Home » Posts tagged 'Independent'
Tag Archives: Independent
I can see why some Doctors would be driven to suicide. I was mentally ill, and felt the same with the GMC FTP.

At least 96 doctors have died while facing a fitness-to-practise investigation from the General Medical Council since 2004, though it is not clear how many of these cases were suicide.
I can understand exactly how this has happened.
I had a prolonged GMC investigation between 2004 and 2006. At no point during this process was I told when then this mentally arduous process would come to an end.
I think now, seven years into recovery, that there by the grace of God go I.
The media have a remarkably high level of detail of understanding from the perspective of the General Medical Council about forthcoming cases. It is impossible for the Doctor to get his side across in the media.
The GMC claim they don’t do show trials.
But my father was fully humiliated with the media storm.
My father was faced with a Doctor son who was in denial and lacked insight. My father is now dead, but I should like to say he probably died in complete humiliation of his son.
My experience is of a GMC which plays to people’s weaknesses in low self esteem and low confidence, a personality trait shared by many with addiction disorders.
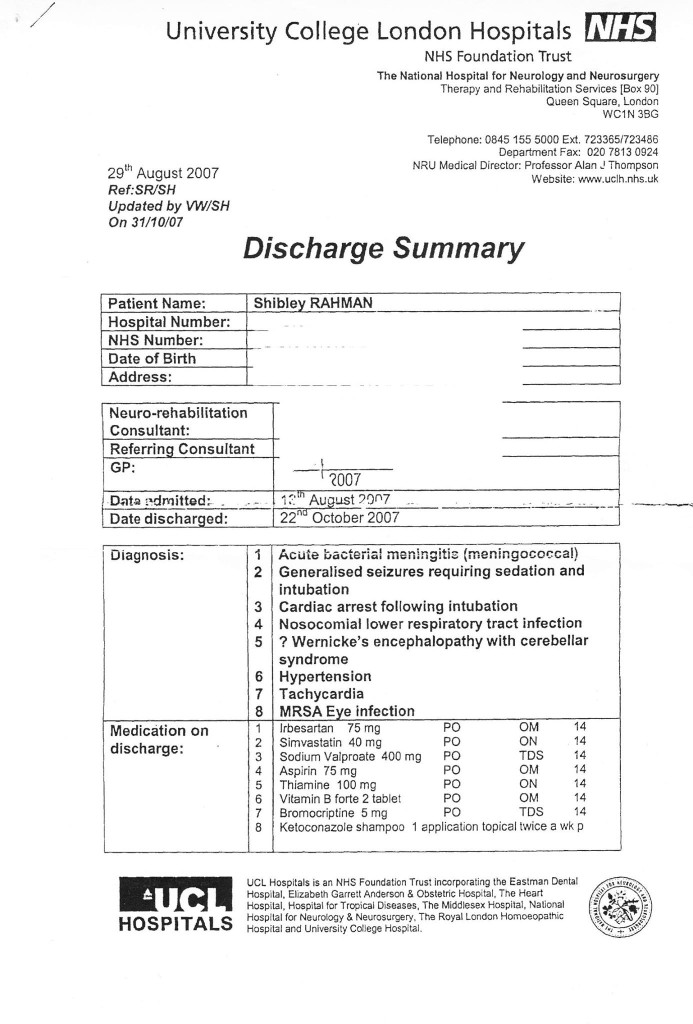
Not one report in the mainstream media reported that I was severely alcoholic. And yet the GMC, prior to their erasure of me, erased me with five independent reports stating clearly that I had at least a severe alcohol problem; and that I needed help.
One of the referrals to the GMC was when I attended the A&E of a hospital with acute intoxication. In addition to the referral to the GMC by the Consultant in A&E, I was not offered any post-event support for alcoholism.
The GMC know how to present themselves in the media, but this is in contradistinction to the experience of those who have experienced the Fitness to Practise process first hand.
Dr Peter Wilmhurst writes in 2006 in a wide-ranging criticism of the GMC as follows:
In wishing to infer ‘bad character’, the General Medical Council must not go beyond its statutory duty of promoting public safety. Otherwise, there is simply mission creep and a torrent of smears into a hate campaign by the regulator or its company.
In 2005, one year before I was eventually due to see the GMC, I was suspended. This was due to an alcoholic bender in Northwick Park. I was crying all day in a pub because I could not cope with the investigation any more.
I had waved goodbye to my late father, and lied to him saying I was going shopping.
I didn’t. I ended up being sectioned by a psychiatric hospital in North London, and my father spent ages talking to the medical staff there.
I was then suspended. It was at that point, I wished to call it a day.
I phoned the Samaritans, and they talked me out of it.
I have never told anyone this story. I feel very strongly about what the General Medical Council did to me, even though it might have been merely a product of their inefficiency.
Nobody appears to wish to want to change the system. I’m pretty sure that there are juniors who wish to hold tight until they are Consultants.
What happened to me is that I had consultants in two Trusts in West and North London who said I was ‘late for work’, ‘smelling of alcohol’ and ‘dishevelled’.
None of this got reported in the main media.
I was erased. To this day, I still have no idea who retrospectively complained in graphic detail about my alcoholism did not offer me sick leave, or help with occupational health.
One of them even had the gall to write in his witness statement for the GMC that he gave me the phone number of a private clinic.
I find this particularly ironic as I was later done for incompetence, when that North London trust had allowed me to finish my medical job there, successfully running cardiac arrests there. I passed my Advanced Life Certificate there. I even have the certificate to prove it.
I feel disgusted by the way that the General Medical Council goes about its business.
Far too many one-sided media reports appear in the media containing detailed accounts, as yet unproven. There’s a sense of being hung before you even go to the gibbet.
I am now in my seventh year in recovery. I have done four books, and my Bachelor of Law, Master of Law and Master of Business Administration.
I even completed my pre-solicitor training, as I am regulated by the Solicitors Regulation Authority.
My late father died two months before the Solicitors Regulation Authority gave me permission to finish my legal training, after a meticulous consideration of various factors including details of my erasure.
I am now applying to be restored. And so everything gets racheted up again. The dogs will get unleashed.
And so far they’ve dragged me up to the City where I was struck off, without my late father, surrounded by the same bars and clubs and restaurants. I didn’t have a relapse. Care and compassion are simply two words which are not in the GMC’s dictionary.
I am even applying to go to a desk, non “facing job”. I am now following my erasure newly disabled, so I would not wish to do clinical medicine in any form.
I do not want to be in public health with the stigma of having been erased, for a period of life when I was very ill, and the undoubted discrimination that that would entail.
I had one year of sitting in a pub all day after I was eventually erased in 2006.
This was an extremely dangerous part of life. For my father, it was unbelievably distressing. Nonetheless, he came to visit me every day on the ITU when I was in a coma due to this a year later.
I so understand why there have been so many deaths of Doctors waiting GMC FTP. That could easily have been me.
But I am fighting fit now, and looking forward to my hearing very much.

A person newly diagnosed with dementia has a question for primary care, and primary care should know the answer

Picture this.
It’s a busy GP morning surgery in London.
A patient in his 50s, newly diagnosed with Alzheimer’s disease, a condition which causes a progressive decline in structure and function of the brain, has a simple question off his GP.
“Now that I know that I have Alzheimer’s disease, how best can I look after my condition?”
A change in emphasis of the NHS towards proactive care is now long overdue.
At this point, the patient, in a busy office job in Clapham, has some worsening problems with his short term memory, but has no other outward features of his disease.
His social interactions are otherwise normal.
A GP thus far might have been tempted to reach for her prescription pad.
A small slug of donepezil – to be prescribed by someone – after all might produce some benefit in memory and attention in the short term, but the GP warns her patient that the drug will not ultimately slow down progression consistent with NICE guidelines.
It’s clear to me that primary care must have a decent answer to this common question.
Living well is a philosophy of life. It is not achieved through the magic bullet of a pill.
This means that that the GP’s patient, while the dementia may not have advanced much in the years to come, can know what adaptations or assistive technologies might be available.
A GP will have to be confident in her knowledge of the dementias. This is an operational issue for NHS England to sort out.
He might become aware of how his own house can best be designed. Disorientation, due to problems in spatial memory and/or attention, can be a prominent feature of early Alzheimer’s disease. So there are positive things a person with dementia might be able to do, say regarding signage, in his own home.
This might be further reflected in the environment of any hospital setting which the patient may later encounter.
Training for the current GP is likely to differ somewhat from the training of the GP in future.
I think the compulsory stints in hospital will have to go to make way for training that reflects a GP being able to identify the needs of the person newly diagnosed with dementia in the community.
People will need to receive a more holistic level of support, with all their physical, mental and social needs taken into account, rather than being treated separately for each condition.
Therefore the patient becomes a person – not a collection of medical problem lists to be treated with different drugs.
Instead of people being pushed from pillar to post within the system, repeating information and investigations countless times, services will need to be much better organised around the beliefs, concerns, expectations or needs of the person.
There are operational ways of doing this. A great way to do this would be to appoint a named professional to coordinate their care and same day telephone consultations if needed. Political parties may differ on how they might deliver this, but the idea – and it is a very powerful one – is substantially the same.
One can easily appreciate that people want to set goals for their care and to be supported to understand the care proposed for them.
But think about that GP’s patient newly diagnosed with dementia.
It turns out he wants to focus on keeping well and maintaining his own particular independence and dignity.
He wants to stay close to his families and friends.
He wants to play an active part in his community.
Even if a person is diagnosed with exactly the same condition or disability as someone else, what that means for those two people can be very different.
Once you’ve met one person with dementia, you’ve done exactly that: you happen to have met one person with dementia.
Care and support plans should truly reflect the full range of individuals’ needs and goals, bringing together the knowledge and expertise of both the professional and the person. It’s going to be, further, important to be aware of those individuals’ relationships with the rest of the community and society. People are always stronger together.
And technology should’t be necessarily feared.
Hopefully a future NHS which is comprehensive, universal and free at the point of need will be able to cope, especially as technology gets more sophisticated, and cheaper.
Improvements in information and technology could support people to take control their own care, providing people with easier access to their own medical information, online booking of appointments and ordering repeat prescriptions.
That GP could herself be supported to enable this, working with other services including district nurses and other community nurses.
And note that this person with dementia is not particularly old.
The ability of the GP to be able to answer that question on how best her patient can lead his life cannot be a reflection of the so-called ‘burden’ of older people on society.
Times are definitely changing.
Primary care is undergoing a silent transformation allowing people to live well with dementia.
And note one thing.
I never told you once which party the patient voted for, and who is currently in Government at the time of this scenario.
Bring it on, I say.

I bought today my own book “Living well with dementia” at a bargain price from Primrose Hill Books
I got a bargain today.
I have been quite a good mood recently, getting ready for my book launch in Camden on the afternoon of February 15th, 2014. We’re all going out for dinner in Pizza Xpress later that evening, somewhere in Central London.

I bought my own book ‘Living well with dementia’ from Primrose Hill Books for the very much discounted price of £16.99.
This is not because it was a soiled copy, or because I was the buyer.
It was because they had ordered it in especially from the wholesalers, and managed to sell it onto me a very much reduced price.

Of course I am very grateful, as I think it’s important to support local independent booksellers in the community.
Here’s a good piece from last year on ‘five reasons to support your local indie bookseller‘.
Here are the full details of ‘Primrose Hill Books’. They’re on the main road which passes through Primrose Hill. This book is called Regents Park Road.


Nonetheless, I appreciate that some people will prefer to use the bigger well known book retailers, especially if they do not time to browse or travel to such bookstores.
After a bit of haggling, we got Amazon this afternoon to reduce their delivery time from 9-11 days to fewer than 24 hours. This is of course a huge result for me. Their page on my book is here.

The Blackwells Bookstore is normally a good place to find the book for immediate delivery, but not at the time of writing this blogpost. The book is currently out of stock, but I do know reliably they had a good stock once upon a time. Here is their page.
But Primrose Hill Books will always have a special place in my heart. I’ve bought books there I’d never have ordered on Amazon, for example, through browsing.
It’s run by Jessica and Marek (and Kelly is often there too). All three have an enclopaedic knowledge of current books, some well known, some not so well known.
Of course, it was a source of great pride to see my book there. I’ve published specialist textbooks, but not the type which would look in place in the bookshop above or any other high street bookseller.
Here’s Jess looking at the book.

She said it was a good book, and we had a discussion of how long it had taken me to write (a year), how this had become a real passion of mine to share this information and to dispel all the scientific misinformation about dementia, and how it was written in the style of a long blogpost but it actually contained a lot of interesting contemporaneous evidence and discussion.
It is of course a bit weird to see the book alongside classics such as Ben Goldacre’s “Bad Pharma: How medicine is broken, and how we can fix it” and Naomi Wolf’s “Vagina”. But hey ho.

You can buy the book from the publishers’ website too.
Their is their official flier. You get 20% off if you use the promotional code ‘AUTHOR20′. You enter this code apparently just when you are completing the ‘checkout’ in this e-bookstore.
And finally, one of the people I genuinely admire the most is Tommy Whitelaw (please support Tommy at “@tommyNTour“).
You can read about Tommy’s campaign for giving carers ‘a voice’ on my blog here. His story continues to motivate me very much – and not just because he’s a Glaswegian like me!
Tommy is very honoured that his campaign and letters in Sally Magnusson’s Book “Where Memories go”.

Hopefully the episode where Sally talks to Tommy in “Medical matters: caring for carers” will be made available on the BBC iplayer shortly.
And finally – here’s Sally’s book on the Hodder website.
All in it together, and all that.
Reform of legal aid in England and Wales: the Government response, June 2011
Legal Aid, Sentencing and Punishment of Offenders Bill
This is what two of the broadsheets said today.

The vital advice provided by these specialists in social welfare law has helped many of the families and individuals that I see to avoid costly litigation and prevent or mitigate the effects of marital and family breakdown.
Over 650,000 people, at recent estimates, and half a million according to the Ministry of Justice’s own impact assessment, will lose out on this vital help through changes to legal aid alone, at a time where other funding streams for free advice have already been cut or are under threat. About 6,500 social welfare law cases will no longer be funded in Birmingham. Liverpool will see about 9,800 cases cut. Each of these represents a loss of specialist help at a time when it is most needed.
Legal aid funding is being withdrawn from all employment advice, all welfare benefits advice and virtually all debt advice, nearly half of housing advice and nearly all of education advice. There can only be one outcome: avoidable poverty and distress for many thousands of people.
Not only will people be less likely to receive advice, but advice will be harder to find as agencies currently funded through legal aid find it more and more difficult to carry on. For example, the average impact on individual, not-for-profit providers of the cuts being proposed will be a 92% drop in income from legal aid.
Wesley Johnson in the Independent:
Vast swathes of the British population will be barred from accessing publicly-funded legal advice and representation following Justice Secretary Kenneth Clarke’s decision to press ahead with reforms, campaigners said.
Legal aid “will no longer routinely be available for most private family law cases, clinical negligence, employment, immigration, some debt and housing issues, some education cases, and welfare benefits”, Mr Clarke said.
The moves will put publicly-funded legal advice and representation “beyond the reach of vast swathes of the British population”, the civil rights group Liberty said.
Mr Clarke said they will still be able to use “alternative, less adversarial means of resolving their problems” and insisted that “fundamental rights to access to justice will be protected”.
But Liberty director Shami Chakrabarti said the moves were a “slap in the face” for “ordinary families, children and the disabled”.
