discussed properly. We do know, however, that the current cost of the NHS reorganisation is in the region of £3bn, but estimates of the actual cost inevitably have to be taken with a pinch of salt, as say the cost of Margaret Thatcher’s funeral. But to use this issue as a wish to stop discussion of this area is lazy, as one of the issues, as indeed as with Thatcher’s funeral, is that is this a sensible use of money compared to how it could be used elsewhere (so called “opportunity cost“)? Some people argue that the marketisation of the NHS has failed, in that any money spent on restoring a state-funded NHS would be money well spent. Restoring a state-funded service would get out of the idea of private companies being driven by maximising their profit margin, and not running a ‘more for less’ approach for delivering a service. Cynics might argue that the cost of restoring a state-run service is peanuts compared to waging a war abroad. Many remain unconvinced about the mantra that economic competition drives up quality, when it is the professional standards of healthcare staff, including doctors, nurses and allied health professionals, which appear to be at the heart of quality. The debate we have just had about the mode of procurement in the NHS was not one any of us as such elected; in other words, it has no mandate. If the Conservatives and the right-wing media appear so pre-occupied about having a referendum next parliament on our membership of the EU, many are (rightly) asking why Ed Miliband cannot ask for a mandate to take sensible decisions about the nature of the NHS. It is a given that there will always be a proportion of services which are outsourced to the private sector, but the question should be ‘how much’. Whilst a full-blown privatisation of the NHS has not happened yet, we have not even had a discussion of how much of the NHS should be outsourced.
And anyway Labour has to ask what really concerns all voters? In Mid Staffs and Cumbria, it is reported that there have been concerns about patient safety, and it may be mere coincidence that Labour failed to convince the voters in both places in the local elections over their offerings. However, there is certainly a ‘debate to be had’, about whether “efficiency savings” in the NHS are justified to produce surpluses in the NHS which get ploughed back into the Treasury (and therefore might be used for international overseas aid rather than frontline care.) Labour equally seems unable to look another ‘white elephant’ in the eye. That is of course the concept of a NHS hospital going bust. Should a NHS Trust which is in financial difficulty be simply allowed to go insolvent after a period of administration, or should the State pump money into it to maintain a local service to people in the community? This requires a fundamental reappraisal of how important “solidarity” and “social democracy” are, in fact, to Labour, and whether it wishes to use its extensive brand loyalty to have a mature, if sobering, discussion of the extent to which it wishes to fund a SOCIALIST National Health Service. Whilst in extremis it can be argued that a nostalgic return to ‘The Spirit of ’45” is not attainable, and is the wrong solution for the wrong times, there is a genuine perception that Labour has lost sight of its founding values. And why has this not been addressed in focus groups? It is well known that, in marketing, if you ask the wrong questions, you ubiquitously get the wrong answers.
Labour needs a mandate to confront these issues. And it should not be afraid to look for a resounding mandate, either. Whilst it might stick its fingers in its ears, and claim it’s nothing to do with them (arguing instead for integrated, “whole person” care), unless these ideological issues are confronted, NHS policy will continue to go down a right-wing path. For example, there is not much further to see GP ‘businesses’ being offered by the private sector, and the NHS pays for them; in this model, GP ‘businesses’ could operate under a standard 5-year contract, using NHS branding, under a ‘franchising’ model like Subway. And “The Tony Blair Dictum” is far from resolved, although currently there are issues more worthy of ‘firefighting’ in service delivery, such as the fiasco over ‘1111’. Labour’s problem is that it does not see the NHS as a ‘vote winner’, in the same way it doesn’t see the plight of disabled citizens experiencing difficulty with their benefits or people feeling genuinely threatened by ‘the bedroom tax’ as a top priority. Whilst Labour is unable to prioritise its issues in a way to align its aspirations with the concerns of the general public, there is no way on Earth it can hope to govern a convincing majority. If Labour wishes to learn a really useful trick from marketing, it could no better than to look at the ‘GAP analysis’ – looking at what the current situation is, and what the expectations of people are, and thinking how to get to a position of what people want. If people actually want a socialist universal, comprehensive NHS, paid for not in a private insurance system, Labour can be expected to work hard for a mandate to deliver this. If it doesn’t, that’s another matter, and it can witter on about whole-person care to its heart’s content.

We've just had a huge debate about the NHS. It's just a pity that it's been the wrong one.

Think of how much time we’ve just all spent, in thinking about the way in which services will be mostly put out for competitive tendering in the National Health Service. One of the first rules in law is that you fight your battles to the hilt, but, at first, you pick the right battles first. This is precisely what Labour appears not to have done. When Harriet Harman recently said on Question Time that the Conservatives are definitely not ‘to be trusted with the NHS’, Harriet curiously did not refer to the battle and war just won by the Conservatives (and Liberal Democrats) over NHS procurement. And yet the public desperately want Labour to stand up for the NHS. One member even suggested that, if Labour gave its unequivocal backing for restoring the NHS, Labour could even find itself with a massive vote winner.
Labour is clearly going through policy strands with a fine tooth comb, looking at, for example, the way in which multinational companies might employ workers at below the national minimum wage; effectively, controlling immigration through a wage policy. It does not appear to have worked out unequivocally whether it would reduce the rate of VAT, meaning possibly that the state borrowing requirement would temporarily increase. But do you see what they all did there? For days, weeks, or even months, we have been subjected to a relentless debate about EU immigration, when most surveys probably place the issue at number ten on the list of voters’ concerns. Unsurprisingly, the economy remains in ‘pole position’, but the ability of Labour to turn the opinion of the public, particularly in the South of England, away from the idea that Labour is ‘fiscally incontinent’ remains unconvincing. Labour is still considered to be the “tax and spend” party, for example, and Miliband appears painfully aware of that. So, when it comes to policy, there seems to be an odd combination of Labour shooting itself in the foot, or completely picking the wrong battles. And then you add in a complete inability to look at elephants in the room. Labour, to state the obvious, has no ability to implement any of its policies, if it is unable to win a General Election, and the confidence of Labour to win an election on its own is reflected accurately in Lord Adonis promoting his book that ‘if he were to form a new Lib-Lab pact, he wouldn’t start from here.‘
The NHS remains pivotal in Labour’s electoral chances, and Labour has been unable to use the resentment over the section 75 NHS regulations to maximise political capital. Why this should have happened in itself is interesting, as Andy Burnham, MP for Leigh, is a more than capable Shadow Secretary of State for Health. One of the issues is an ability to choose the right battle, possibly. Burnham, with some support from the right-wing media and thinktanks, has been banging on about integrated and whole-person care. Whether through conspiracy or cock-up, there will be short-term interest in how integrated care might be delivered. Think about a justification for State spending in the ‘mission impossible’ of implementing a NHS IT system. Why on earth would a right-wing libertarian government promote something which is national? Why on earth should you abort an ethos of ‘bonfire of the QUANGOs’ to introduce the biggest QUANGO in the country, viz NHS England? Whether you’re into conspiracy or cock-up, the integration of financial and medical information (including mental, physical and social care systems) allows for the perfect infrastructure for an insurance-based system. Insurance works on the basis of misrepresentation or non-disclosure to invalidate claims, so ‘big data’ serve a perfect storm for this. It won’t have escaped anybody’s attention that Labour (as indeed the Conservative Party) has been heading towards an insurance-based system for social care, so it does not require a massive ideological leap to think how this could be extended for all care with time. This does not involve any degree of paranoia, please note.
There is overwhelmingly an intellectual depravity in the bereft notion of producing policy through poll results and focus groups. New Labour clearly loved focus groups, with Philip Gould in ‘The Unfinished Revolution’ having devoted much airspace to developing a product in line with customers’ wishes. Of course, the Conservatives have a special affinity for polling organisations themselves, Nadhim Zadawi, in 2000 he co-founded YouGov and on its flotation became its CEO. YouGov is now one of the world leaders in political and business information gathering, polling and analysis. It employs over 400 staff on three continents and is listed on the London Stock Exchange. Again – it begs the question on why should Labour should wish to outdo the Conservatives on its own ability to use polling data? One of the polls which has become a toxic meme is how a high proportion of all voters would not mind who provides the NHS services, as long as it’s free at the point of use. However, this is intrinsically linked to other questions. Would you be prepared more in national insurance if it meant the NHS were able to provide a more comprehensive (universal) service?
It is indeed correct to state that the costs of renationalising the NHS might be overwhelming, although no accurate costings of this have ever been discussed properly. We do know, however, that the current cost of the NHS reorganisation is in the region of £3bn, but estimates of the actual cost inevitably have to be taken with a pinch of salt, as say the cost of Margaret Thatcher’s funeral. But to use this issue as a wish to stop discussion of this area is lazy, as one of the issues, as indeed as with Thatcher’s funeral, is that is this a sensible use of money compared to how it could be used elsewhere (so called “opportunity cost“)? Some people argue that the marketisation of the NHS has failed, in that any money spent on restoring a state-funded NHS would be money well spent. Restoring a state-funded service would get out of the idea of private companies being driven by maximising their profit margin, and not running a ‘more for less’ approach for delivering a service. Cynics might argue that the cost of restoring a state-run service is peanuts compared to waging a war abroad. Many remain unconvinced about the mantra that economic competition drives up quality, when it is the professional standards of healthcare staff, including doctors, nurses and allied health professionals, which appear to be at the heart of quality. The debate we have just had about the mode of procurement in the NHS was not one any of us as such elected; in other words, it has no mandate. If the Conservatives and the right-wing media appear so pre-occupied about having a referendum next parliament on our membership of the EU, many are (rightly) asking why Ed Miliband cannot ask for a mandate to take sensible decisions about the nature of the NHS. It is a given that there will always be a proportion of services which are outsourced to the private sector, but the question should be ‘how much’. Whilst a full-blown privatisation of the NHS has not happened yet, we have not even had a discussion of how much of the NHS should be outsourced.
And anyway Labour has to ask what really concerns all voters? In Mid Staffs and Cumbria, it is reported that there have been concerns about patient safety, and it may be mere coincidence that Labour failed to convince the voters in both places in the local elections over their offerings. However, there is certainly a ‘debate to be had’, about whether “efficiency savings” in the NHS are justified to produce surpluses in the NHS which get ploughed back into the Treasury (and therefore might be used for international overseas aid rather than frontline care.) Labour equally seems unable to look another ‘white elephant’ in the eye. That is of course the concept of a NHS hospital going bust. Should a NHS Trust which is in financial difficulty be simply allowed to go insolvent after a period of administration, or should the State pump money into it to maintain a local service to people in the community? This requires a fundamental reappraisal of how important “solidarity” and “social democracy” are, in fact, to Labour, and whether it wishes to use its extensive brand loyalty to have a mature, if sobering, discussion of the extent to which it wishes to fund a SOCIALIST National Health Service. Whilst in extremis it can be argued that a nostalgic return to ‘The Spirit of ’45” is not attainable, and is the wrong solution for the wrong times, there is a genuine perception that Labour has lost sight of its founding values. And why has this not been addressed in focus groups? It is well known that, in marketing, if you ask the wrong questions, you ubiquitously get the wrong answers.
Labour needs a mandate to confront these issues. And it should not be afraid to look for a resounding mandate, either. Whilst it might stick its fingers in its ears, and claim it’s nothing to do with them (arguing instead for integrated, “whole person” care), unless these ideological issues are confronted, NHS policy will continue to go down a right-wing path. For example, there is not much further to see GP ‘businesses’ being offered by the private sector, and the NHS pays for them; in this model, GP ‘businesses’ could operate under a standard 5-year contract, using NHS branding, under a ‘franchising’ model like Subway. And “The Tony Blair Dictum” is far from resolved, although currently there are issues more worthy of ‘firefighting’ in service delivery, such as the fiasco over ‘1111’. Labour’s problem is that it does not see the NHS as a ‘vote winner’, in the same way it doesn’t see the plight of disabled citizens experiencing difficulty with their benefits or people feeling genuinely threatened by ‘the bedroom tax’ as a top priority. Whilst Labour is unable to prioritise its issues in a way to align its aspirations with the concerns of the general public, there is no way on Earth it can hope to govern a convincing majority. If Labour wishes to learn a really useful trick from marketing, it could no better than to look at the ‘GAP analysis’ – looking at what the current situation is, and what the expectations of people are, and thinking how to get to a position of what people want. If people actually want a socialist universal, comprehensive NHS, paid for not in a private insurance system, Labour can be expected to work hard for a mandate to deliver this. If it doesn’t, that’s another matter, and it can witter on about whole-person care to its heart’s content.
The section 75 NHS regulations exposed muddled thinking all round; but is there really no alternative?
It’s easy to lose sight of Labour’s fundamental question in terms of the economic model; viz, whether the State should, in fact, intervene in any failing #NHS healthcare (in a financial sense). That is what distinguishes it from neoliberal models of healthcare, including the New Labour one. It is a reasonable expectation that the healthcare regulators will uphold professional standards of the medical and nursing professions, whether in the public or private sector.
One of the most memorable experiences in my whole journey of the section 75 NHS regulations was Richard Bourne, the Chair of the Socialist Health Association, asking me what would probably happen at the end of the day. I originally replied saying that I was not an astrologer, but, as I thought about that question more, I became totally convinced it was a very reasonable question to ask. In management, private or public, when one is uncertain about the outcome, a perfectly valid tool is the ‘scenario analysis’, where one considers the various options and their likelihood of success. Also, if you really don’t know what the eventual outcome is, which might be the case, say, if you have to produce a complicated budget for the whole of the next year, you can to some extent ‘hedge your bets’ by doing a rolling forecast which updates your plan on the basis of virtually contemporaneous information.
Section 75 NHS regulations had become a very ‘Marmite issue’. Richard was right to pick up on the fact that the world would not necessarily implode with the successful resolution by the House of Lords of the second version of the regulations. On the other hand, the event itself marked a useful occasion for us all to take stock of where the overall ‘direction of travel’ was heading. Wednesday’s charge, led by Lord Phil Hunt, was as ‘good as it gets’. Reasons for why Labour in places produced a lack lustre attack is that some individuals themselves were alleged to have significant conflicts of interest, or some elderly Peers were unable to organise suitable accommodation so that they could negotiate the ‘late night’ vote. Lord Walton of Detchant, whom all junior neurologists will have encountered in their travels at some point in the UK, said convincingly he had a look at the Regulations, and felt that they would be OK even given the ‘torrent’ of communication he had personally received about it.
I certainly don’t wish to rehearse yet again the arguments for why the section 75 NHS regulations appears to be farming out the NHS to the private sector, but in the 1997 Labour manifesto, where Tony Blair was likely to win, Labour promised to abolish the purchaser-provider split. It didn’t. Labour likewise is promising now the repeal the current reincarnation of the Health and Social Care Act. It might not. There is substantial brand loyalty to Labour, over the NHS, such that the Conservatives would find it hard to emulate the goodwill of the public towards it that is shown to Labour. Given that the market has been implemented in the NHS, the Conservatives and Liberal Democrats are now arguing that they wish to make the market ‘a fair playing field’, which is of course a reasonable aspiration provided that a comprehensive NHS can be maintained for the public good.
Many have no fundamental objection to running a NHS most efficiently. I often find that health policy experts who have little clinical knowledge find themselves going on wild goose chases about efficiency in the NHS. For example, I remember the biggest barrier to progressing with a patient with an acute coronary syndrome is that it would be impossible to get a troponin blood result off the HISS computer system for hours, such that you would be forced to track somebody down from the laboratory itself. Co-ordinated care can mean better care. The best example I can think of is where a GP prescribes Viagra for a man with erectile problems in the morning, the patient collects all his new medication from the local chemist, the patient then takes the first tablet around lunchtime, the patient has sex with his partner in the evening, but unfortunately attends A&E in the evening for angina (chest pain). Modern advice (for example here) would argue that an emergency room should take a very cautious approach in administering nitrates, a first line medication for angina, within 24 hours of a dose of viagra. What a Doctor would do in this particular scenario is not something I wish to discuss, but it is simply to demonstrate that patient care would benefit from ‘joined up’ operational processes, where the emergency room doctor had knowledge of what had been prescribed etc. that day.
So, it probably was no wonder that there was ‘muddled thinking’ all round. Baroness Williams is a case in point. She acknowledges that many in the social media think that she personally, with the Liberal Democrats en masse, has ‘sold out’ on the NHS. And yet she talks about a deluge of misinformation from organisations such as 38 degrees who cannot be shot for being the messenger for a concerned public; that presumably is consistent with the Liberal Democrats yearning for ‘a fair society’? Lord Clement-Jones attacked the person not the ball, advancing the argument that lawyers will always provide a legal opinion which favours the client. However, many agree with David Lock QC in his concerns on how the legislation could be interpreted to go further than the previously existant legislation from Labour over the Competition and Cooperation Panel. Indeed, Labour in the late 2000s had tried to legislate for public contracts, with attention to how their statutory instruments might be consistent with EU competition law.
However, the muddled thinking did not stop there. Only a few people consistently explained why the regulations were a ‘step too far’, and it is no small achievement that the original set of regulations had to be abandoned. The general public themselves can be legitimately blamed for muddled thinking. The general impression is that they resent bankers being awarded bonuses, resent the explosion of the deficit due to the banking crisis, but did not wish the banks to implode. The general impression is also they are happy with the previously high satisfaction ratings of the NHS, do not wish the NHS budget to be cut, and yet do not want ‘failing NHS trusts’ to be shut down altogether. Meanwhile, the Francis report exposed sheer horror in how some patients and their relatives or families experienced care from the NHS, and there are concerns that similar phenomena might be exposed in other Trusts. All of this is totally cognitively dissonant with the idea of ‘efficiency savings’ in the NHS, with billions of surplus being given back to the Treasury instead of frontline patient care. The issue about whether private companies should be allowed to make a profit from healthcare is a difficult one, when compared to an issue of whether parents can have a ‘choice’ as to whether to send their children to independent schools. However, many members of the general public would prefer any profit made in the NHS to be put back into patient care, rather than lining the pockets of shareholders or producing healthy balance sheets of private equity investors. The section 75 NHS regulations has done nothing for a discussion about how to maximise patient safety, nor the value of employees in the NHS. Managers in the NHS appear to be pre-occupied with ‘excellence awards’, innovation and leadership, but appear to have lost sight of the big picture of the real distress shown by some working at the coal face in the NHS.
Monitor, the new economics healthcare regulator, has a pivotal part to play; but they are an economic regulator ensuring fair competition, so it is hard to see as yet how they can best secure value for the patient rather than dividend for the providers. This is a Circle to be squared (pardon the pun). Possibly the only way to ensure that the NHS does not become a ‘race to the bottom’ (where “I don’t care who provides my healthcare as long as it’s the most efficient” becomes “I don’t care who provides my healthcare as long as it’s the cheapest and delivers most profit for the private provider)” is to ensure that people who are clinically skilled are involved in procurement decisions, or in regulatory decisions. This is the only way where yet another one of Earl Howe’s promises might be fulfilled; that local commissioners can commission services, even if they are only available from the NHS, if it happens that ‘there is no alternative’. Possibly doom-and-gloom is not needed yet, but it cannot be said that Lord Warner did much to inspire faith as the only Labour peer to vote against Labour’s “fatal motion”. Many people did indeed share the sense of despair felt by Lord Owen before, during and after the debate. However, Labour has to react to the present and think about the future. It cannot rewind much of the past, for example current PFI contracts in progress. The public have already exhausted themselves with the debate over ‘who is to blame over PFI?’, where both Labour and Conservatives have contributed in different ways to the implementation of PFI, and there are still some who believe that the benefits of infrastructure spending through PFI are yet to be seen. But blaming people now is probably a poor way to use precious resources, and there is a sense of ‘in moving forward, I wouldn’t start from here.’ Labour has to think now carefully of what exactly it is that it intends to repeal and reverse. Its fundamental problem, apart from sustainability, is to what extent the State should ‘bail out’ parts of the system which, for whatever reason, aren’t working; but this is essentially the heart of the neoliberal v socialism debate, without using such loaded language?
Shibley tweets at @legalaware.
Mud sticks: the new s.75 NHS regulations once enacted will be the ultimate disaster

“Mud sticks”
The Canadian model is built on a recognition of the limits of markets in distributing medically necessary care. Most markets distribute goods on the basis of supply and demand, with price signals used to affect production and consumption decisions. When price drops, demand should increase, with a near-infinite demand for free goods. Conversely, with fixed supply and high demand, price should rise until enough people get priced out of the market to balance supply against this new (lower) level of demand at the new equilibrium price.
Yet health care markets stubbornly refuse to follow these economic laws. Economists have debated why this is so and whether they can force health care to behave in accordance with theory. In Canada, there is remarkable tension with power being devolved to the provinces, meaning that if anything goes wrong, it is hoped that central government can escape the blame.
This latest set of ‘top-down reforms’ of the NHS are estimated to cost £2bn, and the widespread perception is that the system has been thrown into chaos because of a lack of fundamental understanding of the pre-existing culture of the NHS and overcoming the “barriers to change”. GPs in the UK are likely to be the ‘fall guys’ for this failed implementation. When the US sneezes, the UK catches a cold. We can already see this phenomenon being rehearsed ad nauseam across the pond. For example, in a recent American blogpost, “Who is to blame for the current healthcare crisis?” , Dawn J. Lipthrott comments that, “Doctors are to blame when they try to make up loss by over-scheduling and growing careless, or by failing to communicate with their patients.
The devolution of power to the locality is critical in ensuring that as much blame can be directed locally as possible. Of course, the idea of real local democracy is an illusory one, when you consider the emotional trauma local residents of Lewisham or Mid Staffs, for example, have experienced.
The Royal Free Hospital in its guide to NHS Foundation Trusts writes,
“The introduction of NHS Foundation Trusts represents a profound change in the history of the NHS and the way in which hospital services are managed and provided. NHS Foundation Trusts are a new type of NHS Trust in England. They are part of the Government’s plan for creating a patient-led NHS. The aim of these reforms is to provide high quality care, shaped by the needs and wishes of today’s patients, in the most efficient way. NHS Foundation Trusts have been created to devolve decision-making from central Government to local organisations and communities so they are more responsive to the needs and wishes of their local people. They are also at the leading edge of many of the other reforms and improvements that are creating a patient-led NHS.”
Meanwhile, the scandal-hit Mid Staffordshire has just become the first NHS foundation trust to be put into administration, The sector regulator Monitor said it has appointed two trust special administrators to “safeguard the future of health services” currently provided at the trust.
The “Local Government Lawyer” magazine writes in February 2013:
“In conclusion, local authorities have unique powers to scrutinise NHS functions, to call for information and explanations, to question proposed plans, and to invite senior managers to attend and provide evidence. However unwelcome their attentions may be, they do have a responsibility to exercise these powers “positively and proactively”, and that includes recognising that the function goes beyond the occasional attention of well-intentioned but lay members, to include demanding the information and providing the professional resource and competence to be able to do the job effectively.”
The notorious Section 75 regulations – set the legal framework for NHS competition under the government’s health reforms. They have already been revised once, after opposition to an original version from both the Liberal Democrats and Labour.The original plans would have seen NHS trusts forced to ask private companies to bid for every service, even if commissioners were satisfied with the way it was being run by the public sector. The new revised regulations insist that Clinical Commissioning Groups must invite bids for services in all cases except those which they are sure can be provided only by the current provider. This will mean only the most difficult and expensive contracts will be held by public sector organisations, as private companies will say they are capable of providing all others.
The concerns were confirmed by a recent Lords committee, which said the revised rules were “substantially the same as the original regulations”. Although many members of the committee said the new wording was an improvement, they also warned: “The wide range of interpretations of the substitute regulations is, we believe, likely to translate into uncertainty about how they will operate.”
Even with the new section 75 NHS regulations, when the private providers take the CCGs to court over the tenders, and the judge rules against the CCG on the process grounds of openness, transparency, Wednesbury reasonableness or even proportionality, and there is a huge public outcry, the Department of Health can easily blame the CCGs for a failure in the procurement process, especially as they do not have a comparable skill-set for doing slick procurement. It is widely believed that the new regulations lack sufficient clarity, so that the litigation option outside Monitor can easily be exercised by private providers.
The LibDems, of course, don’t want any of the mud sticking to them. The Liberal Democrat Lords health spokeswoman Baroness Jolly said she had received assurances from health minister Earl Howe that critics’ fears about the revised regulations were unfounded, and that this would be made clear when healthcare sector regulator Monitor published its guidance on them. That news only came a day after a coalition of influential charities, including Marie Curie Cancer Care, Sue Ryder, and Help the Hospices issued a parliamentary briefing warning that the new rules could mean competitive tendering for NHS services becomes “mandatory in all but the most exceptional circumstances”. On the other hand, the controversial regulations should be withdrawn, according to the BMA ahead of crucial Lords debate on 24th April 2013.
Meanwhile, the media is already gearing up to blame the CCGs. In March 2013, it was reported that one in three GPs who are running new organisations that are about to be given £65bn of the NHS’s budget also help run or hold shares in a private healthcare firm, a study shows. The disclosure has sparked concern that such widespread conflicts of interest will threaten patients’ trust in GPs, who they may see as lining their own pockets out of public funds. Overall 426 (36%) of the 1,179 family doctors on a board of one of the 211 clinical commissioning groups (CCGs) in England have an interest in for-profit firms, including those providing common NHS services such as diagnostics, minor surgery and out-of-hours GP care, an investigation by the British Medical Journal (BMJ) found. Some of them, it is alleged, are senior directors of such firms, while others have a shareholding in major private health companies such as Harmoni and Circle Health, which already earn hundreds of millions of pounds a year for doing NHS work alongside local doctors.
As usual, the LibDems are ferreting around to make sure that none of the mud of the failed section 75 NHS regulations sticks ultimately with them. You have to be either beyond stupid or fraudulent to claim that the current regulations are workable, even with the veneer of ‘integrated care’, as CCGs will be forced into a competitive process unless there are drastic reasons. The whole situation has gone beyond pathetic now, and is not even worthy of a ‘The Thick of It” script. Mud sticks: the new section 75 NHS regulations once enacted will be the ultimate disaster.
My blogposts on section 75 NHS competition regulations and the current situation

Whatever the victories claimed by the political parties, it does not matter what the niceties are about how bids will be considered (integration, “best value”, etc.), it will virtually always be possible there should be a costly competition process. The regulations (made under Section 75 of the Health & Social Care Act [2012]) still require all NHS services to be put out to competition unless the commissioners can prove there is only one provider capable of delivering them. Far from putting competition ‘back in its box’ as some have suggested, these regulations open the floodgates to legal challenges outside of Monitor, and will lead to an extensive and expensive extension of privatisation in the NHS, causing a bitty disjointed service. Whenever you introduce transaction costs into anything, the bill goes massively up.
We are now in April, but since 7 January 2013, I have written a number of blogposts detailing the legal and policy implications of the Health and Social Care Act and the two statutory instruments pertaining to section 75. Soon Caroline Molloy (@carolinejmolloy) will be updating everyone on how you can get involved, such as writing to your MP or a Peer.
Here is a summary of what has been done and what remains to be done:
My main article from early January 2013:
Posts on the first statutory instrument SI 2012/057 which was later discarded:
National Health Service (Procurement, patient choice and competition) Regulations 2013: what is “best value”?
The legal issues in the statutory instrument (2013, No. 257) on NHS procurement in England
Possible letter to send to the Clerk of the Committee
VERY IMPORTANT. Tomorrow is the last day to the write to the Clerk about SI 257
A post on Lord Owen’s Bill and supported by Prof Allyson Pollock:
History:
Initial reaction to SI2013/057:
Rainbow coalition warns about section 75 NHS Regulations
Thank you very much for the positive feedback which I have kindly received for my work above.
Further reading material:
1. A cartoon which brilliantly explains in a nutshell the thrust of these NHS statutory instruments
2. Guardian article by Prof Bob Hudson
3. Open democracy article on amended section 75 regulations by Caroline Molloy
4. Expert legal opinions (commissioned by 38 degrees): original SI 2013/057 regulations and “No. 2″
6. Comments by experts (article by Caroline Molloy)
7. Lords scrutiny committee on No. 2
At this stage of the NHS privatisation, the pro-privatisation lobbies get more desperate



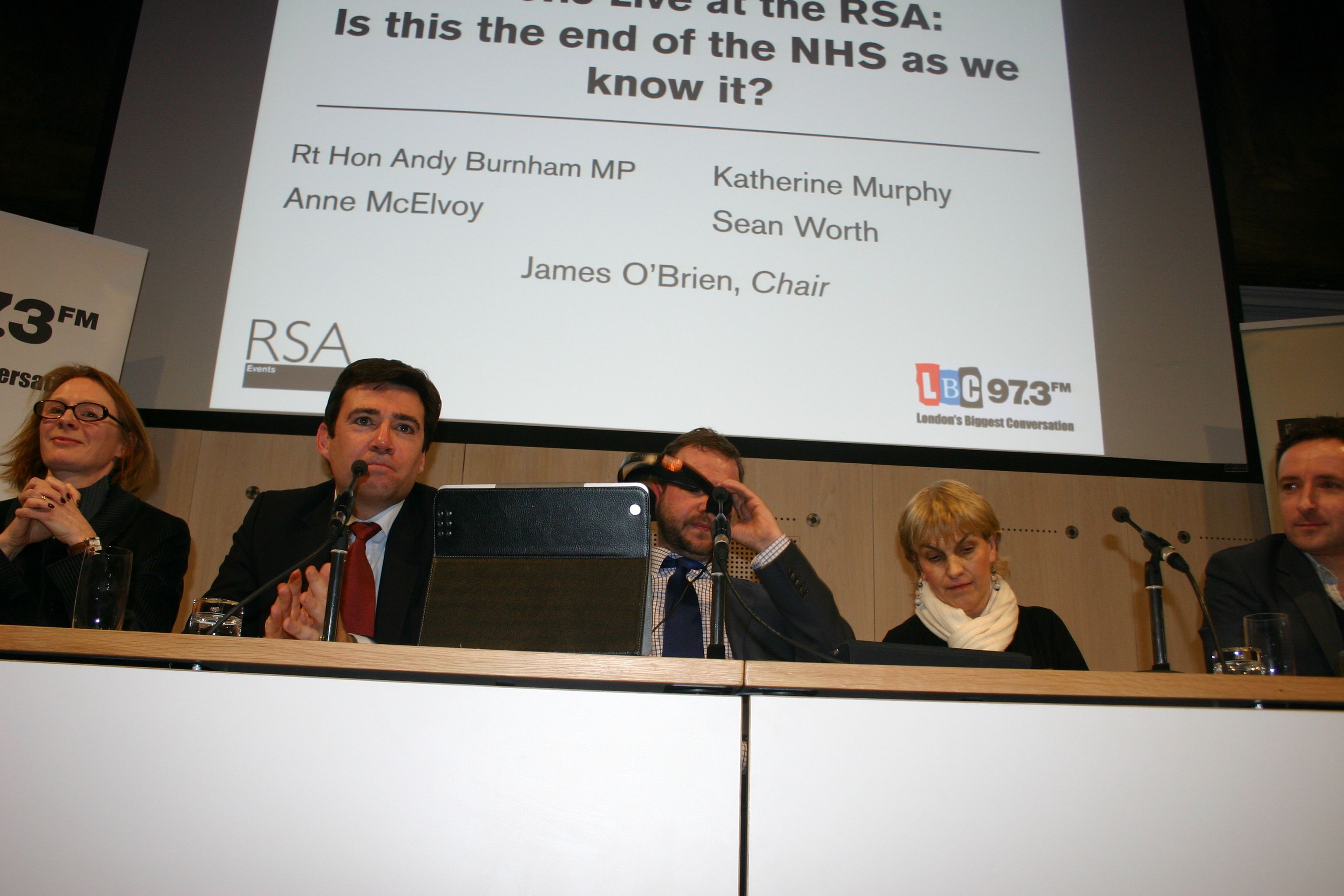
I went this evening to the RSA this evening to sit in the front row of the “LBC 97.3 Live at the RSA: Is this the end of the NHS as we know it?” debate. I’ve never seen James O’Brien chair a live debate, but I was genuinely impressed with how he managed to multi-task a live feed from Leicester Square and the debate at the RSA.
Speakers included: Sean Worth, Policy Exchange; Rt Hon Andy Burnham MP, Shadow Health Secretary; Katherine Murphy, chief executive, Patients Association; and Anne McElvoy, public policy and education editor, The Economist.
It seems as if there will, after all, be a window between April 22 2013 – when the Lords return – and May 7 2013, when time for ‘praying’ expires. In that period it will be possible in principle to have the regulations annulled. The regulations otherwise get enacted on 1 April 2013, and they will be implemented at any time thereafter.
With a mild irony, Sean Worth at the last minute took the place of the Government minister, Dr Dan Poulter. What struck me was how Sean Worth was completely undeterred from producing unmitigated garbage, from the perspective of anyone with a good grasp of macroeconomics and English health policy. He accused the Royal Colleges, which have a proud history of maintaining standards in and training of the medical professions, as “hard-left wing”.

This attempt to discredit the Royal Colleges was met with absolute disbelief and laughter from the audience. Whilst previously all stakeholder from the Doctors, in the form of the BMA, has been smeared as ‘left wing’, there is absolutely no evidence to show that the membership of the Royal Colleges have had any political motives. In a free and democratic country, you have to worry profoundly if any dissent at all on policy is due to you being on a different part of the political spectrum. Furthermore, in a totally disingenious argument, he tried to claim that any competition would be on the basis of quality not cost, but that is the whole point; in the absence of any meaningful information from Monitor, and the badly redrafted section 75 regulations, we have absolutely no idea how this “mumbo jumbo” will be put into action, nice though it sounds.
Anne McElvoy’s argument was that involvement of the private sector was to be welcomed, but in the absence of any detail how this would be implemented was utterly infantile. The problem is by producing an odd hybrid of private-public sector, without carefully policy measures, the market will be occupied by a small number of providers. Andy Burnham MP was indeed correct to call it ‘provider led’, because that is EXACTLY the problem with these type of markets with few providers, “oligopolies”, which exist to maximise shareholder dividend. McElvoy indeed shot down her own argument in flames when she tried to argue that she wished to aspire for comprehensive healthcare, while somehow reconciling some degree of rationing. So overall, McElvoy’s argument did not even make sense from a policy sense, let alone economic sense.
Andy Burnham put forward a convincing case for integrated care which concentrated on the “whole person” needs, including physical health, social care and mental care. He was quizzed quite carefully on how the ‘target-led culture’ might have been damaging, but Burnham as usual explained there had been some benefits of implementing targets for waiting times for surgery, for example. Burnham remained deeply apologetic about Mid Staffs, outlining the Government’s official response was tomorrow, but this is where I think he failed to join-up the argument with his original argument. Burnham had been arguing that the effect of the Health and Social Care Act had been to remove the ‘N’ from NHS – this is an extremely important point, as a privatised market, like the railways, will lead to reduced value for the end user, maximised shareholder dividend, and a fragmented service. Fragmentation matters, not least because of abolition of the Health Protection Agency clearly pivotal in public health, but also because of the abolition of the National Patient Safety Agency which was, arguably, even more important in the privatised NHS.
As for Worth’s claim that “competition saves lives”, Worth did not even bother to begin even his evidence for this bold claim, or even refuting a non-competitive service does not save lies (all students of logic will realise this is a false conclusion anyway.) Burnham correctly stated that there has never been any evidence that competition has improved inequality in healthcare outcomes. By that stage, Worth was looking as if he was throwing everything but the kitchen sink at the topic, but the claims sounded progressively more desperate as the evening progressed. All of this will not matter if the Liberal Democrats fail to mount an effective opposition to the new section 75 regulations, even though the legal advice has been that these new regulations will cause a mess in the law courts, with the Liberal Democrats relying on the dubious ‘kitemark’ of quality provided by Baroness Shirley Williams.
1. Sean Worth and “hard left organisations like the Royal Colleges”
Sean Worth describes accurately the starting point that “there are huge pressures on the NHS”; he says that there are “more babies being born and people living longer”. “Costs will rise”, and that there is also a big pressure posed by advances. “£600 million at least comes purely from advances in new medicines, but this costs us a lot of money. Whoever is in government faces the reality that NHS costs are going through the roof. We either put more money in or we reform it.” Worth uses patients to drive the justification for reforms, saying this is “What patients want; the Patients Association are right”. Worth claims that this has been a “big debate”, involving Trade Unions and hard left wing groups like the Royal Colleges”; this appears to have been driven “not out of what people want but because it meets their own needs”. Instead, Worth argues that people (presumably he means patients at this point) “want more choice in the NHS”. Worth claims that people say, “I don’t care who provides the care, all I want is good quality care.” However, Worth states that the discussion has become between Ministers and ideological groups. Worth said he had been part of the Government, and “not many people realise that, while the NHS is brilliant and is one of the best providers in the world, the system is of complete chaos.” Worth says that previously with 1: 5 hip operations having being done by a private firm there had been “no transparency”. Worth believes that patients are attracted by “The Tony Blair argument”, “where there aren’t give private sector perks, there’s a proper level playing field, and with patient choices not politicians driving change.
2. Targets and NHS culture
Burnham argues that bringing in a “top-down reorganisation” was the very worst thing to do at a time when the NHS was facing substantial financial pressures. The ‘reforms’ themselves brought in great instabiity into the workforce, according to Burnham. Mid Staffs was a “dark chapter”, and was a Trust that “lost the plot” when it became a Foundation Trust. Burnham feels that part of how this came about was through the Trust functioning independently. However, Burnham argues that he “brought Francis in” as an independent review, and agreed to all the original Francis recommendations; he adds that he expects Hunt to accept all the recommendations of the second Francis Report on 27 February 2013. McElvoy believes that “structural change is not the be-all-and-end-all”, and that some of the cultural change can be achieved by structural change; however some of the cultural change comes from ‘better management'; targets indeed were a ‘good start’ which were given a “bad name” through Mid Staffs.
3. A need for “comprehensive, universal” care?
McElvoy argues that universal care is a very good “guiding principle”, given that different jurisdictions have different priorities. However, “the NHS cannot do everything”. “We close to our eyes to the fact that a lot of elective treatments are being squeezed out of the NHS”, and McElvoy argues that we need to consider solutions to this (such as “co-payments” introduced by the last Government.”)
4. How do Bevan’s principles apply to the new NHS?
Bevan’s principles “meets the needs of everyone”, “free at the point of delivery” and “not based on an ability to pay”. Worth argues that the reforms “have to be put in place to preserve these principles”, that it is not possible to “keep pouring money” into the NHS; “without reforming these principles are gone”, “competition is not the answer, but in some areas it works’, and concedes competition can work in some areas. “If you want a NHS free-at-the-point-of-use, you have to pay for it, and that is a decision that politicians have to make.” However, Worth wants to avoid a situation of the 1970s, where “the Trade Unions and Labour Party run everything”. Burnham thinks the solution is ‘service reform’ conversely, cites clearly that more competition does not equal more efficiency: in the US, 18% of GDP is paid on healthcare, whereas it is 9% in the UK. Burnham argues that setting national pay levels helps to “keep a control on costs”. O’Brien summarises Burnham’s vision has a potential advantage of a “monolithic organisation”, but Burnham thinks competition introduces “division”. Instead, Burnham argues that a national strategy would help the NHS to be ‘cost-effective’. Worth then says that Labour introduced competition, but Burnham emphasises that he did so to increase ‘competition’.
5. Katherine’s Murphy introduction, including the NHS Patients’ Constitution
Katherine Murphy argues that the NHS Constitution must be “properly promoted”, but there is “little awareness” of it. “Access to services for all” and “not on the basis of an ability to pay” should be important from 1 April 2013. “Patients must have a right to be treated with dignity and respect”, but Murphy explains that still many patients access their confidential helpline. However, Murphy explains that people in the NHS must be “responsible for their actions.” “Patients want to be treated as equal partners”, however “there is a lot of work to be done for the public to understand the new system.” Murphy finally says that she is yet to see any information about what a CCG is, and why this reorganisation was necessary in the first place?
6. Anne McElvoy, a case for reform from a personal perspective
McElvoy explains that the impossible default position is that the NHS “never wants to change”, and it is impossible to keep on giving the NHS money irrespective of other areas. This leads to a situation where you have to make savings. McElvoy has noticed that, after Mid Staffs, “large chunks of the service are failing people”, and interventions are failing. McElvoy believes that “universal treatment can be maintained”. McElvoy says that “Cuba has 2 private hospitals, but we have one”, and that “we are not allowing competition”. “Tony Blair was a good example of seeing an opportunity here”. In conclusion, “things in the NHS are great… bad hospitals should be taken over by better ones.. we need to open it up to more providers… I don’t want a NHS to be run by whistleblowers when things go wrong’.
7. Andy Burnham, with his key criticisms of the Health and Social Care Act (2012)
“This Act removes the N from NHS” appears to be the core message that Andy Burnham wishes to impart to confused members of the public, but Burnham calls it ‘almost illegal’ that the reforms themselves have siphoned £3bn from frontline care as per costs of reorganisation. Burnham argues this on three fronts. Firstly, it removes the duty of the Secretary of State to provide comprehensive universal care, leading to a “postcode lottery”, citing for example the withdrawal of certain cataract operations. Secondly, Burnham believes that the Act legislates for the NHS to begin to mimic the US system, where half of the facilities can now be devoted to private operations, making the system more like the US system. Thirdly, this system mandates “competitive tendering” for all doctors. This is “telling what Doctors to do”, rather than “letting Doctors decide”. “All the evidence from all around the world is that competition does not save money”. “The N in NHS means that you can can save money”. The “recipe given by Sean is a recipe for fragmentation”, but Burnham wants a system represented by integration. With a National Health Service you are able to plan nationally for services, Burnham argues. “Nobody has given this Government to put the NHS up-for-sale.”
8. Patient choice: its importance (from the perspective of the “Patients’ Association”)
Katherine Murphy argues that in the current system “patients have very little choice”. According to Murphy, patients just want to be treated by compassionate doctors in their local hospital. O’Brien says that this is not a choice, and Murphy replies ‘absolutely’. Murphy says there is very little information, e.g. about the complaints mechanisms, about infection rates. Murphy “needs leaders who sign up to the values of the NHS who put the patients at the centre of everything which they do.”
And so the march of the NHS privatisation moves on. Unless the Liberal Democrats support the Fatal Motion,

it is likely that despite the public protest against this policy move (356578 e-signatures and still counting against the section 75 Regulations on “38 degrees”), the next stage of the privatisation plan will have been completed successfully (see here my original article here on this website.)

Please feel free to contact me on @legalaware if you wish to have a constructive debate about any of the issues therein. Many thanks.
Thanks to Caroline Molloy for truly ground-breaking campaigning on this issue: to read her latest blogpost on this blog, please see here.

How is parliamentary procedure being followed to take the previous statutory instrument on NHS procurement out-of-action?

A Statutory Instrument is used when an Act of Parliament passed after 1947 confers a power to make, confirm or approve delegated legislation on: the Queen and states that it is to be exercisable by Order in Council; or a Minister of the Crown and states that it is to be exercisable by Statutory Instrument. 1.15 pm last Tuesday (5 March 2013) saw Andy Burnham MP, the Shadow Secretary of State for Health, go head-to-head with Norman Lamb (The Minister of State, Department of Health). Lamb was invited to comment on the regulations on procurement, patient choice and competition under section 75 of the Health and Social Care Act 2012.
The discussion is reported in Hansard.
Lamb describes an intention to ‘amend’ the legislation
Lamb explains:
“Concerns have been raised that Monitor would use the regulations to force commissioners to tender competitively. However, I recognise that the wording of the regulations has created uncertainty, so we will amend them to put this beyond doubt.”
The problem is that this statutory instrument would have become law automatically on 1 April 2013, and still promises to do so in the absence of anything else happening. The safest way to get this statutory instrument out-of-action is to ‘annul’ the law, rather than having the statutory instrument still in force but awaiting amendment. Experts are uncertain the extent to which statutory instruments can be so easily amended, while in force.
Most Statutory Instruments (SIs) are subject to one of two forms of control by Parliament, depending on what is specified in the parent Act.
Fatal motion
There is a constitutional convention that the House of Lords does not vote against delegated legislation. However, Andy Burnham has said the exceptional nature of the Section 75 regulations, which force all NHS services out to tender, meant he needed to table a ‘fatal’ motion in the second Chamber. Indeed, Lord Hunt later tweeted that this fatal chamber had forced a rethink on the original Regulations:

The main effect of delegated legislation being made by Statutory Instrument is that it is effective as soon as it is made, numbered, catalogued, printed, made available for sale, and published on the internet. This ensures that the public has easy access to the new laws. This statutory instrument (SI 2013/057:The National Health Service (Procurement, Patient Choice and Competition) Regulations 2013) is still available in its original form, with no declaration of its imminent amendment or annulment, on the official legislation website here.
The “Prayer”
The more common form of control is the ‘negative resolution procedure’. This requires that either the Instrument is laid before Parliament in draft, and can be made once 40 days (excluding any time during which Parliament is dissolved or prorogued, or during which both Houses are adjourned for more than four days) have passed unless either House passes a resolution disapproving it, or the Instrument is laid before Parliament after it is made (but before it comes into force), but will be revoked if either House passes a resolution annulling it within 40 days.
A motion to annul a Statutory Instrument is known as a ‘prayer’ and uses the following wording:
- That an humble address be presented to Her Majesty praying that the [name of Statutory Instrument] be annulled.
Any member of either House can put down a motion that an Instrument should be annulled, although in the Commons unless the motion is signed by a large number of Members, or is moved by the official Opposition, it is unlikely to be debated, and in the Lords they are seldom actually voted upon.
Indeed, this is exactly what happened. Ed Miliband submitted EDM 1104 on 26 February 2013, which currently – at the time of writing – has 183 signatures – with the exact wording:
“That an humble Address be presented to Her Majesty, praying that the National Health Service (Procurement, Patient Choice and Competition) Regulations 2013 (S.I., 2013, No. 257), dated 11 February 2013, a copy of which was laid before this House on 13 February, be annulled.”
The purpose of “amending” the legislation
Lamb later provides in his answer:
“Concerns have also been raised that competition would be allowed to trump integration and co-operation. The Future Forum recognised that competition and integration are not mutually exclusive. Competition, as the Government made clear during the passage of the Bill, can only be a means to improve services for patients—not an end in itself. What is important is what is in patients’ best interests. Where there is co-operation and integration, there would be nothing in the regulations to prevent this. Integration is a key tool that commissioners are under a duty to use to improve services for patients. We will amend the regulations to make that point absolutely clear.”
How the Government “amends” the legislation is clearly pivotal here. Integration is another “buzzword” in the privatisation ammunition. Colin Leys wrote in 2011:
“In the emerging vision of the Department of Health, however, integrated care has always been associated with the drive to enlarge private sector provision, and the Kaiser [Permanente] connection emphasised this. The competitive culture attached to integrated care in the Kaiser model, coupled with the keen interest of private providers in all integrated care initiatives, were constants, and put their stamp on official thinking about the future NHS market.”
A possible reason for why this emphasis on competition has failed is that in other markets, such as utilities, rail and telecoms, there is a strong case that competition has not driven down cost at all, because of shareholder dividend primacy. Another good reason for people in favour of the private market to discourage competition is that competition might even inhibit a drive to integration, and integration is strongly promoted by private providers (and, incidentally, New Labour).
What does the Act itself say about ‘annulling’ statutory instruments?
According to s. 304(3), “Subject to subsections (4) to (6), a statutory instrument containing regulations under this Act, or an order by the Secretary of State or the Privy Council under this Act, is subject to annulment in pursuance of a resolution of either House of Parliament.” So, at the moment, we are clearly in limbo, with parliament yet to pass a EDM, and new redrafted Regulations yet to appear. However, it is still a very dangerous situation, as the original set of Regulations is still yet to be enacted on 1 April 2013.

My blogposts on Section 75 Health and Social Care Act and NHS England Procurement Regulations (SI 2013/057)

Since 7 January 2013, I have written a number of blogposts detailing the legal and policy implications of the Health and Social Care Act and the statutory instrument 2012/057.
These are on the “Legal Aware” blog.
Main article:
SI 2012/057:
The legal issues in the statutory instrument (2013, No. 257) on NHS procurement in England
Possible letter to send to the Clerk of the Committee
VERY IMPORTANT. Tomorrow is the last day to the write to the Clerk about SI 257
Lord Owen’s Bill:
History:
This one on stakeholder reaction is published on the ‘Socialist Health Association’ (independently authored) blog:
Rainbow coalition warns about section 75 NHS Regulations
