Home » Posts tagged 'privatisation'
Tag Archives: privatisation
Dementia care in the whole person care age
The Australian jurisdiction have recently provided some helpful inroads here.
The narrative has changed from one of incessantly referring to people living with dementia as a ‘burden’ on the rest of society. For example, to push a sense of urgency that we have an ‘ageing population timebomb’, the cost of the ageing people with dementia flies completely in the face of other public health campaigns which emphasise, for example, “dementia is not a natural part of ageing”.
“The NHS as a whole and individual hospitals recognise that dementia is a significant, growing and costly problem for them” is the opening gambit of the Alzheimer’s Society “Counting the cost” report.
An easy to use online resource, Valuing People from Alzheimer’s Australia has been developed in collaboration with community aged care providers who have helpful in stablishing a person centred approach to service delivery.
Person centred care is a development to provide ervices provided in a way that is respectful of, and responsive to, the preferences, needs and values of people and those in the care and support network.
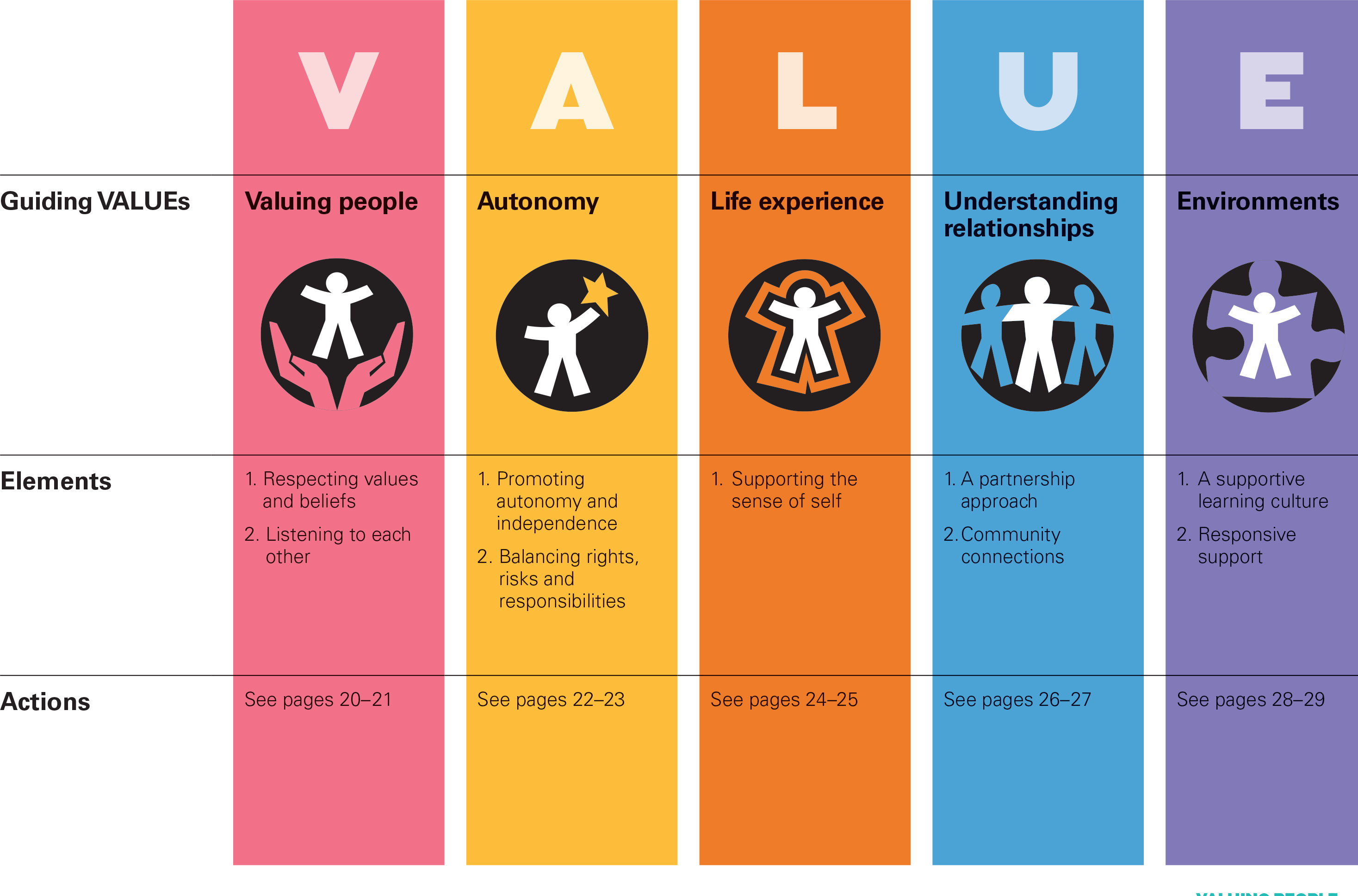
I cannot recommend this resource highly enough. The main source is here.
In fact, it summarises succinctly the conclusions I came to after my exploration of personhood in my book ‘Living well with dementia’. The late great Prof Tom Kitwood said of personhood, “It is a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being. It implies recognition, respect and trust”.
If a Labour government is elected on May 8th 2015, the first necessary step is to legislate for the repeal of the Health and Social Care Act (2012) and to enact new legislation to allow for integrated packages provided they are justified by clinical outcome. For this to happen, it will be necessary for Labour to undergo a ‘conscious uncoupling’ from all the baggage of EU competition law. For this, it is essential also that the UK government is able to carve out provisions from the investor protection clauses and/or the rest of the EU-US free trade treaty (TTIP).
The “whole person care model” has become attractive to those who wish to break down silos between different physical health, mental health and social care “silos”. It has been worked up in various guises by various parties.
A helpful construct is provided in the document, “Healthcare for complex populations: the power of whole-person care models” originally published by Booz & Company in 2013.
A major problem with dementia care, however it is delivered, is that it is full of divisions: public vs private care, fragmented vs national care, competitive vs integrated models. Operating in silos can’t work because of the nature of the dementias: the mood and cognition of a person with dementia profoundly affects how they might interact with the outside world, for example perform activities in the outside world. And we know that taking part in leisure activities can promote a good quality of life.
Their model is, though, a useful starting point.

Dementia cannot be only addressed by the medical model. In fact, it is my sincere belief that it would be highly dangerous to put all your eggs in the physical health basket, without due attention to mental health or social care. For example, last week in Stockholm, the international conference on Parkinson’s disease, a condition typified by a resting tremor, rigidity and slowness of movement, which can progress to a dementia, often is found to have as heralding symptoms changes in cognition and mood.
So it’s pretty clear to me that we will have to embark on a system of multidisciplinary professionals who could all have a part to play in the wellbeing of a person with dementia, depending on his or her own stage in life, and ability or need to live independently. “Care coordinators” have traditionally been defined incredibly badly, but we do need such an identity to navigate people with dementia, and actors in the care and support network, through the maze.
“Care collaborators” in their construct are very wonkily articulated, like “pre-distribution”, but the concept is not stupid. In fact it is very good. One idea is that people with dementia could act as support as other people with dementia, for people on receiving a diagnosis of dementia. The rationale for this is that people living with long term conditions, such as for example recovery from alcoholism, often draw much support from other people living with other long term conditions, away from a medical model. There needs to be safeguards in the system to safeguard against a lot of unpaid goodwill (which currently exists in the system.)
Informatics would have a really helpful rôle here, being worked up in telecare and assistive technology. But even simple disruptions such as a person living with dementia at risk of falling from problems with spatial depth perception being able to ‘hot email’ a care coordinator about perceived problems could trigger, say, an early warning system. And with various agents in the provision of care being involved in differing extents it will be up to NHS England to work out how best to implement a single accountable tariff. Falls are just the sort of ‘outcome metric’ which could be used to determine whether this policy of ‘whole person care’ for people living with dementia is working. And, even though everyone ‘trots it out’, the performance on avoided hospital admissions could be put into the mixer. It’s already well recognised that people with dementia can become very disoriented in hospital, and, and despite the best efforts of those trying to improve the acute care pathway, people with dementia can often be better off away from hospital in the community. But it’s imperative that care in the community is not a second-rate service compared to secondary care, and proper resourcing of community whole person care is essential for this before any reconfiguration in acute hospital services.
But the private sector has become such a ‘bogey term’ after arguably the current Government overplayed their hand with the £3bn Act of parliament which turbo-boosted a transfer of resource allocation from the public to private sector. Any incoming government will have to be particularly sensitive to this, as this is a risk in strategy for the NHS.
In October 2005, Harold Sirkin, Perry Keenan and Alan Jackson published a highly influential article in the Harvard Business Review entitled “The hard side of change management“. Whilst much play has in fact been made of politicians having to be distant from running the NHS, a completely lubricous line of attack when it is alleged that Jeremy Hunt talks regularly to senior managers and regulators in the NHS, the benefits of clear political leadership from an incoming Labour government are clear.
Andy Burnham MP has already nailed his colours to the mast of ‘whole person care’ on various occasions, and it is clear that the success of this ambitious large scale transformation depends on clear leadership and teamwork from bright managers. Take for example the DICE criteria from Sirkin, Keenan and Jackson:

But this is perfectly possible from an incoming Government. The National Health Service has a chance to lead on something truly innovative, learning from the experience of other jurisdictions such as Australia and the USA.
As alluded to in the new resource from the Alzheimer’s Australia, this cultural change will require substantial ‘unfreezing’ from the current mindset for provision of care for people with dementia. It will require a change in explicit and implicit sources of knowledge and behaviours, and will need to be carefully brought about by learning from the successes and failures of pockets of implementation.
The whole project’s pretty high risk, but the rewards for people living with dementia, and members of the care and support network, are potentially vast. But it does require the implementation of a very clear vision.
[First posted on the 'Living well with dementia' blog]
NHS campaigners know that state ownership is ‘box office’ stuff, and a perfect way to win hearts not just minds

Labour’s business spokesman, Chuka Umunna, uttered in January 2014: ‘The big difference between 1979 and 2013 is that we are all capitalists now.’ Is he right? Have the Thatcher and New Labour years changed everyone? And the Guardian ran a poll to see if their readers agreed with him.
In response to Ed Miliband’s conference speech last year, Jonathan Freedland mentioned that he had witnessed “a new and emerging strain of left populism”. For Freedland, “It confirms Miliband’s larger ambition: not merely to win power the Blair/Brown way, within parameters set by Conservatism, but to redraw those lines, to shift the centre ground itself leftward.”
Today, Simon Stevens takes over the rôle from Sir David Nicholson of leading NHS England. It is known that Stevens used to be a SpAd to Frank Dobson MP, a former Labour Secretary of State for the Health. It is alleged that he used to be, at least, a member of the Socialist Health Association. It is clear that there is some sort of crisis on the right about the unpopularity of privatisation, for example this short piece by Ryan Bourne is head of economic research at the Centre for Policy Studies. Latterly, I’ve felt the public respond very well to emotions-based campaigning rather than cognition-based campaigning. For example, rather than thinking for ages about whether it ‘matters’ whether the NHS is ‘operationally delivered’ by private companies, the general public are more concerned about ‘State assets being sold off’, or even private and public limited companies ‘are able to profit out of your illness’. But there is an overlap: privatised railways can offer poor value for the consumer in a fragmented service, whereas people intuitively like the idea of a nationally-run well-organised State-run transport service.
So it is therefore noteworthy that ex-Employment lawyer, and poster boy for responsible capitalism, is so critical of the Royal Mail sell off. Royal Mail for many epitomises the best aspects of socialism – i.e. it sends as much to send a first class letter to Crewe as it does to Cowes. Companies, thus far, had not been bickering on who is actually going to deliver the letters – who funds for the postman. So Chuka Umunna’s standpoint of criticising the Royal Mail flotation is clearly bound to be anaemic for socialists in comparison. And yet it’s clear that the privatisation of Royal Mail has benefited hardworking hedgies. Vince Cable said it had achieved its primary objective of selling the shares and reducing the risk to taxpayers, but the inherent risk in privatising NHS services, defined as fielding out them to the private sector, is surely greater? Calls for the resignation of Vince Cable, a former socialist, came after the National Audit Office said too much emphasis was put on rushing the sale, at the expense of value for money. Royal Mail shares are more than 70% higher than the 2013 sale price. Billy Hayes, general secretary of the Communication Workers Union, said it was a “botched, panic sale” and the business secretary “should consider his position”. The anger for many is that Royal Mail had become profitable in the public sector, and now transferring it to the private sector will in reality benefit certain stakeholders predominantly.
As opposed to the NHS ‘sale of the century’, it’s been mooted that new era of public ownership of the railways could save the Treasury more than £1bn a year and deliver improved services and lower rail fares for passengers. England’s fragmented railway system be gradually brought back into public hands as franchises expire or companies break the terms of their franchise agreement. This movement had intensified after the TSSA union argued that Network Rail bosses could earn more than £10m in bonuses over the next three years under a new scheme – as well as RMT figures showing that 65% of Britain’s rail operators are owned by overseas companies, with 60% owned by European state rail arms. Since privatisation nearly 20 years ago, the cost of train travel has risen by 17% compared to a 7% drop in the cost of motoring, while in recent years the bill for the taxpayer of running the trains has shot up by 2 to 3 times.
The “Great Train Robbery” is said to be a blatant transfer of public money to private interests at the expense of the taxpayer and rail passengers, who are forced to endure the consequences of a deeply complex and fragmented system while ticket prices get bigger and bigger. And going back to the ‘raw emotions’ of it it’s known that Clem Attlee was a hugely popular Labour Prime Minister, and saw the benefits of state ownership. Attlee became prime minister on 26 July 1945 as the leader of a Labour party that had won a landslide general election victory with a majority of 144 seats. His government was a transformational one. Its strategy of maintaining high levels of employment, with major industries under public ownership, was the governing model in post-war British politics until Margaret Thatcher’s Conservative government of 1979–90. And political parties do appear to swop ideologies – take for example George Osborne’s nostalgic return to full employment yesterday. Hot fast emotions are likely to make more impact than cold decision making, as recently discussed in the celebrated book “Thinking fast and slow” by Daniel Kahneman.
Tony Benn MP, much revered in recent days, was very scathing about the term ‘responsible capitalism’ in his final set of diaries, “An autumn blaze of sunshine”. Some call ‘responsible capitalism’ an oxymoron, as ‘responsible’ implies moral accountability while capitalism is driven by self-interest. Others insist that it defines the state’s obligation to balance social justice with individual freedom. And this is not trivial, as private investors seek to ‘pick winners’ through offering long-term debt finance through ‘social impact bonds’ for social enterprises. In truth, behind a bland phrase lurk there is quite a fierce discussion we mean by “socially responsible.” In Bush’s view, “socially responsible” means that large corporations should provide more jobs, pay better wages, compensate host communities for the burdens of resident corporations, stop polluting, and so on. And there is no doubt right to call these goals and objectives desirable. But Ed Miliband should not set his sights on ‘Being George Bush’ in a crazy form of ‘Stars in your Eyes’. NHS campaigners know that state ownership is ‘box office’ stuff, and a perfect way to win hearts not just minds. We may not be all capitalists now.
Will the war over NHS privatisation be won on the social media or on Question Time?
In his lecture for the LSE recently called “These European Elections Matter”, Nigel Farage explained how the 1999 European Elections had been a ‘gamechanger’. This election had apparently returned three MEPs, and Farage explained that this result had only been achieved through the method of proportional representation. Farage concluded that, despite no MPs, this had meant UKIP was suddenly being involved in contemporary political debates on the BBC such as “Question Time” or “Any Questions”.
The situation how the UK entered Europe is almost a counterpoint to the situation why people want the NHS to leave behind market dynamics. The United Kingdom referendum of 1975 was a post-legislative referendum held on 5 June 1975 in the United Kingdom to gauge support for the country’s continued membership of the European Economic Community (EEC), often known as the Common Market at the time, which it had entered in 1973 under the Conservative government of Edward Heath. Labour’s manifesto for the October 1974 general election promised that the people would decide “through the ballot box” whether to remain in the EEC. The electorate expressed significant support for EEC membership, with 67% in favour on a 65% turnout. This was the first referendum that was held throughout the entire United Kingdom.
There has never been as such a referendum on whether the market should be forced to leave the NHS, but many feel that this is an equally totemic issue. It’s quite possible that the 2015 general election on May 7th, will have a low turnout generally if all the main political parties fail to capture the imagination of the general public. Using a market entry analogy, the question is how UKIP and NHAP enter the market of politics. It’s possible that UKIP could manage to come top in the European elections, though this is yet to be seen. UKIP are not opposed to UK in some sort of market with Europe, whilst wishing to not be embroiled in ‘spending £7 million a day for something undemocratic and unaccountable from Brussels’. Likewise, NHAP (National Health Action Party) is also concerned about the lack of democracy and accountability which appears to have become a pervasive theme in English NHS policy, and wish the NHS not to be fettered by the markets (for example European competition law). UKIP appear virtually weekly on Question Time, so the question is in part how can health issues compete for air time? Labour could even benefit from their greater presence in explaining their health policy, which is supposedly to escape the free market and TTIP. And NHAP could hold Labour to account on this issue, and other significant issues such as NHS reconfigurations and PFI. Conversely, UKIP is all for free trade.
Dr Lucy Reynolds soldiers on. As an academic in the highly prestigious London School of Hygiene and Tropical Medicine, Reynolds has developed an understanding of health policy which is unrivalled by many. Lucy has been quite successful in getting her well informed views across in the social media.
Dr Lucy Reynolds doesn’t have the luxury of Question Time.
Nigel Farage’s main complaint about Question Time is one of hostility to his party’s stance:
“I am one of the few people who can’t really complain about the editorial policy of Question Time having been on it 26 times since I was first elected in 1999. In terms of the coverage it gives Ukip I have found it fair and in the past few years the programme has even started accepting Ukip panellists other than me! But there have been a couple of programmes in which my colleagues and I have faced a hostile audience which in no way represents how Ukip is normally received or which are representative of the opinion polls. I am not pointing the finger of blame at the QT team but the question I want to ask is whether the Question Time audiences being exploited by the hard left?”
Even when Question Time was recently hosted at Lewisham, the number of questions on the NHS was kept to a bare minimum. This has been a general trend with this flagship TV programme, although the producers consistently cite that they can only air debates on questions proposed by audience members. However, occasionally dissent does ‘break though’ unpredictably. There have been over 86,000 ‘hits’ for a lady in the audience in Lewisham QT here

If it feels as if Nigel Farage is rarely off Question Time, that’s because he isn’t. Farage appeared more times on the programme than any other politician in the last four years. Top performers on #BBCQT include Nigel Farage, Vince Cable, Ken Clarke, Caroline Flint, Peter Hain, Caroline Lucas, Theresa May, and Shirley Williams. The arguments for Farage appealing to producers are that he is charismatic, inspires debate and helps them to fufil their requirement to give representation to smaller parties. But surely the same can be said for some experts in health policy?
Dr Louise Irvine (@drmarielouise), a GP in New Cross, south east London, and chair of the ‘Save Lewisham A&E’ campaign, has recently announced she will be standing for the National Health Action Party in the European Parliament elections on the 22 May 2014. Dr Irvine has said the NHS was under threat from an impending EU-US trade deal and the Government’s policies of ‘top down reorganisation, cuts and privatisation’.
She said: ‘I want to use this election to raise awareness of the imminent danger posed to the NHS by the EU/US trade agreement which will allow American companies to carve up the NHS and make the privatisation process irreversible.
‘I also want to alert the public to the gravity of the threat to the NHS from this Government with its programme of cuts, hospital closures and privatisation and to send a powerful message to politicians in Westminster and Brussels that people will not stand by and let their NHS be destroyed.
‘If elected, I will strive to ensure that EU regulations don’t adversely affect the NHS and are always in the best interests of the health of British people. The health of the nation spans all areas of policy from the environment to the economy.’
Dr Irvine is not only the “new kid on the block”. Rufus Hound is planning to run for the European Parliament to campaign against the privatisation of the NHS, saying he wants to preserve “one of the single greatest achievements of any civilisation”. In an impassioned blog post, he accused the Conservatives of wanting to sell off the health service to party donors – claiming that the Health Secretary, Jeremy Hunt, was “killing the NHS so that his owners can bleed you dry”.
The NHA was set up by Dr Richard Taylor, a former independent MP, to campaign against the Government’s Health and Social Care Act, introduced under the previous health secretary, Andrew Lansley. The party plans to field 50 candidates in the 2015 general election. Dr Clive Peedell (@cpeedell) has also been talking to the social media to get the NHAP’s message across’ he is one of the co-leaders.
The Max Keiser/Clive Peedell interview is here.
To give them credit, Dr Marie Louise Irvine and Rufus Hound offer us a chance to discuss the NHS, in the same way Nigel Farage and, say, Patrick O’Flynn (@oflynnexpress) offer us a chance to discuss our membership of Europe. The criticism is that they represent single issues and do not have a coherent corpus of policies across the full range of policy areas, and indeed have no realistic chance of forming a government. But paradoxically they both do offer a chance for domestic policy to operate in such a way Portcullis House doesn’t become another neoliberal outpost of the Federal United States of Europe. In the NHS’ case, socialism might only survive if it is not engulfed with yet more Atlantic Bridge-type stuff next parliament. But UKIP would not probably stop that. Who knows if Labour would be able to either in reality.
Lucy Reynolds is back – a chat with Bob Gill on how the marketing of NHSprivatisation has been tweaked
This was the front page of the Daily Mirror at the time.
The original video is here.
This video is a follow up on Dr Lucy Reynolds’ earlier analysis of the government’s ongoing programme to privatise the NHS by stealth.
Talking to local GP Dr Bob Gill (@drbobgill), she also elaborates on measures people can take to head off this programme, particularly in relation to the House of Lords debate on April 24th.
NHS Privatisation: The end-game
where you see * you can click to the hyperlink to bring you to the original website source of the direct quote.

I was recently reminded of a debacle under a Labour government in 2006 which the Guardian reported as follows*:
“A secret plan to privatise an entire tier of the NHS in England was revealed prematurely yesterday when the Department of Health asked multinational firms to manage services worth up to £64bn.
The department’s commercial directorate placed an advertisement in the EU official journal inviting companies to begin “a competitive dialogue” about how they could take over the purchasing of healthcare for millions of NHS patients. …
The advertisement asked firms to show how they could benefit patients if they took over responsibility for buying healthcare from NHS hospitals, private clinics and charities. The plan would give private firms responsibility for deciding which treatments and services would be made available to patients – and whether NHS or private hospitals would provide them.” (The Guardian)
“How to create money” in the NHS has always been one about denigrating the views of its professional social capital, and thinking about ways of maximising income.
As we approach the ‘E day’, May 7th 2015, when we know that the UK will go to the polls, it is useful to consider now the end-game of NHS privatisation.
False reassurances have been a-plenty.
Privatisation, when you apply common sense, is simply diversion of resources into the private sector from the public sector. Outsourcing (enacted through section 75 Health and Social Care Act (2012) and its regulations) is a key part of that.
But it’s not the full story. You’d have to be a complete idiot to wish to maintain that the NHS is not being privatised.
Some people, it seems, are prepared to perform that rôle.
The end-game
Nearly a year ago, before the section 75 regulations had been discussed in parliament, I introduced here how this somewhat ignored clause would fix the NHS into a competitive market.
I wrote a blogpost on the predictable trajectory of the NHS privatisation which clearly argues that this had started with shifts in policy from the Thatcher and Major governments.
If you want to understand the model, it’s worth tracking it back to the horses’ mouths: Conservative MPs Mr John Redwood and Dr Oliver Letwin.
In a now seminal article, “Opening the oyster: the 2010-1 NHS reforms in England” by academics Dr Lucy Reynolds and Prof Martin McKee for the Journal of the Royal College of Physicians of London (2012), known as “Clinical medicine”, the background to this journey to full privatisation is laid bare [Clin Med, April 1, 2012 vol 12 no 2, pp. 128-132.]
Reynolds and McKee argue in their conclusion*:
“Enthoven’s description of the HMO model, which he explicitly stated was at least as problematic but more expensive than the NHS, has somehow been adopted as a blueprint for the privatisation of the NHS. It was recently reported that the newer ‘accountable care model’ now finds favour with the secretary of state for health. This flexible model is a successor to the HMO model, although it is not greatly different in concept or operation. It involves a managed care arrangement in which the private sector primary care gatekeeper receives a subsidy from the government to pay all or part of the individual premiums due for the people registered with it, with the individuals concerned expected to pay any shortfall between the personal budgets provided by government and the amount charged by the accountable care organisation.
… Fulfilment of the longstanding ambition, documented by Redwood and Letwin, to expand private financing of the healthcare system through user contributions is thus now imminent. Enthoven’s reasoned view that market-based healthcare provision is more expensive and less universal than the NHS system consistently has been overlooked. …” (Reynolds and McKee, 2012)
“Commissioning support units” are for the time-being part of the new NHS landscape. Here they are discussed by Veronika Thiel on the King’s Fund website (linking to an article in the HSJ)*:
“Commissioning support units are set to take on important functions in the new NHS structure. They will support clinical commissioning groups by providing business intelligence, health and clinical procurement services, as well as back-office administrative functions, including contract management.” (Thiel, King’s Fund website)
The immediate future steps are something like this:
1. CSUs spun off as private entities, to private equity firms.
2. CSUs provide support to CCGs.
3. CCGs commission services from providers.
4. Each of us given a voucher worth what it is predicted we will cost.
5. We then exercise our choice to find an option that meets our expectations.
6. If the value of our voucher is insufficient, we top it up ourselves.
7. There’s some safety net for the very poor perhaps (and there’s a bit of lee-way here for anti-immigration politics).
8. CCGs compete with each other.
Commissioning support units and private equity
Roy Lilley, a health commentator, only this week reported on the big problem with the CSUs in an article entitled “Trojan Horse”*:
“The DH has a problem. By 2016 CSUs have to be off the NHS’s books as their grace period as chaperoned NHSE organisations comes to an end. They could be taken over and run by their staff, as a social enterprise or the private sector encouraged to buy-in. The usual suspects, Capita, Serco, Atos, and McKinsey are having a look. KPMG are not. …
Will they make money? Not now, not next year, but assuming there is no political upheaval in 2015, CSUs, as a long term punt, with payback measured in years not months might make them Primary Care’s Trojan Horse.” (Roy Lilley)
On 3 November 2013, the Financial Times had reported the following*:
“The NHS has approached private equity companies about taking over organisations that help buy billions of pounds of services for hospitals and GPs. The talks focus on the 19 commissioning support units (CSUs) set up last year to provide services to the new doctor-led commissioning groups that spend more than two-thirds of the NHS budget. …
CSUs were created as part of contentious healthcare reforms pushed through by the coalition government last year in the teeth of fierce opposition from Labour and much of the medical profession. Although the turnover of the 19 units range from just £21m to £62m a year, together they employ nearly 9,000 staff, designing health services and providing back office IT, procurement and payroll services to clinical commissioning groups. While the CSUs are subsidised by the NHS, they are expected to become self-sufficient profitmaking businesses or form joint ventures with the public or private sectors by 2016.” (Financial Times)
The public’s lack of appetite for privatisation
The public generally think that all privatisations work with a lot of publicity like the BT or Royal Mail one. Where ‘word-of-mouth advertising’ has usually effective (e.g. “Tell Sid”), campaigns anti-NHS privatisation can all too easily go viral (pooled efforts of NHS activists on the section 75 regulations, which saw withdrawal of the original statutory instrument.)

The situation of the ongoing NHS privatisation, across a number of successive UK administrations, is fundamentally different, as in this case the whole project can only work if the public do not realise that they are being duped. Many organisations, politicians, and other leaders can rightly share the blame for not been truthful about the situation. What in fact is most incredible that the process of privatisation of the NHS has been so vehemently denied by politicians and think-tanks, when it is all so incredibly blatant.
There are still a few ‘barriers’ to the ultimate end described below, but these are not impossible for the ‘privateers’ given the right environment.
These include the election of a government which can implement the final steps (this could be any of the main political parties based on their past performance), a NHS IT system ‘fit for purpose’, a method of allocating funds for CCGs depending on individuals’ contributions, a method for allowing top-up payments, to name but a few. However the privateers will be encouraged by the privatisation ‘progress’ which has been made in the last few years.
Appetite for privatisation had failed to increase prior to the last election, despite little manoeuvres like the NHS logo available to private companies to make it hard for patients to distinguish between services provided by them and the NHS proper; and permitting private hospitals to compete to sell whichever procedures they wish to offer. With all three main major political parties having converged on the market, there was barely a cigarette paper’s difference between these parties from which to choose.
Arguably, however, it would be quite unfair to blame unilaterally the UK Labour Party with the benefit of hindsight. Labour remain adamant that they would never have enacted a statutory instrument such as the Health and Social Care Act (2012). There is no indication that Labour had intended to publish a similar Act from Hansard. Furthermore, they did consistently fight tooth-and-nail against the Act in the lower House and the House of Lords.
Clinical-based commissioning
Doctors have been sold a bit of a pup, but the media and politicians were adamant that GPs would have a greater rôle in commissioning.
A starting point for understanding the relevance of commissioning to the privatised NHS is the famous Adam Smith Institute’s Pirie and Butler document, which includes a description of their proposed final phase of a switch from a classic NHS to a US-style system. Madsen Pirie and Eamonn Butler are the well known free market gurus at the Adam-Smith Institute. Their entire document reads like a promotion glossy for privatisation, completely bereft of evidence-based academic references.
The end point is a US-style health maintenance organisation (HMO).
The problem of starting new system such as Health Maintenance Organisations is largely avoided by keeping patients with their present GP. In theory, the resources go to the CCG selected by the doctor, although the ultimate choice lies with the patient, who can change CCG by going to a doctor registered with another one. The resources are thus supposed to be directed to the CCGs which are most favoured by doctors and patients.
Nonetheless, it is the CCG who holds the power. As such, CCGs don’t need to have any medical expertise.
Even a Tory MP, Dr Sarah Wollaston, has drawn attention* to how CCGs appear to have gone ‘gun-ho‘ in privatising when David Bennett from Monitor had not felt such a need:
“The existing guidance is widely ignored. David Bennet (sic), the Chief Executive of the regulator Monitor, has set out in a number of settings that commissioners are putting too many services out to tender and yet the waste of resources continues. Perhaps because no commissioners have the spare cash to fight a legal challenge themselves.” (Dr Sarah Wollaston’s blog)
That is why this from Earl Howe is pure ‘smoke and mirrors’ from when the section 75 Regulations were being discussed (shared by Clive Peedell of the National Health Action Party):

Resource allocation and “vouchers”
There are various accounts of how resource allocation works in the NHS, and indeed one of the challenges of understanding NHS privatisation is understanding new parts of the puzzle as they fall into place. NHS England, as Baumann offered in his Health Select Committee evidence this week, will be describing yet another configuration of this formula in December which is apparently going to factor in inequality as well.
In this model, each individual would receive from the state a health voucher, equivalent in value to what he or she approximately is currently ‘consuming’. Making the maths work is of course made a lot easier if the allotted budgets have already been worked out through implementation of ‘personal health budgets‘.
The voucher can be used towards the purchase of private health insurance or exchanged for treatment within the public sector health system. This can easily be sold on the basis of ‘equity’ – that each person has equal access to a ‘National Health Service’ – whereas people actually have access to an inter-tradeable insurance scheme.
Those who opt into private insurance can use the voucher to pay their premiums, and the insurance companies then collect the cash value of the “voucher” from the government. This is the most odd aspect of the model, but easy if you understand the apparent ease with which successive Conservative governments have effectively provided state benefits for their private sector colleagues (see recent outsourcing debacles across a number of sectors.)
The issue of co-payments had been kicked into the long grass.
Sir David Nicholson gave a further reassurance recently (irony klaxon) that it was unlikely that such payments would be introduced imminently on a BBC Radio 4 discussion programme called “Costing the NHS“.
People who decide that health care is particularly important to them are free to add to the amount covered by the voucher and thus purchase more expensive forms of insurance, perhaps covering more unlikely risks or providing superior standards of comfort or convenience.
This is where the right-wing are able to allow for the fact that people who want to pay more can. People on the centre and left, however, interpret this as producing potentially a ‘two tier system’. It is currently not that difficult to find stories of how inadequate the US Medicaid services are currently, and it is a national disgrace of theirs that there are some citizens who are too poor or too ill to be able to afford an insurance-based healthcare.
The voucher would not force people into private insurance, although it certainly makes the option of going private instantly available to everyone. Those who want to use the state service will continue to receive it, their voucher being their ticket to free treatment just as their national insurance number is at the moment.
The distinction between a public health service which does what it can on a take-it-or-leave-it basis, and a private system for the rich which offers choice and competition begins to overlap.
The demise of the CCGs
“Integration” is the standard weapon in the war of words which tries to legitimise the smuggling of the US health insurance industry into running the NHS. The insurance/voucher system fits snugly into such “integration” (or even “whole person care”), and could see one arm of the system (e.g. “universal credit”) enmeshing with another (e.g. “personal health budgets”) for whole person care. This is of course is hugely dangerous without the proper safeguards. Successsive governments have tried so hard to shore up the NHS IT system, under various pretences such as “the paperless NHS”, precisely for this purpose.
A possible relationship between universal credit and whole person credit was mooted here in the mysteriously insightful article by Jennie Macklin and Liam Byrne.
Why are MasterCard so keen on working on payment mechanisms? This article explores possibly why.
The public sector CCGs, taking responsibility for total health care of NHS patients, are not too far removed in structure from private insurance and management bodies. The funds for premiums are publicly provided, but the same competition and incentives operate, and the same choices are made available. Experience, however, from the US is that it is difficult for a patient to sue a CCG directly if a problem arises.
So the Clinical Commissioning Group (CCG) still remains a favourite means of achieving the NHS privatisation ‘end game’. The CCG format simply lays the groundwork and the basis for further changes at a later stage.
One of the first things to happen is that CCGs receive their population-based allowances. Whilst it is likely that this will be done on an incremental basis from what the current allocations might be, as CCGs become more sophisticated, they might make use of other techniques such as ‘the dementia prevalence calculator‘ which appears to have achieved somewhat of a pedestal status in dementia public health.
Another trick in the ‘registration process’ is hoping that some members of the public never register and so never receive their allowance. This is known to be a trick of the Department of Work and Pensions which have often failed to notify benefit claimants that their welfare benefits have come to an end.
CCGs might become themselves sitting ducks for becoming insolvent.
The Department of Health will have to conjure up increasingly imaginative methods of arranging CCG funding sharing so as to not make them look like cuts (and find a mouthpiece to publicise them).
A final change of direction for the NHS hoped by some?
Nick Seddon has recently been reported to have caused some controversy by proposing NHS cuts and GP charges. He of course has been the Deputy Director of the think-tank Reform. In 2008, published during the time of a Labour government, Reform produced a pamphlet entitled, “Making the NHS the best insurance policy in the world “.
Their “top recommendations” included the following*:
“These incentives could be introduced by changing the National Health Service to a National Health Protection System. Taxpayer funding and guaranteed access would continue, but individuals would be empowered to decide which approved Health Protection Provider to use. Custody of individual health outcomes would be made independent; it would no longer be in the hands of politicians.
This would mean the following for individuals:
- A “healthcare protection premium” of £2,000 per year would be paid out of general taxation, equivalent to the current NHS cost per individual in England. NB this is similar to the cost of health insurance in France and the Netherlands.
- A choice of where to spend the health protection premium, between Health Protection Providers (HPPs). Coverage for a wide, core level of health treatment, including all essential operations and treatments.
- Extra services, such as gym membership, and rebates for healthy living, for example smoking cessation, offered by HPPs to attract customers.
- Regulation of HPPs by government to ensure they reach minimum standards.
- The ability to top-up their premium to have extra services such as certain drugs, cosmetic surgery or better accommodation in hospitals. People in the UK already value their healthcare enough to spend £1,600 per family per year on health and fitness.The current Departmental review of top-up payments for cancer drugs and the draft EU Directive on cross-border healthcare are likely to lead to greater clarity over what individuals are entitled to and to a new market in insurance for top-up payments.
- Guaranteed accident and emergency cover through a general agreement with insurers, on the model of the Dutch compulsory insurance system.
Because of the positive developments in the UK, this is a task of evolution rather than revolution which could be complete in three to five years. The key steps would be turning Primary Care Trusts (PCTs) into Health Protection Providers; allowing other insurers to join the system; and defining the core entitlement to healthcare.
In January 2008 the Prime Minister described the NHS as “the best insurance policy in the world”. That is the right idea. It means radical change, to combine universal coverage with the focus on the patient evident in other countries. Success would see the UK rejoin the top rank of international health systems and become again the envy of the world.” (Reform Report, 2008)
I remember when I was once in a cab in London, and the cabbie was telling me how, for some private care his wife had received, the insurer had refused to pay for certain aspects of after-care. This is somewhat reminiscent for me of the following criticism made by Reynolds and McKee (2012) in relation to the Reform report*:
“This plan is alluded to in the 2010 white paper in the opaque phrase ‘money will follow the patient’. This refers to the impending roll-out of personal health budgets for all those registered with the NHS. These have been greeted with enthusiasm by patient groups, somewhat strangely when one considers that the NHS currently undertakes to cover all costs of care, whereas the concept of a finite budget implies that it is possible that the actual costs of care could exceed that budget, leaving the patient to cover the excess.” (Reynolds and McKee, 2012)
Andy Burnham MP: “I admit it – we let the market in too far”
Andy Burnham MP is reported on June 9th 2013 as saying the following*:
“When Shadow health lead Andy Burnham MP visited Lewisham the previous evening, he began his speech:
“I admit it – we let the market in too far and now on the 65th anniversary of the NHS we need to renew our commitment to Bevan’s NHS: public service over privatisation; collaboration over competition and people’s wellbeing before self-interested profit.”” (“Left Foot Forward” blog)
This was an important statement to have made.
And Burnham is reported in the same article as wishing to put a stop to the neoliberal firestorm of hospital reconfigurations:
“Later in the day Burnham left his Lewisham audience in no doubt as to his feelings and his intention :
“I give my full support and backing to Lewisham Hospital. 25,000 people marching through the streets is a remarkable achievement. We support the campaign.””
Conclusion
It’s all fairly predictable.
Or so it might appear. You could mount an argument that the present system is far better (having “liberalised” the NHS with non-NHS providers) than having an insurance-based system.
Indeed, indeed Andrew Lansley, the former Secretary of State for Health preceding Jeremy Hunt in the current government, claimed to be opposed to be against such a method of funding the NHS when the Bill was beginning to reach a climax in its discussions.
(see beginning of this video)
Aside from who exactly is in the market post 2015, whether it’s Andy Burnham MP’s “NHS preferred provider” or the Coalition’s “Any qualified provider”, it’s still of concern that there’s still a market. As a first step, Burnham in October 2012 asked for a block on the further ‘roll out’ of “any qualified provider”.
There’s no ‘conspiracy theory’ about it.
For anyone with a training in business and commercial or corporate law, it’s dead obvious.
If you wish to look at what we might be heading to, this overview of the ‘current problems’ of the US healthcare system is a good introduction.
‘Competition’ was used to crowbar the market in. Everyone knows that. People who aggressively pimped competition as a means of improving quality know exactly how faulty their reasoning was (see my previous blogpost). Unfortunately this has done massive damage to English health policy.
This video’s quite useful as it approaches some topics which will are likely to become inevitable for us in this jurisdiction, if we should decide to go down this route: what the process of transformation will cost, how the insurance packages are likely to have to be controlled, competition between CSUs and competition between CCGs in the private market (we know quite how successful competition has been in the energy market), what clinical services will still become out-of-scope, and so on.
The current ‘state of play’ is that Labour has stated categorically to repeal the Health and Social Care Act (2012) on many occasions. This is a determined attempt to ‘turn back the tide’ on NHS privatisation, which is a highly popular move amongst potential Labour voters.
Specifically, Labour wishes to put the stuff on competition in part 3 of the Act into reverse. Both Andy Burnham MP and Ed Miliband MP have stated their intention for this independently. Andy Burnham MP is reported as recently as 25 September 2013 as emphasising that he will end ‘fast track privatisation’.
A shift in emphasis from competition to collaboration will make it difficult to run the NHS as a market based on the rules of EU competition, with the correct adjustments in legislation from the Executive.
Many brilliant NHS activists have had landmark successes in opposing Government policy, too.
Never have the stakes been higher for the NHS with the election of the next UK Government, to take place during the course of May 8th 2015.
Try to talk to someone else about it to see what they think?
#Lab13 Stop #NHS2?

Whilst many of us find the concept of the NHS being outsourced and privatised to the highest bidder quite revolting, there is also a vocal minority, with cumulatively sufficient numbers of them to hold office if not power, who believe that the Health and Social Care Act (2012) and concomitant “top down reorganisation” bring innovative, free market forces to make the NHS a “global brand leader” in the competitive world of healthcare. They believe it’s simply about making the new NHS, ‘NHS2′, “fit for purpose”, and it was only a matter of time under the two main parties (Labour and Conservative) that yet a further reorganisation of the NHS would become necessary. Arguably, the public would learn to love its benefits. Similarly, the public would learn to love HS2, “high speed 2″. Problematically, despite supportive noises from Osborne and Hammond about HS2, HS2 could still become derailed.
As the UK Labour Party hit their latest debacle of a Philip Morris stand at conference, having wished to make a stance on standard packaging of cigarettes, the tensions between populist stances maximising Labour’s electoral chances on May 7th 2015 and highly principled strategic stances based on policy have arguably never been stronger. If you’re not in Brighton for the Labour Party Conference, you might have caught sight of the “#stopHS2″ campaign in the social media. Also, if you have been spending time looking at tweets about Labour’s health and social care policy, you can see the criticism of Labour over the accelerated privatisation of the NHS is not without its critics. Even intelligent well-meaning Labour supporters have been collecting electronic clippings of the continued interest in the private finance initiative (and the involvement of Coopers and Lybrand in the Major and Blair governments) and the independent sector treatment centres of the Blair government. At a time when Labour is seeking to restore faith in the political process under Lord Ray Collins of Highbury, the question that Labour is so strapped of cash that it needs Philip Morris support remains an irritating one? The notion of the ‘democratic deficit’ is seen in both HS2, as such a policy issue not even mooted in the 2010 general election which seems to have gathered cross-party support (a bit like ‘personal health budgets), and in ‘NHS2′, the top-down NHS reorganisation implemented by the Conservatives with the Liberal Democrats aiding and abetting. So if nobody voted for either policy, where did the policies from? It might not be quite the “smoke-filled rooms of beer and sandwiches”, but powerful lobbying of private commercial interests are likely to have been proven influential in the past.

Whatever the official party positions on HS2 (and this has been subject to flux in recent months), both HS2 and NHS2 have formidable national grassroot campaigns in places. Stop HS2 is the national grassroots campaign against HS2, the proposed new High Speed Two railway. Theri mission is To Stop High Speed Two by persuading the Government to scrap the HS2 proposal and to facilitiate local and national campaiging against High Speed Two.Their supporters come from a wide range of backgrounds and from across the political spectrum. The “Stop Section 75 campaign” from 38 degrees aimed at thwarting the major competitive tendering construct of the Health and Social Care Act (2012), but it was ultimately unsuccessful. 38 Degrees is the one of the UK’s biggest campaigning communities, with over 1 million members. They share a desire for a “more progressive, fairer, better society”. They tried to argue earlier this year to all MPs and members of the House of Lords that our NHS is precious – and the public overall don’t want it privatised. Privatisation for both HS2 and NHS2, here, essentially means diverting of state resources into private sector hands.
Both HS2 and NHS2 are staggeringly expensive projects in this day when we keep on having austerity rammed down our throats, but admittedly the scale of spending of each project is different. Nonetheless by anyone’s standards, £32 billion as an estimate for #HS2 is an eye-watering amount of cash. It works out at well over £1,000 for every single family up and down the United Kingdom, and large numbers of us remain unconvinced that this will be money well spent. The exact cost of the NHS2 top down reorganisation is in its own different way unclear. Following on from Labour’s claims of ‘hidden costs’ last November, Shadow Health Secretary Andy Burnham claimed that the reorganisation planned in the Government’s Health and Social Care Bill (as it was then) amounted to costs of £3.5 billion, far more than the £1.2 – £1.3 billion claimed by the Government. Minister of State for Health Simon Burns branded this figure a ‘mistake’, reasserting the Government’s own figures as the correct estimate.
Also, both policies HS2 and NHS2 are “unpopular” with the general public. This is reflected by the fact they have never been openly discussed with the public before implementation. The public remain unconvinced about the actual rationale for HS2 to bring greater equity between London and regions of England (critics argue that the plan would benefit London more than the regions). Likewise, at a time when the ‘cost of living’ has been thrust into pole position by Ed Miliband, the cost of non-NHS providers providing NHS products and services for a cost which enhances shareholder dividend, the case for pimping out the NHS to the private sector has never been more badly timed. A YouGov poll into spending cuts commissioned by the TaxPayers’ Alliance last summer found that 48 per cent of people supported cancelling plans for HS2, with barely a third wanting to press ahead with the scheme. And it’s hardly surprising that the public remains so reluctant to support it. Andrew Lansley’s NHS reorganisation is unpopular both with the public and health service staff. Such a large scale reorganisation (likened to “throwing a grenade into the NHS”, by Conservative MP Dr Sarah Wollaston) would be difficult even in the Blair years of increased funding.
Research published by the TaxPayers’ Alliance last year into the hidden costs of HS2 further set alarm bells ringing, highlighting, for example, the billions of additional funding that would be necessary to mitigate the environmental effects of the line by running more of it underground or through tunnels. Andy Burnham, Shadow Health Secretary, spoke of a “bruised and battered” NHS that was in a “fragile” state. Burnham believes there is now a choice to be made about whether we want to allow the inexorable advance of competition in the market, or whether we want to hold on to a planned national system that many successive generations in England have benefited from.
Both HS2 and NHS2 pose fundamental problems for the Labour policy review, still currently underway. They poses problems for the UK economy – how much benefit are we actually going to get from this surge of spending to implement them? They also pose problems for the public’s institutions. Both the railway network and the NHS are cherished by the public but in different ways. Many citizens, whether they are Labour voters, think that the privatised railway industry has become costly, fragmented and essentially a shambles following Tory privatisation, and some would fundamentally like it in state ownership. While Burnham has consistently said the dichotomy between public and private is a false dichotomy, he has also reiterated his affirmation for the ‘NHS preferred provider’ policy which is a small attempt to mitigate against the loss of a state-run comprehensive universal National Health Service.
Both HS2 and NHS2 are ‘elephants in the room’, and it is merely a question of time for how long they may remain hidden.
Outsourcing has become a policy drug, and they need to kick the habit

Taking a hammer to the NHS
If you don’t want to do something, you pay somebody else to do it. Hopefully you pay them peanuts. Doesn’t matter if the actual product or service is a bit shit. Or you could allow somebody else to do it under your identity still. Everyone thinks you’re the author it. But you pay that person a massive mark up so they make a tidy profit. Everyone’s a winner.
For this Government under Frances Maude, Chris Grayling and Jeremy Hunt, “outsourcing” is a drug. They need more of it to get the same kick (an increasing degree of tolerance), and if they don’t outsource something they get nasty withdrawal symptoms. Outsourcing is consider a useful step along the way to privatisation, and of course many less intelligent people have been arguing that the Health and Social Care Act is not privatisation. It is clearly privatisation if you outsource what should be a state-run health service into private hands for profit or surplus, and it is privatisation if you allow up to 50% of income to come from private sources. Both are new developments under this Government. Everyone’s a winner here – especially the hedge funds who are the major institutional shareholders of the private healthcare companies, the private companies who can find through slick procurement bids willing funders, and, of course management consultants, accountants and lawyers who can send a NHS Trust into one of the many detailed insolvency and failure régimes outlined in the Health and Social Care Act (2012). Mind you, there’s not a single clause on ‘safe staffing requirements’ in NHS Trusts, as a necessary and proportionate ‘check and balance’ on overzealous managers inflicting ‘efficiency cuts’ to frontline doctors and nurses. “More for less” is the mantra, and, with the Secretary of State now legally not obligated for the NHS for the first time (but responsible for ‘special measures’ presumably so that he can take control of both lack of patient safety in extreme measures and which private sector advisors can advise), outsourcing is not the next scandal waiting to happen. It is well and truly alive. While the ideological concern has been ‘privatising profits, socialising losses’ a concept coined by Andrew Jackson as far back as 1834 (and maybe the Royal Mail and RSB may be worthy examples to consider here), there is now an added dimension that foreign multinationals can raid the NHS, take over vast bits of it, and their registered offices for tax reasons might be abroad. The line of attack has always been that Doctors and nurses contribute nothing to the ‘wealth’ of this country not being wealth creators (footballers possibly do contribute more in a similar way to “Top Gear” by being potent foreign merchandising exports inter alia). The massive irony is that the tax from profits ends up in foreign jurisdictions, and contribute to the economy of those countries not ours. The resolution of the US-EU Free Trade Agreement, which may or may not include the NHS, will be important here, and there’s still no answer to Debbie Abrahams’ inquiry to my knowledge:
Debbie Abrahams (Oldham East and Saddleworth) (Lab): Will the Prime Minister confirm that the NHS is exempt from the EU-US trade negotiations?
The Prime Minister: I am not aware of a specific exemption for any particular area, but I think that the health service would be treated in the same way in relation to EU-US negotiations as it is in relation to EU rules. If that is in any way inaccurate, I will write to the hon. Lady and put it right.
In an article by Patrick Wintour published recently, Cruddas describes a ‘modern anomie’, a breakdown between an individual and his or her community, and alludes to the challenge of institutions mediating globalisation. Cruddas also describes something which I have heard elsewhere, from Lord Stewart Wood, of a more ‘even’ creation of wealth, whatever this means about the even ‘distribution’ of wealth. One of the lasting legacies of the first global financial crisis is how some people have done extremely well, possibly due to their resilience in economic terms. For example, it has not been unusual for large corporate law firms to maintain a high standard of revenues, while high street law has come close to total implosion in some parts of the country. In a way, this reflects a shift from pooling resources in the State to a neoliberal free market model. The global financial crash did not see a widespread rejection of capitalism, although the Occupy movement did gather some momentum (especially locally here in St. Paul’s Cathedral). It produced glimpses of nostalgia for ‘the spirit of ’45”, but was used effectively by Conservative and libertarian political proponents are causing greater efficiencies. Indeed, Marks and Spencer laid off employees, in its bid to decrease the decrease in its profits, and this corporate restructuring was not unusual. A conservative and a libertarian have several things in common, the most important is the need for people to take care of themselves for the most part. Libertarians want to abolish as much government as they practically can. It is thought that the majority of libertarians are “minarchists” who favour stripping government of most of its accumulated power to meddle, leaving only the police and courts for law enforcement and a sharply reduced military for national defence. A minority are possibly card-carrying anarchists who believe that “limited government” is a delusion, and the free market can provide better law, order, and security than any goverment monopoly.
Essentially a libertarian would fund public services by privatising them. In this ‘brave new world’, insurance companies could use the free market to spread most of the risks we now “socialise” through government, and make a profit doing so. That of course would be the ideal for many in reducing the spend on the NHS, to produce a rock-bottom service with minimal cost for the masses. And to give them credit, the Health and Social Care Act was the biggest Act of parliament, that nobody voted for, to outsource the operations of the NHS to the private sector, which falls under the rubric of privatisation. Outsourcing is an arrangement in which one company provides services for another company that could also be or usually have been provided in-house. Outsourcing is a trend that is becoming more common in information technology and other industries for services that have usually been regarded as intrinsic to managing a business, or indeed the public sector. Many expected the election of the present government to herald a more determined approach to outsourcing public services to the private sector. Initially came the idea of the “big society”, with its emphasis on creating and using more social enterprises to deliver public services, but the backers for this new era of venture philanthropism were not particularly forthcoming. The PR of it, through Steve Hilton and colleagues, was disastrous, and even Lord Wei, one of its chief architects, left. No one in the UK likes the idea of domestic jobs moving overseas. But in recent years, the U.K. has accepted the outsourcing of tens of thousands of jobs, and many prominent corporate executives, politicians, and academics have argued that we have no choice, that with globalisation it is critical to tap the lower costs and unique skills of labour abroad to remain competitive. They argue that Government should stay out of the way and let markets determine where companies hire their employees. But is this debate ever held in public? No, there was always a problem with reconciling the need for cuts with an ideological thirst for cutting the State. Here in the UK, in 2010, the government indicated that it wanted to see new entrants into the outsourcing market, and the prime minister visited Bangalore, the heart of India’s IT and outsourcing industry, for high profile meetings with chief executives of companies such as TCS, Infosys, HCL and Wipro. Nobody ever bothers to ask the public what they think about outsourcing, but if Gillian Duffy’s interaction with Gordon Brown is anything to go by, or Nigel Farage’s baptism in the local elections has proved, the public is still resistant to a concept of ‘British jobs for foreign workers’. However, it is still possible that the general public are somewhat indifferent to screw-ups of outsourcing from corporates, in the same way they learn to cope with excessive salaries of CEOs in the FTSE100. The media have trained us to believe that unemployment rights do not matter, and this indeed has been a successful policy pursued by the Conservatives and Liberal Democrats. People do not appear to blame the Government for making outsourcing decisions, for example despite the fact that the ATOS delivery of welfare benefits claims processing has been regarded by many as poor, the previous Labour government does not seem to be blamed much for the current fiasco, and the current fiasco has not become a major electoral issue yet.
And the list of screw-ups is substantial. G4S – the firm behind the Olympic security fiasco – has nowbeen selected to support the Police Service of Northern Ireland at the G8 Summit next month. Despite the company’s botched handling of the Olympics Games contract last summer, G4S has been chosen to supply 450 security staff for the event at Lough Erne, County Fermanagh The leaders of the world’s eight wealthiest countries are expected in Fermanagh on June 17 and 18. Meanwhile, medical assessments of benefit applicants at Atos Healthcare were designed to incorrectly assess claimants as being fit for work, according to an allegation of one of the company’s former senior doctors has claimed. Greg Wood, a GP who worked at the company as a senior adviser on mental health issues, said claimants were not assessed in an “even-handed way”, that evidence for claims was never put forward by the company for doctors to use, and that medical staff were told to change reports if they were too favourable to claimants. Elsewhere, Scotland’s hospitals were banned from contracting out cleaning and catering services to private firms as part of a new drive towards cutting the spread of deadly superbugs in the NHS. There were 6,430 cases of C. difficile infections in Scotland in one year recently, of which 597 proved fatal. The problem was highlighted by an outbreak of the infection earlier this year at the Vale of Leven hospital in Dunbartonshire which affected 55 people. The infection was identified as either the cause of, or a contributory factor in, the death of 18 patients.
Whatever our perception of the public perception, the impact on transparency and strong democracy merit consideration. As we outsource any public service, we appear to risk removing it from the checks and balances of good governance that we expect to have in place. Expensive corporate lawyers can easily outmanoeuvre under-resourced government departments, who often appear to be unaware of the consequences, and this of course is the nightmare scenario of the implementation of the section 75 NHS regulations. Even talking domestically, where contracts privilege commercial sensitivities over public rights, they can be used to exclude the provision of open data or to exempt the outsourcer from freedom of information requests. Talking globally, “competing in the global race” has become the buzzword for allowing UK companies to outsource to countries that do not have laws (or do not enforce laws) for environmental protection, worker safety, and/or child labour. However, all of this is to be expected from a society that we are told wants ‘less for more’, but then again we never have this debate. Are the major political parties afraid to talk to us about outsourcing? Yes, and it could be related to that other ‘elephant in the room’, about whether people would be willing to pay their taxes for a well-run National Health Service, where you would not be worried about your local A&E closing in the name of QUIPP (see this blogpost ). Either way, Jon Cruddas is right, I feel; the ‘modern anomie’ is the schism between the individual and the community, and maybe what Margaret Thatcher in fact meant was ‘There is no such thing as community’. If this means that Tony Blair feels that ‘it doesn’t matter who supplies your NHS services’, and we then get invasion of the corporates into the NHS, you can see where thinking like this ultimately ends up.
Politically, outsourcing vast amounts of the National Health Service is a big mistake. Take for example the scenario of what happens when something goes wrong. Will you get your money back? The lack of responsibility of the private sector shows how the NHS has to bail out the surgical mistakes of PIP breast implants. The State, evil though it is, does make a habit however of bailing out the private sector, as we all remember from the £860 bailout for the banking industry. It seems like a ‘cost saving’, but it clearly isn’t, in the same way that the private finance initiative has become a ‘cash cow’ for corporates. The essence of NHS policy is not to let the policy lunatics take over, in this case people with clearly vested interests having more impact on policy than professionals in the field. Part of the problem is that there is a lot more in common for Conservative and Labour policies, and indeed this is contributing to a growing sentiment that Labour is becoming complacent on the NHS (tweet by @gabyhinsliff):
Time will tell whether such fears will indeed materialise.
So what of social enterprises and the NHS? Corporate social responsibility and marketing revisited.

Milton Friedman’s famous maxim goes as follows:
“there is one and only one social responsibility of business – to use its resources and engage in activities designed to increase its profits so long as it stays within the rules of the game, which is to say, engages in open and free competition without deception or fraud.”
The history of social enterprise in fact extends as far back to Victorian England (Dart, 2004; Hines, 2005). The worker cooperative is one of the first examples of a social enterprise. Social enterprises prevail through- out Europe, and are most notable in the form of social cooperatives, particularly in Italy, Spain and increasingly France (Mancino and Thomas, 2005).
More recently, Clare Gerada, the Chair of the Royal College of General Practitioners, yesterday on BBC’s “The Daily Politics”, stated the following:
“Privatisation is the moving of State resources into the for full profit or non-profit sectors. And – the previous debate is that ‘if you don’t pay for therefore it’s not privatisation – it is privatisation. The profit that Specsavers or Harmoni make, they will not go back into the State: they will go straight into the shareholders.”
Currently, the position in English law is that the directors of every private limited company in law, whether they are called ‘social enterprises’ or not, have a statutory duty to the environment and stakeholders of their company. This is embodied in s.172 Companies Act (2006):
In an article by Rachel C. Tate, provocatively entitled, “Section 172 Companies Act 2006: the ticket to stakeholder value or simply tokenism?”, Tate argues as follows that stakeholder interests do not trump the interests of the company, i.e. to make profit. Interestingly. s.172 has no corollary in the common law.
“As highlighted, s172(1) formally obliges directors to consider stakeholder interests during the decision-making process. Yet, it is crucial to note that shareholder interests remain paramount. The interests of non-shareholding groups are to be considered only insofar as it is desirable to ‘(…) promote the success of the company for the benefit of its members.’17 A director will not be required to consider these factors beyond the point at which to do so would conflict with the overarching duty to promote company success. Stakeholder interests have no independent value in the consideration of a particular course of action.19 In addition, no separate duty or accountability is owed to the stakeholders included in the section.Thus, the duties of nurturing company success and having regard to the listed interests ‘(…) can be seen in a hierarchal way, with the former being regarded more highly than the latter.’21 Consequently, it would be wrong in principle to view s172 as requiring directors to ‘balance’ shareholders and stakeholder interests.22 These views are supported by industry guidance published on the effects of s172.”
“Social enterprises” are actually very hard to define. According to the United Kingdom (UK) government’s Department of Trade and Industry (2002), in the era of Tony Blair and Patricia Hewitt, a social enterprise is:
“a business with primarily social objectives whose surpluses are principally reinvested for that purpose in the business or in the community, rather than being driven by the need to maximise profit for shareholder and owners’”
Therefore, in theory, social ends and profit motives do not contradict each other, but rather have complementary outcomes, and constitute a ‘double bottom line’.
Nonetheless, the UK Government website contains a list of possible entities which could be described as ‘social enterprises’, namely:
- limited company
- charity, or from 2013, a charitable incorporated organisation (CIO is the new legal structure for charities)
- co-operative
- industrial and provident society
- community interest company (CIC)
- sole trader or business partnership
Note that in one of the vehicles, the limited company, as stated above, the primary duty of the directors is to promote success of the company. And that can be a “social enterprise”. Furthermore any contracts supplied to social enterprises can still still meet the definition of ‘privatisation’ above, not least because social enterprises are considered not to be wholly in the public sector (for example this EU definition, link here, where “Social enterprises are positioned between the traditional private and public sectors.”). Social enterprises do not meet the definition of what is typically in the public sector, by reference to the European System of Accounts 1995, link here. It is striking that the EU concede that one feature of social enterprises is a “significant level of risk”, so one has to question the long-term wisdom of competitive tendering contracts increasingly to social enterprises. Indeed, given that directors of English private limited companies are supposed to have due regard to wider “stakeholder” factors, one has to wonder quite what the point of the Public Services (Social Value) Act 2012 is. “Third Sector” magazine on 9 October 2012 reported that this enactment was not going that well:
“The Public Services (Social Value) Act could end up as a missed opportunity and more work needs to be done to encourage its use by commissioners and procurement professionals, delegates at the Labour Party conference heard. The act became law in March and places a duty on public bodies in England and Wales to consider “economic, social and environmental wellbeine in connection with public service contracts’! But at a fringe event hosted by the local infrastructure body Navca and the think tank ResPublica in Manchester, Hazel Blears, vice-chair of the All-Party Parliamentary Group on Social Enterprise, said she was concerned that many local authorities would not give it the attention it deserved.”The wording is weak,”she said.”If they had to ‘take account of social value, that would have been a harder position.””
There has been concern that in social enterprises, whilst the external environment may be given prominence, the internal environment may suffer (Cornelius et al., 2008):
“Since many social enterprises exist predominantly to address social ends (one key feature of the triple bottom line), it could be argued that the prevalence of their CSR policy and practice require close investigation. Emanuele and Higgins (2000) con- tribute to this agenda by challenging the assumption that non-profit organisations can offer comparatively lower wages, because they are more pleasant places to work. The authors emphasise that employees in this sector are often second income earners, and therefore are less concerned with lower wages and reduced benefits more characteristic of the private sector. They highlight how the voluntary sector is often a job entry point for new employees, who later move on to other sectors offering more fringe benefits, better financial security and healthcare programmes. They conclude with the assertion that ‘‘we must begin to exert the same pressure for ‘corporate responsibility’ among non-profit employers, as we demand in the private sector’’ (Emanuele and Higgins, 2000: 92), implying that the social enterprise sector needs to treat its employees better. Distinguishing between external and internal CSR may be beneficial, with social enterprises clearly focusing upon serving communities and overlooking crucial internal human resource issues.”
Grimsby “Care Plus” has been, in fact, highly commended in the UK Social Enterprise Awards (link here). The national competition, organised by Social Enterprise UK, recognises excellence in Britain’s growing social enterprise sector. And yet it was recently reported that, “More than 800 staff employed by the Care Plus Group – which provides adult health and social care across North East Lincolnshire – are in consultation over cuts to their pay and conditions.” Lance Gardner, the Chief Executive of the organisation, is reported as saying, “There is a lot of goodwill here. Our staff go that extra mile for their patients and have a passion for caring. They would not want to see them suffer. I do not want to take our goodwill for granted.”
The story of what happened between UNISON and Circle Hinchingbrooke is of course well known now (link here):
“Christina McAnea, head of health at Unison, said Circle could “cream off nearly 50% of the hospital’s surpluses” which would make it “virtually impossible to balance the books”.
“This is a disgrace. Any surpluses should be going directly into improving patient care or paying off the hospital’s debt, securing its future for local people – not ploughed into making company profits.
“Instead patients and staff are facing drastic cuts. The hospital was already struggling, but the creep in of the profit motive means cuts will now be even deeper. And it is patients and staff that will pay the price.””
Of course, ‘corporate social responsibility’ (“CSR”), abbreviated to ‘people, planet, profit’ somewhat tritely, has clashed before with marketing, so it is no wonder that businesses should wish to look ‘socially responsible’ to seek competitive advantage. Corporates have long been criticised for using diversity as a marketing ploy, e.g. putting in their promotional literature photos of employees in wheelchairs to demonstrate they are disabled-friendly. Pitches from social enterprises are likely to come with them ‘a feel good factor’ in competitive tendering, and of course any pitch which complies with adding social value in keeping with the new legislation is perfect “rent-seeking” fodder. But at the end of the day they are a range of entities seeking to make money which does not necessarily get fed back into frontline care, but used to generate a surplus aka profit. In an outstanding essay by Anna Kim for the 8th Ashbridge Business School MBA award, the author writes:
“Many critics believe that most of so-called CSR activities are nothing but a deceptive marketing tool, such as greenwashing. Can British American Tobacco be a ‘responsible’ cigarette manufacturer? Is Nestle really moving towards social values, or simply trying to wash its image around the baby milk and other ethical issues by putting a Fairtrade label on its 0.2% of coffee product line? From the green policy of oil giants BP and Shell to the childhood obesity research fund of McDonald’s, the list of controversial CSR examples is not exhaustive.”
So what of social enterprises and the NHS – remember Milton Friedman and Clare Gerada….
References
Cornelius, N., Todres, M., Janjuha-Jivraj, J., Woods, A., and Wallace, J. (2008) Corporate Social Responsibility and the Social Enterprise, Journal of Business Ethics, 81, pp. 355–370.
Dart, R. (2004) The Legitimacy of Social Enterprise’, Nonprofit Management and Leadership ,14(Summer), pp. 411–424.
Department for Trade and Industry (2002) Social Enterprise: A Strategy for Success, available at http://www.seeewiki.co.uk/~wiki/images/5/5a/SE_Strategy_for_success.pdf .
Hines, F. (2005) Viable Social Enterprise – An Evaluation of Business Support to Social Enterprises’, Social Enterprise Journal, 1(1), pp. 13–28.
Mancino, A. and Thomas, A. (2005) An Italian Pattern of Social Enterprise: The Social Cooperative, Nonprofit Management and Leadership, 15(3), pp. 357–369.
The Tories have never had any ideology, so it's not surprising they've run out of steam

A lot of mileage can be made out of the ‘story’ that the Coalition has “run out of steam”, and this week two commentators, Martin Kettle and Allegra Stratton, branded the Queen’s Speech as ‘the beginning of the end’. There is a story that blank cigarette packaging and minimum alcohol pricing policies have disappeared due to corporate lobbying, and one suspects that we will never get to the truth of this. The narrative has moved onto ‘immigration’, where people are again nervous. This taps into an on-running theme of the Conservatives arguing that people are “getting something for nothing”, but the Conservatives are unable to hold a moral prerogative on this whilst multinational companies within the global race are still able to base their operations using a tax efficient (or avoiding) base. Like it or now, the Conservatives have become known for being in the pockets of the Corporates, but not in the same way that the Conservatives still argue that the Unions held ‘the country to ransom’. Except things have moved on. The modern Conservative Party is said to be more corporatilist than Margaret Thatcher had ever wanted it to be, it is alleged, and this feeds in a different problem over the State narrative. The discussion of the State is no longer about having a smaller, more cost-effective State, but a greater concern that ‘we are selling off our best China’ (as indeed the late Earl of Stockton felt about the Thatcherite policy of privatisation while that was still in its infancy). The public do not actually feel that an outsourced state is preferable to a state with shared responsibility, as the public do not feel in control of liabilities, and this is bound to have public trust in privatisation operations (for example, G4s bidding for the probation service, when operationally it underperformed during the Olympics).
It is possibly this notion of the country selling off its assets, and has been doing so under all administrations in the U.K., that is one particular chicken that is yet to come home to roost. For example, the story that the Coalition had wished to push with the pending privatisation of Royal Mail is that this industry, if loss making, would not ‘show up’ on the UK’s balance sheet. There is of course a big problem here: what if Royal Mail could actually be made to run at a profit under the right managers? Labour in its wish to become elected in 1997 lost sight of its fundamental principles. Whether it is a socialist party or not is effectively an issue which seems to be gathering no momentum, but even under the days of Nye Bevan the aspiration of Labour was to become a paper with real social democratic clout. One of the biggest successes was to engulf Britain in a sense of solidarity and shared responsibility, taking the UK away from the privatised fragmented interests of primary care prior to the introduction of the NHS. The criticism of course is that Bevan could not have predicted this ‘infinite demand’ (either in the ageing population or technological advances), but simply outsource the whole lot as has happened in the Conservative-led Health and Social Act (2012) is an expedient short-term measure which strikes at the heart of poverty of aspiration. It is a fallacy that Labour cannot be relevant to the ‘working man’ any more, as the working man now in 2013 as he did in 1946 stands to benefit from a well-run comprehensive National Health Service. Even Cameron, in introducing his great reforms of the public sector in 2010/1 argued that he thought the idea that the public sector was not ‘wealth creating’ was nonsense, which he rapidly, unfortunately forgot, in the great NHS ‘sell off’.
The Conservatives have an ideology, which is perhaps outsourcing or privatisation, but basically it comes down to making money. The fundamental error in the Conservative philosophy, if there is one, is that the sum of individual aspiration is not the same as the value of collective solidarity and sharing of resources. This strikes to the heart of having a NHS where there are winners and losers, for example where the NHS can run a £2.4 bn surplus but there are still A&E departments shutting in major cities. Or why should we tolerate a system of ‘league tables’ of schools which can all too easily become a ‘race to the bottom’? Individual freedom is as relevant to the voter of Labour as it is to the voter of the Conservative Party, but if there is one party that can uphold this it is not the Conservatives or the Liberal Democrats. No-one on the Left can quite ignore why Baroness Williams chose to ignore the medical Royal Colleges, the RCN, the BMA or the legal advice/38 degrees so adamantly, although it does not take Brains of Britain to work out why certain other Peers voted as they did over the section 75 regulations as amended. But the reason that Labour is unable to lead convincingly on these issues, despite rehearsing well-exhausted mantra such as ‘we are the party of the NHS’, is that the general public received a lot of the same medicine from them as they did from the Conservatives or the Liberal Democrats. Elements of the public feel there is not much to go further; the Labour Party will still be the party of the NHS for some (despite having implemented PFI and NHS Foundation Trusts), and the Conservatives will still be party of fiscal responsibility for some (despite having sent the economy into orbit due to incompetent measures culminating in avoidance of a triple-dip).

It doesn’t seem that Labour is particularly up for discussion about much. It gets easily rumbled on what should be straightforward arms of policy. For example, Martha Kearney should have been doing a fairly uncontroversial set-piece interview with Ed Miliband in the local elections, except Miliband came across as a startled, overcaffeinated rabbit in headlights, and refused doggedly to explain why his policy would not involve more borrowing (even when Ed Balls had said clearly it would.) Miliband is chained to his guilty pleasures of being perceived as the figurehead of a ‘tax and spend’ party, which is why you will never hear of him talking for a rise in corporation tax or taxing excessively millionaires (though he does wish to introduce the 50p rate, which Labour had not done for the majority of its actual period in government). It uses terms such as “predistribution” as a figleaf for not doing what many Labour voters would actually like him to do. Labour is going through the motions of receiving feedback on NHS policy, but the actual grassroots experience is that it is actually incredibly difficult for the Labour Party machine even to acknowledge actually well-meant contributions from specialists. The Labour Party, most worryingly, does not seem to understand its real problem for not standing up for the rights of workers. This should be at the heart of ‘collective responsibility’, and a way of making Unions relevant to both the public and private sector. Whilst it continues to ignore the rights of workers, in an employment court of law over unfair dismissal or otherwise, Labour will have no ‘unique selling proposition’ compared to any of the other parties.
Likewise, Labour, like the Liberal Democrats, seems to be utterly disingenious about what it chooses to support. While it seems to oppose Workfare, it seems perfectly happy to vote with the Government for minimal concessions. It opposes the Bedroom Tax, and says it wants to repeal the Health and Social Care Act (2012), but whether it does actually does so is far from certain; for example, Labour did not reverse marketisation in the NHS post-1997, and conversely accelerated it (admittedly not as fast as post-2012). No-one would be surprised if Ed Miliband goes into ‘copycat’ mode over immigration, and ends up supporting a referendum. This could be that Ed Miliband does not care about setting the agenda for what he wants to do, or simply has no control of it through a highly biased media against Labour.
Essentially part of the reason that the Conservatives have ‘run out of steam’ is that they’ve run out of sectors of the population to alienate (whether that includes legal aid lawyers or GPs), or run out of things to flog off to the private sector (such as Circle, Serco, or Virgin). All this puts Labour in a highly precarious position of having to decide whether it wishes to stop yet more drifting into the private sector, or having to face an unpalatable truth (perhaps) that it is financially impossible to buy back these industries into the public sector (and to make them operate at a profit). However, the status quo is a mess. The railway industry is a fragmented disaster, with inflated prices, stakeholders managing to cherrypick the products they wish to sell to maximise their profit, with no underlying national direction. That is exactly the same mess as we have for privatised electricity, or privatised telecoms. That is exactly same mess as we will have for Royal Mail and the NHS. The whole thing is a catastrophic fiasco, and no mainstream party has the bottle to say so. The Liberal Democrats were the future once, with Nick Clegg promising to undo the culture of ‘broken promises’ before he reneged on his tuition fees pledge. UKIP are the future now, as they wish to get enough votes to have a say; despite the fact they currently do not have any MPs, if they continue to get substantial airtime from all media outlets (in a way that the NHS Action Party can only dream of), the public in their wisdom might force the Conservatives or Labour to go into coalition with UKIP. There is clearly much more to politics than our membership of Europe, and, while the media fails to cover adequately the destruction of legal aid or the privatisation of the NHS, the quality of our debate about national issues will continue to be poor. Ed Miliband must now focus all of his resources into producing a sustainable plan to govern for a decade, the beginning of which will involve an element of ‘crisis management‘ for a stagnant economy at the beginning. The general public have incredibly short memories, and, although it has become very un-politically correct to say so, their short-termism and thirst for quick remedies has led to this mess. Ed Miliband seems to be capable of jumping onto bandwagons, such as over press regulation, but he needs to be cautious about the intricacies of policy, some of which does not require on a precise analysis of the nation’s finances at the time of 7th May 2015. With no end as yet in sight for Jon Cruddas’ in-depth policy review, and for nothing as yet effectively Labour to campaign on solidly, there is no danger of that.
The price tariffs political mess might be a taster of the economic mess in the NHS to come

Several sectors have tried to address how competition might provide better quality for the customer. The basic hope is that by ‘opening up the market’ to more providers, the private market is more intense, the choice is wider, and customers receive a ‘good deal’. However, there are very few markets in the U.K. where this can be said to have worked. We can all think of the big five in supermarkets, including Tesco, Sainsbury’s, Asda, Safeway and Morrison’s. Earlier this year, 2,000 dairy farmers attended a rally in Westminster to bring attention to the situation. The following weekend they picketed branches of Asda, Morrisons and the Co-operative, which pay less than Tesco, Sainsbury’s, Marks & Spencer and Waitrose. More pickets are expected this weekend, powered by movements such as Farmers for Action and #sosdairy, which has been trending on Twitter. As little as far back as 2011, the Office of Fair Trading (OFT) said it saw clear problems with competitiveness in the audit market, meaning referral to the Competition Commission is almost certain. The OFT said the dominance of by so few firms – PricewaterhouseCoopers, Ernst & Young, Deloitte and KPMG – made it hard for rivals to compete and didn’t allow for companies to switch auditors, creating what critics have described as a dangerous dependence on too few firms.
Today, David Cameron’s pledge to ensure that gas and electricity consumers get the lowest tariff was thrown into confusion today as the Government staged a partial retreat. Labour accused the Prime Minister of presiding over another “omnishambles” after John Hayes, the Energy Minister, stopped short of repeating Mr Cameron’s promise on Wednesday of legislation to ensure “energy companies have to give the lowest tariff to their customers.” Last year, John Robertson, a Glasgow MP and member of the Energy Commons Select Committee, called on the regulator to use its toughest penalty – fining suppliers up to 10pc of their turnover – as dual-fuel bills have risen to a record £1,300 per year. In a Commons motion, he claims that recent energy price rises by the “Big Six” are “clear acts of anti-competitive behaviour” . Across these companies – British Gas, npower, E.ON, EDF, SSE and Scottish Power, the maximum fine for their supply businesses could be around £4bn in total, based on last year’s revenues. Mr Robertson wants to see any penalties imposed on the companies put in a “consolidated fund via the Treasury” and dispersed to consumers. He further added: “These companies are pinching money out of the pockets of the poorest people in this country at a time when snow is about to fall and when wholesale energy prices are low. Yet the Government and Ofgem are acting like there is nothing they can do”. The executive director of Which?, Richard Lloyd, has recently written a strongly worded letter to David Cameron: “It’s time to face facts: the energy market is broken. The sector is dominated by a handful of big and powerful players who are seemingly unaffected by the normal competitive pressure of price and customer service.” Reacting to Cameron’s announcement yesterday, Lloyd said: “Legislating so energy companies have to give the lowest tariff to their customers is a big statement from the prime minister and acknowledges that competition in the energy retail market has failed. This is a big moment for consumers, but we must now see these words turned into action and see the detail from the government in the energy bill.”
An obvious solution to increasing the scope for competition is to lower the barriers-to-entry for new entrants to the market. Interestingly, in the new legal services market of England, reported today, the Solicitors Regulation Authority has made a conscious decision not to place too many conditions on new alternative business structures (ABSs), its leader has revealed. Chief executive Antony Townsend said the terms of the licence had deliberately been kept simple for the 33 entities that have been granted ABS status by the regulator so far. Speaking today at the Westminster Legal Policy Forum, Townsend said the aim was not to tie the SRA or applicants ‘up in knots’ and instead to monitor their behaviour after they had become an ABS. ‘We’re supervising appropriately and managing risk appropriately rather than trying to put in place elaborate licensing conditions,’ according to Townsend. The new NHS, which has allowed greater scope for private provision, faces a similar task. In a pamphlet for the King’s Fund by Loraine Hawkins from July 2011, entitled “Can competition and integration co-exist in a reformed NHS?”, it is conceded that much of the public debate about the Health and Social Care Act 2012 has focused on proposals to give Monitor, the sector regulator for the NHS, a duty to promote competition (where appropriate) and to apply national and EU competition law to foundation trusts. The emphasis in Monitor’s competition role will instead focus on prohibiting behaviour that prevents, restricts or distorts competition contrary to the interests of NHS patients. This revised formulation of Monitor’s duties will mirror the language of competition law, instead of using more activist pro-competition language modelled on legislation governing economic regulation of the privatised utilities. However, this is potentially worrying, if the blueprint for regulation of the NHS is a sector where there have been massive problems thus far.
For competition to work in the NHS, it will be necessary likewise to ensure that the barriers-to-entry for new entrants to the healthcare market are not onerous so as to prevent entry, but high enough to ensure quality of healthcare and trust of the public in the reputation in the NHS. “Any Qualified Provider” is a procurement model which clinical commissioning groups could use to develop a register of providers accredited to deliver a range of specified services within a community setting. The model aims to reduce bureaucracy and barriers to entry for potential providers. However, thus far, the NHS market could face the same problems in supermarkets and accounting, with a dominance on a few firms which have a legal obligation to maximise dividend for the shareholder. For example, it was reported only this month that two major players in the private healthcare market, Virgin and Serco, have considerable made strides into the NHS as business gurus claim the private sector is set to cash in on community services. All of this is deeply worrying, as the track history in disasters of privatisation is now getting quite substantial. Other examples are wide-ranging, described here, including railways, hospital cleaning, bus services, prisons, and social care.
