Home » 2014 (Page 3)
Yearly Archives: 2014

The general public have never needed the NHS campaigners as much before. The situation is critical.

“The past is a different country. They did things differently there.’
One of the favourite weapons in the armoury of supporters of the present Coalition is that the warning claims over the NHS have been in the past ‘exaggerated’ or ‘scaremongering’.
And yet today broke records being broken, for the longest waits in the Accident and Emergency departments in England; and a record number of emergency admissions.
The National Health Service currently has a statutory duty to promote innovation. But nobody would have thought that Mr. Hunt (who is not a professional surgeon, or professional medic, to my knowledge) would have ‘done things differently'; by adding a ‘Spring Crisis’, ‘Summer Crisis’ and ‘Autumn Crisis’ to a ‘Winter Crisis’.
Put simply, sadly the claims by NHS supporters do not constitute merely ‘scaremongering’. It may have been urgent to ‘save the NHS’ in the past; as indeed Labour had to do in 2007 when the service was teetering on the brink last time. But the situation is now critical.
The last few years have seen a litany of errors in public health policy; such as in standard packaging of cigarettes, or minimum pricing of alcohol. It has been impossible for the Conservatives and the Liberal Democrats, who are both devoted to the multinational free movement of capital, to act in the true public interest.
But by far the worst event to have happened were the Conservatives and Liberal Democrats getting onto the state books the ‘Health and Social Care Act’.
The Liberal Democrats’ contribution to this statutory instrument cannot be underestimated by any means. Despite the noblest actions of a minority of ‘good LibDems’, such as Dr Charles West, the cheap words of some LibDems Peers in the debate over the toxic ‘section 75′ made their position perfectly clear.
Section 75 of ‘the Lansley Act’, which senior Conservatives now claim not to have understood, couldn’t have been clearer. It was a clear departure from the previous law. It laid out a clear threat in law for the first time a legal threat to any commissioners departing from putting contracts out to formal competitive tender, if there were not a sole bidder.
The Liberal Democrats, Conservatives and UKIP may now show what can best be described as ‘amnesia’ over this instrument which some of them actually legislated for, as well as the £3bn ‘top down reorganisation’ which David Cameron swore blind would never be introduced, but “the facts speak for themselves”: or, as my learned legal colleagues, put it, ‘res ipsa loquitur’.
Andy Burnham MP this morning in an article in the New Statesman laid bare the sheath of lies by Nick Clegg in the House of Parliaments over the NHS.
Sadly, while Jeremy Hunt and Dan Poulton fiddle while the NHS collapses, there is a record number of admissions in emergency departments in England, and the most vulnerable people are labelled ‘bed blockers’ by a supine and ineffective English media as they cannot leave hospital to a social care system which has now collapsed through starvation.
Labour argues that it last used the private sector in needing to address a ‘backlog’ in demand, but the question is how the NHS get to this state in the first place? It’s because for decades, as NHS campaigners rightly argue, the NHS and social care systems have been given the bare minimum to carry out their functions.
NHS managers, many of whom are generously paid more than their ability might suggest, and certainly much more than frontline nurses implementing a policy savaged by staffing cuts in the name of ‘efficiency savings’, have been trying to balance the books through a number of mechanisms, such as laying off staff, not giving existent staff a pay rise, or paying corporates loan repayments for PFI or lawyers for doing their administration.
Labour possibly can argue then it was a temporary measure to pay off people in the private sector to do the work the NHS had been carrying out, but the mainstream parties should be in the business of delivering a well functioning NHS. As Andy Burnham MP said in launching his party’s campaign on the NHS in the European Election in 2014, we’ve got a sad state when the Conservatives and LibDems are competing for the lowest social care bills irrespective of whether the services are awful.
And it’s sacracant to criticise the NHS managers, but any reasonable guardian of these managers will ask why they have allowed their own senior pay to balloon;
why performance management of Doctors and nurses in the NHS is so poor, with performance management being regularly done by the regulator not by human resources;
why so much money has been siphoned off for ‘transaction costs’ of law and admin the implement the NHS reforms;
why PFI contracts have been so poorly negotiated such that the cost to the State is enormous;
how come so many private providers are being directly paid out of the NHS monies provided by taxpayers;
why there seems to be an enthusiasm to pay short-term locum staff at exorbitant rates instead of investment in the current workforce;
and so on?
The Health and Social Care Act (2012) drove the NHS over the edge. Put simply, the NHS and social care systems would not be able to survive another sudden legislative mechanism designed to privatise the NHS?
On this Camilla Cavendish is simply incorrect. You would have thought with all her experience she should have come up with a better definition of ‘privatisation’ on BBC Question Time last night. it is the standard argument of those who say it is not privatisation to say that privatisation is accompanied by a ‘tell Sid’ type flotation (also called the “initial public offering’).
It is not.
Privatisation is simply wholesale transfer of assets and resources from the public sector to the private sector.
There has been every possible last-ditch effort to deny this was NHS privatisation from the current neoliberal Coalition parties. It is definitely privatisation. The taxpayer is paying private companies for functions which the State should be providing, without private companies footing properly their part of the ‘bill’ including for training of the current workforce of professionals.
The ratcheting up of how ‘it is not privatisation’ or ‘we should look at whether private provision is a bad thing’ is a testament to this.
Quite simply, the NHS would not survive another five years of the Conservatives. We should rally around NHS campaigners of all parties to ensure the Conservatives and Liberal Democrats are not re-elected nationally to run the NHS for their benefit.
The National Health Service is not supposed to be run for the benefit of private sector ‘rent seekers’, or MPs who also have interests in the private health industry. Keep our NHS public. Keep the NHS National run for the public good.
Support your NHS campaigner. He or she needs you.

Dementia Friendly Employers
HRM TV: Ita Buttrose on dementia at work from AHRI on Vimeo.
Writing my book ‘Living better with dementia: champions for enhanced dementia friendly communities’ has been a real eye opener for me.
I think it’s terribly easy to carp from the sidelines about the ‘dementia friendly communities’ policy as implemented in England, but England is in fact helping to lead the way with this policy. ‘Dementia friendly communities’ is a policy which has a strong global backing, with links to the World Health Organisation’s “Age friendly cities”.
The WHO “Age Friendly Cities” recognised that there are basic design features of an urban city, wherever in the world, which might make living in it much easier; such as ‘inclusive design’ which is accessible to people.
Dementia is not just about ageing, so it is a challenge to think about what a dementia friendly ‘community’ might be. It’s important for this to be a ‘community’ not just a city, as it is recognised that around the world there are remote or rural areas where people who’ve been diagnosed need to feel welcomed.
When I went up to the Alzheimer’s Europe conference in Glasgow earlier this year, I had the good luck to meet Ann Pascoe in the hôtel where we weree having her fringe events. She has been doing groundbreaking work on rural dementia friendly communities in Scotland. I subsequently met one of team doing great work on dementia friendly rural communities in Wiltshire at the Dementia Action Alliance meeting the other day.
I met Toby Williamson from the Mental Health Foundation too at Glasgow, as well as Grainne McKettrick who first started her work on equality and equity at the Alzheimer’s Society in Scotland. I am delighted that Grainne has allowed me to quote from her speech in my one of my book chapters for the book I am submitting.
That chapter is on reconciling a rights-based approach promoting dignity and autonomy, with other mechanisms to promote ‘choice’, in a more consumerist way, through ‘personal budgets’ or ‘self directed support’.
Grainne remarked in her email to me yesterday how she had been really impressed with how fast the policy stream for this has taken pace in the last few years.
I think this is indeed worth noting for England. In the last fee years, we have seen a number of aspects suddenly converge at once, which have made a really big impact: these include the recognition of the UK government of the UN Convention on rights for disabled citizens (a few years ago), the Equality Act (2010), “dementia friendly communities” and the Prime Minister’s Dementia Challenge.
A welcome move will be there will be some sort of ‘standard setting’ for dementia friendly communities. It is far too easy for some communities to claim that they are ‘dementia friendly communities’, for their own promotion, rather than meeting an accepted reasonable level of requirements.
I think it’s great that people living with dementia can expect now a better level of service in the high street, say from a high street bank. But it’s important that this policy doesn’t raise inappropriate expectations.
But it is also true that this policy should raise expectations on employers dealing with people of a certain age, say in their early 50s, who might be developing a dementia in the younger age group, such as diffuse levy Body disease, vascular dementia or Alzheimer’s disease.
It’s a legal obligation for employers to make ‘reasonable adjustments’ against anyone with a ‘protected characteristic'; and dementia is one such characteristic, coming under the disability umbrella.
So why are there not many test cases for unfair dismissal for people who are sacked ultimately because of developing dementia? I have given this some considerable thought in the last few months since meeting Toby Williamson, and I reckon the answer is predominantly two fold.
Firstly, I don’t think it’s thought to be certain that the problems faced by an employee is due to a dementia at the time of ‘sacking’ with an element of mutual collusion that neither party is hoping for the likelihood of such a diagnosis. There are also intrinsic problems in England in areas of the country for achieving the diagnosis in a prompt manner. Prof Sube Banerjee warned recently how policy should not promote ‘high quantity, low quality’ of dementia diagnoses, on the other hand.
Secondly, I don’t think people are also aware of their legal rights under discrimination law, and, even so, don’t wish to take their employer to court for fear of losing any retirement packages or loss of goodwill, or inherent problems in access to justice. In England, under the current government, the legal aid budget has been slashed due to the Legal Aid and Sentencing and Punishment of Offenders Act (2012).
And another reason is that whilst we may have been promoting dementia friendly communities encouraging companies to cater for their customers living with dementia we haven’t been so keen to push ‘dementia friendliness’, a responsibility (rather obligation) of the employer.
There is, though, encouraging progress being made in other jurisdictions. I think we could no worse than to take a leaf out of the consumer action group of the Alzheimer’s Australia set up in England in pursuing this policy further.

George Osborne’s “duty of candour”

I’m pretty certain that George Osborne is actually quite a nice guy.
I know of people who know people who’ve had dealings with him on a chat-chat level. And apparently he’s perfectly harmless.
George Osborne’s one job was to run the UK economy. And he’s failed at that.
The LibDems had a job to deliver to deliver ‘a strong economy and fair society’. Add in the murder of English legal aid, we can confidently say the LibDems failed on their side of the bargain.
It doesn’t matter which particular metric you wish to use. The only good soundbites came from the rose garden soundbites from the Office for Budget Responsibility in 2010 informing us of the shiny uplands.
But it turns out that the incline of the uplands was steeper than we first thought. Osborne kept on telling us this was due to the Eurozone crisis. This is the same Eurozone crisis which has suddenly disappeared with one us being one of the ‘best performing economies’ in the G20.
Osborne’s pitch is that he needs just a little more time, as the famous Reet Petite song goes. He needs to ‘finish the job’ to put the UK back ‘on the path to prosperity’. This is the “long term economic plan”.
Except… the long term economic plan is not working. A record number apparently in employment with really bad income from as receipts? How did that happen?
Was it something, perhaps, to do with a record number on low security “zero hour contracts”, topped up with tax credits, who do not end up paying much income to the State?
The Conservative (Ronald Reagan) doctrine of a small state is creepy. The drastic diet of an ‘over bloated’ State has left a State which is anorexic – and which is dangerously fragile.
The Coalition’s anorexic state is consequently far from resilient. Most reasonable people agree that the anorexic State would simply be unable to cope with the Conservatives’ further planned cuts in the next term of office.
This is not the “shock doctrine” of Greece. It is a reality of something happening in the UK not seen since the 1930s.
The current Government has successfully relaunched the ‘duty of candour’. The duty of candour, about being open in the NHS when a mistake is made, already existed in the regulatory codes of the clinical professionals.
And again – it’s not actually the legal instrument as drafted which is the main problem (though there are problems here). It’s whether anyone is observing them properly: see for example ‘wilful neglect’ (section 44 Mental Capacity Act), national minimum wage, or deprivation of liberty safeguards.
Osborne does not want to come even close for apologising for the record debt, the colossal borrowing, the poor living standards, or the fact that his plan to pay off the deficit has been tragically bad.
I don’t know whether this is a pride thing, but in the real world it has a knock on effect for whether you can pay for health and care. We know the social care budget has been on its knees for years.
Many NHS Trusts are in deficit. This can’t be due to the nurses, most of whom have not experienced a pay rise for years. It may be due to the salaries of top CEOs in the NHS who have to ‘deliver’ on metrics which do not necessarily reflect high quality care (e.g. the ‘four hour wait’). Or it could be due to paying off the loan prepayments for PFI under successive governments.
I really like members of the NHS campaigning parties, but discussions about the NHS have to be linked with the discussions of the state of the economy. It’s an elephant in the room.
Likewise, for all of the slagging off of the Efford Bill, I can guarantee that the statutory instrument UKIP would like to introduce would be far more controversial.
UKIP at least do entertain a discussion on leaving Europe and European law, sort of, even if they do not have any plans for the UK economy.
The Efford Bill was seen in some quarters as ‘the trojan horse for privatisation’, and I can see how interpretation of the clauses might result in this conclusion. I think a problem the Efford Bill was ‘reverse engineering’ to comply with EU competition law – i.e. clauses which perhaps sound as if they’re providing exemptions from EU law, but nobody actually knows.
Not even the best legal minds in the country, of which I am not one, know.
But the EU is founded on free movement of people. Tick – I remember working as a junior in NHS hospitals in London, and simply the day to day operations of these Trusts would have been impossible without the hard work of staff nurses predominantly from India and the Philippines.
And it is also founded on free movement of capital.
There is a genuine feeling of ‘I wouldn’t start from here’ for NHS campaigners in NHAP and Keep our NHS Public. They certainly want to go to a NHS inspired by Nye Bevan which had never heard of section 75 or TTIP.
But it is impossible to have this debate in the absence of a discussion of Europe. It’s impossible to have a debate on the NHS in the absence of a wider debate on the economy.
Russell Brand and Nigel Farage may be grandstanding, but on the face of it they seem to be coming from different places, and with huge followings.
This all matters as it is highly unlikely a Labour-UKIP coalition could be made to work on the NHS, given we know such little about what accommodations UKIP might make on EU competition law or the economy.
We don’t know whether UKIP supports ‘efficiency savings’ however.
All of this is not a leading to a conclusion of ‘Vote Labour’. Labour has not overtly apologised for some thorny apsects of NHS policy, in the same way that Osborne has not apologised over the economy. But it does seem to have apologised for a lot – like letting the market in too far – but curiously not PFI?
I am particularly mindful that there are some ‘real’ experts in NHS policy who are far more experienced and wiser than me. I am also in strong admiration of campaigners wherever they hail from; many of whom have experience of seeing patients regularly.
I never see patients unless they’re friends of mine; and that’s purely for social reasons.
But the next Government’s policy on the NHS will be severely affected by the mistakes of the current Government, part of which ironically has a catchphrase ‘strong economy, fair society’.

‘Friendly’ is one thing, but communities need to ensure people with dementia have the law working for them
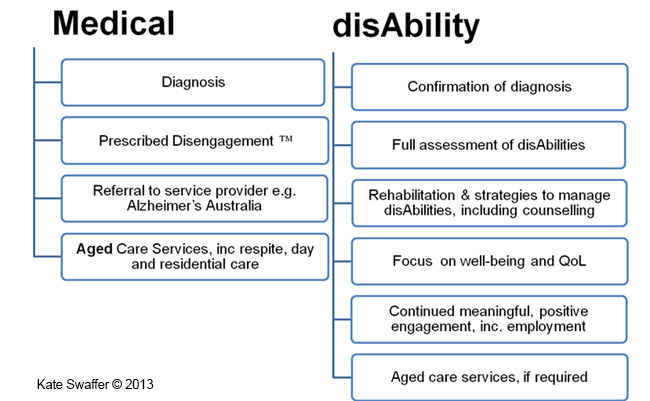
Kate Swaffer (2014) has written about her perception of the receipt of a diagnosis of dementia. The account given by Swaffer is widely held, it turns out.
“The cost of this Prescribed Disengagement™ sets up people with dementia to become victims or sufferers, their partners to eventually start behaving like martyrs and to take over for the person diagnosed. It sets up people with dementia to believe there is no hope, there are no strategies to manage the symptoms of dementia, and more importantly, that it’s not worthwhile trying to find any. It negatively impacts self-esteem, a person’s finances, relationships and the ability to see any sort of positive future. Having dementia does not mean you have to give up living a pre-diagnosis life, nor living beyond your diagnosis. For some, following a diagnosis of dementia, their whole life becomes about dementia and many seem to forget to keep living the other parts of their lives. This is the negative effect of the Prescribed Disengagement™.
Prescribed Disengagement™ also takes away any power or control of the person diagnosed, giving it all to the family carers and service providers. It is unhealthy and wrong. Dementia is the only terminal illness I know of where people are told to go home and give up, rather than to fight for their lives. Prescribing disengagement also lowers a person’s own expectations about how they can live, and it lowers others’ expectation about how we can function and live, including employers, health care professionals and service providers.”
(Swaffer, 2014)
Under international law, the Convention on the Rights of Persons with Disabilities exists to protect citizens with disability.
a) of the Preamble states:
“The States Parties to the present Convention,
- Recalling the principles proclaimed in the Charter of the United Nations which recognize the inherent dignity and worth and the equal and inalienable rights of all members of the human family as the foundation of freedom, justice and peace in the world,”
The Equality Act (2010) in England and Wales makes discrimination against persons living with disabilities unlawful. Dementia is a disability.
On 6 December 2014, the BBC news website ran article with the title “Disabled people’s access to High Street ‘shocking’, audit finds”.
According to the report, accessibility experts DisabledGo visited all of the 30,000 venues in person to assess them, in the largest ever audit of its kind in the UK. They found a fifth of shops had no wheelchair access, only 15% of restaurants and shops had hearing loops and three quarters of restaurants did not cater for those with visual impairments.
If we are shocked about this lack of access for people who are physically disabled, we should be equally shocked for lack of accessibility for people with cognitive or behavioural problems from living with dementia.
Swaffer in her analysis goes onto compare the medical and the social responses to the event that is the disclosure of the dementia diagnosis.
“Misguided and preconceived misconceptions about the symptoms of dementia are used to support telling us to give up living our pre-diagnosis lives. Instead, the recognition of the symptoms as disabilities would assist with a more equitable and dementia-friendly experience for the person with dementia after diagnosis. In contrast to the medical model, the disAbility model of care is positive and supports continued engagement with our prediagnosis lives. “
This picture is from: here.
For the sake of parity of esteem, in other words not treating mental health as inferior to physical health, we need to apply the same rigour for ‘reasonable adjustments’ for cognitive or behavioural interventions as for physical ones.
Equality law recognises that bringing about equality for disabled people may mean changing the way in which employment is structured, the removal of physical barriers and/or providing extra support for a disabled worker (see, for example, the Equality and Human Rights Commission website, 2014).
Coincidentally, yesterday, the British Psychological Society (2014) launched its new publication on care pathways for early stage dementia and psychological interventions in early dementia.
Here’s Agnes by their stall in Glasgow (Scotland).

In other words, buildings should have adequate signage for people living with dementia of the Alzheimer Type. It is beyond reasonable doubt that early dementia of the Alzheimer type is characterised by problems in learning and memory, including in spatial navigation (Serino and Riva, 2013).
It is also beyond reasonable doubt that people with such cognitive disabilities will benefit from specialist design as a reasonable adjustment (Habell, 2013).
The recognition process for dementia friendly communities is currently being developed by the Alzheimer’s Society (2013). I feel itwill be a valuable opportunity for people to demonstrate that they are not only obeying the letter of the law, but they are also entering into the spirit of it.
References
Alzheimer’s Society (2014) Recognition process for dementia friendly communities. http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=2136
BBC News website (6 December 2014). “Disabled people’s access to High Street ‘shocking’, audit finds” http://www.bbc.co.uk/news/uk-politics-30342957
British Psychological Society. 3 Days To Go to Launch of ‘Clinical Psychology in Early Stage Dementia Care Pathway’ and ‘A Guide to Psychosocial Interventions in Dementia’ (1 December 2014) http://www.psige.org/news/33/3+Days+To+Go+to+Launch+of+%27Clinical+Psychology+in+Early+Stage+Dementia+Care+Pathway%27+and+%27A+Guide+to+Psychosocial+Interventions+in+Dementia%27
Equality and human rights commission. (2014) Workplace adjustments. http://www.equalityhumanrights.com/private-and-public-sector-guidance/employing-people/work-place-adjustments
Habell M. Specialised design for dementia. Perspect Public Health. 2013 May;133(3):151-7. doi: 10.1177/1757913912444803. Epub 2012 Jun 22.
Serino S, Riva G. Getting lost in Alzheimer’s disease: a break in the mental frame syncing. Med Hypotheses. 2013 Apr;80(4):416-21. doi: 10.1016/j.mehy.2012.12.031. Epub 2013 Jan 29.
Swaffer, K. (2014) Reinvesting in life is the best prescription (1 December 2014) Australian Journal of Dementia Care, http://journalofdementiacare.com/reinvesting-in-life-is-the-best-prescription/
UN Convention on the Rights of Persons with Disabilities, http://www.un.org/disabilities/convention/conventionfull.shtml

Clinical nursing specialists for dementia put the precise rôle of the third sector to the test
Ed Miliband, most people agree, is set to be the leader of the largest party at Westminster next year at least. This would give him overall charge of the legislature and the executive on 8 May 2015.
He has also pledged to produce 20,000 extra nurses, though talk is cheap. George Osborne has failed on virtually all ambitions that were set for the economic performance of the current Government. The Conservative-Liberal Democrat coalition therefore bequeath the next Government with a society with a terrible frail economy.
This UK economy is essentially a bargain basement one. It is easy to spot the major fault with ‘the record number of jobs’ meme, as the actual till receipt income is very low. And yet the Conservative want to pay for tax cuts – we’ve gone from an over bloated state to an under nourished one.
I had the enormous pleasure, with two other Dementia Friends Champions Chris Roberts and Jayne Goodrick, of giving a Dementia Friends information session at my law school yesterday. I can’t praise enough the amount of support we were given from the people who run Dementia Friends.

Forgive my photography. I am no David Bailey*. We actually had a good turnout, but I managed to capture the part of the audience which was very lean. Chris Roberts (@mason4233) lives well with a mixed type of dementia, thought to be a mixed Alzheimer’s disease and vascular dementia.
Somebody came up to me at the end of the audience and said, “It was absolutely brilliant as it was just incredible to see for my own eyes somebody living well with dementia.”
The “Dementia Friends” initiative has been a successful one. From the Alzheimer’s Society, and supported at a distance by Public Health England, it is modelled on the Japanese ‘caravan befriending’ movement. Its aim in policy terms was to break down the stigma, prejudice and discrimination which can happen against people living with dementia. These factors can contribute to the social isolation often experienced by people on receipt of a probable diagnosis.
“Dementia Friends” has been brilliant for myth busting, with actual facts about dementia too.
Recently, Kate Swaffer (@KateSwaffer), leading international advocate living well with dementia, and working with Alzheimer’s Australia, leading for the Dementia Alliance International, met Dennis Gillings this week in a small group of people for dinner. Gillings is the newly appointed World Dementia Envoy.
For reasons which are completely inexplicable, there is no established substantial representation on that panel from the communities of people living with dementia or caregivers, although Hillary Doxford was documented in the Communiqué of the last meeting just gone.
When Dennis met Kate recently, Kate quipped, typically characteristically in a beautiful tongue-in-cheek manner, she had not ben dribbling into her soup (Kate’s blogpost here).
But “Dementia Friends” is an interesting example of a private-public initiative with a £2.4 million funding base. Had this been left entirely to ‘market forces’, it is unlikely there would have been national outreach for this unique project. Inevitably the topic in policy terms is whether the substantial cost of Dementia Friends is offset by the value of raising the profile of dementia and caregivers. Where it might fail on its outcomes, and time will tell, is how the pledges of turning communication into action are actually hard evidenced through the number of pledges (irrespective of whether it will hit its target of one million within an extended deadline of the end of 2015).
In my opinion, it has been.
Two days previously, I enjoyed being at the Methodist Central Hall for a day for the Dementia Action Alliance.

And yet it is also true that social care is on its knees.
You don’t have be a great story teller to communicate a tale of the NHS on its knees.
This is somewhat cognitively dissonant with MPs wearing their Dementia Friends badges with pride, one could argue.

I agree with Jeremy (tweet here) in that the third sector should not need to apologise for fundraising. Making a surplus for a charity is a raison d’être for a charity akin to the duty to maximise shareholder dividend for a business.
But larger charities share many operational and cultural characteristics with corporates conceivably, and therefore the principles of a good ‘corporate citizen’ could easily apply to large charities with substantial revenues.
Sube Banerjee, long time supporter of the Alzheimer’s Society, and, perhaps more significantly here, co-author of the previous 2009 English dementia strategy came to the Dementia Action Alliance table with some noteworthy criticisms of how the current strategy had been executed.
Firstly, Sube, now a Chair of dementia at the Brighton and Sussex Medical School, commented on the devaluing of the ‘cost’ of a diagnosis to £45, and commented specifically on the culture of a ‘high quantity low quality’ approach to diagnosis.
Indeed, the 2009 English dementia strategy, called ‘Living well with dementia’, refers to the need for high quality diagnosis.
And the English dementia policy as it was then, before it got taken over by the Prime Minister’s Dementia Challenge, due to expire next March 2015, also warned about the lack of post-diagnostic support.
People living with dementia, and their family members, have consistently remarked to me how they have been told by medical professions that their rôle is at the very start and very end of “the dementia journey”. They won’t be there for them in between.
We are all aware of recent findings that 9 out of 10 care homes failing to meet standards set by the regulator the Care Quality Commission, reported not just in the Daily Mail.
So there is an overwhelming sense that people with a possible diagnosis of dementia are being set up for a fall by an inadequate care system, which is disjointed, increasingly privatised, and undervalued.
One of the undesirable consequences of this bargain basement economy is the sheer undervaluing of paid carers on zero hour contracts, some not even getting any travel expenses or the national minimum wage.
This poses serious questions about us as a society. So does the lack of support we appear to be giving unpaid family caregivers, an army of which nearing a million are the backbone of the entire system.
But Jeremy’s tweet does also pose serious questions about what charities could or should fundraise for. I say this as I remember one of own interview questions to read medicine at Cambridge – which I did between 1993 and 2001 – “to what extent should charities take the place of a properly funded NHS?”
Well, this question has taken on a new twist. I do not see there to be a ‘competition’ as such between ‘dementia advisers’ of one charity and ‘specialist nurses’ from another third sector charity. I think they co-exist. ‘Dementia advisers’ are possibly more useful for the more independent parts of the support of “the dementia journey”. ‘Specialist nurses’ are pivotal at all parts, including the care part of ‘the dementia journey’.
It has struck me how not only cost effective clinical specialist nurses are, in providing proactive case management for people with dementia with personalised care plans, ‘nipping in the bud’ complications from medical conditions. I know internationally one of the campaigning for fundraising themes is the substantial co-morbidity of dementia. People living with dementia often have a plethora of other problems, such as in joints, heart or lung.
Sally Greengross has long made it been known that the post diagnostic support for dementia is not good enough. Sally Greengross is the current Chair of the All Party Parliamentary Group on dementia. Her predecessor, Jeremy Wright MP, currently the Government’s Attorney General, launched the highly successful policy here in England of an ambition to reduce the number of inappropriate prescriptions for antipsychotics predominantly in care homes.
Hospitals can be some of the worst places a person with dementia to end up in. Likewise, it shouldn’t be conceived that secondary hospital care is necessarily synonymous with someone who has ‘failed’ somehow. But, say, end of life nurses will be able to provide expert help, wherever the appropriate care setting is deemed to be for a person living with dementia (and his/her friends or family).
And it is therefore possible charities such as Dementia UK and others might be able to fill these gaps in service provision. For a start, clinical nursing specialists comprise an innovative way of delivering the dementia post-support service. And the NHS has a statutory duty to promote innovation.
 However, I should say that that statutory clause (14X) on CCGs is from the much loathed Health and Social Care Act (2012), about to be repealed by the next Labour government.
However, I should say that that statutory clause (14X) on CCGs is from the much loathed Health and Social Care Act (2012), about to be repealed by the next Labour government.
It is sometimes the case innovation can be incubated in places other than the NHS, and we’ve already seen a lot of goodwill and real-life financial support for Macmillan nurses. It would be impossible now to think of palliative care for nursing in cancer to be without Macmillan nurses – and the prime contractor model could be a way of providing sustainability in critical areas of services. This is ONLY provided that the quality and cost effectiveness components are managed correctly and for the benefit of the taxpayer. The next Labour government wishes to bring out a huge systemic innovation of integrating health and care into whole person care. This is long overdue, as, for example, it is impossible in places to discharge NHS patients to social care in s timely fashion. This is not cost effective; it is insulting particularly to patients including frail old citizens who do not wish to be in hospital anyway, and do not deserve the pejorative insulting label of “bed blocker”.
I am sure Alistair (@ABurns1907), or whoever ends up predominantly penning the new English dementia strategy, will wish to give careful consideration to how this post diagnostic support can be provided. Jeremy has a point, but up to a point.
*Joke by @JayneGoodrick.

Why are some journalists getting snooty over the social media campaign #CameronMustGo?

One of my fondest memories is when the late great Tony Benn used to pronunciate ‘socialism’ as ‘social-ism’.
I remember sitting in countless snooty debates about how the social media will never have any influence on mainstream politics.
And it is complete bollocks.
Andrew Neil’s style of interviewing, in which he blatantly despises the socialist point of view, makes my hair stand on end.
I’ve lost count of where the BBC have parrot-repeated press releases getting rid of the words “Jeremy Hunt said…”
The social media is great as we discuss issues which nobody wants us to talk about. We discuss how it has been observed that the welfare reforms are alleged to have driven some disabled citizens to suicide.
We discuss how the recovery led by the Conservatives and the Liberal Democrats is utter bollocks. The income from the tax receipts is unsurprisingly low due to the sheer number of employment contracts which pay a pittance to staff that they have to be topped up by working tax credits.
Employers are having a laugh.
The debate is utter crap. I don’t give a shit what White Van Man thinks, and that’s got nothing to do with living with North London. I do however care about social care being on its knees so that NHS hospitals can’t discharge patients in a timely prompt fashion.
So do I care about #CameronMustGo?
Too right I do, as I have absolutely zero confidence in the BBC domestic news, which has failed to discuss the legislation of the Health and Social Care Act (2012), nor the annihilation of legal aid in England.
They have refused to mention the flagship policy of Labour of finally integrating at a national level the health and care systems.
More and more people are regarding voting behaviour like customer behaviour. But I liken this to shoppers wanting to base THEIR judgment instead of buying the product that is being continually rammed down their throats.
I don’t give a monkeys about Nigel Farage and his merry band of men alleging that the quality of life of indigenous Brits is suffering due to immigrants. This is an insult to all the hardworking staff in NHS hospitals, including the ones who treat White Van Man.
This is a Government on its last legs. The LibDems may think it’s delivering a strong economy with national debt going through the roof.
I’m not sticking to their long term plan.
In fact, I’m flushing it down the toilet with a bottle of Domestos.
Welcome to Political Blogs
I am basically a member of the UK Labour Party. I thank the late Baroness Thatcher, as I found her administration repulsive. I think though her greatest achievement was toxifying the Labour Party, and we are slowly making up for lost time. It is clear that some people are sick of being enslaved by financial markets, while some people seem to be doing extremely well, thank you. The way that the sick and disabled have been treated by the Liberal Democrats working for a ‘fair society and strong economy’, The annihilation of legal aid in their bid for a ‘fair society’ equally repels me. in conjunction with their Conservative masters disgusts me. In the Wartime coalition, Labour criticised the Conservatives’ policies and got credit for it. Instead, the Liberal Democrats have bent over backwards so much it hurts. They will reap what they so. We seem to have enough money to go to war, but not enough money to keep an adolescent with mental health problems out of a police cell for a night. The economy is clearly screwed, with falling tax receipts, in a race to the bottom with zero hour contracts favouring hedge funds and employers who don’t give a monkeys about workers’ rights. I have never seen David Cameron eat a bacon butty, but I don’t think I would like that either.

Yes, I am getting totally sick of NHS campaigners too

The tragedy about the context to what I am about to say is that the NHS is THE issue of the next election.
Cameron is not a leader. He’s a manager, and not a very good one.
A couple of days ago, the ‘New Economics Foundation’ published an interesting report on how the NHS reforms had been sold on false pretences.
It was an excellent report.
The story starts in the 1980s with full gusto.
Market-based reforms began in the 1980s, when support services were first contracted out, but, according to the report, continued in the 1990s, with the creation of an internal market for clinical services.
The claim was that increased competition can improve both efficiency and quality of care is a central justification of market-based reforms and the Health and Social Care Act.
The King’s Fund thought it might do too.
But many of us knew this was utter bollocks.
Reams and reams of evidence was published to the contrary, such as on the LSE blogs.
On page 5 of the Report, the experience from Serco makes chilling reading:
“Before pulling out of the Cornwall contract, Serco had replaced clinicians on its out- of-hours service with call-handlers who did not have medical training but followed a computer-generated script. The new system quadrupled ambulances called. Call handlers were then told to make new checks before calling 999 when they received what appeared to be emergency cases, so that managers could cut down the number of referrals they made to the ambulance service. A leaked management email to staff described how they should use their computer system to meet targets set down in the company’s contract on 999 responses.”
Often the NHS discussion goes round and round and round and round and round and round in circles of who started it and who continued it.
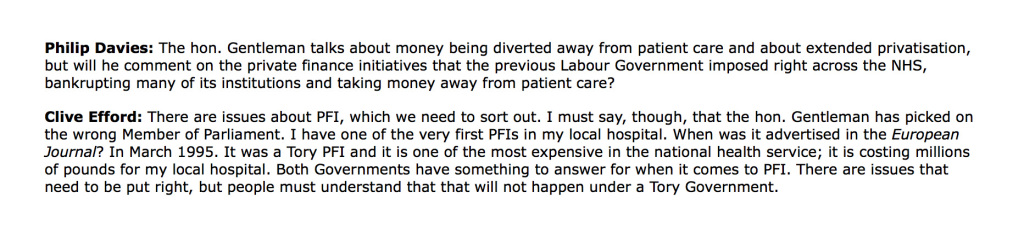
On the “private finance initiative” –
“This is a scheme that enables private companies to design, build and operate NHS (and other) facilities, using capital raised through financial markets, and then rent them back under long-term contracts lasting 30 years or more.
First introduced by the Major government, this approach was popular with New Labour, with nearly three-quarters of hospital building schemes funded through PFI between 1997 and 2009.”
And desperate Dan Poulter pulled the same rabbit out of the same that last week.
Labour “started it” with their NHS Competition and Co-operation units. They started it with their “Independent Sector Treatment Centres”.
Except… Labour didn’t start two things in particular.
One – the breach of the “four tests” in reconfiguration, which saw Lewisham win both in the High Court and Court of Appeal.
Second – the legal provision in section 76(7) Health and Social Care Act (2012), from the current Government, of a threat if services do not go to out to competitive tender if there is not a sole bidder.
We saw the same crap last week.
People saying the Clive Efford Bill didn’t go far enough – except nobody said it would abolish the purchaser provider split, PFI, the £2bn funding gap, Foundation Trusts or mutuals, or advance integration of health and care.
NHAP and KONP have gone mute on integrated care and whole person care.
There is absolutely no doubt that the situation where NHS hospitals cannot discharge patients to social care is a situation which cannot carry on.
NHS campaigners seem more concerned about proving how correct they are, than offering constructive thoughts on, say, how to improve wellbeing in long term conditions.
Mid Staffs in some quarters has furthered a toxic atmosphere of malice and retribution, and a culture of fear and nastiness, rather than thinking about how things can improve.
And it has produced a generation of journalists who are the new model jury of the health and care professions.
… except regulation of primary care was not built entirely around Harold Shipman… Harold, under a Tory Government, in case you’re wondering.
No wonder the Staffs area was plunged into a recruitment crisis after all their negative publicity.
GP surgeries are shutting like no tomorrow, and yet Hunt puts pathetic above more pathetic, while some of us are trying to put people before profit.
There will be only one party of Government on May 8th 2015. It might be a temporary Government but we don’t know who it is yet.
UKIP has made utterly contemptible comments about the NHS in the past which are well documented. The idea that Labour can work with UKIP in promoting the NHS is more than disgusting.
So another week and it’s the same old same old tired discussions.
It’s clear to me that some people prefer the foreplay to the actual act.
And it’s entirely all driven by egos. Again.

Who exactly is in denial over the Clive Efford Bill?

The Private Member’s Bill brought forward by backbencher Clive Efford MP passed by 241 votes to 18.
“From crisis to opportunity — putting citizens and companies on the path to prosperity: A better functioning internal market is a key ingredient for European growth” was updated in November 2014.
This publication is part of a series that explains what the EU does in different policy areas, why the EU is involved and what the results are.
It provides that, “The European internal market, also referred to as the single market, allows people and businesses to move and trade freely across the 28-nation group. In practice, it gives individuals the right to earn a living, study or retire in another EU country.”
It further adds that, “It also gives consumers a wider choice of items to buy at competitive prices, allows them to enjoy greater protection when shopping at home, abroad or online and makes it easier and cheaper for companies large and small to do business across borders and to compete globally.”
Not wanting to be part of Europe was of course how the late great Tony Benn used to be in agreement with Enoch Powell, even though they came from totally different political stables.
On 1 January 1973, Britain joined the “Common Market”, the European Economic Community, under a previous Conservative administration.
There has of course been a strident debate as to whether the free movement of capital, so important for capitalism, is inherently compatible with socialism at all.
Being a member of the EU, the UK has to sign up to the rules and regulations of EU law.
The current position of Labour is that the market ideology went too far under previous Labour administrations.
Critics of Labour say that they are still in denial over the “sweetheart deals” to encourage private provision under a previous administration. Labour argues that this private provision was necessary to improve clear a backlog in NHS work which existed at the time, rather than introducing private provision for the sake of it.
Much criticism centres around the “independent sector treatment centres”. John Rentoul unsurprisingly found himself in agreement with the approach Labour took at the time.
Many still within Labour still loathe what happened here. NHS campaigners affiliated to other parties have been critical of Labour in inadvertently contributing to the privatisation of the NHS, and are concerned it will happen again.
Critics point to unconscionable transactions under the private finance initiative, for example.
But historically this strand of policy started under a previous Conservative administration under Lord Major.
Clive Efford MP even referred to his local hospital in Eltham having been set up as the country’s first PFI hospital in last week’s debate on “The Clive Efford Bill”.
Given that we are under treaty obligations, unless there were a radical renegotiation of an unilateral exemption of the market aspect of the EU, we are stuck with a market in some form.
To argue otherwise would be in denial.
None of the front team of Labour have argued for abolition of the market altogether, to my knowledge.
But that is not to say that the ‘purchaser provider split’ might be abolished internally within England, notwithstanding treaty obligations.
The argument is that the market costs billions as it introduces “transaction costs”. The ‘household analogy’ is often used to explain the diversion of resources needed to monitoring the various transactions within a household at microlevel.
The market has become particularly problematic for the NHS, as was widely predicted before the Health and Social Care Act (2012). I myself wrote an article on the impact that section 75 Health and Social Care Act (2012) would have on the Socialist Health Association blog on 7 January 2013.
And the former CEO of NHS England, Sir David Nicholson, himself drew attention to how it had become a magnet for competition lawyers.
This was entirely to be expected as it was this clause which signalled a marked diversion from previous law under the most recent Labour government (viz section 76 sub 7 Health and Social Care Act 2012).

Elsewhere in the legislation it says that you do not have to put contracts out to competitive tender if there is only one sole bidder, which hardly ever happens.
To deny that the current legislation departs from the previous legislation is, arguably, denial.
So the “Clive Efford Bill” was finally debated last week. You can read it here. The official explanatory notes for the Bill are here.
The guidance given to the legislature is useful.
For example, for clause 6, it is provided: “The clause also enables the NHS to take advantage of exemptions to procurement obligations as set out in the European Union Directive 2014/24/EU.”
The Directive provides the ‘codification of the Teckel exemption‘.
The Teckel Exemption has proved important as an exemption from EU competition law when applied to the NHS.
Clause 1 posits that the NHS is a system based on ‘social solidarity’.
Solidarity is another mechanism of providing an exemption from EU competition law. In fact, the lack of solidarity was one of the criticisms of the Health and Social Care Bill made at the time made by ‘Richard Blogger’.
The Poucet and Pistre Case C-159, 160/91 case sheds light not heat on the ‘social solidarity’ exemption of competition law.
A reasonable concern is whether the ‘Clive Efford Bill’ hangs on by its claws to the notion of the NHS being comprised of ‘units of economic activity’ as per s.1 sub (2)(b):
But here it is the “Clive Efford Bill” which may be in denial.
Scrutiny in the Committee stage will have to be given as to whether the term here should be “general economic interest” or “general interest”.
The Government’s own guidance on this implementation of EU law is here.
If the direction of travel for all mainstream governments is genuinely to keep the proportion of private provision low, “general interest”, arguably, would be more suitable if the majority of health provision is not intended for profit.
It has been a consistent mantra from the Labour front bench “to put people before profit”, for example.
There are other issues about the significance of the words ‘deliver’ and ‘promote’ in the duty of the Secretary of State for Health.
The view of David Lock QC is here. The view of “The Campaign for the NHS 2015 Reinstatement Bill” is here.
Would a rose by any other name smell as sweet? It is a deeply entrenched position of the legal profession that lawyers look at the substance not the form.
As a statutory aid to the wording of this legislation, there is this paragraph lurking on the internet from David Lock QC from June 2013 which lends support to the notion that it is most useful if the ‘Clive Efford Bill’ is a statutory instrument best read as a whole.
Assuming that events do not overtake us, in other words we do not get chucked out of Europe imminently or the UK does not get bound in indefinitely over TTIP, we should in theory have some freedom to legislate for what sort of health service we want.
This is provided for in Article 168(7) TFEU.

It is therefore crucial we draft this legislation correctly.
Taking the position that there must be no criticism of the drafting of the Clive Efford Bill, arguing that it will undermine its implementation at Committee Stage, I think is an unreasonable position to adopt.
Likewise, grandstanding over “who is right” is inappropriate as well. There are possibly as many legal opinions as there are lawyers. We will not know with any certainty unless the Clive Efford Bill, if enacted, is put to the test by the judiciary; and even then, it will not be absolutely certain.
I think the Clive Efford Bill clearly positions itself as exempting itself from the overall gambit of EU competition law.
“It says what it does on the tin”. It is an immediate mechanism, if enacted, for getting rid of the toxic section 75 and baggage. It has been a useful campaigning tool.
But, if there is a Labour government of some sort in May 2015, it is already proposed that there will be regulation of health and care professionals as per the recommendations of the English Law Commission. This should have been in the last Queen’s Speech just gone, but the current Government chose to park this issue. Furthermore, quite drastic changes to the law will still be needed to promote integration of health and care to make whole person care work smoothly and legally. I first wrote about that issue here on this blog in June 2013. Decisions, made on clinical grounds, must be clear of competition obstructions, Enmeshing the NHS with the Enterprise Act over mergers has been a disastrous development in national policy, for example witnessed in the Bournemouth and Poole merger.
So it’s pretty likely that “The Efford Win” is the opening salvo in a war for the soul of the NHS. Time will tell whether UKIP are genuinely against privatisation. I’d bet my life on the fact are far from cuddly socialists. Their policy across a number of areas changes very rapidly, so only time will tell. The more parsimonious explanation is that UKIP are acting completely opportunistically, and wish to win seats off disaffected members across all the mainstream parties. A Labour-UKIP coalition would be very difficult to implement, whatever one thinks of Ed Miliband’s ability to negotiate a bacon butty.
The final conclusion to my book on living better with dementia
Anything can happen to anyone at any time. Despite all the best initiatives in the world, it will be unachievable to extinguish all negative perceptions about dementia. Nobody can deny the imperative for communities and society to be inclusive and accessible for people with dementia, but is no mean feat to rationalise with more individualistic approaches ranging from personal budgets, human rights and equality law responsibilities. It really is not a question of what a person can no longer do. It is an issue of what a person can currently do, and this might include, for example, unleashing of previously unwitnessed artistic and creative talents.
All jurisdictions converge on the right for a timely diagnosis and a right to timely post-diagnostic support, but political grandstanding over cures will be small change to those people currently wanting to live better with dementia. People who have received a diagnosis of dementia are not all consumers, and some do not even interact with health and care services as patients. They are all persons, however, and wish for inalienable dignity and respect. Everyone knows that the diagnosis affects not just the person with dementia,but their whole network of friends and family. There now must be a political will to do something about this, and this is not just a societal issue for the G7. Silos must be abolished; for example, in considering eating better with dementia, the emphasis can no longer be on the design of ‘finger snacks’, but responsible thought has to be put into how certain mealtime environments work (or do not work). It is utterly pointless talking about joining initiatives to encourage ‘dementia friendliness’, while words such as ‘victim’ continue to litter the mainstream press. And “leading” scientists and practitioners can unwittingly perpetuate stigma through somewhat perjorative language such as ‘wanderer’; the willful blindness to this must stop too. Living better with dementia is not just an aspiration; it is in many places legally enforceable.
Bring it on.

