Home » Posts tagged 'prevention'
Tag Archives: prevention

The references for chapter 1 of my book on prevention/risk factors in dementia
These are the references to Chapter 1 “Introduction”, mainly an overview of English dementia policy, prevention and risk factors, for my new book, “Living better with dementia: championing change for the future” (to be published early 2014).
Websites
“Call to action: the use of antipsychotics for people with dementia” http://www.institute.nhs.uk/qipp/calls_to_action/Dementia_and_antipsychotic_drugs.html
A letter to the Prime Minister charting progress on the Prime Minister’s Dementia Challenge (dated 7th May 2014). https://s3-eu-west-1.amazonaws.com/media.dh.gov.uk/network/353/files/2014/05/10092-2902335-TSO-Dementia-Letter-to-PM-ACCESSIBLE.pdf
All Party Parliamentary Group (APPG) on dementia. (2012) Unlocking the diagnosis: the key to improving the lives of people with dementia http://www.alzheimers.org.uk/site/scripts/download_info.php?fileID=1457 (dated June)
Dementia 2013: The hidden voice of lonelineness http://www.alzheimers.org.uk/dementia2013
Dementia Roadmap. http://dementiaroadmap.info
Department of Health (2012) Prime Minister’s Dementia Challenge: delivering major improvements in dementia care and research by 2015 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/215101/dh_133176.pdf
Making a Difference in Dementia: Nursing Vision and Strategy https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/147956/Making_a_Difference_in_Dementia_Nursing_Vision_and_Strategy.pdf
Memory Services National Accreditation Programme (Royal College of Psychiatrists) http://www.rcpsych.ac.uk/workinpsychiatry/qualityimprovement/qualityandaccreditation/memoryservices/memoryservicesaccreditation.aspx
NHS Confederation website/NHS Voices blog. (2014) A people-centred response to the 2015 Challenge is vital for the future of health and care, says Jeremy Taylor, http://www.nhsconfed.org/blog/2014/06/a-people-centred-response-to-the-2015-challenge-is-vital-for-the-future-of-health-and-care
PM Challenge on dementia (Alzheimer’s Research UK) http://www.alzheimersresearchuk.org/news-detail/10688/PM-Challenge-on-Dementia-a-year-of-progress-and-new-promise-for-research/ (dated 15 May 2013)
Public Health England and UK Health Prevention First (2014). The Blackfriars Consensus on promoting brain health: reducing risks for dementia in the population http://nhfshare.heartforum.org.uk/RMAssets/Reports/Blackfriars%20consensus%20%20_V18.pdf (“Blackfriars Consensus Statement”)
Rahman, S. (2014) “It’s time we talked about ‘dementia friendly communities’” Living well with dementia blog, http://livingwelldementia.org/2014/03/25/its-time-we-talked-about-dementia-friendly-communities/ (25th March 2014).
Report on the prescribing of anti-psychotic drugs to people with dementia (author: Professor Banerjee) http://webarchive.nationalarchives.gov.uk/20130107105354/http:/www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_108303 (November 2009)
WHO (2013) [ed. Wilkinson, R., Marmot, M.] Social determinants of health: the solid facts. http://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf
Other references
Ahlskog, J.E., Geda, Y.E., Graff-Radford, N.R., Petersen, R.C. (2011) Physical exercise as a preventive or disease-modifying treatment of dementia and brain aging, Mayo Clin Proc, 86(9), pp. 876–84.
Albert, M.S., DeKosky, S.T., Dickson, D., Dubois, B., Feldman, H.H., Fox, N.C,., Gamst, A., Holtzman, D.M., Jagust, W.J., Petersen, R.C., Snyder, P.J., Carrillo, M.C., Thies, B., Phelps, C.H. (2011) The diagnosis of mild cognitive impairment due toAlzheimer’s disease: recommendations from the National Institute on Aging–Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease, Alzheimers Dement, 7, pp. 270–9.
Alzheimer’s Association Expert Advisory Workgroup on NAPA (2012) Workgroup on NAPA’s scientific agenda for a national initiative on Alzheimer’s disease, Alzheimer Dement, 8, pp. 357–361.
Bambra, C., Gibson, M., Sowden, A., Wright, K., Whitehead, M., Petticrew, M. (2010) Tackling the wider social determinants of health and health inequalities: evidence from systematic reviews, J Epidemiol Community Health, Apr, 64(4), pp. 284-91.
Barberger-Gateau, P., Raffaitin, C., Letenneur, L., Berr, C., Tzourio, C., Dartigues, J.F., Alpérovitch, A. (2007) Dietary patterns and risk of dementia: the Three-City cohort study. Neurology, Nov 13, 69(20), pp. 1921-30.
Bennett, D.A., Schneider, J.A., Tang, Y., Arnold, S.E., Wilson, R.S. (2006) The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: a longitudinal cohort study, Lancet Neurol, 5(5), pp. 406–12.
Beydoun, M.A., Beydoun, H.A., Wang, Y. (2008) Obesity and central obesity as risk factors for incident dementia and its subtypes: a systematic review and meta-analysis, Obes Rev, 9, pp. 204–218.
Biessels GJ. Capitalising on modifiable risk factors for Alzheimer’s disease. Lancet Neurol, Aug, 13(8), pp. 752-3.
Black, S.E., Patterson, C. Feightner, J. (2001) Preventing dementia, Canadian Journal of Neurology Science, 28 (Suppl 1), pp. S56–66.
Blackburn, D.J., Krishnan, K., Fox, L., Ballard, C., Burns, A., Ford, G.A., Mant, J., Passmore, P., Pocock, S., Reckless, J., Sprigg, N., Stewart, R., Wardlaw, J., Bath, P.M. (2013) Prevention of Decline in Cognition after Stroke Trial (PODCAST): a study protocol for a factorial randomised controlled trial of intensive versus guideline lowering of blood pressure and lipids, Trials, Nov 22, 14: 401.
Bond, J. (1992) The medicalization of dementia, Journal of Aging Studies, 6, 397–403.
Bowling, A. (2007) Aspirations for old age in the 21st century, what is successful aging? The International Journal of Aging and Human Development, 64, 263–297.
Boyle, P.A., Buchman, A.S., Wilson, R.S., Yu, L., Schneider, J.A., Bennett, D.A. (2012) Effect of purpose in life on the relation between Alzheimer disease pathologic changes on cognitive function in advanced age, Arch Gen Psychiatry, 69(5), pp. 499– 505.
Brodaty, H., Howarth, G., Mant, A., Kurle, S. (1994) General practice and dementia, A national survey of Australian GPs, Medical Journal of Australia, 160, 10–14.
Brooker, D., La Fontaine, J., Bray, J., Evans, S. (for the University of Worcester Association of Dementia Studies) (2013), Timely diagnosis of dementia: ALCOVE WP5 Task 1 and 2.
Brunet M. (2014) Targets for dementia diagnoses will lead to over-diagnosis, BMJ, 348:g2224.
Brunnström, H., Gustafson, L., Passant, U., Englund, E. (2009) Prevalence of dementia subtypes: a 30-year retrospective survey of neuropathological reports, Arch Gerontol Geriatr, Jul Aug, 49(1), pp. 146-9.
Buchman, A.S., Wilson, R.S., Bienias, J.L., Shah, R.C., Evans, D.A., Bennett, D.A. (2005) Change in body mass index and risk of incident Alzheimer disease, Neurology, 65, pp. 892–897.
Burns, A., Robert, P. (2009) The National Dementia strategy in England, BMJ, Mar 10, 338:b931.
Chang, M., Jonsson, P.V., Snaedal, J., Bjornsson, S., Saczynski, J.S., Aspelund, T., Eiriksdottir, G., Jonsdottir, M.K., Lopez, O.L., Harris, T.B., Gudnason, V., Launer, L.J. (2010) The effect of midlife physical activity on cognitive function among older adults: AGES—Reykjavik study, J Gerontol A Biol Sci Med Sci, 65(12), pp. 1369–74.
Cooper, C. (2013) G8 Dementia Summit: PM pledges to double funding for research by 2025, 11 December 2013, The Independent newspaper, http://www.independent.co.uk/life-style/health-and-families/health-news/g8-dementia-summit-pm-pledges-to-double-funding-for-research-by-2025-8996377.html
Crampton, J., Dean, J., Eley, R. (2012) Joseph Rowntree Foundation: Creating a dementia friendly York, http://www.jrf.org.uk/sites/files/jrf/dementia-communities-york-full.pdf.
Cunningham, E.L., Passmore, A.P. (2013) Drug development in dementia, Maturitas, 76(3), pp. 260-6.
Daviglus, M.L., Bell, C.C., Berrettini, W., Bowen, P.E., Connolly, E.S. Jr, Cox, N.J., Dunbar-Jacob, J.M., Granieri, E.C., Hunt, G., McGarry, K., Patel, D., Potosky, A.L., Sanders-Bush, E., Silberberg, D., Trevisan, M. (2010) National institutes of health state-of-the-science conference statement: preventing Alzheimer disease and cognitive decline, Annals of Internal Medicine, August 3, 153(3), pp. 176–81.
De Lepeliere, J., Wind, A., Iliffe, S., Moniz-Cook, E., Wilcock, J., Gonzalez, V., Derksen, E., Gianelli, M., Vernooij-Dassen, M. the Interdem Group. (2008). The primary care diagnosis of dementia in Europe: An analysis using multi-disciplinary, multi-national expert groups, Aging & Mental Health, 12(5), 568–576.
Desmond, D.W., Tatemichi, T.K., Paik, M., Stern, Y. (1993) Risk factors for cerebrovascular disease as correlates of cognitive function in a stroke free cohort, Archives of Neurology, 50, pp. 162–166.
Devi, G., Ottman, R., Tang, M., Marder, K., Stern, Y., Tycko, B., Mayeux, R. (1999) Influence of APOE genotype on familial aggregation of AD in an urban population, Neurology, 53: 789.
Devore, E.E., Grodstein, F., van Rooij, F.J., Hofman, A., Stampfer, M.J., Witteman, J.C., Breteler M.M. (2010) Dietary antioxidants and long-term risk of dementia, Arch Neurol, Jul, 67(7), pp. 819-25.
Downs, M., Turner, S., Iliffe, S., Bryans, M., Wilcock, J., Keady, J. (2003) Improving the response of primary care practitioners to people with dementia and their families: A randomised controlled trial of educational interventions. Final Report to the UK Alzheimer’s Society, Bradford: UK Alzheimer’s Society.
EClipSE Collaborative Members, Brayne, C., Ince, P.G., Keage, H.A., McKeith, I.G., Matthews, F.E., Polvikoski, T., Sulkava, R. (2010) Education, the brain and dementia: neuroprotection or compensation? Brain, Aug, 133(Pt 8), pp. 2210-6.
Gao, S., Hendrie, H. C., Hall, K. S, Hui, S. (1998) The relationships between age, sex, and the incidence of dementia and Alzheimer disease: a meta-analysis, Archives of General Psychiatry, 55, 809–815.
Gauthier, S., Leuzy, A., Racine, E., Rosa-Neto, P. (2013) Diagnosis and management of Alzheimer’s disease: past, present and future ethical issues, Prog Neurobiol, Nov. 110:102-13.
Gustafson, D.R., Backman, K., Waern, M., Ostling, S., Guo, X., Zandi, P., Mielke, M.M., Bengtsson, C., Skoog, I. (2009) Adiposity indicators and dementia over 32 years in Sweden. Neurology, 73, pp. 1559–1566.
Haase, H., Rink, L. (2009) Functional significance of zinc-related signaling pathways in immune cells, Annu Rev Nutr, 29, pp. 133–152.
Håkansson, K., Rovio, S., Helkala, E.L., Vilska, A.R., Winblad, B., Soininen, H., Nissinen, A., Mohammed, A.H., Kivipelto, M., .Soininen H., Nissinen, A., Mohammed, A.H., Kivipelto, M. Association between mid-life marital status and cognitive function in later life: population based cohort study, BMJ, 339:b2462.
Hansen, E.C., Hughes, C., Routley, G., Robinson, A.L. (2008) General practitioners’ experiences and understandings of diagnosing dementia: factors impacting on early diagnosis, Soc Sci Med, Dec, 67(11), pp. 1776-83.
Harvey, R.J., Rossor, M.N., Skelton-Robinson, M. (1998) Young onset dementia: epidemiology, clinical symptoms, family burden, support and outcome, London: Dementia Research Group.
Hofman, A., Ott, A., Breteler, M.M., Bots, M.L., Slooter, A.J., van Harskamp, F, van Duijn, C.N., Van Broeckhoven, C., Grobbee, D.E. (1997) Atherosclerosis, apolipoprotein E, and prevalence of dementia and Alzheimer’s disease in the Rotterdam Study, Lancet, 349, pp. 151–154
Holland, W. (2012) Competition or collaboration? A comparison of health services in the UK, Clinical Medicine, 10(5), pp. 431–3
Imtiaz, B., Tolppanen, A.M., Kivipelto, M., Soininen. H. (2014) Future directions in Alzheimer’s disease from risk factors to prevention, Biochem Pharmacol, Apr 15, 88(4), pp. 661-70.
Innes, A., Manthorpe, J. (2013) Developing theoretical understandings of dementia and their application to dementia care policy in the UK, Dementia (London), Nov, 12(6), pp. 682-96.
Ionicioiu, I., David, D., Szamosközi, S. (2014) A quantitative meta-analysis of the effectiveness of psychosocial interventions in dementia, Procedia – Social and Behavioral Sciences, 27, pp. 591 – 594.
Jenkins, C.R., Thien, F.C.K., Wheatley, J.R., Reddel, H.K. (2005) Traditional and patient-centred outcomes with three classes of asthma medication, European Respiratory Journal, 26(1), pp. 36-44.
Jiang, T., Yu, J.T., Tian, Y., Tan, L. (2013) Epidemiology and etiology of Alzheimer’s disease: from genetic to non-genetic factors, Curr Alzheimer Res, Oct, 10(8), pp. 852-67.
Johansson, L., Guo, X., Waern, M., Ostling, S., Gustafson, D., Bengtsson, C., Skoog, I. (2010) Midlife psychological stress and risk of dementia: a 35-year longitudinal population study. Brain, Aug, 133(Pt 8), pp. 2217-24.
Jorm, A.F., Jolley, D. (1998) The incidence of dementia: a meta-analysis, Neurology, 51, 728–33.
Kehne, J.H. (2007) The CRF1 receptor, a novel target for the treatment of depression, anxiety, and stress-related disorders, CNS Neurol Disord Drug Targets, 6, pp. 163–182.
Khachaturian, A.S., Meranus, D.H., Kukull, W.A., Khachaturian, Z.S. (2013) Big data, aging, and dementia: pathways for international harmonization on data sharing, Alzheimers Dement, 9 (5 Suppl), pp. S61-2.
Khachaturian, Z.S., Petersen, R.C., Snyder, P.J., Khachaturian, A.S., Aisen, P., de Leon, M., Greenberg, B.D., Kukull, W., Maruff, P., Sperling, R.A., Stern, Y., Touchon, J., Vellas, B., Andrieu, S., Weiner, M.W., Carrillo, M.C., Bain, LJ. (2011) Developing a global strategy to prevent Alzheimer’s disease: Leon Thal Symposium 2010, Alzheimers Dement, Mar, 7(2), pp. 127-32.
Kim, J.W., Lee, D.Y., Lee, B.C., Jung, M.H., Kim, H., Choi, Y.S., Choi, I.G. (2012) Alcohol and cognition in the elderly: a review, Psychiatry Investig, Mar, 9(1), pp. 8-16.
Kivipelto, M., Ngandu, T., Fratiglioni, L., Viitanen, M., Kareholt, I., Winblad, B., Helkala, E.L., Tuomilehto, J., Soininen, H., Nissinen, A. (2006) Obesity and vascular risk factors at midlife and the risk of dementia and Alzheimer disease, Arch Neurol, 62, pp. 1556–1560.
Kmietowicz, Z. (2012) Cameron launches challenge to end “national crisis” of poor dementia care, BMJ, 344, e2347.
Kmietowicz, Z. (2014) Recorded diagnosis of dementia in England increases by 62% since 2006, BMJ, 349, g4911.
Koch, T., Iliffe, S. (2011) Implementing the National Dementia Strategy in England: Evaluating innovative practices using a case study methodology, Dementia, 10(4) 487–498.
Kopelman, P.G., (2000) Obesity as a medical problem, Nature, 404, pp. 635–643.
Lautenschlager, N.T., Cupples, L.A., Rao, V.S., Auerbach, S.A., Becker, R., Burke, J., Chui, H., Duara, R., Foley, E.J., Glatt, S.L., Green, R.C., Jones, R., Karlinsky, H., Kukull, W.A., Kurz, A., Larson, E.B., Martelli, K., Sadovnick, A.D., Volicer, L., Waring, S.C., Growdon, J.H., Farrer, L.A. (1996) Risk of dementia among relatives of Alzheimer’s disease patients in the MIRAGE study: What is in store for the oldest old? Neurology, 46, pp. 641–50.
Leonard BE. (2006) HPA and immune axes in stress: involvement of the serotonergic system. Neuroimmunomodulation, 13, pp. 268–76.
Lieb, W., Beiser, A.S., Vasan, R.S., Tan, Z.S., Au, R., Harris, T.B., Roubenoff, R., Auerbach, S., De- Carli, C., Wolf, P.A., Seshadri, S. (2009) Association of plasma leptin levels with incident Alzheimer disease and MRI measures of brain aging, JAMA, 302, pp. 2565–2572.
Ligthart, S.A., Moll van Charante, E.P., van Gool, W.A., Richard, E. (2010) Treatment of cardio-vascular risk factors to prevent cognitive decline and dementia: a systematic revie, Vascular Health & Risk Management, (6), pp. 775–85.
Lincoln, P., Fenton, K., Alessi, C., Prince, M., Brayne, C., Wortmann, M., Patel, K., Deanfield, J., Mwatsama, M. (2014) The Blackfriars Consensus on brain health and dementia, Lancet, May 24, 383(9931), pp. 1805-6.
Lindsay, J., Hebert, R.Rockwood, K. (1997) The Canadian Study of Health and Aging – Risk Factors for Vascular Dementia, Stroke, 28, 526–530.
Lupton, D. (1999) Risk. London: Routledge.
Lyman, K. A. (1989) Bringing the social back in: a critique of the bio-medicalisation of dementia, Gerontologist, 29, pp. 597–604.
Masi, C.M., Chen, H.Y., Hawkley, L.C., Cacioppo, J.T. (2011) A meta-analysis of interventions to reduce loneliness, Pers Soc Psychol Rev, Aug, pp. 15(3):219-66.
McCullagh, C.D., Craig, D., Mollroy, S.P., Passmore, A.P. (2001) Risk factors for dementia, Advances in Psychiatric Treatment, 7, pp. 24-31.
McKhann, G.M, Knopman, D.S., Chertkow, H., Hyman, B.T., Jack, C.R. Jr, Kawas, C.H., Klunk, W.E., Koroshetz, W.J., Manly, J.J., Mayeux, R., Mohs, R.C., Morris, J.C., Rossor, M.N., Scheltens, P., Carrillo, M.C., Thies, B., Weintraub, S., Phelps, C.H. (2011) The diagnosis of dementia due to Alzheimer’s disease: recommendations from the National Institute on Aging–Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease, Alzheimers Dement, 7, pp. 263–9.
Milne, A. (2010) Dementia screening and early diagnosis: The case for and against, Health, Risk & Society, 12(1), pp. 65–76.
Mizutani, K., Nishimura, K., Ichihara, A., Ishigooka, J. (2014) Dissociative disorder due to Graves’ hyperthyroidism: a case report, Gen Hosp Psychiatry, Mar 19. pii: S0163 8343(14)00073-5.
Monastero, R., Mangialasche, F., Camarda, C., Ercolani, S., Camarda, R. (2009) A systematic review of neuropsychiatric symptoms in mild cognitive impairment, J Alzheimers Dis, 18(1), pp. 11–30.
Moroney, J.T., Tang, M.X., Berglund, L., Small, S., Merchant, C., Bell, K., Stern, Y., Mayeux, R. (1999) Low density lipoprotein cholesterol and the risk of dementia with stroke, Journal of the American Medical Association, 282, pp. 254–260.
Morris, J.C. (2005) Early-stage and preclinical Alzheimer disease, Alzheimer Dis Assoc Disord, 19, pp. 163–5.
Morris, M.C., Evans, D.A., Bienias, J.L., Tangney, C.C., Bennett, D.A, Aggarwal, N., Schneider, J., Wilson, R.S. (2003) Dietary fats and the risk of incident Alzheimer disease, Arch Neurol, 60(2), pp. 194-200. [Erratum in: Arch Neurol. 2003 Aug;60(8):1072.]
National Audit Office (2007) Improving services and support for people with dementia, London: The Stationary Office.
Ngandu, T., Helkala, E.L., Soininen, H., Winblad, B., Tuomilehto, J., Nissinen, A., Kivipelto, M. (2007) Alcohol drinking and cognitive functions: findings from the Cardiovascular Risk Factors Aging and Dementia (CAIDE) Study, Dement Geriatr Cogn Disord, 23(3), pp. 140-9.
Ngandu, T., von Strauss, E., Helkala, E.L., Winblad, B., Nissinen, A., Tuomilehto, J., Soininen, H., Kivipelto, M. (2007) Education and dementia: what lies behind the association? Neurology, Oct 2, 69(14), pp. 1442-50.
Norton, S., Matthews, F.E., Barnes, D.E., Yaffe, K., Brayne, C. (2014) Potential for primary prevention of Alzheimer’s disease: an analysis of population-based data, Lancet Neurol, Aug, 13(8), pp. 788-94.
Panza, F., Frisardi, V., Seripa, D., Logroscino, G., Santamato, A., Imbimbo, B.P., Scafato, E., Pilotto, A., Solfrizzi, V. (2012) Alcohol consumption in mild cognitive impairment and dementia: harmful or neuroprotective? Int J Geriatr Psychiatry, Dec, 27(12):1218-38.
Peters, R. (2012) Blood pressure, smoking and alcohol use, association with vascular dementia. Exp Gerontol, Nov, 47(11), pp. 865-72.
Piazza-Gardner, A.K., Gaffud, T.J., Barry, A.E. (2013) The impact of alcohol on Alzheimer’s disease: a systematic review, Aging Ment Health, 17(2), pp. 133–46.
Prasad, A.S. (2009) Impact of the discovery of human zinc deficiency on health, J Am Coll Nutr, 28, pp. 257–265.
Prasad, A.S. (2003) Zinc deficiency, BMJ, 326, pp. 409–410.
Ratnavalli E, Brayne C, Dawson K, et al. (2002) The prevalence of frontotemporal dementia. Neurology, 58:1615–21.
Redman, R.W., Lynn, M.R. (2004) Advancing patient-centred care through knowledge development, Canadian Journal of Nursing Research, 36(3), pp. 116-129.
Rissman, R.A., Staup, M.A., Lee, A.R., Justice, N.J., Rice, K.C., Vale, W., Sawchenko, P.E. Corticotropin releasing factor receptor-dependent effects of repeated stress on tau phosphorylation, solubility, and aggregation, Proc Natl Acad Sci USA, Apr 17, pp. 109(16):6277-82.
Ritchie, C.W., Ritchie, K. (2012) The PREVENT study: a prospective cohort study to identify mid-life biomarkers of late-onset Alzheimer’s disease, BMJ Open, Nov 19, pp. 2(6).
Rusanen, M., Rovio, S., Ngandu, T., Nissinen, A., Tuomilehto, J., Soininen, H., Kivipelto, M. (2010) Midlife smoking, apolipoprotein E and risk of dementia and Alzheimer’s disease: a population-based cardiovascular risk factors, aging and dementia study. Dement Geriatr Cogn Disord, 30(3), pp. 277-84.
Saleem, A., Sophia, R. (2014) Voltage-gated potassium channel antibody-associated limbic encephalitis, Age Ageing, Jul, 43(4), pp. 583-5.
Sapolsky, R.M. (1996) Why stress is bad for your brain, Science, 273, pp. 749–50.
Scarmeas, N., Stern, Y., Tang, M.X., Mayeux, R., Luchsinger, J.A. (2006) Mediterranean diet and risk for Alzheimer’s disease, Ann Neurol, Jun, 59(6), pp. 912-21.
Schliebs, R., Arendt, T. (2011) The cholinergic system in aging and neuronal degeneration, Behav Brain Res, Aug 10, 221(2), pp. 555-63.
Skoog, I., Kalaria, R.N., Breteler, M.M. (1999) Vascular factors and Alzheimer disease, Alzheimer Dis Assoc Disord, 13(suppl 3), pp. S106–S114
ofi, F., Valecchi, D., Bacci D., Abbate, R., Gensini, G.F., Casini, A., Macchi, C. (2011) Physical activity and risk of cognitive decline: a meta-analysis of prospective studies, J Intern Med, 269(1), pp. 107–17.
Sperling, R.A., Rentz, D.M., Johnson, K.A., Karlawish, J., Donohue, M., Salmon, D.P., Aisen, P. (2014) The A4 study: stopping AD before symptoms begin? Sci Transl Med, Mar 19, 6(228), pp. 228fs13.
Stern, Y., Gurland, B., Tatemichi, T.K., Tang, M.X., Wilder, D., Mayeux, R. (1994) Influence of education and occupation on the incidence of Alzheimer’s disease, JAMA, 271(13), pp. 1004–10.
Szewczyk, B. (2013) Zinc homeostasis and neurodegenerative disorders. Front Aging Neurosci, Jul 19, 5:33.
Tischler V, D’Silva K, Cheetham A, Goring M, Calton T. Involving patients in research: the challenge of patient-centredness, Int J Soc Psychiatry, 2010 Nov, 56(6), pp. 623-33
Tyas, S.L., White, L.R., Petrovitch, H., Webster Ross, G., Foley, D.J., Heimovitz, H.K., Launer, L.J. (2003) Mid-life smoking and late-life dementia: the Honolulu-Asia aging study, Neurobiol Aging, 24(4), pp. 589–96.
van der Linde, R.M., Stephan, B.C., Matthews, F.E., Brayne, C., Savva, G.M. (2013) Medical Research Council Cognitive Function and Ageing Study. The presence of behavioural and psychological symptoms and progression to dementia in the cognitively impaired older population, Int J Geriatr Psychiatry, Jul;28(7):700-9.
van Duijn, C.M., Hendriks, L., Cruts, M., Hardy, J.A., Hofman, A. (1991) Amyloid precursor protein gene mutation in early-onset Alzheimer’s disease, Lancet, 337(8747): 978.
Vellas, B., Gillette-Guyonnet, S., Andrieu, S. (2008) Memory health clinics-a first step to prevention, Alzheimers Dement, Jan, 4(1 Suppl 1):S144-9.
van El, C.G., Cornel, M.C., Borry, P., Hastings, R.J., Fellmann, F., Hodgson, S.V., Howard, H.C., Cambon-Thomsen, A., Knoppers, B.M., Meijers-Heijboer, H., Scheffer, H., Tranebjaerg, L., Dondorp, W., de Wert, GM, ESHG Public and Professional Policy Committee. (2013) Whole-genome sequencing in health care: recommendations of the European Society of Human Genetics, Eur J Hum Genet, Jun;21(6):580-4.
Verity, C.M., Nicoll, A., Will, R.G., Devereux, G., Stellitano, L. (2000) Variant Creutzfeldt-Jakob disease in UK children: a national surveillance study, Lancet, Oct 7, 356(9237), pp. 1224-7.
Victor, M., Adams, R.D., Collins, G.H. (1971) The Wernicke–Korsakoff syndrome. F.A. Davis.
Vileland, T. (2002) Managing chronic disease: evidence-based medicine or patient-centred medicine? Health Care Analysis, 10(3), pp. 289-98.
Wang, H.X., Gustafson, D.R., Kivipelto, M., Pedersen, N.L., Skoog, I., Windblad, B., Fratiglioni, L. (2012) Education halves the risk of dementia due to apolipoprotein ?4 allele: a collaborative study from the Swedish brain power initiative, Neurobiol Aging, 33(5). 1007.e1-7.
Warren, M.W., Hynan, L.S., Weiner, M.F. (2012) Lipids and adipokines as risk factors for Alzheimer’s disease, J Alzheimers Dis, 29, pp. 151–157.
WHO (Revised February 2012) Variant Creutzfeldt-Jakob disease: factsheet no 180, available at http://www.who.int/mediacentre/factsheets/fs180/en/ [accessed 12 June 2014].
Wilson, R.S., Scherr, P.A., Schneider, J.A., Tang, Y., Bennett, D.A. (2007) Relation of cognitive activity to risk of developing Alzheimer disease, Neurology, 69(20), pp. 1911–20.
Wise J. (2014) £90m package to improve dementia care is announced in England, BMJ, 348, g1879.
Zecca, L., Youdim, M.B., Riederer, P., Connor, J.R., Crichton, R.R. (2004) Iron, brain ageing and neurodegenerative disorders, Nat Rev Neurosci, 5, pp. 863–873.
Source of the graphic in the top left corner of this page is here.

‘Reasons to be cheerful’ part 4. Prof Sube Banerjee’s inaugural lecture in Brighton on living well with dementia.
For me the talk was like a badly needed holiday. I joked with Kay there, a colleague of Lisa, that it felt like a (happy) wedding reception.
@charbhardy hello Chars – not at all the same without you. Thinking of you and G. Very windy on seafront here at Brighton x
— shibley (@legalaware) February 27, 2014
Unknown to me, the title of Prof Banerjee’s talk is an allusion to this famous track from 1979 (when I was five). It’s “Reasons to be cheerful (part 3)” by Ian Drury and the Blockheads.
The Inaugural Lecture – Professor Sube Banerjee (“Professor of Dementia”), ‘Dementia: Reasons to be cheerful’ was held on 26 February, 2014, 6:30 pm – 8:30 pm, at Chowen Lecture Theatre, Brighton and Sussex Medical School, Sussex Campus. BN1 9PX. Details are here on the BSMS website.
I found Prof Banerjee to be a very engaging, ‘natural’ speaker.
I arrived with hours to spare, like how the late Baroness Thatcher was alleged to have done in turning up for funerals.

Brighton are very lucky to have him.
But his lecture was stellar – very humble, yet given with huge gravitas. Banerjee is one of the best lecturers of any academic rank in dementia I have ever seen in person.

Banerjee started off with a suitable ‘icebreaker’ joke – but the audience wasn’t at all nervous, as they all immediately warmed to him very much.

He is ‘quite a catch’. He is able to explain the complicated issues about English dementia policy in a way that is both accurate and engaging. Also, I have every confidence in his ability to attract further research funding for his various teaching and clinical initiatives in dementia for the future.
Most of all, I was particularly pleased as the narrative which he gave of English dementia policy, with regards to wellbeing, was not only accurate, but also achievable yet ambitious.
1979 was of course a big year.

Prof Banerjee felt there were in fact many ‘reasons to be cheerful’, since Ian Drury’s remarkable track of 1979 (above), apparently issued on 20 July of that year.
Banerjee argued that the 1970s which had only given fruit to 209 papers, but things had improved ever since then.
It was the year of course Margaret Thatcher came to power on behalf of the Conservative Party.

In contrast, there have already been thousands of papers in the 2000s so far.
Banerjee also argued that “what we know is more likely to be true” which is possibly also true. However, I immediately reminisced of the famous paper in Science in 1982, “The cholinergic hypothesis of geriatric memory dysfunction”. This paper, many feel, lay the groundwork for the development of cholinesterase inhibitors such as donepezil (“Aricept”, fewer than twenty years later.
It is definitely true that ‘we are better at delineating the different forms of dementia’.
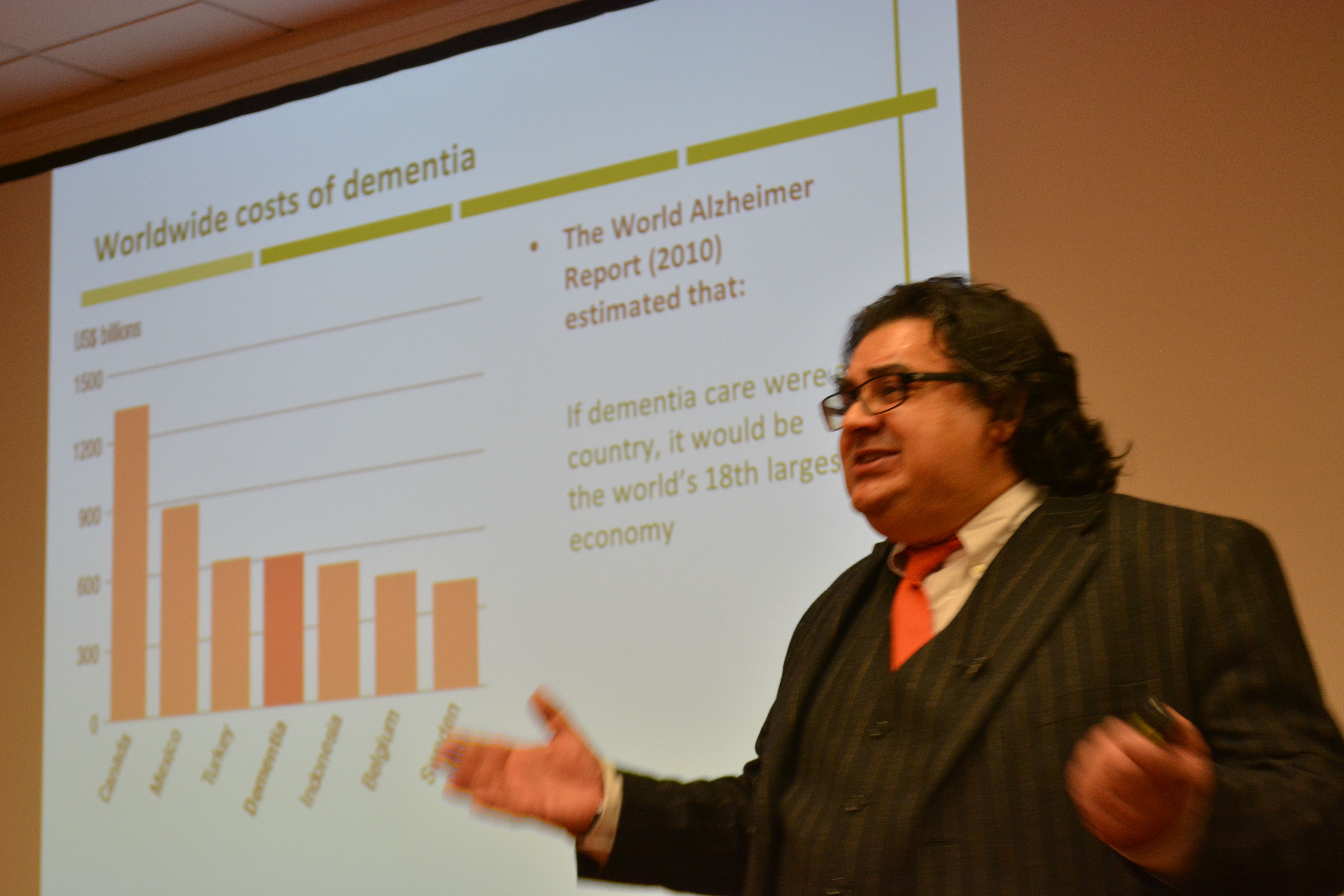
I prefer to talk of the value of people with dementia, but Banerjee presented the usual patter about the economic costs of dementia. Such stats almost invariably make it onto formal grant applications to do with dementia, to set the scene of this particular societal challenge.
I am of course a strong believer in this as my own PhD was in a new way to diagnose the behavioural variant of frontotemporal dementia. In this dementia, affecting mainly people in their 50s at onset, the behavioural and personality change noticed by friends and carers is quite marked. This is in contrast to a relative lack of memory of problems.
Not all dementias present with memory problems, and not all memory problems have a dementia as a root cause. I do happen to believe that this is still a major faultline in English dementia policy, which has repercussions of course for campaigns about ‘dementia awareness’.
A major drive in the national campaigns for England is targeted at destigmating persons with dementia, so that they are not subject to discrimination or prejudice.
The dementia friendship programmes have been particularly successful, and Banerjee correctly explained the global nature of the history of this initiative drive (from its “befriending” routes in Japan). Banerjee also gave an excellent example to do with language of dementia friendship in the elderly, which I had completely missed.

Raising awareness of memory problems in dementia is though phenomenally important, as Alzheimer’s disease is currently thought to be the most prevalent form of dementia worldwide.
The prevalence of dementia may even have been falling in England in the last few decades to the success prevention of cardiovascular disease in primary care.
The interesting epidemiological question is whether this should have happened anyway. Anyway, it is certainly good news for the vascular dementias potentially.
That dementia is more than simply a global public health matter is self-evident.
I’m extremely happy Banerjee made reference to a document WHO/Alzheimers Disease International have given me permission to quote in my own book.

Banerjee presented a slide on the phenomenally successful public awareness campaign about memory.

Nonetheless, Banerjee did speak later passionately about the development of the Croydon memory services model for improving quality of life for persons with mild to moderate dementia.
In developing his narrative about ‘living well with dementia’, Banerjee acknowledged at the outset that the person is what matters at dementia. He specifically said it’s about what a person can do rather than what he cannot do, which is in keeping to my entire philosophy about living well with dementia.
And how do we know if what we’re doing is of any help? Banerjee has been instrumental in producing, with his research teams, acceptable and validated methods for measuring quality of life in dementia.
The DEMQOL work has been extremely helpful here, and I’m happy Banerjee made a point of signposting this interesting area of ongoing practice-oriented research work.
Banerjee of course did refer to “the usual suspects” – i.e. things you would have expected him to have spoken about, such as the National Dementia Strategy (2009) which he was instrumental in designing at the time: this strategy was called “Living well with dementia”.

“I’m showing you this slide BECAUSE I want YOU to realise it IS complicated”, mused Banerjee at the objectives of the current English dementia policy.

I asked Banerjee what he felt the appropriate ‘ingredients’ of the new strategy for dementia might be – how he would reconcile the balance between ‘cure’ and ‘care’ – “and of course, the answer is both”, he said to me wryly.
Banerjee acknowledged, which I was massively pleased about, the current ‘barriers to care’ in this jurisdiction (including the known issues about the “timely diagnosis of dementia”.
Clearly the provision at the acute end of dementia care is going to have to come under greater scrutiny.

I increasingly have felt distinctly underwhelmed by the “medical model”, and in particular the repercussions of this medicalisation of dementia as to how grassroots supporters attempt to raise monies for dementia.
That certain antidepressants can have a lack of effect in dementia – Banerjee’s work – worries me.
That antipsychotics can have a dangerous and destructive effect for persons with dementia – also Banerjee’s work – also clearly worries me.
I am of course very proud that Prof Alistair Burns is currently reading my book focused on the interaction between the person and the environment in dementia.
And of course I’m ecstatic that Lisa Rodrigues and Prof Sube Banerjee signed my book : a real honour for me.

I signed Lisa’s book which was most likely not as exciting for her! X
Tour de force #ProfSubeBanerjee inaugural lecture made extra special by presence of @legalaware #reasonstobecheerful pic.twitter.com/qRpWReZOt0
— Lisa Rodrigues (@LisaSaysThis) February 26, 2014
There was a great atmosphere afterwards: the little chocolate brownies were outstanding!
Being an antisocial bastard, I didn’t mingle.

BUT I had a brilliant chat with Lucy Jane Marsters (@lucyjmarsters) who gave me a little bag of ‘Dementia is my business’ badges, very thoughtfully.

We both spoke about Charmaine Hardy. Charmaine was missed (and was at home, devoted to G.)
I’ve always felt that Charmaine is a top member of our community.
@legalaware oh Shibley how did you enjoy it? I wish I could have been there but it’s not possible to leave G anymore. Good being by the sea.
— Charmaine Hardy (@charbhardy) February 27, 2014
This apparently is a ‘Delphinium’.

A reason not to be cheerful was leaving Brighton, for many personal reasons for me.

Not even the Shard was a ‘reason to be cheerful’, particularly.

@legalaware @lucyjmarsters Come back soon, missing you already!!!
— Lisa Rodrigues (@LisaSaysThis) February 27, 2014
But when I came back, I found out that ‘Living well with dementia’ is to be a core part of the new English dementia policy.
Good to see ‘Living well with dementia’ will be a core part of England’s new dementia strategy 14-19 http://t.co/4rknTTzvl9 @nursingtimesed
— Living Well Dementia (@dementia_2014) February 27, 2014
I have, of course, just published a whole book about it.
The photograph of the poppy was of course taken by Charmaine Hardy: I have such great feedback on that one poppy in particular!

And what does the future hold?
Over to Prof Banerjee…

Is prevention of dementia merely a pipe dream?

Predicting the future on the basis of your past is of course the ultimate goal of the shopping industry.
It also seems to be the goal of healthcare, as consumer behaviour and patient care appear to converge in ever-marketised healthcare.
When you ‘sign up’ for a health subscription somewhere, one day, it’s possible you’ll be offered “packages” most suitable for you. Consider them like targetted adverts on Facebook. Of course, with disease registries compiled on your behalf by public health through data sharing, tomorrow’s world is getting ever closer.
So how much of dementia is in your ‘control’, if you haven’t yet developed it?
Is prevention of dementia a pipe dream? There are, after all, many factors which we’re born with which can have a huge influence. These are known as generic factors.
Amazon, the world’s largest online retailer, is already testing unmanned drones to deliver goods to customers. The drones, called Octocopters, could deliver packages weighing up to 2.3kg to customers within 30 minutes of them placing the order. Amazon has filed a patent that will allow it to ship a package to you before you even know you’ve bought it.
To give you another example, I know someone who was being given sponsored ads for hotels in Bilboa after Facebook had picked up her location by GPS.
Now back to the past.
Back to Black in fact.
The Black report was a 1980 document published by the Department of Health and Social Security (now the Department of Health) in the United Kingdom, which was the report of the expert committee into health inequality chaired by Sir Douglas Black. It was demonstrated that although overall health had improved since the introduction of the welfare state, there were widespread health inequalities.
Full Text of the Black Report, supplied by the Socialist Health Association website.
Surprisingly enough, it’s not all doom and gloom.
Modulating the environment might have some sort of impact on prevention of dementia, even if we don’t yet know how big or small this impact is.
The study of exceptionally long-living individuals can inform us about the determinants of successful aging. There have been few population-based studies of centenarians and near-centenarians internationally. But a recent study involving individuals 95 years and older were recruited from seven electoral districts in Sydney provided evidence that dementia is not “inevitable” at this age and independent living is common.
Low socioeconomic status in early life is well known to affect growth and development, including that of the brain; and it has also been shown to affect the risks of other chronic diseases.
Over a decade ago, a real attempt was made to relate early socioeconomic status to later dementia. We found results consistent with the hypothesis that a healthier socioeconomic environment in childhood and adolescence leads to more “brain reserve” (the brain’s ability to cope with increasing age- and disease-related changes while still functioning) and less risk of late-life dementia, including Alzheimer’s disease, later on.
Results from two major cohort studies, led by the University of Cambridge and supported by the Medical Research Council, have reveal that the number of people with dementia in the UK is substantially lower than expected because overall prevalence in the 65 and over age group has dropped.
Three geographical areas in Newcastle, Nottingham and Cambridgeshire from the initial MRC Cognitive Function and Ageing Study (CFAS) examined levels of dementia in the population. The latest figures from the follow up study, CFAS II, show that there is variation in the proportion of people with dementia across differing areas of deprivation, suggesting that health inequalities during life may influence a person’s likelihood of developing dementia.
The prevalence of dementia in the general population might be subject to change.
Factors that might increase prevalence include: rising prevalence of risk factors, such as physical inactivity, obesity, and diabetes; increasing numbers of individuals living beyond 80 years with a shift in distribution of age at death; persistent inequalities in health across the lifecourse; and increased survival after stroke and with heart disease.
By contrast, factors that might decrease prevalence include successful primary prevention of heart disease, accounting for half the substantial decrease in vascular mortality, and increased early life education, which is associated with reduced risk of dementia.
The study was led by Professor Carol Brayne from the Cambridge Institute of Public Health at Cambridge University. She opined that whether or not these gains for the current older population will be borne out in later generations might depend on whether further improvements in primary prevention and effective health care for conditions which increase dementia risk can be achieved, including addressing inequalities.
In fact, it has been recently appreciated that cardio-metabolic risk factors have been associated with poor physical and mental health.
An association of low education with an increased risk of dementia including Alzheimer’s Disease, the most common cause of dementia globally, has been reported in numerous cross-sectional and longitudinal studies. Education and socioeconomic status are highly correlated, it turns out.
The reserve hypothesis has been proposed to interpret this association such that education could enhance neural and cognitive reserve that may provide compensatory mechanisms to cope with degenerative pathological changes in the brain, and therefore delay onset of the dementia syndrome.
The complexity of people’s occupations also positively influences cognitive vitality, and this relationship becomes increasingly marked with age.
Further evidence from studies suggests that a poor social network or social disengagement is associated with cognitive decline and dementia.
The risk for dementia including Alzheimer’s Disease was also increased in older people with increasing social isolation and less frequent and unsatisfactory contacts with relatives and friends. Rich social networks and high social engagement imply better social support, leading to better access to resources and material goods.
Previous studies have also shown that social determinants not directly involved in the disease process may be implicated in the timing of dementia diagnosis. Possibly the living situation is related to the severity of dementia at diagnosis. If so, primary care providers should have a low threshold for case-finding in older adults who live with family or friends?
Regular physical exercise was reported to be associated with a delay in onset of dementia including Alzheimer’s Disease among cognitively healthy elderly.
In the Kungsholmen Project, the component of physical activity presenting in various leisure activities, rather than sports and any specific physical exercise, was related to a decreased dementia risk. It is generally thought that physical activity is important not only in promoting general and vascular health, but also in promoting some form of brain rewiring.
Various types of mentally demanding activities have been examined in relation to dementia in general, including knitting, gardening, dancing, playing board games and musical instruments, reading, social and cultural activities, and watching specific television programs, which often showed a protective effect.
So it really might not all the doom and gloom, and certainly we are much further forward than we were 33 years ago with the publication of “The Black Report”.
For the record, this Report doesn’t even mention dementia.
Prof Alistair Burns in New Scientist writing “Dementia: A silver lining but no room for complacency” summarised elegantly the situation as follows, on 10 January 2014:
“While it is true that there is no cure, the findings suggest that prevention is at least possible. This must surely explain any reduction in prevalence, so what might be behind it? Improved cardiovascular health, better diet and higher educational achievement are all plausible explanations. This opens up the possibility that people who are able to take control of their lives can reduce their individual risk of dementia.”
So, to answer the actual question.
There is a realistic possibility that we might be able to identify certain people who are most at risk of developing a dementia, and modifying the known risk factors constitutes ‘low hanging fruit’ for policy. If you park aside the corporate capture potential of making new markets through development of health promotion packages, this is indeed an example, shock horror, of where data sharing across the whole population might be helpful and direct the health of the nation in future.
Is prevention of dementia a pipe dream?

Predicting the future on the basis of your past is of course the ultimate goal of the shopping industry.
It also seems to be the goal of healthcare, as consumer behaviour and patient care appear to converge in ever-marketised healthcare.
When you ‘sign up’ for a health subscription somewhere, one day, it’s possible you’ll be offered “packages” most suitable for you. Consider them like targetted adverts on Facebook. Of course, with disease registries compiled on your behalf by public health through data sharing, tomorrow’s world is getting ever closer.
So how much of dementia is in your ‘control’, if you haven’t yet developed it?
Is prevention of dementia a pipe dream? There are, after all, many factors which we’re born with which can have a huge influence. These are known as generic factors.
Amazon, the world’s largest online retailer, is already testing unmanned drones to deliver goods to customers. The drones, called Octocopters, could deliver packages weighing up to 2.3kg to customers within 30 minutes of them placing the order. Amazon has filed a patent that will allow it to ship a package to you before you even know you’ve bought it.
Now back to the past. Back to Black in fact.
The Black report was a 1980 document published by the Department of Health and Social Security (now the Department of Health) in the United Kingdom, which was the report of the expert committee into health inequality chaired by Sir Douglas Black. It was demonstrated that although overall health had improved since the introduction of the welfare state, there were widespread health inequalities.
Full Text of the Black Report, supplied by the Socialist Health Association website.
Surprisingly enough, it’s not all doom and gloom.
Modulating the environment might have some sort of impact on prevention of dementia, even if we don’t yet know how big or small this impact is.
The study of exceptionally long-living individuals can inform us about the determinants of successful aging. There have been few population-based studies of centenarians and near-centenarians internationally. But a recent study involving individuals 95 years and older were recruited from seven electoral districts in Sydney provided evidence that dementia is not “inevitable” at this age and independent living is common.
Low socioeconomic status in early life is well known to affect growth and development, including that of the brain; and it has also been shown to affect the risks of other chronic diseases.
Over a decade ago, a real attempt was made to relate early socioeconomic status to later dementia. We found results consistent with the hypothesis that a healthier socioeconomic environment in childhood and adolescence leads to more “brain reserve” (the brain’s ability to cope with increasing age- and disease-related changes while still functioning) and less risk of late-life dementia, including Alzheimer’s disease, later on.
Results from two major cohort studies, led by the University of Cambridge and supported by the Medical Research Council, have reveal that the number of people with dementia in the UK is substantially lower than expected because overall prevalence in the 65 and over age group has dropped.
Three geographical areas in Newcastle, Nottingham and Cambridgeshire from the initial MRC Cognitive Function and Ageing Study (CFAS) examined levels of dementia in the population. The latest figures from the follow up study, CFAS II, show that there is variation in the proportion of people with dementia across differing areas of deprivation, suggesting that health inequalities during life may influence a person’s likelihood of developing dementia.
The prevalence of dementia in the general population might be subject to change. Factors that might increase prevalence include: rising prevalence of risk factors, such as physical inactivity, obesity, and diabetes; increasing numbers of individuals living beyond 80 years with a shift in distribution of age at death; persistent inequalities in health across the lifecourse; and increased survival after stroke and with heart disease.
By contrast, factors that might decrease prevalence include successful primary prevention of heart disease, accounting for half the substantial decrease in vascular mortality, and increased early life education, which is associated with reduced risk of dementia.
The study was led by Professor Carol Brayne from the Cambridge Institute of Public Health at Cambridge University. She opined that whether or not these gains for the current older population will be borne out in later generations might depend on whether further improvements in primary prevention and effective health care for conditions which increase dementia risk can be achieved, including addressing inequalities.
In fact, it has been recently appreciated that cardio-metabolic risk factors have been associated with poor physical and mental health.
An association of low education with an increased risk of dementia including Alzheimer’s Disease, the most common cause of dementia globally, has been reported in numerous cross-sectional and longitudinal studies. Education and socioeconomic status are highly correlated, it turns out.
The reserve hypothesis has been proposed to interpret this association such that education could enhance neural and cognitive reserve that may provide compensatory mechanisms to cope with degenerative pathological changes in the brain, and therefore delay onset of the dementia syndrome.
The complexity of people’s occupations also positively influences cognitive vitality, and this relationship becomes increasingly marked with age.
Further evidence from studies suggests that a poor social network or social disengagement is associated with cognitive decline and dementia.
The risk for dementia including Alzheimer’s Disease was also increased in older people with increasing social isolation and less frequent and unsatisfactory contacts with relatives and friends. Rich social networks and high social engagement imply better social support, leading to better access to resources and material goods.
Previous studies have also shown that social determinants not directly involved in the disease process may be implicated in the timing of dementia diagnosis. Possibly the living situation is related to the severity of dementia at diagnosis. If so, primary care providers should have a low threshold for case-finding in older adults who live with family or friends?
Regular physical exercise was reported to be associated with a delay in onset of dementia including Alzheimer’s Disease among cognitively healthy elderly.
In the Kungsholmen Project, the component of physical activity presenting in various leisure activities, rather than sports and any specific physical exercise, was related to a decreased dementia risk. It is generally thought that physical activity is important not only in promoting general and vascular health, but also in promoting some form of brain rewiring.
Various types of mentally demanding activities have been examined in relation to dementia in general, including knitting, gardening, dancing, playing board games and musical instruments, reading, social and cultural activities, and watching specific television programs, which often showed a protective effect.
So it really might not all the doom and gloom, and certainly we are much further forward than we were 33 years ago with the publication of “The Black Report”.
For the record, this Report doesn’t even mention dementia.
Prof Alistair Burns in New Scientist writing “Dementia: A silver lining but no room for complacency” summarised elegantly the situation as follows, on 10 January 2014:
“While it is true that there is no cure, the findings suggest that prevention is at least possible. This must surely explain any reduction in prevalence, so what might be behind it? Improved cardiovascular health, better diet and higher educational achievement are all plausible explanations. This opens up the possibility that people who are able to take control of their lives can reduce their individual risk of dementia.”
