Home » Posts tagged 'PFI'
Tag Archives: PFI
Could the “social impact bond” help to improve services in dementia care?
This blogpost first appeared on the ‘Living well with dementia’ blog yesterday.
It’s impossible to ignore the occasional spate of reports of ‘care home scandals’, including Winterbourne View and Orchid View.
Whilst a direction of travel might be to advance people living ‘successfully’ as long as possible independently, there’ll be some people for whom a care home might be appropriate. There are particular aims of policy designed to support living well with dementia, such as combating loneliness and providing meaningful leisure activities, which can possibly be achieved through high quality care homes.
It’s pretty often that you hear of social care being “on its knees”, due to drastic chronic underfunding. A concern about attracting investment from the private sector is that this will help to accelerate the lack of financial resource allocation from the State. And yet this is the opposite to the argument of resources ‘leeching’ out of the public sector into the private sector.
In terms of the ‘business model’, there are concerns that, to maximise shareholder dividend, staff will not be incentivised to ‘care well’, if they are barely meeting the requirements of the national minimum wage. Whilst the employer emphasises ‘flexibility’ of zero hours contracts, for many such contracts are symbolic of a lack of commitment for sustained employment by the employer.
So the idea of bonds being used to prop up dementia care, currently one of the three big arms of the Prime Minister’s Dementia Challenge, has gained some momentum, for example here. Bonds are effectively “IOUs“, and concerns remain for them as in the private finance initiative – such as who actually benefits, the prolonged threat of penalty for not being able to meet your loan repayments, the issue of who decides the outcomes by which performance will be assessed, and who actually manages or controls the enterprise.
Social Impact Bonds (SIBs) are depicted as “a way of enabling innovation, creating flexible contracts around social outcomes and providing linked investment“. But for some, they are a vehicle for enabling ‘privatisation by stealth’.
The current Labour opposition officially is trying to distance itself from any mechanisms promoting the privatisation of the NHS, and yet it is known Chris Ham and Norman Lamb wish to publish a report imminently on the possible use of SIBs in policy under the auspices of the King’s Fund.
This is the title slide of Hazel Blears’ presentation for the Alzheimer’s Show on Friday.

And here is a section of her talk.
[apologies for the sound quality]
Hazel has a strong personal attachment to campaigning on dementia, and is particularly interested and influential in the direction of travel, not least in her rôle as Vice Chair of the All Party Parliamentary Group on dementia, a cross party group made up of MPs and Peers with an interest in dementia.
Andy Burnham MP, Shadow Secretary of State for Health, has made it clear that it is his firm and settled intention to repeal the Health and Social Care Act (2012). The current Prime Minister’s Dementia Challenge is to come to an end officially in March 2015.
Dementia UK set up some time ago its innovative ‘Admiral Nurses’ scheme, to provide specialist nurses who could help people with dementia and family carers to improve the quality of life of people with dementia and family carers.
Burnham has also let it be known that he intends to subsume social care within the NHS under the construct of ‘whole person care’. Whichever various formulations of ‘whole person care’ you look at, you tend to find a ‘care coordinator’ somewhere. The exact job description of the care coordinator, nor indeed which specialisms might be best suited to accomplish this rôle, is somewhat unclear presently.
But it is all too common to hear of people being diagnosed with dementia being ‘lost in the system’, sometimes for years without follow up.
A “care coordinator” might help to boost access to the following services: emotional support, enable short breaks for people with dementia and anyone in a caring role, promote nutritious meals, ensure medications are given on time, ensure the correct medications have been subscribed (for example avoiding antipsychotic medications in individuals who might be unsuited to these), advice about suitable housing (including downsizing), ensure all physical commodities are properly medically managed; and so the list goes on.
I feel it’s pretty likely there’ll be a ‘first mover advantage‘ effect for any entity which takes up this coordination rôle in dementia care. But the tension between this and the Opposition’s policy is palpable: one cannot talk of this entity being ‘the first to enter the market’, as many wish (and expect) Labour to abolish the internal market in health care.
Such a coordinating entity could well be a recipient of a SIB – but is this like the PFI of social care? PFI by and large has an incredibly negative press amongst members of the general public.
But on the other hand, is it vindictive to prevent a social enterprise from pitching from such a service? If that entity has the technical ‘know how’ to run operations nationally competently and at a reasonable price, would that be preferable to the State running such services when projects such as NHS IT and universal credit have not gone terribly well?
In our jurisdiction, private companies can hide easily being a corporate veil, and are for example currently not readily accountable through freedom of information legislation. This is despite numerous requests to Jeremy Hunt in parliament about parity in disclosure requirements from both private and public providers.
And the track record of some outsourcing companies in the private sector, it is said, has been terrible.
Jeremy Hunt and Norman Lamb are currently in control of NHS and care policy, but there might be a fundamental change in direction from the next Government.
Or there might not be.

Could the “social impact bond” help to improve services in dementia care?
It’s impossible to ignore the occasional spate of reports of ‘care home scandals’, including Winterbourne View and Orchid View.
Whilst a direction of travel might be to advance people living ‘successfully’ as long as possible independently, there’ll be some people for whom a care home might be appropriate. There are particular aims of policy designed to support living well with dementia, such as combating loneliness and providing meaningful leisure activities, which can possibly be achieved through high quality care homes.
It’s pretty often that you hear of social care being “on its knees”, due to drastic chronic underfunding. A concern about attracting investment from the private sector is that this will help to accelerate the lack of financial resource allocation from the State. And yet this is the opposite to the argument of resources ‘leeching’ out of the public sector into the private sector.
In terms of the ‘business model’, there are concerns that, to maximise shareholder dividend, staff will not be incentivised to ‘care well’, if they are barely meeting the requirements of the national minimum wage. Whilst the employer emphasises ‘flexibility’ of zero hours contracts, for many such contracts are symbolic of a lack of commitment for sustained employment by the employer.
So the idea of bonds being used to prop up dementia care, currently one of the three big arms of the Prime Minister’s Dementia Challenge, has gained some momentum, for example here. Bonds are effectively “IOUs“, and concerns remain for them as in the private finance initiative – such as who actually benefits, the prolonged threat of penalty for not being able to meet your loan repayments, the issue of who decides the outcomes by which performance will be assessed, and who actually manages or controls the enterprise.
Social Impact Bonds (SIBs) are depicted as “a way of enabling innovation, creating flexible contracts around social outcomes and providing linked investment“. But for some, they are a vehicle for enabling ‘privatisation by stealth’.
The current Labour opposition officially is trying to distance itself from any mechanisms promoting the privatisation of the NHS, and yet it is known Chris Ham and Norman Lamb wish to publish a report imminently on the possible use of SIBs in policy under the auspices of the King’s Fund.
This is the title slide of Hazel Blears’ presentation for the Alzheimer’s Show on Friday.
And here is a section of her talk.
[apologies for the sound quality]
Hazel has a strong personal attachment to campaigning on dementia, and is particularly interested and influential in the direction of travel, not least in her rôle as Vice Chair of the All Party Parliamentary Group on dementia, a cross party group made up of MPs and Peers with an interest in dementia.
Andy Burnham MP, Shadow Secretary of State for Health, has made it clear that it is his firm and settled intention to repeal the Health and Social Care Act (2012). The current Prime Minister’s Dementia Challenge is to come to an end officially in March 2015.
Dementia UK set up some time ago its innovative ‘Admiral Nurses’ scheme, to provide specialist nurses who could help people with dementia and family carers to improve the quality of life of people with dementia and family carers.
Burnham has also let it be known that he intends to subsume social care within the NHS under the construct of ‘whole person care’. Whichever various formulations of ‘whole person care’ you look at, you tend to find a ‘care coordinator’ somewhere. The exact job description of the care coordinator, nor indeed which specialisms might be best suited to accomplish this rôle, is somewhat unclear presently.
But it is all too common to hear of people being diagnosed with dementia being ‘lost in the system’, sometimes for years without follow up.
A “care coordinator” might help to boost access to the following services: emotional support, enable short breaks for people with dementia and anyone in a caring role, promote nutritious meals, ensure medications are given on time, ensure the correct medications have been subscribed (for example avoiding antipsychotic medications in individuals who might be unsuited to these), advice about suitable housing (including downsizing), ensure all physical commodities are properly medically managed; and so the list goes on.
I feel it’s pretty likely there’ll be a ‘first mover advantage‘ effect for any entity which takes up this coordination rôle in dementia care. But the tension between this and the Opposition’s policy is palpable: one cannot talk of this entity being ‘the first to enter the market’, as many wish (and expect) Labour to abolish the internal market in health care.
Such a coordinating entity could well be a recipient of a SIB – but is this like the PFI of social care? PFI by and large has an incredibly negative press amongst members of the general public.
But on the other hand, is it vindictive to prevent a social enterprise from pitching from such a service? If that entity has the technical ‘know how’ to run operations nationally competently and at a reasonable price, would that be preferable to the State running such services when projects such as NHS IT and universal credit have not gone terribly well?
In our jurisdiction, private companies can hide easily being a corporate veil, and are for example currently not readily accountable through freedom of information legislation. This is despite numerous requests to Jeremy Hunt in parliament about parity in disclosure requirements from both private and public providers.
And the track record of some outsourcing companies in the private sector, it is said, has been terrible.
Jeremy Hunt and Norman Lamb are currently in control of NHS and care policy, but there might be a fundamental change in direction from the next Government.
Or there might not be.
Burnham is aware of the influence of the NHA Party. Policy-wise it could be a kick in the goolies.
“I’m gonna find the man who’s selling the NHS and kick him in the goonies” – what @RufusHound‘s son said to him ahead of our euro launch.
— NHA Party (@NHAparty) April 27, 2014
Clearly this should have read ‘goolies’ ideally, but part of the joke might have been that the remark was made by a six-year old (Rufus Hound’s son).
No offence therefore to any Arsenal fans!
In as much the NHAP has a ‘poster boy’, it is Aneurin Bevan.
Numerous offerings from the NHAP have elaborated on a theme of how good it would be if the ‘fight for the NHS’ , which no-one really expected, could pay due respects to the origins of the NHS and the “spirit of ’45”.
The NHAP had its launch for the European elections this morning at the Roxy Bar and Restaurant, Borough High Street, London SE1.

Previously, in the campaign trail, there had been eyebrows raised at something which came from the NHA Party’s direction.
Rufus Hound, a confirmed atheist, is without doubt a compelling force to be reckoned with.

Hound, who announced his desire to stand for the NHA Party on the BBC “Jonathan Ross Show” at the end of January 2014, had made in parody the remark, “David and Jeremy love your children so much they could just die, squealing in ecstasy”.
Even candidate Louise Irvine had been asked about the general area of comment by Andrew Neil.
But Irvine gave an explanation for the comment, and Neil was clearly going through the motions in political discourse.
Here is Louise Irvine’s pitch from today.
Hound explained beyond any reasonable doubt that the comment had been meant as a joke, making a passing reference to Toby Young of ‘free schools fame’, and son of the very influential Labour peer Lord Young.
One of the biggest bits of news of the day was that Marcus Chown, @marcuschown, author of “What a wonderful world: one man’s attempt to explain the big stuff” and other hugely popular science books, announced his intention to stand in the European elections. This is a major coup for the NHA Party as Chown has a remarkable social media presence.
A recurrent theme, unsurprisingly for the European elections, was how the transatlantic trade treaty between the EU-US could, unless properly negotiated, give excessive negotiating power to multinational corporates.
This is now a significant issue in the way the NHS is run, as it potentially takes away too social, economic and political sovereignty through what is technically known as the ‘investor protection clauses’.
It has been frustrating for many that there has been thus far little discussion of this matter in the traditional media, though the people I spoke to this morning, quite unrepresentative of the usual general public, were extremely well informed about the issue.
Dr Clive Peedell MRCP, one of the Co-Leaders of the NHA Party, is a Consultant Oncologist (Physician) in the NHS, with insights into how marketisation in the NHS has gone catastrophically wrong.
He kicked off with the issue this morning:

And resuming the football theme, Hound likened the NHS to a “political football” which was “gradually becoming deflated due to all the kicking by all the major political parties.”
It is inconceivable that the NHA Party will form the next Westminster government on their own, but they have never had public aspirations for that. Because of the way that the European elections work through proportional representation, they have a chance to make an impact in the European elections, though heavily disadvantaged by lack of interest from the mainstream media.
But these are issues which resonate with many.
For example, many people are concerned in the stranglehold that the private finance initiative, criticised recently by Margaret Hodge MP in the influential Public Accounts Committee, has had on NHS policy.
Various frontline nurses explained to me their concerns about unsafe staffing, in not being able to deliver the care that they would like to deliver.
One candidate has even been a registered nurse for 35 years, now specialising in the tricky area of pain management.

The unanimity in the ‘efficiency savings’ in national policy weighs heavily against them.


The analogy to football may not be the right one.
Rugby may be more suitable. It’s possible that an incoming Labour government might have to pick up the ball on May 8th 2015, and issues such as the notorious efficiency savings, PFI and even TTIP might have to be settled by the Chancellor of the Exchequer rather than the Secretary of State for Health at the time.
So continuing the sporting analogies, the ball might end up out of Burnham’s court, and this would indeed be very disappointing for many grassroots activists in the meantime.
But, notwithstanding, the NHA Party, whatever their ultimate fate as individuals, are clearly a bunch of plucky determined individuals who feel they’ve made the correct diagnosis, and do not wish to step back and do nothing. They should be given enormous credit for that, at least.
Burnham goes from strength to strength as ‘striker’, but who’s the David Moyes?
There’s no doubt Andy Burnham MP drives the Conservatives potty.
Despite the Conservatives’ best attempts to annihilate Burnham MP, Burnham keeps on scoring goals.
Meanwhile Jeremy Hunt continues to score blanks, apart from where profits from ‘Hot Courses’ are concerned.
But Burnham is more concerned about the day job, and that is running the NHS to a level of some degree of competence.
Hunt meanwhile continues to run his NHS into the ground, paying for costly advice on the managerial implementation of compassion, when he could be paying nurses to do the professional job they’re trained to do.
So Burnham can certainly hold his head up high as chief striker or scorer for Labour United.
As the Conservatives spit out the oranges from their half-time pep talk, as the oranges were in fact horsemeat due to the abolished Food Safety Agency, it’s time to recapitulate.

Clive Peedell kindly tweeted the other day points on which he would like Labour to play ball.
@legalaware @andyburnhammp 1. Fill £30bn funding gap by abolishing PFI & cracking down on tax avoidance 2. Get NHS exempted from TTIP
— Clive Peedell (@cpeedell) April 22, 2014
Before the 2010 election, Liberal Democrat leader Nick Clegg indeed condemned PFI as “a bit of dodgy accounting – a way in which the government can pretend they’re not borrowing when they are, and we’ll all be picking up the tab in 30 years”. It’s well known that PFI is a relic of the John Major government from 1995 (predating New Labour in fact). In opposition, Osborne pledged that the Conservatives would stop using PFI and denounced Labour for relying so much on a source of finance that he said was “totally discredited”. “We need to find new ways to leverage private-sector investment. Labour’s PFI model is flawed and must be replaced,” Osborne muttered in November 2009. Indeed Margaret Hodge, chair of the powerful Commons public accounts committee, said the coalition had failed to come up with the promised alternative since coming to power. The facts speak for themselves.
And Burnham is handicapped by not being the actual Secretary of State for Health at this crucial time for the NHS.
He nonetheless did go to Strasbourg last month to try to explain the case:
(This is a video recording I took of Andy’s talk at the Southwark Labour meeting recently.)
Labour will need to abolish PFI contracts or renegotiate them or both. But Ed Balls will need to be on the wing to help Burnham shoot. And it’s hoped the football manager is not asleep on the job. Labour has indeed proposed a five point plan to tackle ‘tax avoidance’. Labour supports a form of country-by-country reporting. It would extend the Disclosure of Tax Avoidance Schemes regime, which Labour introduced, to global transactions. It would open, further, open up tax havens, with requirements to pass on information about money which is hidden behind front companies or trusts. Crucially, Labour also wants to see fundamental reform of the corporate tax system. But Peedell’s work is not done.
@legalaware @andyburnhammp 3. Abolish purchaser provider split 4. Improve NHS accountability with transparency & openness — Clive Peedell (@cpeedell) April 22, 2014
The abolition of the purchaser-provider split remains one of the totemic political decisions to be made, as is not a ‘deal maker’ for many grassroots voters.
In fact, the whole issue of whether the general public is interested by public health or competition remains uncertain.
Nonetheless, a pioneering integrated healthcare scheme in New Zealand has improved the care of patients while reducing demand on hospital services.
On the contracting side, the report said that the abolition of the purchaser-provider split in the health system was important as it gave boards the autonomy to decide how to fund their hospitals.
The project was launched in 2007 in response to rising hospital admissions and waiting times and to a population that was ageing more rapidly than in other parts of New Zealand and other developed countries.
Similar to the drive towards whole person care in this jurisdiction, is aim was to create a “one system, one budget” approach to health and social care, together with various aspects as centrepieces: sustained investment in training, support for staff to innovate, and new forms of contracting, including abolition of the split between healthcare service purchasers and providers.
The outgoing NHS England chief executive Sir David Nicholson last year told HSJ his organisation was looking at “whether the straightforward commissioner-provider split is the right thing for all communities”.
Hospitals wish to focus on delivering better services to patients and often get frustrated by the amount of time they have to spend negotiating contracts with commissioners with the legal shutgun pointing in the direction of their necks.
And there’s no doubt there’s a steady stream of whistleblower tragedies, with Raj Mattu the latest in the long line of casualties.
People still struggle to think of a NHS whistleblower who has had a good outcome.
The Nursing Times ‘Speak Out Safely’ has only so far succeeded in signing up 30% of NHS Trusts.
Most people accept that the whole system is rotten, not least in how clinical regulators appear to pass the buck or even worse target whistleblowers.
Many do not think the Public Interest Disclosure Act, enacted by New Labour is 1998, is fit for purpose either.
So Clive Peedell is right, but Andy Burnham may have trouble in shooting goals on target with nobody on wing or a manager more concerned about ‘One Nation’.
Moyes, sacked by United on Tuesday after the 2-0 defeat at former club Everton on Sunday confirmed their failure to secure Champions League qualification, oversaw just 51 games in charge of the team after succeeding Sir Alex Ferguson last summer.
Moyes, like Ed Miliband, though had his army of people who thought he was doing a good job.
But Burnham like many, although focused on sorting out the undeniable problems of the NHS, is avoiding relegation for his team too.
I certainly don’t want to ask who the Ryan Giggs is. That certainly would be tempting fate.
I agree. The effects of the free market on the NHS are indeed terrifying.
Tony Benn said famously, of Tony Blair, “It’s not up to Mr Blair to rename my party. I haven’t suddenly become a member of New Labour. I was never a member of Old Labour.”
There is a therefore a strange cognitive dissonance in this picture to come out of the Spectator factory.
It mixes a parody of the famous Tony Blair ‘evil stare’ with the letters ‘Old Labour’.
Presumably the overall message, unsubtle though it is, is that a vote for Ed Miliband is a vote for socialism.
And the advertising shill in this is that socialism represents a ‘danger’.
No.
Let’s get this clear.
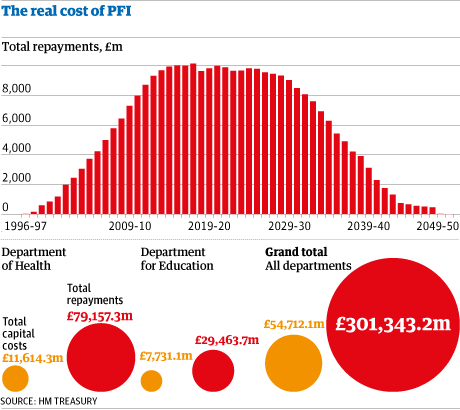
The private finance initiatives led to some investors in the private sector making very good deals on the financing of hospitals and associated services, often with exorbitant profit.
Andy Burnham’s message of letting the market creep in too far is understating the severity of the problem.
There is a plethora of NHS trusts which have been crippled by PFI loan repayment debts.
These loan repayments possibly represent the biggest single threat to the financial stability of the NHS in the forthcoming decades, not the ageing population.
The PFI situation has gone beyond farcicle. An instrument first developed in John Major’s government in 1995, later welcomed with open arms by Tony Blair’s governments and beyond, has clearly been an abuse of power.
Not only can NHS entities conceal their staffing data under freedom of information, but PFI shares in hospitals which may ultimately shut down may be freely traded like carbon credits on the stock market.
That’s what letting the market has become.
You can now hire consultants who are experts and could make you millions on predicting whether your local hospital will shut.
There is no doubt that these market considerations have impacted on the provision of care, which should be made on clinical conditions. And yet the current regulatory set up, which gives a lot of power to Monitor’s elbow, is clearly unable to cope.
It is now widely recognised that the NHS has lacked both the expertise and the resources to cope with the aggressive pimping of services into the private sector.
And private investors are now lining up to provide financing for social value impact bonds, which could help to sustain multinational corporates to enter markets they otherwise would have dreamt of.
This further leads to leeching out of resources away from the NHS to the private sector.
So long as senior leaders in the NHS say technology and innovation need to drive the NHS, you will see further leeching of money into the private markets.
This shift on emphasis, to people ‘finding opportunities in the NHS’, is by far the biggest danger in the NHS. And the political dynamite question is to what extent does Ed Miliband produce a killer stroke?
Everyone concedes the PFI situation is a mess, but should Miliband simply buy back these hospitals into the public sector?
After all buying back shares is common currency currently in corporate land, pardon the pun.
And there is never any shortage of money for illegal wars.
That would be quite a break from New Labour, but the public, and the Spectator know this, might actually welcome a return to state ownership. This is borne out by all the polling evidence in fact.
Despite the undeniable popularity of issues such as immigration considered to be “right wing”, the Spectator might have done Labour a favour – in telling Labour that the Tories are in fact terrified of Miliband and Burnham.
Review: A film by Peter Bach called “Sell off: the abolition of your NHS”
For health reasons, I don’t drink. After a six week coma due to meningitis at the Royal Free, which left me disabled, I have a massively personal reason why I am grateful to the NHS.
This one event taught me that anything can happen at any time. Last night, I went along to a private viewing of “Sell-off: The abolition of your NHS” at the BAFTA in Piccadilly. Not having drunk for alcohol for seven years, I don’t feel any particular urge to drink. In fact, I quite liked the atmosphere of their bar in the complete absence of alcohol. I quite like diet Coke.
The bar made me think of New York in fact in a brief period of escapism from a wet and miserable evening in March in Central London.
While I was sat thinking about how unusual it was for me to go to bars these days, I heard a voice I recognised. Then I suddenly twigged who it was – Tamasin Cave, Director of Spinwatch, was talking with someone about the “Lobbying Tour”. I said as politely as I could to her that the YouTube video of her tour is very famous.
“Famous for a certain group of people perhaps!”, she replied.
Peter Bach’s film, which is currently in an uncut stage, is exquisitely done. It covers all the points you’d expect in a documentary about a piece of legislation which was railroaded in without meaningful discussion. The frames of those people interviewed flow nicely, and the resulting narrative is coherent. I know this particular narrative extremely well, but there were some points for seasoned viewers like me too.
The views on the NHS captured in Bach’s film impressively don’t sound like one spiteful rant, though, which is the really clever aspect of the film. The film is possibly best described as a clear fly-on-the-wall documentary where patients and doctors clearly feel utterly disenfranchised from the NHS. This is of course in total contrast to the humanistic foundations of the NHS in the 1940s.
Peter Bach, the filmmaker, talks about how he went to a basement in Earls Court, to say how “he was bombarded by a litany of complaints” from a group of people concerned about the running of the NHS. Whilst Max Keiser argues in his interview with Peter Bach ‘you can’t put a price tag on the NHS’ (see below), you unfortunately can put a price tag on the costs to make this film. If you’d like to support this very important initiative of public interest, please go to this ‘StartJoin’ website for crowdfunding.
If the film set out to achieve a fascinating overview of the issues engulfing the NHS, it certainly did that. The concern, of course, is that this film ends up ‘preaching to the converted’, and it contains still a mystery why the mainstream media seem reluctant to discuss the running of the NHS. Supporters of NHS privatisation have argued that it doesn’t matter who runs the NHS as long as it’s run well and free at the point of use. Supporters of the NHS privatisation therefore tend to argue that the public do not want to have this debate. Conversely, people who support a NHS which is state-run obviously argue, instead, that this debate does matter; and the film indeed posits very good clear arguments why the market does not work in the NHS. The film clearly states that competition doesn’t work effectively for the NHS; measuring all the activity in the NHS itself wastes resources (going up from about 2% of the budget to 30%). The youthful and inspiring Dr Clive Peedell was spitting bullets at the encroachment of the market – and of course is right.
The film flows effortlessly, for example, from an excellent description bogus nature of running the finances of a hospital, compared to a household budget, by Dr Bob Gill to a mention of indexation in the private finance initiative (PFI) by Prof Allyson Pollock. Pollock is clearly somebody who should have been listened to much earlier. At least Pollock is completely vindicated. Whilst politicians of all shades have argued the beneficial effects of PFI, the concerns are brilliantly enuniciated by Pollock. An on-running theme of this film evidently is that it’s not the case that this is a fait accompli of the corporatisation of the NHS, though time is running out now. Something can be done about PFI contracts (and may require attention due to the repercussions of PFI on freedom of information requests concerning safe staffing). It might be late in the day, but it wouldn’t be too late for a candid repentance. Likewise, the public lawyer states correctly the Health and Social Care Act (2012), which led to the £2.4 million ‘reforms’, can be repealed. And it would take one Bill to restore of the duty of the Secretary of State for Health in running the NHS.
Both Dr Jacky Davis and Dr Louise Irvine speak brilliantly in the film on the issues of the ‘democratic deficit’. Given that the mainstream media have continued to ignore the changes in the NHS traditionally, their opinions are clearly a polite (not desperate) plea for members of the general public to become involved. Meanwhile, in the film itself, Dr Lucy Reynolds, who clearly has many interesting insights about cross-jurisdictional aspects of healthcare systems, describes how she left a U.K. where the N.H.S. was respected to one where the N.H.S. was pilloried on a daily basis. I also had a nice chance to chat with Dr Davis and Dr Irvine before the film, and with Dr Jonathon Tomlinson afterwards.
As I left the theatre and the BAFTA building, I caught sight of Lord Owen. On seeing Owen, I was reminded of an interview by the late Tony Benn. Benn’s remarks about how the SDP had been partly launched as a reaction to the inadequacy of Labour still irritate some. In that particular interview these remarks preceded a diatribe also by Benn about how it wasn’t the Left’s fault that Labour had been unelectable. Bach’s film brilliantly doesn’t shovel the blame at the doorstep of any one political party, though clearly no Government (especially this one) comes out of it particularly well.
Many seasoned commentators have learnt that there is a consistent pattern of unsafe practice, where people have not been empowered to speak out safely. I am very glad that Bach’s film approached this intelligently, in a constructive and altogether non-vindictive manner. Peter Brambleby talks with much dignity about how his concerns well known elsewhere fell on deaf ears. Dr Kim Holt also talks about the well known phenomenon of how whistleblowers are first ostracised before being silenced and finally excluded.
The argument that Foundation Trusts, such as Mid Staffs, allegedly made staff cuts endangering patient safety in the rush to meet financial targets to gain Foundation Trust status is elegantly made. Meanwhile, the 6Cs, and indeed lack of minimum staffing, many believe, do not protect against the basic threat of unsafe staffing on the delivery of NHS care.
In a weird way, the film is as iconic as the best of them such as “Breakfast at Tiffany’s”, despite being in a completely different genre. I think it’s inevitable that this film will connect with people in a way which reflects the subject-matter being more significant than the usual party-politics. If the problem was explaining the complex narrative of the failures of NHS policy in a succinct, understandable manner, Bach has just achieved a First with Distinction. It’s a remarkable piece of work, which, whether you are particularly interested in the NHS or not, deserves to be widely seen; and indeed deserves the highest official praise.
Should we more worried about a Trust in deficit or a deficit in trust?

“You can cut all the flowers but you cannot keep Spring from coming.”
? Pablo Neruda
For all the witch Hunts for looking for someone or something to blame, the number of constructive solutions has been unimpressive.
Some might say some of the media are part of the problem, not the solution, an anonymous friend said. But there are clearly ‘debates to be had’ about the news stories about the NHS which emerge into our popular press in short bursts.
Twitter trolls are people who land from nowhere, insult you and then disappear. They are the internet version of a random person sitting next to you on a crowded London bus, punching you in the face, and then getting off at the next stop.
And that’s the way we’re engaged in a debate about the NHS.
The French curiously have an opposite in their language to the word ‘inevitability’. It is called ‘evitability’. Part of the reason, I feel, that people feel so depressed is that they do not feel that they have actual control over the NHS policy in England from all the mainstream political parties.
Healthcare is expensive, but the NHS, when compared by percentage of GDP spent on health with countries with similar outcomes, is very good value for money. And yet it turns out that almost one in three NHS trusts in England is now forecasting they will end the financial year overspent, official figures show.
The term “self-fulfilling prophecy” was coined in 1948 by Robert Merton to describe “a false definition of the situation evoking a new behavior which makes the originally false conception come true”. He illustrated the concept with a run on a bank (a fictitious “parable”); his main application was to racial discrimination. The term has since entered social science and even everyday English, a rare feat for a sociological neologism.
So we are told that more NHS organisations are now in difficulty, compared with the same point last year. So what are we going to do about it?
There is no alternative (shortened as TINA) was a slogan often used by the Conservative British Prime Minister Margaret Thatcher. In economics, politics, and political economy, it has come to mean that “there is no alternative” to economic liberalism—that free markets, free trade, and capitalist globalisation are the best or the only way for modern societies to develop. The phrase may be traced to its emphatic use by the nineteenth-century classical liberal thinker Herbert Spencer.
But this lack of control, partly due to the quite manipulative way the debate tends to be framed by ‘influential’ thinktanks and media outlets, can lead to general dysphoria, perhaps apathy or depression. This is clearly relevant if members of the chattering political classes wish to seek out reasons why many potential voters feel disenfranchised.
A similar phenomenon is now happening with gusto, regarding NHS policy. That’s because we’re not offered any solutions, and feel powerless in controlling events.
Services have also been told to put aside £15bn in efficiency savings by 2015, in order to cushion themselves against further rises in demand.
This is clearly relevant to the ability of the NHS to hire new nurses. Many organisations are spending heavily on agency staff, with a 60 per cent rise in the total bill for locum doctors in the past three years, with doctors being paid up to £1,500 a shift.
Many of the worst problems are in London, where Barts Health NHS trust is predicting a deficit of £50m by the end of the financial year, and has drawn up plans to reduce the numbers of nursing staff on the wards.
Although the NHS has been protected from savings cuts, the demands from an ageing population and increasing costs of drugs mean services are struggling to meet demands on them, according to some ‘experts’.
The idea “reform is inevitable due to the ageing population” is immediately harpooned by issues when you look at the small print. For example, the cost savings from expensive cholinesterase inhibitors used to treat the symptoms of Alzheimer’s Disease to modest effect might be better put to use in guiding persons with inexpensive interventions to promote living well with dementia.
Professor John Lister, a health expert at Coventry University, said: “There are going to be more hospitals running into trouble due to debt problems.
“Some of the debts are astronomical. Repayments would have been tough enough in normal times but the recession and the need to cut £20billion from NHS spending has been the straw that broke the camel’s back.”
It’s a bit hit-or-miss whether you get a full account of events from such news items. For example, many articles couch the staffing of the NHS as a luxury, completely ignoring the issue that there is a minimum safe level of staffing on wards, whether Jeremy Hunt wishes to legislate for this or not.
Controversial private finance initiative which allowed more than 20 hospitals to borrow at high interest rates to secure new buildings have left some struggling to pay off the expensive mortgages, repayments can be up to five times the building costs.
The assumption that an ageing population makes the NHS unsustainable is not completely backed up by evidence. Indeed, increased life expectancy can increase the economic contribution of individuals, and need not be accompanied by increased morbidity – a concept known as ‘compression of morbidity’.
But should we more worried about a Trust in deficit or a deficit in trust?
David Cameron also promised to safeguard the NHS, lead the greenest government ever, create a fairer and more equal society, clamp down on tax evasion and clean up politics…
Regarding ‘clause 118′ giving special powers for a firestorm of NHS reconfigurations, Grahame Morris, Labour MP for Easington, recently commented,
“If the clause is agreed, we can expect tensions to be further exacerbated, and it should serve as a warning to us that the lack of meaningful consultation in the trust special administrator process leaves a huge democratic deficit and a black hole in accountability. ”
By the time the Health and Social Care Bill passed into law, becoming an Act, on 20th March 2012, it had garnered almost universal condemnation, with unprecedented agreement between the medical Royal Colleges, the British Medical Association, the Royal College of Nursing, the Royal College of Midwives, and many others – not forgetting nearly 180,000 signatures on the ‘Drop the Bill’ Government e?petition (the second?most signed petition on the site).
With the new construct of ‘accountability’ in the NHS, including for example Health and Wellbeing Boards and HealthWatch, it is hard to see how competitive tendering decisions can be challenged effectively without recourse to the law courts.
And now the Information Commissioner’s Office is concerned that the information provided to patients on care.data is not clear enough about how to opt out of the programme. The fiasco over care.data was possibly avoidable if the information leaflet had not been so badly prepared, and NHS England had given the appearance of seeking informed consent from individuals in the general public.
I think a Trust in deficit and a deficit in trust are all part of the same problem – a rational debate about the NHS being completely misrepresented in the media such that things which could be avoided are presented as inevitable.
I will inevitably buy a new car, but the longer I drive my current one only delays the inevitable. But allowing a storm to flood my car could speed up my search for a new car. In this case, God’s inevitability overruled my delay.
Likewise, from Cornwall to London, to Cardiff, Leeds and Northumberland, is it true that local authorities across England and Wales have been ignoring the Environment Agency’s protests and waving through developments on flood-prone land?
What Labour must do to prove that the NHS is ‘safe in its hands’

The problem with the mantra, “The NHS is safe in our hands”, is that it sums up a lean-management approach to management of the NHS. Whilst heralded by some as a ‘success’ in the National Health Service as an efficient way of doing things, its reputation in the private sector is rather more notorious. It is associated with a ‘just-in-time’ approach, where things are always done at the last minute. Where there is relevant to operations management is that if anything untoward happens the system becomes quite unable to cope. Take for example a major road traffic accident, or any similar clinical incident.
Labour will ultimately wish more than the basic aspiration that “NHS is safe in its hands”. This would be like me reassuring you if you asked me to childmind your baby, “You can rest assured that I won’t kill your lovely baby tonight.” And yet possibly expectations for the NHS have become rather low. The formidable campaigner, Marcus Chown, has a tweet which you often see in circulation thus:
Take for example this tweet from 18 March 2012:
 Many accept this claim to be a bare-faced lie. The idea that David Cameron and the Conservative Party are simply pathological liars about the NHS is not new. They intended a full-blown reorganisation of the #NHS prior to coming into Government, and yet stubbornly refused to put it in their 2010 manifesto. Further to this, Cameron has previously made pledges to save A&E hospitals which his Government has subsequently shut down, and yesterday did a full-frontal U-turn on minimum pricing in alcohol. In terms of currency in credibility, Cameron needs to ‘sell, sell, sell’, encapsulated in the spirit of another famous tweet by Marcus Chown:
Many accept this claim to be a bare-faced lie. The idea that David Cameron and the Conservative Party are simply pathological liars about the NHS is not new. They intended a full-blown reorganisation of the #NHS prior to coming into Government, and yet stubbornly refused to put it in their 2010 manifesto. Further to this, Cameron has previously made pledges to save A&E hospitals which his Government has subsequently shut down, and yesterday did a full-frontal U-turn on minimum pricing in alcohol. In terms of currency in credibility, Cameron needs to ‘sell, sell, sell’, encapsulated in the spirit of another famous tweet by Marcus Chown:
 Again, it’s a case maybe of, “If I were starting now, I wouldn’t go from here.” But we’re now stuck with the Health and Social Care Act (2012), that is until Labour decides to repeal it. However, that as we all know is only part of the story. Removing the 50% of cap from private income (section 164(1)(2A)) and redrafting the Regulations associated with procurement such that the default option is not price competitive tendering (section 75) should be the relatively easy parts. There’s still the problem for all parties of how the NHS can be legislated for integration, as strictly speaking bundling offends EU competition law if it distorts trade.
Again, it’s a case maybe of, “If I were starting now, I wouldn’t go from here.” But we’re now stuck with the Health and Social Care Act (2012), that is until Labour decides to repeal it. However, that as we all know is only part of the story. Removing the 50% of cap from private income (section 164(1)(2A)) and redrafting the Regulations associated with procurement such that the default option is not price competitive tendering (section 75) should be the relatively easy parts. There’s still the problem for all parties of how the NHS can be legislated for integration, as strictly speaking bundling offends EU competition law if it distorts trade.
Ed Miliband has been deeply immersed in a debate about party funding and transparency. Whilst Matt Forde claimed this week on “This Week”, the flagship politics show presented by Andrew Neil, that the Unions to have a “strangehold” on the Labour Party, it is not terribly certain how robust Labour’s opposition to Royal Mail privatisation will be. It is also noteworthy that UNISON violently opposed the ‘Private Finance Initiative’, admittedly brought in through Ken Clarke and John Major in the mid 1990s, but which Labour (and the Conservatives) have subsequently embraced. The loans for PFI have benefited the private sector, and the funding of NHS Foundation Trusts via this route has led some lawyers representing these trusts to withhold vital information such as staffing levels on the grounds that such information is “commercially sensitive”.
Therefore, Labour, even if offers a ‘safe alternative’ to the funding gap and the mechanism of procurement in a future Government, does not offer anything startingly different on the Private Finance Initiative. This would not matter if this issue was completely unknown to voters, but the issue is very well known. Some members of the public know that it is known as ‘off ledger accounting’, and that City firms are still very positive about it. Andy Burnham MP has long argued that the PFI was essential for improving the infrastructure of hospitals, e.g. spanking new businesses, but this is small beer for wards and NHS services being stripped to the bone. NHS Trusts being run with a skeleton staff at full capacity, such that Doctors and nurses feel they can’t cope, are becoming commonplace. This is as being justified in terms of the ‘necessary’ £20bn of NHS savings which have to be found until 2020 at least. No party wishes to challenge these savings, and that is partly the reason they find Sir David Nicholson a useful lightning conductor. He is the natural conduction rod for public anger, and indeed the Daily Mail’s anger, whereas all that is happening is that the messenger is being shot, and another messenger will possibly take over next year, for example Mark Britnell.
Labour does not wish to challenge the idea that the NHS is being stripped of necessary funds to do the job properly. If the demands from ageing and technological advances have increased as Nicholson and others claims, surely it is unfeasible to maintain the same level of service when you are barely changing the budget in incremental terms from year to year? Labour’s failure to challenge this dogma is at the heart of its other failings. It cannot embrace the disasters at Mid Staffs and Morecambe Bay while it is fully signed up to efficiency savings. Nobody can deny that any large organisation needs to be run at maximum productivity and efficiency, but when there is consistent robust evidence that adequate numbers of Doctors and Nurses saves lives this is a problem. Labour’s new line of attack is that the “hedgies” (hedge funds) have a strangehold on Tory policy, a weapon utilised to great effect by Ed Miliband in Prime Ministers’ Questions only this Wednesday (10 July 2013). It is a poorly kept secret that private sector entities made massive donations to the Conservative Party prior to the 2010 General Election, and as a result of the new NHS legislation, this situation latterly appeared (source):

For all the ranting by the Conservatives and Labour about “choice”, ultimately voters seem to have little choice where it matters. Citizens of Trafford and Lewisham appear to have little choice over their A&Es locally shutting. Reconfigurations seem to happen from Jeremy Hunt with little consultation with the public. Labour’s public opposition to these distressing reconfigurations seems to be minimal, in a way almost to suggest a collusion with the Government agenda to “reconfigure to save money”. And the dogma of the efficiency savings from the Department of Health goes unchallenged, including the surplus returned to the Treasury, in parallel to the big ticket numbers expenditure-wise going unchallenged. How come it’s possible to find the billions of HS2, another initiative which few people remember ‘voting for’, which has a dodgy business plan, and yet is unanimously agreed upon by all parties (like PFI)? It has become unacceptable to challenge anything coming out of the private sector, whether it’s the efficiency savings advised by McKinsey’s who have been advising on re-disorganisations since time began, well certainly since 1974 anyway. Coupled with this with toothless regulators (and in the CQC’s case a regulator which is allocating resources to protect its own reputation and whose own Report it is alleged is a ‘cover up of a cover up’), it is possible that the damage done by efficiency savings will go unnoticed. If the focus remains on reputational succes of NHS Trusts, and the reputational success of politicians of all ilk, any collusion between the Regulators and politicians to achieve NHS Foundation Trust will be disastrous. Andy Burnham has vehemently denied that there has been any such pressure thus far, but the future of the NHS Foundation Trust is highly relevant. Despite it being a noteworthy policy failure in Spain, the widespread conversion of hospitals to NHS Foundation Trusts could be the perfect stepping stone for super-hospitals, and in a market where supplier power is King, they may prove yet to be the perfect vehicle for the final part of NHS privatisation.
The thing is while it is easy to hide poor financial performance of the hospital, and this is after all the metric that will pay the salaries of CEOs in NHS Foundation Trusts, it is alarmingly easy to hide morbidity and excess mortality of NHS hospitals. Nobody wants to go into hospital to put their own life at risk, and yet we have this ludicrous situation, generated by all the political parties, where nobody accepts blame, and senior managers are in a ‘revolving door’ around the system with generous rewards for, ultimately, failure. The idea of the National Health Action party being the next Government is frankly ludicrous, which is why it is all the more important that Labour can strengthen its relationship with the Unions. However, the efforts of the NHA Party in putting this crucial agenda on the map are completely worthwhile if they move forward from being simply a ‘party of protest’. Maybe despite having been born out of the Unions to represent workers in Parliament, Labour does not feel that it should offer unfair advantage to the Unions, but this would be catastrophic in policy terms. The “democratic deficit” on the NHS is extremely bad, with the general public and the medical professions completely ignored on a range of issues, most recently plain packaging of cigarettes and minimum alcohol pricing. It’s the singularly obsessional Labour phobia of the perception of its relationship with the Unions with the right-wing press which means that it too might easily go down the route of being susceptible to powerful corporate lobbying over diet, alcohol, smoking, and the such like. This stems from the basic issue of turning the NHS into a profitable business, as a “wealth creator”. It is a world apart from “The Spirit of 45″, and Labour knows that it is sitting on an extremely comfortable lead of about 10% compared to the Conservatives.
Labour has to learn not to abuse this public faith in it regarding the NHS, and take a “second look” at NOT embracing a neoliberal, un-evidence based approach to medicine. It, like the NHS, has to learn from failure. Whilst whole-person or integrated care is important, it must never become, fundamentally, distraction therapy from the threats still posed by PFI and efficiency savings. Labour has been desperate for the Risk Register to be published, but it is highly likely that the Risk Register will also expose failures from their watch in Government.
It’s not the case that Labour is ‘sleepwalking’ into a disaster. It already has sleep-walked into a disaster, and it’s high time to retreat. Soon, it will be the case, at best, that people are not wishing to vote Labour over the NHS, but they represent “the best of a bad bunch”. Yet this ironically is entirely in keeping with the “just in time” philosophy of doing the rock bottom or “more for less”. Labour appears to be suffering from a ‘poverty of aspiration’, and whilst the emphasis in policy seems to be one of ‘equality of opportunity’ for profit-making healthcare private providers, it is this poverty of aspiration that might ultimately kill the NHS.
The author can easily be contacted on Twitter @legalaware.
Dr Lucy Reynolds with a very clearly evidenced explanation of UK NHS privatisation

“Patient choice? Always choose the NHS”
Dr Lucy Reynolds is an academic in health policy at the London School of Hygiene and Tropical Health (for biography, please see here.) In a wide-ranging interview with Jill Mountford, Dr. Reynolds explains in very clear language how English health policy has progressed in recent years, charting the progress of the current legislation enabling the NHS privatisation. However, Dr. Reynolds states clearly that the current developments in the NHS privatisation would have been virtually impossible but for the policy developments under New Labour from the mid 2000s. Dr Reynolds also explains how the idea of PFI was sold to the private sector and public in different ways, and has been an important step for this privatisation routemap.
Dr Reynolds’ analysis is crystal-clear. What has been frustrating is how senior journalists, including at the BBC, have “failed to understand” the process sufficiently to be able to describe it ‘for the public good’. It is extensively referenced, and also draws on findings and observations from other jurisdictions about “lessons learnt” about the organisation of their healthcare. She describes the recent section 75 Regulations (both the original one and as amended) as the “jet engine” for the “plane” of privatisation which was launched last year, but notes that nobody knew what the jet engine precisely was until relatively recently. Furthermore, Reynolds notes that the legislation sets up a competitive market blatantly rigged in the favour of private entities who can operate in the marketplace, and establishes the supporting evidence for that.
As you’ll see from the comments on this YouTube thread, the explanations have been very well received.
For some further explanations of aspects of this narrative, I have blogged on this website, as described here:
“Competition Regulations issued under Section 75 of the Health and Social Care Act (2012) will lock CCGs into arranging all purchasing through competitive markets”
my blogpost on 7 January 2013 here
“The privatisation of the NHS appears to be going to plan”
my blogpost on 3 January 2013 here
“Rainbow coalition warns about section 75 NHS regulations”
my blogpost on 27 February 2013 here
Further reading
“NHS Plc” by Prof Allyson Pollock
“The plot against the NHS” by Prof Colin Leys and Stewart Player
