Home » Posts tagged 'neuroimaging'
Tag Archives: neuroimaging

My personal view of the importance of high quality #research in dementia for the #G8summit
I have a foot in both research camps.
I believe in good quality research about the ‘medicine’ of dementia.
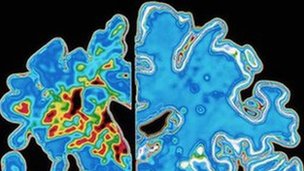
In the world of research, I am known to have contributed an original paper in the diagnosis of the frontal-variant of frontotemporal dementia.
This paper explained why people with a dementia could even end up having a diagnosis of this type of dementia, even though presenting in clinic with normal blood tests, psychological tests or brain scans.
Such patients did, however, have profound changes in behaviour and personality noticed by their closest ones, usually friends and family.
The paper itself has been quoted in the current Oxford Textbook of Medicine chapter reviewing the most common types of dementia, their diagnosis and management.
I do however have academic views on the importance of the ‘timely’ correct diagnosis of dementia, rather than early diagnosis.
I never give advice about anything on Twitter, as I am not a physician, but it is nice when what you say has an impact on general education of people about dementia.
I can be found on both @dementia_2014 and my other Twitter account (as I am trained in academic law as well as research in dementia) @legalaware.
Take for example how depression can be in the wrong hands misdiagnosed as dementia.

This is an example, perhaps, of where a diagnosis is a label, and disabling not enabling.
But for very many a correct diagnosis of a type of dementia will be a key to the door for opening up the relevant care.
I feel that, whatever the ‘fiscal constraints’ the NHS finds itself in now and the future, despite the argued need for transformational change in NHS services, people with dementia should be at some stage diagnosed by somebody with specialist medical experience.
This is reflected here in a recent excellent article in the Telegraph.
The other camp is this, and oddly enough there is some overlap in my wish for people with dementia to be given the highest priority in society.
I also firmly believe in good quality research of allowing people to live as best a life they can.
This is intensely personal, as I am physically disabled, and I am all too aware about how people can make crash judgments of you.
I am about to publish a book on ‘Living well with dementia’ on January 13th 2014.
I am honoured to be well respected by academics in the field of dementia, including Prof Alistair Burns the current lead for dementia in England.
I thrive from the research contributions daily all around the world in research into dementia.
I would like to see the UK play a part in leading the research community about all aspects, including the medicine of the condition itself, its possible cure one day, and current practical help in improving quality of life.
Finally, I think with the current academic community in the UK in dementia, the UK can and should achieve this.

Neuroscience and the law focus: what's the point of regulating advertising?
I have no doubt after reading the article entitled “The advertising effect – how do we get the balance of advertising right?” published today by Compass by Zoe Gannon and Neal Lawson that the major thesis of the authors that unregulated advertising is likely to be dangerous for society, and could have a massively detrimental effect.
I really liked this article, as I think that it is one of the few articles which seemed to have an understanding of the modern neuroscience involved in tackling a problem of huge cultural significance, maybe using legal measures. As someone who tends to read the introduction and conclusion of article, I found it most helpful that Gannon and Lawson summarized the gist of their argument successfully in the conclusion,
“If you go to an advertising company to sell a product or service their planners will strip the issue down to bare essentials before building a campaign around it. It is the essence of the message they are after, the essence of the advertising industry is that new technologies, new science and new psychology have put the industry increasingly out of social and political control. Advertising regulations now need to catch up with the reality of the advertising effect on us and our planet.”
On the other hand, I found Jackie Ashley’s response lacked any depth to an analysis of the problem from either a neuroscience or legal perspective (1). However, arguably, one of the most interesting enticing paragraphs begins with the sentence,
“Meanwhile neurologists are working out what images will trigger the buy button in our brains.”
Gannon and Lawson provide that “machines are being used to shed light on brain mechanisms that play a central role in consumer behaviour: circuits that underlie reward, decision making, motivation, emotions and the senses of self.” This would indeed seem to make sense, as the subjective experience of being the target of advertising probably has the same underlying neural basis as our euphoria on sex or drugs of abuse. Indeed, one of the many successes of neurological research in the last century has been to identy a neurobiological mechanism mediating behavior motivated by events commonly associated with pleasure in humans. These events are termed “rewards” and are viewed as primary factors governing normal behavior. The subjective impact of rewards (e.g., pleasure) can be considered essential (e.g., Young, 1959) or irrelevant (e.g., Skinner, 1953) to their effect on behaviour, but the motivational effect of rewards on behavior is now universally acknowledged by experimental psychologists.
In addition, the authors give due credit to one of the most important papers on the subject of “neuromarketing”, a relatively new field. A cognitive neuroscientist (Read Montague) postulated that, if people preferred the taste of Pepsi, the drink should have dominated the market. It didn’t. So in the summer of 2003, Montague gave himself a ‘Pepsi Challenge’ of a different sort: to figure out why people would buy a product they didn’t particularly like. Neuromarketing is effectively the study of the brain’s responses to ads, brands, and the rest of the messages littering the cultural landscape.
Montague had his subjects take the “Pepsi Challenge” while he watched their neural activity with a functional MRI machine, which tracks blood flow to different regions of the brain. Without knowing what they were drinking, about half of them said they preferred Pepsi. But once Montague told them which samples were Coke, three-fourths said that drink tasted better, and their brain activity changed too.

Coke “lit up” the medial prefrontal cortex (a part of the brain very much involved in higher cognitive processes). Montague’s hypothesis was that the brain was recalling images and ideas from commercials, and the brand was overriding the actual quality of the product. For years, in the face of failed brands and laughably bad ad campaigns, marketers had argued that they could influence consumers’ choices. The paper was a substantial contribution to the literature. Montague published his findings in the October 2004 issue of Neuron, and a new field of the neurosciences was born: neuromarketing. (1)
However, there are still some problematic unanswered questions from a neuroethics perspective.
(1) What effect did the Coke label have on the brain that the Pepsi label did not?
(2) What other evidence suggests that taste alone does not determine your favorite cola? Obesity is epidemic in America, and sugared soft drinks are one of the primary culprits.
(3) How might this research help doctors fight obesity?
(4) Suppose both the Coke and the Pepsi labels triggered the same reaction in the brain. What conclusion would you draw?
For a long time, marketing experts have relied on behavioral studies for guidance. In the USA, some companies are taking the practice several steps further, commissioning their own fMRI studies consistent with the research above. For example, in a study of men’s reactions to cars, Daimler-Chrysler has found that sportier models activate the brain’s reward centres as well as activating the area in the brain that recognizes faces, which may explain people’s tendency to anthropomorphize their cars. Steven Quartz, a scientist at Stanford University, is currently conducting similar research on movie trailers. And in the age of poll-taking and smear campaigns, political advertising is also getting in on the game. Researchers at the University of California, Los Angeles have found that Republicans and Democrats react differently to campaign ads showing images of the Sept. 11th terrorist attacks. Those ads cause the part of the brain associated with fear to light up more vividly in Democrats than in Republicans.
Gannon and Lawson in their scholarly article appear to develop their case that, if unregulated, this is dangerous:
“Excessive advertising turns a never ending series of new needs into new wants, and crowds out the space for other visions of the good society, where time and relationships matter more than what we buy. Advertising encourages us to run ever faster on the treadmill of modern consumer life; in so doing it contributes to growing consumer debt, a number of social problems which this report discusses, and to the very real prospect of climate change beyond our ability to manage. So the report calls for a tax on all advertising that encourages greater consumption to limit its scope and slow the pace of growth for the good of society and the future of the planet.”
There are in fact seven ways which Gannon and Lawson perceive as perhaps being capable of solving the problem: e.g. banning advertising in public spaces, controling advertising on the Internet, tax advertising, and probably, most contentiously, introduce statutory regulation of the advertising industry. This would be yet another example of where cognitive neuroscience meets the law in some way – exciting times indeed. If advertising is so rampant, should we spend money researching it like cancer?
References
(1) Jackie Ashley. Let’s take on the ads that fuel such waste, debt and misery. The Guardian, Sunday 24th February 2009.
(2) McGlure SM, Li, J, Tomlin, D, Cypert KS, Montague LM, Montague PR. Neural correlates of behavioral preference for culturally familiar drinks. Neuron 2004 Oct 14;44(2):379-87.
The enigma of the 'freezing-of-gait' in Parkinson's disease: variations on a theme?
This post is in the ‘Dementia’ part of my blog, but please note that not all patients with Parkinson’s disease have dementia. Some patients, however, do.
Parkinson’s disease is easily identifiable to the medical doctor in the UK, it is hoped, because the obvious ‘mask-life’ face of a patient, difficulties in walking (the shuffling gait), a tremor at rest, and stiffness of arms and legs. A particularly intriguing symptom of patients for decades undoubtedly in the research field has been the “freezing of gait” (FOG), which is typically a transient episode – lasting less than a minute, in which gait is halted and the patient complains that his/her feet are glued to the ground. When the patient overcomes the block, walking can be performed relatively smoothly. The most common form of FOG is ‘start hesitation’ (this is what happens when the patient wants to start walking) followed in frequency by ‘turning hesitation’. How or why this happens remains a mystery, but I bet during my lifetime some in-roads will be made into this by academic neurologists (not practising physicians). It is highly relevant as one-day a strategy involving offering cues in the environment may be of use in overcoming FOG problems. This video is for example a remarkable example of this.
As for my own interest in this incredibly interesting phenomenon, I once did at a questionnaire study as a post-doctoral research fellow with Prof Marjan Jahanshahi at Sobell Department of Motor Neuroscience and Movement Disorders, Institute of Neurology and the National Hospital for Neurology and Neurosurgery, University College London. This questionnaire at the factors which cause FOG, as perceived by patients attending the movement disorders clinic of the National. Hospital. This study examined the factors that induce FOG, and identified the cues and strategies that help overcome it through a postal survey of 130 PD patients. 72% reported FoG. The factors that commonly induced FOG, I found, were turning, fatigue, confined spaces and stressful situations, in addition to emotional factors. FOG was also ameliorated by various attentional and external cueing strategies. I feel that one day these results will be enormously useful in patients designing strategies for overcoming FOG, a very real and troublesome phenomenon for patients with Parkinson’s disease. I believe, personally, that it is these trigger factors which help us to understand the phenomenon of FOG, and it is these which my academic colleagues should invest their energies into discovering.

However, in many of the studies, there has been an emergent consensus to identify the factors which can cause patients to ‘unfreeze’ through the phenomenon known as ‘paradoxical kinesia‘. In an academic discussion on the subject, Dr. Friedrich Asmus and colleagues (2009) from the University of Tübingen, Germany, offered that, on the basis of the freezing study above, that, “in this context, visual cueing has a pivotal role, as shown by the report of a patient with PD during the war who was paradoxically able to run by following the footsteps of his wife in front of him. Smilar and reproducible effects of patterned movements like running stairs have been described in the context of paradoxical kinesis“. Another finding from the freezing study was that patients with Parkinson’s disease reported that turning difficulties appeared to be associated with freezing, but the problem was that only limited studies had been conducted to characterize these difficulties. In a formal analysis, the laboratory of Prof. Alice Nieuwboer at the University of Leuven in Belgium indeed this report to be borne out in formal gait analysis, and further found that, during turning, non-freezers and controls decreased their cadence whereas freezers increased it, which may be related to freezing-of-gait.
A major obstruction in this research is the observation that the underlying brain pathology underlying FOG remains largely unknown. Behavioural studies have helpfully identified several gait alterations in patients with Parkinson’s disease with FOG, even when the patient is not experiencing an actual FOG episode. These can be discovered when people with Parkinson’s disease are walking on a treadmill. Alterations include premature timing of muscle activations, increased variability of gait, increased temporal gait asymmetry and faulty generation of postural adjustments before step initiation. Recently, it was suggested that FOG may be caused by a failure to generate adequate amplitudes for the intended movement.
As an advance in the research from Snijders and colleagues published in Brain on 1st December 2010, a study was reported, which looked at gait planning in patients with freezing of gait, using motor imagery of walking in combination with brain scanning. They included 24 patients with Parkinson’s disease: 12 patients with freezing of gait, 12 matched patients without freezing of gait and 21 matched healthy controls. Subjects performed two previously validated tasks—motor imagery of gait and a visual imagery control task. During motor imagery of gait, patients with freezing of gait showed more activity than patients without freezing of gait in the mesencephalic locomotor region.

And what does this brain area do? Well, on deeper examination, it seems that – as usual – no-one precisely knows, and the situation is undoubtedly complicated by the fact that defining this region in the human brain has been troublesome, in relation to our non-human counterparts. Based on biologically hypothesized connections of the central pattern generator in the salamander, it is now a widely held belief that this part of the brain indeed represents some sort of a robotic system which acts as a generator of simple movements. For example, electrical measurement studies from Steeves and Jordan back in 1984 have shown that stimulation of the mesencephalic locomotor region (MLR) located in the brain of the salamander produce different gaits, swimming or walking, depending on intensity level.
So where is this part of the brain exactly? Well, they describe:
Ascending projections were observed to the subthalamic nucleus, caudal hypothalamic nuclei, the centrum medianum nucleus of the thalamus, the ventral tegmental area of Tsai, the superior colliculus, and the periaqueductal gray region. The ascending projections were also ipsilateral, with sparse contralateral labeling confined to areas which received ipsilateral projections. Projections to the contralateral cuneiform nucleus were also consistently observed. The results, when compared to those of another study, suggest that the classical MLR is anatomically distinct from the more medial sites in the mesencephalon which can also induce locomotion.
In all honesty, this leaves me pretty clueless, and I doubt whether a human neurosurgeon would feel particularly comfortable with this working definition, either. But that brings one onto a really interesting point – can knowing the abnormal part of the brain is help with precise neurosurgery into a part of the brain, called ‘stereotactic surgery’? Well – maybe no, if “patients with freezing of gait also tended to have decreased responses in mesial frontal and posterior parietal regions“.
Is what they’ve done useful then? Yeah, but it is also the case they’ve found brain areas which correlate with this abnormal behaviour, rather than necessarily causing it. I remember the classic Psychology finals question from Cambridge from the early 1980s which provided, “If we subtract the brain areas activated by Christian saying the Lord’s Prayer from those activated by atheists saying the same prayer, would we have found the neural substrate of Christianity?” The paper in my sense falls into this classic problem of brain scanning, but what choice did the investigators really have because they couldn’t have got them into a scanner, freeze, and then unfreeze? That would in a sense be the ideal experiment, and it indeed might be possible if there were a convincing animal model of FOG and freezing-of-gait, but this surely is a long-way off.
Interesting further reading
Anke H. Snijders, Inge Leunissen, Maaike Bakker, Sebastiaan Overeem, Rick C. Helmich, Bastiaan R. Bloem, and Ivan Toni. Gait-related cerebral alterations in patients with Parkinson’s disease with freezing of gait Brain first published online December 1, 2010 doi:10.1093/brain/awq324
Steeves JV, Jordan, LM. Autoradiographic demonstration of the projections from the mesencephalic locomotor region. Brain Res. 1984 Jul 30;307(1-2):263-76. http://www.ncbi.nlm.nih.gov/pubmed/6466996
Rahman, S, Griffin, HJ, Quinn, NP, Janahshahi, M. The factors that induce or overcome freezing of gait in Parkinson’s disease. Behav Neurol 2008;19(3):127-36.
