Home » Posts tagged 'Royal College of General Practitioners'
Tag Archives: Royal College of General Practitioners

Living well with dementia: diet not drugs?

There is no cure for dementia currently. The available treatment strategies offer mainly symptomatic benefits. Thus, strategies to prevent or delay onset of dementia by changes in lifestyle factors, such as diet, are therefore important, given finite resources. There is no doubt it’d be wonderful if, after many many years of trying, there might be a breakthrough.
But physicians and politicians have a responsibility to the general public to be honest about what is genuinely achievable. It’s in the interests of charities and research groups which depend on income for their research to raise money for a cure; or in the interests of those research groups wishing to raise money for research which appears linked to that somehow. It’s in the interest of Big Pharma-ceutical companies to raise money for their research funds; and they have a legal duty to their shareholders too. The public appreciate a truthful debate about what might work; and where a lot of monies would in fact would be better spent elsewhere.
It’s certainly low hanging fruit for politicians to support this worthy cause.
However, the scant attention to living well with dementia in many statements, in contrast to drug treatments, is very telling. The Department of Health will, however, be livestreaming the #G8dementia summit proceedings later this week. Details are here.
Not all dementia occurs in the elderly. Nonetheless, it is possible that health problems related to aging (including dementia of the Alzheimer type) are projected to add to the high clinical, social, and economic burden of caring for persons with dementia.
The Mediterranean diet has been associated with reduced risk for a wide range of age-related conditions such as stroke, type 2 diabetes, cardiovascular disease, and all-cause mortality. The traditional Mediterranean diet refers to a multinutrient dietary profile characterized by high intake of fruits, vegetables, cereals, and legumes; low consumption of saturated fats with olive oil as the main source of fat; moderate consumption of fish; low to moderate intake of dairy products (in the form of yogurt and cheese); low consumption of red meat and meat products; and moderate amount of alcohol (especially wine) usually consumed during meals.
Recently, a number of peer-reviewed pieces in the reliable academic literature have presented evidence for an association between a Mediterranean-type diet and decreased risk of dementia. Findings from prospective studies suggest that greater adherence to Mediterranean diet may be associated with slower cognitive decline and reduced risk of Alzheimer disease. In the light of these findings, it has been suggested that improving adherence to the Mediterranean diet may delay or prevent the onset of dementia.
A really helpful review was published by Lourida and colleagues earlier this year in the “Epidemiology” journal (Jul;24(4):479-89). Twelve eligible papers (11 observational studies and one randomized controlled trial) were identified, describing seven unique cohorts.
Despite methodological heterogeneity and limited statistical power in some studies, there was a reasonably consistent pattern of associations. Higher adherence to Mediterranean diet was associated with better cognitive function, lower rates of cognitive decline, and reduced risk of Alzheimer disease in nine out of 12 studies, whereas results for mild cognitive impairment were inconsistent.
Published studies suggest that greater adherence to Mediterranean diet is associated with slower cognitive decline and lower risk of developing Alzheimer disease. Further studies would be useful to clarify the association with mild cognitive impairment and vascular dementia. Long-term randomised controlled trials promoting a Mediterranean diet may help establish whether improved adherence helps to prevent or delay the onset of Alzheimer disease and dementia.
Only today, leading doctors warned the Government the battle against dementia should focus on the benefits of a Mediterranean diet rather than ‘dubious’ drugs. In an open letter to the Health Secretary, they said persuading people to eat fresh fruit and vegetables, nuts, fish and olive oil was ‘possibly the best strategy currently available’ for preventing Alzheimer’s and other memory-robbing diseases.
The letter’s signatories include Prof Clare Gerada, the former chairman of the Royal College of General Practitioners, and Dr David Haslam, chairman of the National Obesity Forum.
It reads:
‘We hope this crisis can be seen as an opportunity towards a real policy change, namely towards a Mediterranean diet, rather than towards the dubious benefits of most drugs.’
It goes on to say the evidence ‘strongly suggests’ that improvements to lifestyle will have a ‘far greater effect’ on the rising tide of dementia than drugs.
The call comes as dementia experts from the G8 countries prepare to travel to London for a summit hosted by the Prime Minister.
Dr Simon Poole, the GP who organised the letter, said: ‘It is all about looking at what pharmaceutical companies can do, which is actually not very much.
‘They talk up their medicine and then it is very often a damp squib. We want some sort of focus on prevention. Educating all generations, including our children, in the importance of a good diet in maintaining health in old age is a project which will take years, but is absolutely essential.’
‘We are calling upon policymakers to not only support the care and treatment of those who are already suffering from dementia, but to make significant investments in work which will see benefits beyond the period of one or two parliaments.’
There has also been a focus on individual components of the Mediterranean diet, such as [omega]-3 fatty acids or olive oil as the main source of monounsaturated fats. Although the advantages of Mediterranean diet are relevant for non-Mediterranean populations, it is often argued that studies are not always comparable because there are substantial differences in dietary composition among countries.
A more detailed examination reveals this is perhaps especially true for fatty acids. Although olive oil is the hallmark of Mediterranean diet, differences in the origin of monounsaturated fats or cooking style (eg, baked vs. fried) could partly explain these inconsistencies. Studies comparing types of olive oil concluded that compared with refined oil, virgin olive oil (rich in phenolic content) has additional anti-inflammatory and antioxidant properties beneficial to cellular function and cardiovascular health.
The Mediterranean diet may exert its effects on cognitive health through multiple biological mechanisms. Relationships with reduced risk of coronary heart disease, hypertension, diabetes, dyslipidemia, and metabolic syndrome have been observed, and these conditions have also been associated with mild cognitive impairment, vascular dementia (a dementia associated with general factors affecting the cardiovascular system such as smoking, cholesterol, diet, family history), or disease of the Alzheimer type.
Sticking to this Meditteranean diet may also facilitate metabolic control because it has been related to improved insulin sensitivity and glucose metabolism. Insulin is a chemical acting in the body which can affect our metabolism – it is an important “hormone” for us.
Furthermore, “oxidative stress” increases with age and results in “oxidative damage”—a state often observed in the brain of patients with Alzheimer disease. Typical components of the Mediterranean diet (namely fruits, vegetables, wine, and virgin olive oil) are rich in antioxidants such as vitamin C and E, carotenoids, and flavonoids. Decreased oxidative stress found in people adhering to a Mediterranean-type diet could partially explain their lowered risk for dementia.
And there’s a plausible biological mechanism for all this. Brain cells (neurone) are protected against oxidative stress by specialist chemicals, called “neurotrophins” (basic proteins) such as the brain-derived neurotrophic factor. There is some evidence that Mediterranean diet may increase plasma brain-derived neurotrophic factor concentrations. Inflammatory processes have also been suggested for Alzheimer pathogenesis. Higher concentrations of C-reactive protein, a nonspecific marker of inflammation, have been associated with increased risk for cognitive decline, Alzheimer disease, and vascular dementia, whereas better adherence to Mediterranean diet has been associated with lower levels of C-reactive protein.
Access to medicine has become a really important issue in the NHS. Already we are getting stories of rationing in the NHS emerging during the period of this Government (such as varicose veins stripping), so it is not particularly surprising if drugs which do have modest effect on memory for dementia are not a top priority. Encouraging people to learn about diet and how this might prevent thinking problems is therefore a worthy aim, as it might actually work better than many of the drugs ‘on offer’. Senior doctors have advised this approach in fact.
Just because it’s not coming from Big Pharma with their massive marketing budgets doesn’t mean it’s a dead duck.
Related articles
- Healthy diet ‘may prevent dementia’ (skynews.com.au)
- Mediterranean Diet is the Key to Preventing Dementia (medindia.net)
- How To Live Longer: Mediterranean Diet Proven To Help Women Live Past 70 (medicaldaily.com)
- Dementia fight must focus on diet, say experts (yorkshirepost.co.uk)

Where is the policy generally heading?
he most ‘perfect’ scenario for dementia screening would be to identify dementia in a group of individuals who have absolutely no symptoms might have subtle changes on their volumetric MRI scans, or might have weird protein fragments in their cerebrospinal fluid through an invasive lumbar culture; and then come up with a reliable way to stop it in its tracks The cost, practicality and science behind this prohibit this approach.
There are well defined criteria for screening, such as the “Wilson Jungner criteria“. Prof Carol Brayne from the University of Cambridge has warned against the perils of backdoor screening of dementia, and the need for evidence-based policy, publicly in an article in the British Medical Journal:
“As a group of clinical and applied researchers we urge governments, charities, the academic community and others to be more coordinated in order to put the policy cart after the research horse. Dementia screening should neither be recommended nor routinely implemented unless and until there is robust evidence to support it. The UK can play a unique role in providing the evidence base to inform the ageing world in this area, whilst making a positive difference to the lives of individuals and their families in the future.”
However, a problem has arisen in how aggressively to find new cases of dementia in primary care, and a lack of acknowledgement by some that incentivising dementia diagnosis might possibly have an untoward effect of misdiagnosing (and indeed mislabelling) some individuals, who do not have dementia, with dementia. Unfortunately there are market forces at work here, but the primary consideration must be the professional judgment of clinicians.
Diagnosing dementia
There is no single test for dementia.
A diagnosis of dementia can only be confirmed post mortem, but there are ‘tests’ in vivo which can be strongly indicative of a specific dementia diagnosis (such as brain biopsy for Variant Creutzfeld-Jacob disease or cerebral vasculitis), or specific genetic mutations on a blood test (such as for relatively rare forms of the dementia of the Alzheimer type).
Memory vs non-memory functions in CANTAB
CANTABmobile is a new touchscreen test for identifying memory impairment, being described as a ‘rapid memory test’. The hope is that memory deficits might be spotted quickly in persons attending the National Health Service, and this is indeed a worthy cause potentially. In the rush to try to diagnose dementia quickly (and I have explained above the problem with the term “diagnose dementia”), it is easy to conflate dementia and memory problems. However, I demonstrated myself in a paper in Brain in 1999 using one of the CANTAB tests that patients with behavioural variant frontotemporal dementia (bvFTD) were selectively impaired on tests sensitive to prefrontal lobe function involving cognitive flexibility and decision-making. I demonstrated further in a paper in the European Journal of Neuroscience in 2003 that such bvFTD patients were unimpaired on the CANTAB paired associates learning test.
bvFTD is significant as it is a prevalent form of dementia in individuals below the age of 60. The description given by Prof John Hodges in the current Oxford Textbook of Medicine chapter on dementia is here. Indeed, this chapter cites my Brain paper:
“Patients present with insidiously progressive changes in personality and behaviour that refl ect the early locus of pathology in orbital and medial parts of the frontal lobes. There is often impaired judgement, an indifference to domestic and professional responsibilities, and a lack of initiation and apathy. Social skills deteriorate and there can be socially inappropriate behaviour, fatuousness, jocularity, abnormal sexual behaviour with disinhibition, or theft. Many patients are restless with an obsessive–compulsive and ritualized pattern of behaviour, such as pacing or hoarding. Emotional labiality and mood swings are seen, but other psychiatric phenomena such as delusions and hallucinations are rare. Patients become rigid and stereotyped in their daily routines and food choices. A change in food preference towards sweet foods is very characteristic. Of importance is the fact that simple bedside cognitive screening tests such as the Mini-Mental State Examination (MMSE) are insensitive at detecting frontal abnormalities. More detailed neuropsychological tests of frontal function (such as the Wisconsin Card Sorting Test or the Stroop Test) usually show abnormalities. Speech output can be reduced with a tendency to echolalia (repeating the examiner’s last phrase). Memory is relatively spared in the earl stages, although it does deteriorate as the disease advances. Visuospatial function remains remarkably unaffected. Primary motor and sensory functions remain normal. Primitive refl exes such as snout, pout, and grasp develop during the disease process. Muscle fasciculations or wasting, particularly affecting the bulbar musculature, can develop in the FTD subtype associated with MND.”
Memory tests, mild cognitive impairment and dementia of Alzheimer type
Nobody can deny the undeniable benefits of a prompt diagnosis, when correct, of dementia, but the notion that not all memory deficits mean dementia is a formidable one. Besides, this tweeted by Prof Clare Gerada, Chair of the Royal College of General Practitioners, to me this morning I feel is definitely true,
A political drive, almost in total parallel led by the current UK and US governments, to screen older people for minor memory changes could potentially be leading to unnecessary investigation and potentially harmful treatment for what is arguably an inevitable consequence of ageing. There are no drugs that prevent the progression of dementia according to human studies, or are effective in patients with mild cognitive impairment, raising concerns that once patients are labelled with mild cognitive deficits as a “pre-disease” for dementia, they may try untested therapies and run the risk of adverse effects.
The idea itself of the MCI as a “pre-disease” in the dementia of Alzheimer type is itself erroneous, if one actually bothers to look at the published neuroscientific evidence. A mild cognitive impairment (“MCI”) is a clinical diagnosis in which deficits in cognitive function are evident but not of sufficient severity to warrant a diagnosis of dementia (Nelson and O’Connor, 2008).It is claimed that on the CANTABmobile website that:
![]()
However, the evidence of progression of MCI (mild cognitive impairment) to DAT is currently weak. It might be attractive to think that MCI is a preclinical form of dementia of Alzheimer Type, but unfortunately the evidence is not there to back this claim up at present: only approximately 5-10% and most people with MCI will not progress to dementia even after ten years of follow-up (Mitchell and Shiri-Feshki, 2009).
An equally important question is also the specificity and sensitivity of the CANTABmobile PAL test. Quite a long explanation is given on their webpage again:
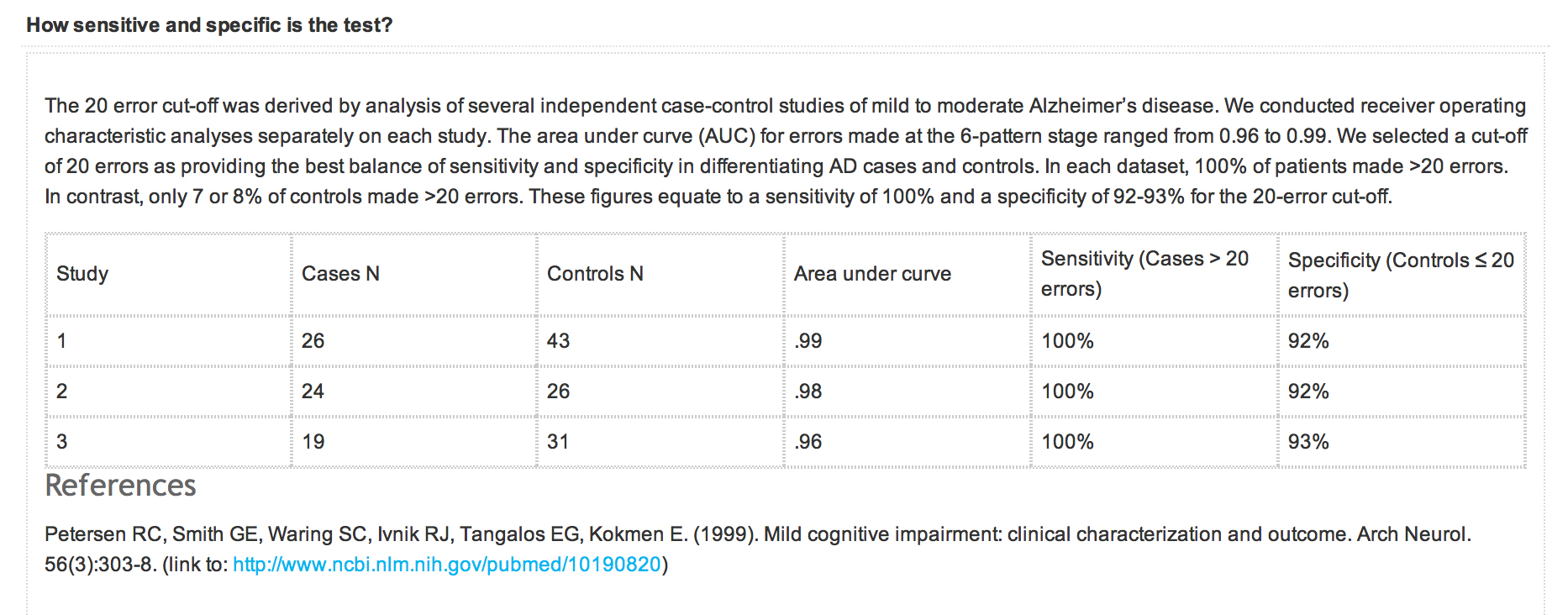
However, the reference that is given is unrelated to the data presented above. What should have appeared there was a peer-reviewed paper analysing sensitivity and sensitivity of the test, across a number of relevant patient groups, such as ageing ‘normal’ volunteers, patients with geriatric depression, MCI, DAT, and so on. A reference instead is given to a paper in JAMA which does not even mention CANTAB or CANTABmobile.
NICE, QOF and indicator NM72
A description of QOF is on the NICE website:
“Introduced in 2004 as part of the General Medical Services Contract, the QOF is a voluntary incentive scheme for GP practices in the UK, rewarding them for how well they care for patients.
The QOF contains groups of indicators, against which practices score points according to their level of achievement. NICE’s role focuses on the clinical and public health domains in the QOF, which include a number of areas such as coronary heart disease and hypertension.
The QOF gives an indication of the overall achievement of a practice through a points system. Practices aim to deliver high quality care across a range of areas, for which they score points. Put simply, the higher the score, the higher the financial reward for the practice. The final payment is adjusted to take account of the practice list size and prevalence. The results are published annually.”
According to guidance on the NM72 indicator from NICE dated August 2013, this indicator (“NM72″) comprises the percentage of patients with dementia (diagnosed on or after 1 April 2014) with a record of FBC, calcium, glucose, renal and liver function, thyroid function tests, serum vitamin B12 and folate levels recorded up to 12 months before entering on to the register The timeframe for this indicator has been amended to be consistent with a new dementia indicator NM65 (attendance at a memory assessment service).
Strictly speaking then QOF is not about screening as it is for patients with a known diagnosis of dementia. If this battery of tests were done on people with a subclinical amnestic syndrome as a precursor to a full-blown dementia syndrome with an amnestic component, it might conceivably be ‘screening’ depending on how robust the actual diagnosis of the dementia of those individuals participating actually is. As with all these policy moves, it is very easy to have unintended consequences and mission creep.
According to this document,
“There is no universal consensus on the appropriate diagnostic tests to be undertaken in people with suspected dementia. However, a review of 14 guidelines and consensus statements found considerable similarity in recommendations (Beck et al. 2000). The main reason for undertaking investigations in a person with suspected dementia is to exclude a potentially reversible or modifying cause for the dementia and to help exclude other diagnoses (such as delirium). Reversible or modifying causes include metabolic and endocrine abnormalities (for example, vitamin B12 and folate deficiency, hypothyroidism, diabetes and disorders of calcium metabolism).
The NICE clnical guideline on dementia (NICE clinical guideline 42) states that a basic dementia screen should be performed at the time of presentation, usually within primary care. It should include:
- routine haematology
- biochemistry tests (including electrolytes, calcium, glucose, and renal and liver function)
- thyroid function tests
- serum vitamin B12 and folate levels.”
It is vehemently denied that primary care is ‘screening’ for dementia, but here is a QOF indicator which explicitly tries to identify reversible causes of dementia in those with possible dementia.
There are clearly issues of valid consent for the individual presenting in primary care.
Prof Clare Gerada has previously warned to the effect that it is crucial that QOF does not “overplay its hand”, for example:
“QOF is risking driving out caring and compassion from our consultations. We need to control it before it gets more out of control – need concerted effort by GPC and RCGP.”
Conclusion
Never has it been more important than to heed Prof Brayne’s words:
“As a group of clinical and applied researchers we urge governments, charities, the academic community and others to be more coordinated in order to put the policy cart after the research horse.”
In recent years, many glib statements, often made by non-experts in dementia, have been made regarding the cognitive neuroscience of dementia, and these are distorting the public health debate on dementia to its detriment. An issue has been, sadly, a consideration of what people (other than individual patients themselves) have had to gain from the clinical diagnosis of dementia. At the moment, some politicians are considering how they can ‘carve up’ primary care, and some people even want it to act as a referral source for private screening businesses. The “NHS MOT” would be feasible way of the State drumming up business for private enterprises, even if the evidence for mass screening is not robust. The direction of travel indicates that politicians wish to have more ‘private market entrants’ in primary care, so how GPs handle their QOF databases could have implications for the use of ‘Big Data’ tomorrow.
With headlines such as this from as recently as 18 August 2013,

this is definitely ‘one to watch’.
Further references
Beck C, Cody M, Souder E et al. (2000) Dementia diagnostic guidelines: methodologies, results, and implementation costs. Journal of the American Geriatrics Society 48: 1195–203
Mitchell, A.J., and Shiri-Feshki, M. (2009) Rate of progression of mild cognitive impairment to dementia -meta-analysis of 41 robust inception cohort studies. Acta Psychiatr Scand, 119(4), pp. 252-65.
Nelson, A.P., and O’Connor, M.G. (2008) Mild cognitive impairment: a neuropsychological perspective, CNS Spectr, 13(1), pp. 56-64.
National Institute for Health and Clinical Excellence (2006) Dementia. Supporting people with dementia and their carers in health and social care. NICE clinical guideline 42
Many thanks to @val_hudson for a useful critical comment about an earlier version of this blogpost.
Time to rate how Doctors are treated in the NHS?
Sir Gus O’Donnell said famously, “If you treasure it, measure it”. This is happening in the medical profession too, with a policy drive that the best people to rate the NHS are the users of the service. These are the patients (or “customers” if you’re that way inclined). The ‘Friends and Family Test’ has come under fierce criticism, not surprising given that it has never been subject to proper analytical rigour, and the criticisms of it have been well rehearsed elsewhere. There is a fundamental difference in assessing your hospital stay, compared to “Trip Advisor”, but it is all part of the information revolution. Information, according to people interested in innovation like me, is not the same as knowledge, and not all information is useful. Whilst the corporates, who introduced their love for Big Data to the rest of the world are fully aware there is a lot of redundant, useless data, and the importance of certain datasets need to be explained carefully, this has completely passed the NHS by. The introduction of the vascular surgery rates was held by some to be a shambles, due to the poor explanation of these data as well as data inaccuracy. Forgetting the fact that certain fields in vascular surgery (e.g. abdominal artery aneurysm repairs for aneurysms diameter > 6.5 cm are considered riskier than sclerosing varicose veins, for example), or that safety is a team activity (though the root cause of a problem can be identified to a single reason), the data explosion is envisaged as empowering patients and persons with ‘choice’.
Enter the market. Jeremy Hunt continues to dodge completely the question why private sector entities under freedom of information legislation introduced by a Labour government are not under obligation to disclose data because of their ‘commercial interest’. As they are not public bodies, they are not amenable to judicial review either. Moving swiftly on, choice is supposed to empower the patient with information. How is that possible, that a patient will be equally fluent as a Doctor of about 7 years’ standing who has achieved registration with the General Medical Council? Very good question. Is it the case that vascular surgeons have a need to improve their mortality data because they are now operating (quite literally) in a free (pseudo)market? No, categorically not. The Royal Colleges of Surgeons and the General Medical Council are responsible for general professional training and higher specialist training standards in surgery. Doctors are increasingly seen as employees in a business case, with Trusts salami-slicing how much they want to spend on staff to achieve their efficiency savings as mandated by Sir David Nicholson and the Department of Health. They are that respect no more essential than an import of horsemeat for lasagna to improve the profitability of a venture capital investment. Registered Doctors are professionals though, and legal.
It has been noted that trust in GPs has plummeted from 70% to 30% since the implementation of the Health and Social Care Act (2012)? I, for one, would quite like to rate how management consultants conducted this important strategic implementation. This £3bn reorganisation had a critical piece of legislation, the “section 75 regulations”, which produced competitive tendering as the default option. The first set of Regulations were so bad they had to be withdrawn. The Medical Royal Colleges, the BMA and RCN all say the Act won’t work. The first rule of strategic implementation is that you involve all the stakeholders and engage in a realistic conversation about what is intended to be achieved, how, why, or when. None of this happened. That is why I award the Department of Health, despite what can be best described as “shuttle diplomacy” by Earl Howe, a big fat result thus:
 And why has trust in GPs plummeted? Is it anything to do with the fact the media and politicians have been force-feeding the public with stories that GPs opted out of out-of-hours some time ago, and they got a deal which was quite lucrative? Or is it because there are now anecdotal reports of GPs having to advise non-NHS care to their patients in the hope that they can jump a lengthy NHS queue? It is very hard to tell. But certainly it is true that GPs have become first in the firing line for the NHS reforms. They in fact opposed the reforms, with clear leadership by Prof Clare Gerada, Chair of the Royal College of General Practitioners. The Government PR went into overdrive that “GPs are at the heart of commissioning”, the ‘clinical commissioning groups’, but this was obviously never the intention. CCGs are merely a vehicle for holding funds and assessing risk in a pooled population, in a manner of ‘statutory insurance schemes’. This has always been the case, and always will be. For all the talk of ‘entrepreneurial GPs’, the public do not appear to warm to the idea of GPs as businessmen (and GPs do not particularly wish to represented as businessmen). Germane to this is the “dual agent” problem, very well known in insurance markets. That is the idea that no person can have “two masters”, without a significant conflict of interest: this might be for example a GP’s professional duty to his or her patient, and his or her duty to the people who ultimately provide the funding. This issue of trust is possibly bound to get worse, as ‘scandals’ are drip fed to the media of a system in distress. The reason this score is nothing to do with Prof Gerada is because Prof Gerada, as the new “NHS SOS” book explains (edited by Dr Jacky Davis and Prof Ray Tallis), was one of the few NHS leaders to have a clear vision and have the charisma to set this out in confidence, a textbook example of a “charismatic leader”, who deservedly was one of the hundred most influential individuals in health. And, very clearly, she appeared to be representing patients as well as GPs.
And why has trust in GPs plummeted? Is it anything to do with the fact the media and politicians have been force-feeding the public with stories that GPs opted out of out-of-hours some time ago, and they got a deal which was quite lucrative? Or is it because there are now anecdotal reports of GPs having to advise non-NHS care to their patients in the hope that they can jump a lengthy NHS queue? It is very hard to tell. But certainly it is true that GPs have become first in the firing line for the NHS reforms. They in fact opposed the reforms, with clear leadership by Prof Clare Gerada, Chair of the Royal College of General Practitioners. The Government PR went into overdrive that “GPs are at the heart of commissioning”, the ‘clinical commissioning groups’, but this was obviously never the intention. CCGs are merely a vehicle for holding funds and assessing risk in a pooled population, in a manner of ‘statutory insurance schemes’. This has always been the case, and always will be. For all the talk of ‘entrepreneurial GPs’, the public do not appear to warm to the idea of GPs as businessmen (and GPs do not particularly wish to represented as businessmen). Germane to this is the “dual agent” problem, very well known in insurance markets. That is the idea that no person can have “two masters”, without a significant conflict of interest: this might be for example a GP’s professional duty to his or her patient, and his or her duty to the people who ultimately provide the funding. This issue of trust is possibly bound to get worse, as ‘scandals’ are drip fed to the media of a system in distress. The reason this score is nothing to do with Prof Gerada is because Prof Gerada, as the new “NHS SOS” book explains (edited by Dr Jacky Davis and Prof Ray Tallis), was one of the few NHS leaders to have a clear vision and have the charisma to set this out in confidence, a textbook example of a “charismatic leader”, who deservedly was one of the hundred most influential individuals in health. And, very clearly, she appeared to be representing patients as well as GPs.
Anyone who wishes to defend the NHS is accused of protecting a ‘national religion’. And yet the NHS is accused of being ‘monolithic’, ‘inefficient’, ‘dangerous’, ‘expensive’, and every negative adjective under the sun. Politicians are responsible for this deprofessionalisation of key non-managerial workers in the NHS, with talk of ‘it doesn’t matter who provides my care as long as it is the…’ (a saying which in the legal and medical sectors has increasingly been completed with the word “cheapest”). Every conceivable thing is blamed for the pressures under which the NHS functions; such as the “burden of the ageing population” and the equally pathetic and untrue myth that high-quality healthcare is dependent on expensive equipment. Tell that to the cardiologist who can discern an early diastolic murmur with a pulmonary hypertensive ‘heave’ due to a crappy £20 stethoscope, not a £5000 portable digital echocardiogram machine. The number of lies in the drive to make the NHS attractive financially to outsourcers and privatisers has been breath-taking. In view of this, isn’t it time perhaps we either rate how Doctors are actually treated in the NHS, or time to turn the tables and rate our NHS management and politicians?
Blindness to the evidence-based change management advice from the NHS' own unit
Of course, the Government was free to consult any number of management consultancies about how to implement this complicated strategic change management. A recent ‘Mail on Sunday’ investigation based on hundreds of official documents disclosed under the Freedom of Information Act, has revealed the full extent of McKinsey’s links to the controversial Health and Social Care Bill. This newspaper alleges that many of the Bill’s proposals were drawn up by McKinsey, and outlines a number of other specific allegations. The irony is that the NHS has its own specialist unit which produces excellent advice about how to manage change in the NHS.
The NHS has in fact a specialist ‘Institute for Innovation and Improvement’. which is geared up to conduct change management throughout the NHS. Most independent experts feel that the way in which this strategic change has been implemented has been a disaster, and whoever advised on it does not appear to have acknowledged the advice from the NHS’ own change management unit as given on this webpage by Dr Helen Bevan. According to elsewhere on the website, “Helen has led change initiatives at local and national level which have created improvements for millions of patients. Her current role is to keep NHS improvement knowledge fresh, relevant, impactful at the leading edge.” It appears that the unit is heavily influenced by a paper from Harvard Business Review in October 2005 by Sirkin, Keenan and Jackson entitled, “The hard side of change management”.
Here are specific sections of Dr Bevan’s views on change management, and you can easily see why the NHS reforms will run into disaster.
The first factor is duration. An underpinning belief in many NHS change programmes is that we need to execute change quickly. Not necessarily so, say the authors. What really matters is having formal, senior management-led, review processes. A long project that is reviewed frequently and effectively is more likely to succeed than a short project that isn’t reviewed. The second factor is performance integrity. This means selecting the right mix of team members to deliver the change; the most results-orientated people with credibility and influence and effective change skills.
Today, a summit was held where a number of key stakeholders were not even invited. including the Royal College of General Practitioners, Royal College of Nurses, British Medical Association, Royal College of Psychiatrists, and the Faculty of Public Health. As Ben Goldacre has alluded to on his secondary blog, there appears to be a good correlation between those who were not invited to the emergency summit and called for the NHS Bill to be dropped. A recent headline in the Telegraph has provided, “Prime Minister David Cameron today insisted he was “committed” to pushing through the Government’s reforms to the NHS, as he met healthcare professionals in Downing Street.”
The next factor is commitment. The authors focus on two critical categories. There must be active, visible backing for the change from the most influential senior leaders. They say that if, as a senior leader, you feel you are talking up the change initiative at least three times as much as you need to, your organisation will feel you are backing the transformation. In addition, the change is unlikely to succeed if it is not enthusiastically supported by the people who will have to operate within the new structures and systems that it creates. Staff need to understand the reasons for the change and believe it is worthwhile.
This change does not have the backing of the majority of doctors and nurses, and there is absolutely no sense that the medical profession is backing this change. In fact, this BBC webpage gives details of who stands where on the change, and many professional bodies would like to “kill the bill”.
When an issue matters so much to the public, why has the Government accidentally or wilfully turned a blind eye to sound change management advice from its own unit?

