Home » Competition and markets
“Think like a multinational corporate leader. Act like the chief of the NHS.”
Simon Stevens’ catchphrase is: “Think like a patient, act like a taxpayer.”
In 2013, the US and EU decided to start negotiations on a new free trade agreement, the Transatlantic Trade and Investment Partnership (TTIP).
In a recent piece for the New Statesman, the most notable comments by Andy Burnham MP in George Eaton’s interview concerned TTIP and its implications for the NHS (apart from he was spitting bullets at aspects of HS2).
Many Labour activists and MPs had been concerned, according to George, “at how the deal, officially known as the Transatlantic Trade and Investment Partnership (TTIP), could give permanent legal backing to the competition-based regime introduced by the coalition.”
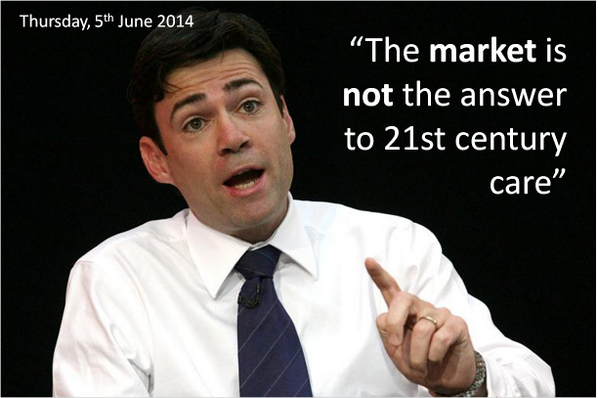
And here was Andy again at the start of the European elections (not reported by the media who were much more interested in Nigel Farage, Roger Helmer, and their ilk.)
As Benedict Cooper wrote recently on The Staggers for the New Statesman:
“A key part of the TTIP is ‘harmonisation’ between EU and US regulation, especially for regulation in the process of being formulated. In Britain, the coalition government’s Health and Social Care Act has been prepared in the same vein – to ‘harmonise’ the UK with the US health system.
“This will open the floodgates for private healthcare providers that have made dizzying levels of profits from healthcare in the United States, while lobbying furiously against any attempts by President Obama to provide free care for people living in poverty. With the help of the Conservative government and soon the EU, these companies will soon be let loose, freed to do the same in Britain …
… The agreement will provide a legal heavy hand to the corporations seeking to grind down the health service. It will act as a transatlantic bridge between the Health and Social Care Act in the UK, which forces the NHS to compete for contracts, and the private companies in the US eager to take it on for their own gain.”
So fast forward a few months.
Ed Miliband asked David Cameron today specifically how TTIP would impact on the NHS.
Cameron reported today that there had been five good meetings on progressing it, and continued thus:
“We are pushing very hard and trying to set some deadlines for the work. No specific deadline was agreed, but it was agreed at the G7 that further impetus needed to be given to the talks and, specifically, that domestic politicians needed to answer any specific questions or concerns from non-governmental organisations, or indeed public services, that can sometimes be raised and that do not always, when we look at the detail, bear up to examination.”
And the attack on NGOs continued:
“I do think this is important because all of us in the House feel—I would say instinctively—that free trade agreements will help to boost growth, but we are all going to get a lot of letters from non-governmental organisations and others who have misgivings about particular parts of a free trade agreement. It is really important that we try to address these in detail, and I would rather do that than give an answer across the Dispatch Box.”
So the upshot was Cameron agreed to write to Miliband in detail to provide an update on TTIP and the NHS at last.
And this is not a moment too soon – it’s almost a year to the day since @Debbie_Abrahams asked about this on 19 June 2013 (see here).
Cameron tried also to advance the rather bizarre argument that TTIP would lift people out of poverty, trying to link up in a very Conservative approach to the free trade arrangements and the social determinants of health.
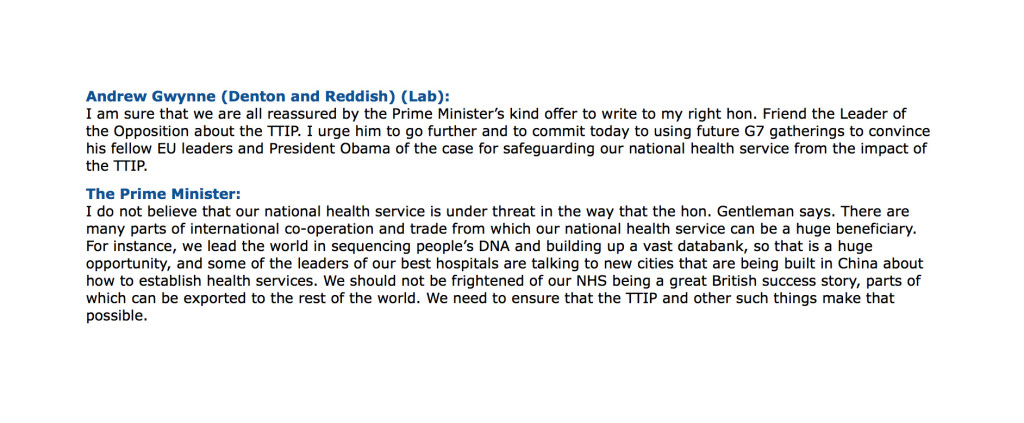
The most helpful exchange, perhaps however, was between Andrew Gwynne and the Prime Minister this afternoon:
From the late 1980s, a narrative surrounding the ethics and economics of human gene patents has been taking shape into a ‘perfect storm’.
The discussion included impact of gene patents on basic and clinical research, on health care delivery, and on the ability of public health care systems to provide equitable access when faced with costly patented genetic diagnostic tests.
Scientists at institutions around the world discovered and sequenced a series of genes linked to breast and ovarian cancer in the early 1990s.
Mutations in these genes prevent the body from producing tumor suppressing proteins, which in turn increases an individual’s risk of contracting breast or ovarian cancer.
A key discovery, for example, was that individuals with these mutations have a cumulative lifetime risk of ~40–85% of developing breast cancer and ~16–40% chance of developing ovarian cancer, compared with 12.7% and 1.4% risk for the general population of developing breast or ovarian cancer, respectively.
So with these cutting edge findings in research, ‘translationary’ laboratories developed diagnostic tests for these mutations, which opened up the possibility of preventive management for breast and ovarian cancer, including prophylactic surgery and the use of certain medications.
There are countless other examples.
There also has been talk about doing a genomic screen with a view to identifying genetic risk factors for the dementias.
And Simon Stevens lovebombed the idea last week at the NHS Confederation:
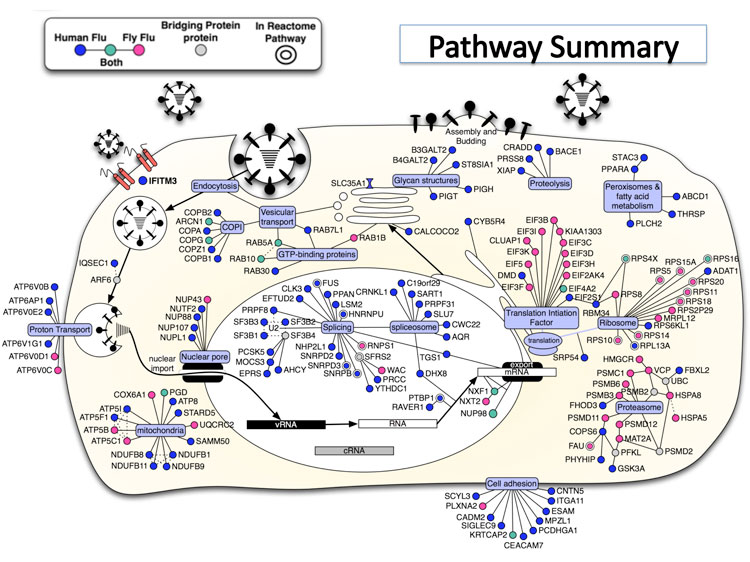
“First, personalisation. A decade and a half on from the Human Genome Project, we’re still in the early days of the clinical payoff. But as biology becomes an information science, we’re going to see the wholesale reclassification of disease aetiologies. As we’re discovering with cancer, what we once thought of as a single condition may be dozens of distinct conditions. So common diseases may in fact be extended families of quite rare diseases. That’ll require much greater stratification in individualised diagnosis and treatment. From carpet-bombing to precision targeting. From one-size-fits many, to one-size-fits-one.”
So a more appropriate catchphrase for Simon Stevens might be:
“Think like a multinational corporate leader. Act like the chief of the NHS.”
One concern has been that TTIP powers would jeopardise well entrenched national laws and regulations.
Frances O’Grady of the UK’s Trade Union Congress for example, is publicly concerned that deregulation and bolstering of corporate rights could mean an accelerated privatisation of the UK’s National Health Service.
“The clauses [of ISDS] could thwart attempts by a future government to bring our health service back towards public ownership”.
A “socialist planned economy” combines public ownership and management of the means of production with centralised state planning, and can refer to a broad range of economic systems from the centralised Soviet-style command economy to participatory planning via workplace democracy.
In a centrally-planned economy, decisions regarding the quantity of goods and services to be produced as well as the allocation of output (distribution of goods and services) are planned in advanced by a planning agency.
According to Linda Kaucher, quoted in the New Statesman:
“[The Health and Social Care Act] effectively enforces competitive tendering, and thus privatisation and liberalisation i.e. opening to transnational bidders – a shift to US-style profit-prioritised health provision.”
“The TTIP ensures that the Health and Social Care Act has influence beyond UK borders. It gives the act international legal backing and sets the whole shift to privatisation in stone because once it is made law, it will be irreversible. Investor State Dispute Settlement (ISDS) laws, fundamentals of the agreement, allow corporations legal protection for their profits regardless of patient care performance, with the power to sue any public sector organisation or government that threatens their interest.”
“Once these ISDS tools are in place, lucrative contracts will be underwritten, even where a private provider is failing patients and the CCG wants a contract cancelled. In this case, the provider will be able to sue a CCG for future loss of earnings, thanks to the agreement, causing the loss of vast sums of taxpayer money on legal and administrative costs.”
Given also Andy Burnham’s reported opposition to TTIP, it would be absolutely ludicrous for the Socialist Health Association to adopt any position other than to oppose the parts of TTIP which are clearly to the detriment of the NHS. This situation, I feel, has arisen because “leaders” who’ve never set foot on a ward in a clinical capacity have little understanding of the social capital of its workforce: doctors, nurses, healthcare assistants, and all allied health professionals. It will be painful for members of the Socialist Health Association if they wish to collude knowingly with this non-socialist agenda. This is all the more telling as the Socialist Health Association seem bizarrely silent concerning the pay freeze for much of the nursing workforce.
And so the NHS strategy is beginning to take shape – parallel worlds of grassroots clinical service delivery (the unprofitable bit which costs money), and the more lucrative bit (where the State can use patient data taken from the general public on the basis of presumed con set to develop diagnostic tests and treatments, with the help of investment from venture capitalists and large charities, to export to the rest of the world under free trade agreements).
It is time for the Socialist Health Association to work out who exactly they represent?
TTIP makes intellectual asset stripping look like taking candy from a baby.
And the jury is out on Simon Stevens and the think tanks, many people will also say. But this is possibly a lost cause.
So we wait with baited breath for Ed Miliband’s reaction to David Cameron’s note about TTIP. Hopefully they will not simply agree to this agenda, ever increasing the democratic deficit.

Why are English policy wonks fixated on the dangerous wrong policy of competition for their NHS?

A series of different amendments are coming from various sources to ask Andy Burnham to scrap the market in the NHS.
And indeed Andy Burnham claims to be well aware of the dangers of the introduction of a sort of-market to the NHS:
In recent years, there has been clear unease at policy wonks ‘doing’ the traditional circuits in think tanks, known to feather each other’s nests, with no clinical backgrounds (including no basic qualifications in medicine or nursing), pontificating at others for a cost and price how to run the NHS in England.
Think tanks have been part of the discussion, with blurred lines between marketing and shill and academic research, exasperating the real research community.
The King’s Fund boasts that, “Providing patients with choice about their care has been an explicit goal of the NHS in recent years. Competition is viewed by the government as a way of both providing that choice and giving providers an incentive to improve. The Health and Social Care Act set out Monitor’s role as the sector regulator with a specific role of preventing anti-competitive behaviour in health care.”
Chris Ham, who has previously marvelled voluptuously at the US provider Kaiser Permanente in the British Medical Journal, goes hammer and tong at it on an article on competition here.
The theme or meme comes up as a recurrent bad smell in the impact assessment for the Health and Social Care Bill here, citing in the need to consider equality concerns in competition the reference Gaynor M, Moreno-Serra R, Propper C, (July 2010) Death by Market Power Reform, Competition and Patient Outcomes in the National Health Service. NBER Working Paper No. 16164, July 2010.
The authors of that impact assessment nonetheless reassuringly observe that “Gaynor et al (2010) found competition impacted differently across certain areas with possible negative impacts on transgender and black and minority ethnic (BME) people. However, further evidence implies that these risks, associated with increasing competition, should not be overstated and may not impact upon equality issues.”
Andy Burnham – and Labour – have pledged many times that the repeal of the failed Health and Social Care Act (2012) will be in the first Queen’s Speech of a Labour government.
Policy wonks are human beings, and can fail.
It is well-known that many errors in anesthesiology are human in nature. It’s argued that because equipment failure is an infrequent explanation for mishaps in the hospital, clinicians should be aware of the human factors that can precipitate adverse events.
While there are various types of human errors that can lead to complications, “fixation errors” are relatively common and deserve particular attention. Fixation errors occur when clinicians concentrate exclusively on a single aspect of a case to the detriment of other more important features. This is exactly what has happened with the undue prominence of the benefits of competition in the NHS.
Put simply, without any of the bullshit, competition is simply the crow bar which puts private providers into the NHS.
Milburn and Hewitt have been reading from this narrative from ages, and it threatens to engulf Labour yet again. Burnham is fighting a battle for the soul of the party now, and one can only speculate how successful he will be. He has said on many occasions that collaboration is the key to running the NHS in England, not competition; integration not fragmentation; people before profit.
But if you look beyond the lobbying – you can find the evidence right before your eyes. Jonathon Tomlinson through an excellent blogpost of his refers to a large body of literature from Professor Don Berwick which has been in the literature. This is clearly worth revisiting now.
The New Statesman published last week an article which should make senior healthcare policy wonks in England weep.
Martin Bromiley is neither a doctor, or a health professional of any kind. He is not even a member of the revolving door policy wonks in English healthcare policy. Bromiley is an airline pilot.
“Early on the morning of 29 March 2005, Martin Bromiley kissed his wife goodbye. Along with their two children, Victoria, then six, and Adam, five, he waved as she was wheeled into the operating theatre and she waved back.”
A room full of experts were fixated on intubating her, instead of doing a tracheostomy, which indeed Bromiley indeed asked for. A tracheotomy is a cut to the throat to allow air in.
What happened next was incredible.
“If the severity of Elaine’s condition in those crucial minutes wasn’t registered by the doctors, it was noticed by others in the room. The nurses saw Elaine’s erratic breathing; the blueness of her face; the swings in her blood pressure; the lowness of her oxygen levels and the convulsions of her body. They later said that they had been surprised when the doctors didn’t attempt to gain access to the trachea, but felt unable to broach the subject. Not directly, anyway: one nurse located a tracheotomy set and presented it to the doctors, who didn’t even acknowledge her. Another nurse phoned the intensive-care unit and told them to prepare a bed immediately. When she informed the doctors of her action they looked at her, she said later, as if she was overreacting.”
This is not the first time that a ‘fixation error’ has had disastrous consequences.
Another example happened on 28 December 1978, the United Airlines Flight 173.
A flight simulator instructor Captain allowed his Douglas DC-8 to run out of fuel while investigating a landing gear problem.
It’s a miracle that only ten people were killed after Flight 173 crashed into an area of woodland in Portland; but the crash needn’t have happened at all.
In a crisis, the brain’s perceptual field narrows and shortens. We become seized by a tremendous compulsion to fix on the problem we think we can solve, and quickly lose awareness of almost everything else. It’s an affliction to which even the most skilled and experienced professionals are prone.
In March 2012, Professor Allyson Pollock wrote an article in the Guardian, stating ‘Bad science should not be used to justify NHS shakeup’.
In this article, Pollock argued that pro-competition arguments from economists Julian Le Grand and Zack Cooper at the London School of Economics had produced an incredibly distorting effect on what was an important discussion and, “[raised] serious questions about the independence and academic rigour of research by academics seeking to reassure government of the benefits of market competition in healthcare.”
Pollock argues that such colleagues had been sufficiently successful for David Cameron to declare “Put simply: competition is one way we can make things work better for patients. This isn’t ideological theory. A study published by the London School of Economics found hospitals in areas with more choice had lower death rates.”
It is reported in one case, the previous chief of NHS England, Sir David Nicholson KCB CBE “said a foundation trust chief executive had been told he could not “buddy” with a nearby trust ? under plans announced last week to help struggling providers ? because “it was anti-competitive”.
He continued: “I’ve been somewhere [where] a trust has used competition law to protect themselves from having to stop doing cancer surgery, even though they don’t meet any of the guidelines [for the service].”
“Trusts have said to me they have organised, they have been through a consultation, they were centralising a particular service and have been stopped by competition law. And I’ve heard a federated group of general practices have been stopped from coming together because of the threat of competition law.”
“All of these [proposed changes] make perfect sense from the point of view of quality for patients, yet that is what has happened.”
Meanwhile, there was more product placement for providers including Kaiser Permanente yesterday by Jeremy Hunt in parliament:
“From next year, CCGs will have the ability to co-commission primary care alongside the secondary and community care they already commission. When combined with the joint commissioning of social care through the better care fund, we will have, for the first time in this country, one local organisation responsible for commissioning nearly all care, following best practice seen in other parts of the world, whether Ribera Salud Grupo in Spain, or Kaiser Permanente and Group Health in the US..”
Everyone appears to be fixated apart from the most junior in the room, or people like me who wouldn’t want to touch these jobs in think tanks with a barge pole.
It is indeed a badge of honour for me that the feeling is likely to be mutual.
Competition does not explain whether a person who has had chest pains due to a clogging heart should have a physical stent to open up the pipes of blood in his heart, or whether he needs tablets he can take. That is down to clinical professional acumen.
Competition with few big providers can lead to massive rip offs in prices, because of the way these markets work (these markets are called ‘oligopolies‘).
And all too easily providers can be in a race to the bottom on quality, cutting costs to maximise profits.
Remember Carol Propper’s research being used to bolster up the failed plank of competition in the Health and Social Care Act impact assessment?
Wow.
Here she is again in the speech by Simon Stevens, the new NHS England chief, being used in a slightly new context for his speech before the NHS Confederation last week: of the “sensible use” of competition in the NHS (somewhat reminiscent of the use of the words “sensible use” in the context of another potentially disastrous area of policy – targets):
“If we want to be evidence-informed in our policy making and commissioning lets pay heed to research from Martin Gaynor, Mauro Laudicella and Carol Propper at Bristol University. They’ve spotted the striking fact that between 1997 and 2006 around half of the acute hospitals in England were involved in a merger. Their peer-reviewed results found little in the way of gains.”
These fixation errors are causing damage to the English NHS.
It’s time some people got out of the cockpit.
I agree. The effects of the free market on the NHS are indeed terrifying.
Tony Benn said famously, of Tony Blair, “It’s not up to Mr Blair to rename my party. I haven’t suddenly become a member of New Labour. I was never a member of Old Labour.”
There is a therefore a strange cognitive dissonance in this picture to come out of the Spectator factory.
It mixes a parody of the famous Tony Blair ‘evil stare’ with the letters ‘Old Labour’.
Presumably the overall message, unsubtle though it is, is that a vote for Ed Miliband is a vote for socialism.
And the advertising shill in this is that socialism represents a ‘danger’.
No.
Let’s get this clear.
The private finance initiatives led to some investors in the private sector making very good deals on the financing of hospitals and associated services, often with exorbitant profit.
Andy Burnham’s message of letting the market creep in too far is understating the severity of the problem.
There is a plethora of NHS trusts which have been crippled by PFI loan repayment debts.
These loan repayments possibly represent the biggest single threat to the financial stability of the NHS in the forthcoming decades, not the ageing population.
The PFI situation has gone beyond farcicle. An instrument first developed in John Major’s government in 1995, later welcomed with open arms by Tony Blair’s governments and beyond, has clearly been an abuse of power.
Not only can NHS entities conceal their staffing data under freedom of information, but PFI shares in hospitals which may ultimately shut down may be freely traded like carbon credits on the stock market.
That’s what letting the market has become.
You can now hire consultants who are experts and could make you millions on predicting whether your local hospital will shut.
There is no doubt that these market considerations have impacted on the provision of care, which should be made on clinical conditions. And yet the current regulatory set up, which gives a lot of power to Monitor’s elbow, is clearly unable to cope.
It is now widely recognised that the NHS has lacked both the expertise and the resources to cope with the aggressive pimping of services into the private sector.
And private investors are now lining up to provide financing for social value impact bonds, which could help to sustain multinational corporates to enter markets they otherwise would have dreamt of.
This further leads to leeching out of resources away from the NHS to the private sector.
So long as senior leaders in the NHS say technology and innovation need to drive the NHS, you will see further leeching of money into the private markets.
This shift on emphasis, to people ‘finding opportunities in the NHS’, is by far the biggest danger in the NHS. And the political dynamite question is to what extent does Ed Miliband produce a killer stroke?
Everyone concedes the PFI situation is a mess, but should Miliband simply buy back these hospitals into the public sector?
After all buying back shares is common currency currently in corporate land, pardon the pun.
And there is never any shortage of money for illegal wars.
That would be quite a break from New Labour, but the public, and the Spectator know this, might actually welcome a return to state ownership. This is borne out by all the polling evidence in fact.
Despite the undeniable popularity of issues such as immigration considered to be “right wing”, the Spectator might have done Labour a favour – in telling Labour that the Tories are in fact terrified of Miliband and Burnham.
For flood victims, the State is not a dirty word. So why should it be for patients of the NHS?

Ironically, just as Ed Miliband gave his Hugo Young 2014 lecture on “an unresponsive State”, many people in the SW England saw their sandbags being delivered to a different location.
The floods have revealed what many of us have suspected all along.
The response to the floods has revealed a painful fault line in our narrative of ‘The State’.
There’s no COBRA meeting when fourteen Trusts run into difficulties with patient safety, because of the common thread that they don’t have a safe minimum level of safe staffing.
The acute general medical take for many health professionals is a ‘firefighting experience’, with the aspiration of lean management to mean there’s actually insufficient capacity in the system to cope with increased demand.
It is now being reported that some British insurers are unwilling to take on the risks of certain flood areas, feeling that the market is somehow rigged towards only benefitting “cherrypickers”.
It makes us wonder who the postman will be, now that Royal Mail is privatised benefitting hardworking hedgies.
And yet this is precisely the criticism that anti-privatisation campaigners on the NHS have been saying since initial discussions of the Health and Social Care Bill (2011) commenced.
The market is unable to guarantee complete coverage for all scenarios. In the case of private insurance and health, rarer ‘unprofitable’ diseases will just become out of scope. Like Owen Paterson’s ‘badgers’, the location of the goalposts will be redefined so that some NHS interventions are no longer ‘necessary’.
David Cameron’s response curiously has not been to resuscitate his flagship turkey.
You would have thought, if you believed any of Steve Hilton’s hype, that people would fight them in the dinghies as a “Big Society” response.
Or somehow the market could be “nudged” into action, where the market could be realigned with financial incentives to make us want to give a shit about our fellow man or woman now underwater.
Instead, David Cameron has been trying to fatten up the impoverished State.
If you think that the current debate about the actual fall in NHS spending is going nowhere, that’s clearly small change compared to what may or may not been happening to Lord Smith’s Environmental Agency.
For flood victims, the State is not a dirty word (save for those victims who feel profoundly let down by the lack of response by the State). So why should it be for NHS patients?
It’s well known that the current Government considered implementing an insurance-based system but eventually went against it. The implementation of personal budgets has been progressing over the few years, with rather little discussion.
And yet, personal budgets could become a major plank of Labour’s “whole person care”. Somewhat reminiscent of ‘expert commentators’ who were slow on the uptake when it came to uptake on competition in section 75, they appear equally sleepy on the significance of unified budgets for health and social care.
From one perspective, they ‘empower’ persons, and give them ‘choice’. But from another perspective, they actually disempower persons when the State runs out of money, and you have to top up your budgets from some other means.
It’s this two tier nature which causes the most alarm. Already, there’s been much finger pointing about ‘personal responsibility’ of people building homes knowingly on flood plains. The shift of potential blame as well as shift in personal responsibility is a deliberate change of emphasis in policy, and one which Labour must have an open discussion about if it wishes to retain any vestiges of trust.
The whole basis of trust of the public has for some time taken a knocking, with implementation of the private finance initiatives (PFI) and discussion of caredata.
While budget sheets are in the hock of paying off loan repayments, rather than paying for much needed staff to take the level of staffing beyond ‘skeleton’ or ‘extra lean’, the talk about a ‘more responsive State’ is all fluff.
While the NHS complaints system remains unfit for purpose, it’s all fluff.
It may be the fluff which keeps Alan Milburn and Tony Blair happy, but, despite the three general election victories, it has been a policy issue which Labour must revisit.
Proper levels of funding of the NHS and social care have long been popular and populist policies for Labour, and so has effective State planning.
It remains thus all the more strange that the only State that the Labour Party in fact cares about is the Square Mile.
David Prior is right, but his solution is wrong. Radical change is needed to abolish the NHS’ internal market.

In an article in the BMJ in 2011, entitled “How the secretary of state for health proposes to abolish the NHS in England” (BMJ 2011; 342 doi: http://dx.doi.org/10.1136/bmj.d1695 (Published 22 March 2011) by Allyson Pollock and David Price), the authors comment:
“The coalition government’s Health and Social Care Bill 2010-11 heralds the most controversial reform in the history of the NHS in England.The government plans to replace the NHS system of public funding and mainly public provision and public administration with a competitive market of corporate providers in which government finances but does not provide healthcare.”
On the other hand, a radical shift in the culture of the NHS is needed to rid it of outdated working practices, cure it of widespread bullying and heal the damaging rift between managers and clinicians, according to David Prior, chairman of the Care Quality Commission (CQC)
Prior has called for serious “transformational change” of the health service, without which it will “go bust”. That is not the radical change the NHS needs.
We need to abolish the internal market of the NHS.
The most significant piece of evidence that supports that view that market failure is the big problem in healthcare delivery is the widespread recognition that price competition actually worsens healthcare outcomes. Economic theory predicts that price competition is likely to lead to declining quality where (as in healthcare) quality is harder to observe than price. Evidence from price competition in the 1990s internal market and in cost constrained markets in the US confirms this, with falling prices and reduced quality, particularly in harder to observe measures.
The opposition to the Health and Social Care Act (2012) ended up being all over the place due to lack of any meaningful media coverage from the BBC and other media outlets, and a failure of supposedly intelligent people to cut through the crap and spin of what the Act was about. The Act was simply about putting in a competitive market, regulating the market, and finding a preliminary mechanism of winding up the ‘unfittest’ so that they couldn’t survive. The Act was nothing to do with patient safety. And we all know what an unmitigated costly fiasco this has been, and decisions have even be made on the basis of competition law rather than the health of the patient.
It’s been a shocking disaster.
The problems of market failure are already well recognised in the UK. Scotland and Wales have both abandoned the purchaser-provider split. In England, the problem of price competition is well recognised and most hospital tariffs/”prices” are fixed. Thatcher’s purchaser provider split (1989) has been well critiqued in the literature and the recent
A Health Select Committee (HSC) report, commissioned by the Department of Health from York University (Karen Bloor), on the current commissioning model was even more damning.
“If it does not begin to improve soon, after 20 years of costly failure, the purchaser-provider split may need to be abolished.”
The HSC report cited that the administrative costs of the purchaser-provider split to be as high as 14% of total NHS budget compared to 5% prior to the purchaser-provider split.
Other examples of where the market has failed the NHS include the use of the Private Finance Initiative (PFI). The NHS IT disaster is a classic case of market failure.
The Baroness Morgan affair has focused attention on the political nature of our unelected quangocrats are. For those unfamiliar with the story, she claims No 10 is “absolutely determined” to ensure that only Tory supporters are appointed to public bodies.
The idea of the free market being the best way of enabling individuals to plan their lives is nonsense. The free market system also generates huge inequalities between countries and regions. In the free market system, investment tends to go already where it is most profitable. Further, the free market system counts or recognises as important considerations only what can be packaged as commodities for individual consumption. The solution is not of course a bureaucratic manipulation of the economy and bureaucratic nationalisation like that being carried out by Bismarck in Germany. Socialist planning does not mean that we want to do away with free markets straight away. Many reasonable individuals recognise that free markets played a huge role in human development, and cannot be dispensed with overnight. Socialist planning is not primarily about faster economic growth. It is not even primarily about increasing control over the economy. It is primarily about decreasing the control of the economy over human lives. Some highly successful capitalist systems, such as Japan’s or South Korea’s, have had effective government planning of major investment. There is no reason to suppose that democratic planning would be less workable.
The importance of planning by the state, within its proper sphere, is unapologetically acknowledged. A free society needs a strong, confident state capable of carrying out on behalf of its citizens its vital role — including the planning required by that role — effectively and efficiently in a world of unpredictable challenges and threats. Under capitalism, there is always a drive for more profit, for this or that new profitable line of production, for increased pressure on the worker to work more. In fact capitalism does not even satisfy the wants which capitalism creates. Signals are sent through the market only by consumers with money, not by human wants or needs. The whim of the rich is satisfied; the desperate need of the poor is not. The real driving principle of capitalist economics is not consumer demand, but profit.
In Japan, they have the most tremendous technology, and they could produce the basics of life with a relatively small effort. It would be possible for people to have a relatively leisured and dignified life. Despite that, something like 70% of Japanese workers say that they constantly feel physically exhausted and mentally exhausted. Socialist planning is not about state planning of people’s whole lives. And even in the area of basic production, we will not be able to plan social needs straightaway. It will take generations before the level of technology, the degree of information and culture, and the spirit of co-operation have developed enough to make the planning of basic economic essentials just an administrative question. Subsidiarity requires that state planning should be restricted to tasks in relation to which individuals and groups cannot plan for themselves, and which cannot be handled by organisations independent of the state and operating in markets, preferably real markets.
It is a highly significant problem that the great majority of the people, toil only to enrich the top 10 per cent, who in Britain own 53 per cent of all marketable wealth and almost all land and shares. Everyone could have a decent job, and the excess of what the workers produce over their own direct consumption would go to social provision and to socially-controlled investment. We could get rid of the vast waste and duplication arising from capitalist competition. A living wage could go a long way to ensuring people are paid a fair amount for their work, giving employees dignity and security
As Alex Andreou wrote earlier this year,
“The richest 85 people in the world have as much wealth as the poorest 3.5 billion – or half the world’s entire population – put together. This is the stark headline of a report from Oxfam ahead of the World Economic Forum at Davos. Is there a reason why the world’s powerful, gathering at the exclusive resort to sip cognac and eat blinis, should care? Well, yes.
If one subscribes to the charitable view that neoliberal philosophy was simply naive or misguided in thinking that “trickle down” would work infinitely, then evidence that it doesn’t, should be cause for concern. It is a fundamental building block of supply-side economic theory – the tool of choice these past few decades for those in charge to make adjustments. The realisation that governments have been pulling at economic levers which, for some time, have been attached to nothing, should be a wake-up call to the deepest sleepers.”
In the absence of free markets, it is said that prices go up or fail to reduce. The way in which companies can collude with each other in delivering excessive profit and poor value-for-money for the consumer is well known in privatised industries. Books have been written on the subject. There are legitimate questions as to the effectiveness of the EU, but hats off to its commission for exposing the scandal of big oil companies allegedly colluding to rig petrol prices for a decade. Prices have risen 80 per cent, from 75p per litre in 2002 to around £1.40 per litre now.
It is also argued that innovation is blocked through collaboration. This is unmitigated rubbish, as collaboration has been well described as a driver for innovation even in the private sector.
“One of the top priorities of the group is to offer consumers innovative products. The ability of its suppliers to propose new solutions and technology and to develop innovative products and services in partnership with the L’Oréal teams makes a direct contribution to the success of new products. This collaborative process is based on trust in an ever more competitive economic climate. L’Oréal establishes an open dialog that stimulates and accelerates innovation for the benefit of consumers.”
Real capitalist markets do not correspond with the “ideal” of efficient, reliable balancing of supply and demand. At almost all times outside wars, capitalist economies generate vast armies of the marginally employed, people defined by the system as “excess supply” of labour-power. Successful service reconfigurations, such as stroke reorganisation in London, involve complex planning and engagement. Market forces cannot be the right way to drive socially responsible and clinically sustainable, equitably distributed and politically palatable service configurations and integration.
David Prior is right. But he’s like a Doctor who’s produced a correct diagnosis of a heart murmur and advised totally the wrong management plan like total bowel resection. The question now is whether a move towards a “NHS preferred provider” is an incremental step, but not sufficiently radical, to abolish the market. The ultimate way to reconcile this would be to have private providers providing NHS and other care services not on a transactional basis, but the choice, as they say, is theirs.
The NHS – the cash cow that keeps on giving

It’s perfectly possible to run a public service into the ground. Then say it’s shit. Then privatise it. Look at British Rail.
The NHS represents the ultimate golden goose. It is pictured as a drain of resources, while year after year it runs at super efficiency supposed to deliver cumulatively £20bn ‘efficiency savings’? And where does this money go? Answers on a postcard. It’s all a big scam, as the Government then consults on what could deliver better care: and after a few Cs, the answer is compassion. What a surprise.
If we had the same level of revolts as in Greece and Spain at this drive in the name of ‘austerity’, ‘sustainability’, or ‘doing more for less’, or any other trite saying which springs to mind, the number of people of arrested could in theory fill private prisons many times over. It doesn’t matter if some of these are ‘false arrests’, as an outsourcing company could run the appeals process for another arm of the outsourced criminal justice system. The State of course doesn’t have to pay for it having torpedoed legal aid. Look at what the criminal barristers are up to.
Guilty when you’re innocent is the legal equivalent of the ‘false positive’. It’s perfectly possible to rustle up false positives in many areas of medicine. Take for example finding the odd demyelinating plaque on a neuroimaging scan, which could then be further investigated by a lumbar puncture, to rule out multiple sclerosis. Or take for example a twang of musculoskeletal pain which gets combined with a borderline blood test result so that an individual ends up having a catheter inserted up his groin to have a look at the arteries in the heart.
The possibilities are endless. This is what goes wrong when you open up the wrong markets. There are many who disagree with the market ethos, and expect Labour to go through the motions of opposing the market. The question though can be asked what exactly it has been done to oppose the TTIP (EU-US Free Trade Treaty), when MPs have been extolling its virtues in other sectors. And does the Labour Party wish to chuck out those MPs or Lords who clearly have been alleged to have conflicts of interest affecting how they vote on matters of competition or procurement law?
Public anger at a cash-starved NHS might get Labour into government, but what happens when Labour comes into government? Certain things, such as the TTIP or European procurement directives) might suddenly come beyond the control of Labour. The ‘efficiency savings’ are set to continue. Will they do anything about the ‘efficiency savings’? Ed Balls yesterday boasted of ‘the Fabian way’, but the description he gave was very free-market with the NHS or socialism barely mentioned. It’s a moot point whether this is of course the ‘Fabian Way’, but the logo of the Fabians used to be a ‘wolf in sheep’s clothing’.
What would a unified budget mean for a combined NHS and social care service? Quite simply, it could become the second reincarnation of ‘The Big Society’. This concept was widely criticised as being a cover for cuts, but a means of legitimately ‘shrinking the state’. The two concepts have thus far not been explained well, although it’s still early days for ‘whole person care’. Merging the budgets could make it much easier to hide further under-resourcing of services. It is potentially a neoliberal shoo-horn, but in the maelstrom of the Labour Party acting as the caped crusader, nobody might notice.
And of course if work pays, private business pays even better. There’s still money to be made from people trapped in the system, if they are incorrectly charged with an offence or wrong diagnosed with a medical condition. If the Government wishes concomitantly to up the number of diagnoses in conditions, you could see the perfect storm, as in the national dementia policy. Things are normally charged on the basis of what it costs plus a bit of a profit, and of course the directors of private companies are obliged to return a porky shareholder dividend.
Yep, it’s the cash cow which keeps on giving. Who knows what Simon Stevens, ex head of a multinational, will make of it as head of the NHS this year.
Size isn’t everything…. except in Labour’s competition policy
 There are a few squares to circle when it comes to how Labour negotiates the future direction of health policy for the National Policy Forum later this year.
There are a few squares to circle when it comes to how Labour negotiates the future direction of health policy for the National Policy Forum later this year.
One of them will have to be Labour’s future direction on “competition”. The basic knub of it is that people or entities which are competing will end up performing better, however that this is measured, to the benefit of the end user (called ‘customer’ traditionally in business or ‘person’ or ‘patient’ in healthcare.)
Ideologically, competition is associated with the neoliberal approach, where market forces will ultimately equilibrate to the benefit of the population. This has been likened to a Darwinian ‘survival of the fitness’.
However, the analogy is not entirely useless. In such a construct, it is perfectly possible that certain living beings become extinct. There may be no love lost over an ancient reptile no longer contributing its DNA to the animal race, but there could be a problem if a NHS unit for a very rare disease becomes financially unviable and goes extinct.
So Labour does have a slight problem on its hands. People disagree on the extent to which the section 75 Health and Social Care Act, which secured competitive tendering as the default option for commissioning NHS contracts (mainly to the private sector), was a a natural extension of the market philosophy which had occurred under the competition and co-operation facility of Labour.
People generally agree that the original arguments about quality and competition in the NHS were extremely badly argued with hindsight, in promoting “the market”. On the whole, members of the general public agree that there might be a rôle for competition in driving up standards in cleanliness of surgeries, such that you might prefer to be a patient of a particular surgery, while trusting a Doctor to be driven by professional standards not by profit.
The idea of the NHS logo becoming a kitemark for private providers long pre-existed this Government, and was alive and well under the previous Labour government. On the other hand, Andy Burnham MP has emphatically pledged that Labour will roll back the market when it comes into government in May 2015.
The repeal of the Health and Social Care Act (2012) is a big thumbs down to its three main planks of policy. One is definitely ‘unfinished business’, as anyone following the arrangements for Trust Special Administrators will see in the insolvency regimes. The other two are intrinsically the full entrenchment of the market through section 75, and its regulation through enhanced powers for an economic regulator called Monitor.
So can it be that Labour per se objects to competition? Historically, this cannot be the case.
Labour wishes to promote collaboration, which is in keeping with socialistic principles of solidarity and co-operation. However, two major areas of criticism emerge from many stakeholders over competition especially from the Unions, who represent many hardworking Doctors and nurses inter alia.
Firstly, the focus of the attack seems to be on corporates rather than SMEs or social enterprises. Indeed, markets tend to break down when large corporates collude in legal price behaviour meaning the end user does not benefit. This has contributed to a ‘cost of living crisis’ in energy and rail fares.
The market especially breaks down when specific corporates or charities collude with the State, producing a near monopolistic effect. This historically has been more likely the greater their size. This effect can be particularly detrimental when this impacts on policy, some of which is best left to non-market forces like subject experts or professionals.
The fundamental problem, if you apply Prof Michael Porter’s influential theory of competition from Harvard, is that smaller sized companies experience formidable barriers to entering the market. For example, they cannot compete on the basis of marketing spend or resources for investment. All too easily they can go out of business – hence the complete banality of claiming to have ‘an equal playing field’. A titchy SEO simply cannot compete with a large multi-national corporate especially if that corporate is already skilled at doing slick commercial pitches.
This is significant in considering the overall shape of how Labour policy is shaping up for 2015. It’s not a general attack on business that Ed Miliband has in mind, but an attack on those large corporates who are abusing their power.
Secondly, large companies under law have a duty for their directors to promote profitability with due regard to their environment, but profitability is generally considered to be dominant by legal experts in this jurisdiction. Social enterprises form an umbrella of different entities, which do not necessarily have to have this duty (for example in talking about a surplus not profit).
There can of course be bad charities or bad other entities in the third sector, just as there can be bad private or public limited companies. Part of the challenge for Labour is to think about how it can reconcile the views of Andy Burnham, who wishes to roll back the market, and Alan Milburn who sees competition as a means of promoting progress. It is crucial to remember that Alan Milburn is not a member of the Shadow Health team: that team is led by Andy Burnham MP.
Hedge funds or private equity will nor necessarily wish to confine their investments to large corporates anyway. Smaller companies may be more nimble and more likely to produce a return on investment, and, should Labour wish to find a place for such activity in the NHS somewhere, Burnham and Milburn might see a way in which their profits can be ploughed back into the general health economy of the NHS. Whilst the NHS has been demonised by lazy journalists and politicians as being ‘monolithic’, with the same old canards put to out to trot (or whatever the phrase is), the NHS can in business management terms benefit from its economies of scale, making it more competitive.
So it might be that Alan Milburn and Andy Burnham are able to define the parameters in which there is a place for competition in the NHS. It could be that many large corporates do not wish to collude in an oligopolistic way at all, and act responsibly in the NHS.
However, Andy Burnham, in promoting his “NHS preferred provider” can provide a way in which social enterprises can legitimately contribute to competition, and even have some input from the multinational corporates in contracts under “the prime contractor model.” This of course can be done within the parameters of maintaining a NHS which is comprehensive, free at the point of need, in as much as some rationing has been taking place, but to avoid a rampant market with powerful private providers cherrypicking profitable work.
But the point is that the positions of Milburn and Burnham are not complete polar opposites. Whilst loyalties to the two individuals can be quite fierce, they both occupy a very senior of level of influence in the Labour Party, and will have a massive say on the future direction of the English NHS. But it is yet again significant to remember that Alan Milburn is not a member of the Shadow Health team: that team is led by Andy Burnham MP.
The NHS and markets – the drugs don’t work

This week, David Cameron MP mocked Ed Miliband MP for sounding like a person who’d rung up a radio show whingeing.
Cameron replied, “And your problem is caller?”
The problem is a complete collapse of ideological position which has lasted decades.
Ed Miliband keeps up the moment today with the market failure of the energy oligopoly (see article by Patrick Wintour in the Guardian.)
It is argued that one of the precursors of Thatcherism was a revival of interest in Britain and worldwide in the work of the Austrian economist and political philosopher, Friedrich Hayek, who won the Nobel Prize for economics in 1974.
Alongside Milton Friedman, who won his Nobel Prize in 1976, Hayek lent great prestige to the cause of economic liberalism, helping to create the sense of a rightward shift in the intellectual climate, complementing the approach of Ronald Reagan across the pond.
These principles of dogma have seen successive Conservative and Labour governments reaching for the drug of privatisation and outsourcing.
But these drugs are not only failing to work. They are having devestating side effects which are killing the patient.
The markets have been outed for being far from liberalising. They create inequality. It is alleged that the austerity-based policies have led to a marked decline in mental health and rates of suicide even.
But it’s not the shocking Gas bill which has delivered the knock-out blow for the Conservatives’ religion.
“Here is the reality. This is not a minor policy adjustment—it is an intellectual collapse of the Government’s position.”
This was Ed Miliband’s verdict in Wednesday’s Prime Minister’s Questions.
Only a day previously, BBC Radio 4’s had played a voxpop of various members of the public speaking about ‘payday loans’ as a prelude to interviewing George Osborne MP.
“I don’t accept it’s a departure from any philosophy. The philosophy is we want markets to for people. People who believe in the markets like myself want the market regulated. The next logical step is to cap the cost of credit. It’s working in other countries. In fixing the banks, we need to fix all parts of the banks and the banking system. It helps all hard-working people.”
During the time of the previous Labour government, the King’s Fund was head-over-heels promoting competition.
It was known that, by shoehorning competition as a policy, private providers would make a killing.
All you had to do was to bring in a £3bn ‘top down reorganisation’, a 500 page Act of parliament containing no clause on patient safety apart from the abolition of the National Patient Safety Agency, and beef up a new consumer regulator (“Monitor”).
But meanwhile back to payday lending, an evidenced case of market failure.
“We’ve always believed in properly regulated free markets, where there’s competition, but where the market is properly regulated. That’s why we created a new consumer regulator.”
Far from being a loveable buffoon Boris Johnson, Johnson has revealed himself to be the toxic political mess he is.
Suzanne Moore, at the risk of being hyperbolic, called out Johnson as ‘sinister’.
Johnson had launched this week a bold bid to claim the mantle of Margaret Thatcher by declaring that inequality is essential to fostering “the spirit of envy” and hailed greed as a “valuable spur to economic activity”.
In an attempt to shore up his support on the Tory right, as he positions himself as the natural successor to David Cameron, the London mayor called for the “Gordon Gekkos of London” to display their greed to promote economic growth.
He qualified his unabashed admiration for the “hedge fund kings” by saying they should do more to help poorer people who have suffered a real fall in income in recent years.
And what’s wrong with greed being good if this improves patient care in the NHS?
The issue always remains ‘zero sum gain’. It’s a problem as it diverts tax-funded resources directly in the coffers of the private sector.
Arguably, it’s not just the failure of the market which is the problem, but ‘the undeserving rich’ who have never ‘seen it so good’ since Tony Blair’s New Labour period of government.
In August 2009, the then leader of the Opposition and Conservative leader, David Cameron, MP defended a shadow health minister for advising a firm which offers customers an alternative to NHS doctors.
Lord McColl was on the advisory board of Endeavour Health, which promised a quick and convenient access to a network of “top” private GPs.
It was claimed then that Endeavour Health is a company set up by two hedge fund advisers which purported to be Britain’s first comprehensive private GP network.
In a video yet to be deleted off You Tube, David Cameron argued that there was nothing ‘improper’.
This was interpreted at the time that the Conservatives “favoured private alternatives”.
Nonetheless, David Cameron claimed that the Conservatives was ‘totally dedicated to the NHS’, but he wished ‘to expand the NHS so that people don’t have to use the private sector’.
What actually happened was the Health and Social Care Act (2012).
In July 2013 in the British Medical Journal, it was reported that the private sector is in line to secure hundreds of millions in NHS funding from services placed out to the open market under the UK government’s latest competition regulations, a study has shown.
Research by the pressure group the NHS Support Federation found that contracts for around 100 NHS clinical services totalling almost £1.5bn (€1.7bn; $2.2bn) have been advertised since 1 April 2013, with commercial companies winning the lion’s share of those awarded to date.
Data from official tenders websites showed that only two of 16 contracts awarded since the government’s section 75 regulations of the Health and Social Care Act came into force have gone to NHS providers, with the remaining 14 going to the private sector.
A few days ago, it was reported tonight that David Cameron is intending to ban branded cigarette cartons, having originally decided last July not to proceed with the plans.
In the summer the Government said it was waiting to see how plain packaging worked in Australia, which introduced the measures a year ago, before making any changes. It has since maintained it is monitoring the situation.
That is the spin. Behind the scenes, it is well known that tobacco corporates have throttled public health policy.
In the third volume of Law, Legislation and Liberty, Hayek argued that there are not two but three kinds of human values: those that are “genetically ordered and therefore innate”; those that are “products of rational thought”; and values that had triumphed in the course of cultural evolution by demonstrating their suitability to the successful organization of social life.
Hayek believed that these values were a cultural inheritance, survivors of a competitive struggle, and essential conditions for the successful evolution of our society.
David Cameron is indeed right to be worried.
There has been a collapse of the ideological position that he and his predecessors, Margaret Thatcher and Tony Blair, stood for.
This is in relation to the markets.
This fundamentally changes the terms of reference for a market-based NHS.
Contagion is likely politically.
If payday lending or the energy markets are anything to go by, there could be trouble ahead.
So what’s the issue? The caller’s problem is that “the markets don’t work”, “they only make you feel worse again”.
And now the caller’s finally worried about the NHS.
Many people were warning about competition in the NHS long before Polly Toynbee. Me for example.

Many people were warning about competition in the NHS long before Polly Toynbee this morning.
Me for example.
There are very few people who registered this issue as such a big issue while devoting reams and reams to talking about English health policy.
Dr Tomlinson’s blogpost is a MASSIVE exception – from 2011.
Here it is.
Later than Dr Tomlinson, at the turn of the year, I too wrote a blogpost about how a little appreciated clause in the Health and Social Care Act (2012) would lock the NHS into a competitive market based on price competitive tendering. I cannot claim credit for how this nightmare had entered my head.
The academic who alerted me to how this clause works is Dr Lucy Reynolds. She explained to me why the clause was so significant in making the NHS run on the basis of competitive tendering in the market, and asked me to look out for the Regulations which subsequently appeared.
Lucy doesn’t know I’m writing this, but she was right. A few in the Socialist Health Association publicly queried what the fuss was about, as the policy appeared at first blush to go no further than the competition and cooperation policy of the last Labour government. But all the ‘scare stories’ came to fruition, and nobody had the dignity to admit it.
I remember I was much derided myself about the blogpost from ‘experts’ in public health. They lunged at me asking me to defend the article, some in a rather unpleasant way.
Prof Allyson Pollock had gone out of her way to explain brilliantly why the competition healthcare experts were barking up the wrong tree years ago.
Less than a year on, I have blogged on the passage of the regulations through the legislature, and even why competition was always a flawed policy plank for the NHS.
I have even blogged on things which haven’t even happened, on how a more useful approach might be to embrace “co-epetition“. I have warned about how bundling in integration may even offend competition law, and how the “prime contractor model” continues to pose problems for legal liability.
And yet I continue to be derided for my input there. My crime is that I do not shill for the Conservative party or any right-wing ideology. I do not present at think tanks, like Kaiser Permanente have done most recently. I’ll let you do your own enquiries where.
It came as a genuine surprise to me that David Nicholson was blaming competition lawyers. To make this claim, you either do so innocently, negligently or fraudulently.
But I will give him the benefit of the doubt. Presumption of innocence is very important in the law.
This policy has cost the NHS a lot of waste. The cost of the implementation of the Health and Social Care Act has been estimated at £3bn thus far. But the consequences of implementing this competitive market are more dire.
About a decade ago, Prof Carol Propper wrote papers on the importance of the market and how it could be regulated. We know have this costly reorganisation and Monitor. But Propper was not the only one.
Journalists, politicians and NHS leaders have all been complicit in turning this agenda into a living dream. Baroness Williams with the help of Liberal Democrat competition lawyer colleagues were able to argue the case for competition law replacing what had gone before.
It’s either me or them?
Thanks to people like Dr Jonathon Tomlinson, Dr Marie-Louise Irvine, Dr Charles West, Dr David Wrigley, Val Hudson, Caroline Molloy, Prof Clare Gerada, Dr Kailash Chand, Dr Jacky Davis, Clive Peedell, Sian Rabi-Laleh, John Hully, Prof Ray Tallis, Prof Allyson Pollock, David Skidmore, and Prof Colin Leys, I came to realise it’s not, in fact, me.
I cannot even begin to explain what a waste of time I feel my efforts have been. But I will soldier on regardless with blogging for this Association which is proud to promote a policy based on universality, free at the point-of-need.
It’s not just the structural disorganisation which has to be reversed. Parts of NHS culture must change too.

The political problem for David Cameron is that all of the current problems of the National Health Service can be blamed on this current Government ‘diverting’ around £2.4 bn resources into implementing a complicated disorganisation.
Lansley, a co-author of ‘Equity and excellence: liberalising the NHS’, the key White Paper of 2010, has always argued that this was never a ‘top down reorganisation’. It was a ‘devolving reorganisation’, according to him re-distributing power to clinical commissioning groups inter alia.
If the Thatcher and Major decades could be characterised as implementing a sort of ‘market’, with purchasers and providers, the Blair (and less so Brown) years might be characterised as a restructuring period for the NHS. This is after all where the PCTs were originally created.
One of the biggest criticisms of how the NHS was run in the latter period of the last Labour government is that CEOs sought to ‘game’ markets so that NHS Trusts could without any difficulty obtain ‘foundation trust status’. Some Trusts for budgetary reasons employed unsafe staffing. With a weak regulator at the time, with culpable CEOs simply moving onto different jobs, the rest of NHS (and some relatives tragically) have been left to pick up the pieces.
Andy Burnham MP is thought to be fairly safe in his Shadow Secretary of State job until 2015 at least. Whether he can remain spend a helpful period of time as a Labour Secretary of State in health, implementing ‘whole person care’, is quite a different matter.
Burnham has categorically pledged to repeal the Health and Social Care Act (2012). He has pledged to reverse part 3 – the section on competition. He insists that he ‘will ask to the same structures to do different things’. This approach is to avoid the accusation that Labour will embark on yet another costly disorganisation, knowing that the public know there have been quite aggressive cuts in nursing staff numbers already.
This might seem fine – but it will not address any latent pathology in culture in the NHS. Unless Labour attempts to consider this build up of pathology, which has taken decades across both Labour and the Conservatives, it is possible that it could become really malignant again. At worst it could kill the NHS.
Evidence that the pathology is relapsing is, for example, given by the recent ongoing debacle at Colchester.
Ecosystems do change however.
Look at Death Valley.
The wettest year on record in 2004/5 transformed the forbidding wilderness of scruffy mountains and scorched earth into a vividly unfamiliar world of wildflowers and reflecting pools, triggering ecological cycles not seen before on so large a scale.
The intense heat was swapped for an environment which living things could flourish.
Against a background of snowcapped peaks, the region’s lands suddenly became populated by bright yellow, pink, white and deep purple blossoms spreading out in all directions.
And why did markets cause so much a problem?
We turned from a market economy to a market society.
Why is this a problem? According to Sandel, two reasons: First, inequality. As money becomes important to access to the essentials of the good life — such as decent healthcare — inequality becomes more and more important.
And the second reason is that when market thinking and values enter the sphere of certain social goods and practices, they change the meaning of those practices — and crowd out attitudes and norms worth caring about.
Sandel gives the example of cash incentives in schools.
Some schools in New York, Chicago and Washington DC have begun programs to motivate students from disadvantaged backgrounds by offering money for grades: $50 for an A, $35 for a B, and so on. A program in Dallas offers students $2 for every book they read.
What was observed at the end of the experiment was that all was more was offered for students reading books, students did indeed read more books with greater financial motivation. But they also read shorter books.
What this illustrates is a false assumption held by many economists, says Sandel: that markets are inert and don’t taint the goods they exchange. This, Sandel argues, may very well be true with material goods, but not so with medical services, engaging in civic life. According to his thesis, market thinking can actually change the “character” of these social practices, so we have to really think about where markets belong and where they don’t.
Look at how GP practices are paid to collect some data under QOF – the use of some of this data is not at all clear.
The National Health Service is in an intrinsically human phenomenon. It is not adequately encapsulated by a series of equations concerning industrial productivity.
Margaret Heffernan gives another striking example.
Gayla Benefield uncovered an awful secret about her hometown that meant its mortality rate was 80 times higher than anywhere else in the U.S. But when she tried to tell people about it, she learned an even more shocking truth: people didn’t want to know.
It turned out the hometown was full of a substance called asbestos, causing individuals to breathe in asbestos and develop fatal lung disease.
In the best organisations, those charged with leading the organisation welcome challenge because it helps the organisation to learn.
But the recent history of the NHS is littered with the casualties of the fear of acknowledging error, especially where such errors might be the tip of a very large iceberg, in an organisation that is more systematically flawed.
Kim Holt, Gary Walker, David Drew, and Steve Bolsin – the list of those who have had the courage to blow the whistle is a long and honourable one.
But people who have tried to speak out have invariably suffered in some form themselves.
The NHS will be doing its ‘change day’ soon in 2014. Part of a way with dealing with a problem, whether it is an assumption of market values not to the benefit of the patient, or a lack of a safe environment to ‘speaking out safely’, is admitting the problem exists.
Only then can you unfreeze yourself from this ‘frozen culture’, shift culture, and move to a new cultural destination.
Whatever is legislated about structures, this change must happen in the next government. It will also be essential for the safe implementation of ‘whole person care’, or similar.
