Home » Posts tagged 'G8'
Tag Archives: G8

Concerns about the paired associates learning test for dementia
To begin to understand how a cathode-ray TV set works, I could remove one component called the “transistor”, and the picture disappears. It would be an incorrect conclusion to say that the purpose of that transistor is to produce the picture. However, I could argue correctly that the transistor was somehow part of the system required to produce the picture.
If I showed the transistor was particularly “hot” while the TV set was on, producing a picture, it might be reasonable for me to conclude the transistor was involved in producing the picture.
This is the sort of basic approach still used to work out what is going on in the brains and minds of people with Alzheimer’s disease, typical presentations of which might be memory problems. You can see whether removing parts of the brain in humans produces similar effects to the problems in thinking found in Alzheimer’s disease. Or alternatively, you could just try to look at the system of components in the brain which might be contributing to memory in brains working normally.

Whatever, it’s a puzzle. In this particular case, it’s a puzzle to solve correctly.
An innovation culture in the diagnosis of Alzheimer’s disease
David Cameron praised Cambridge Cognition’s work in developing new innovative tests for Alzheimer’s disease in the G8 summit held towards the end of last year.
There has been concern that some individuals with Alzheimer’s disease do not receive their diagnoses in a particularly fast way. A number of explanations for this have been offered, including medical personnel not being able to spot the symptoms of Alzheimer’s disease easily.
It is also helpful to understand what an “innovation” is. An innovation might be a product which enables you do something much more easily, and depends for its success popular uptake by the user. Strictly speaking, paper was an innovation too. However, the rise in cost of diagnosing Alzheimer’s disease, arguably, is an intriguing example of “Baumol’s cost disease“.
Individuals with Alzheimer’s disease have memory problems which are typically not thought to be qualitatively similar to those found in ageing elderly individuals. Often such people have real problems in navigating around environments. It is clearly a very laudable aim to have a bedside test which might be able to alert a physician to an underlying memory problem in Alzheimer’s disease.
The benefits and concerns, and my passing involvement
There are a number of important caveats here. Not all dementias are Alzheimer’s disease. There are in fact hundreds of dementias, some of which are reversible. Whatever test is used, the test should be sensitive enough to identify reliably a genuine thinking problem in Alzheimer’s disease, but should not be so ‘broad brush’ the test also misattributes memory problems, say found in the ‘mild cognitive impairment’ or even depression, to Alzheimer’s disease. Such mislabelling can perceivably cause distress, and cause people to be caught up in the medical system for further lengthy tests when they should not have been in the first place. On the other hand, it is of concern that the diagnosis might be missed in some people, and hence the drive from the Department of Health and the Alzheimer’s Society in “The Prime Minister’s Dementia Challenge”.
I wish Cambridge Cognition well, not least because I have worked with CANTAB whilst a graduate student at the University of Cambridge. In fact, some of my papers are cited in their bibliography. Their search facility is here.
The CANTABmobile “paired associates learning” test
To explain the “paired associates learning” test from first principles, and I’m not using actual screenshots, imagine me presenting you with a number of blank boxes dotted around the screen.

And I open each box in turn and reveal a shape to you. I can present the problem with a varying number of shapes.

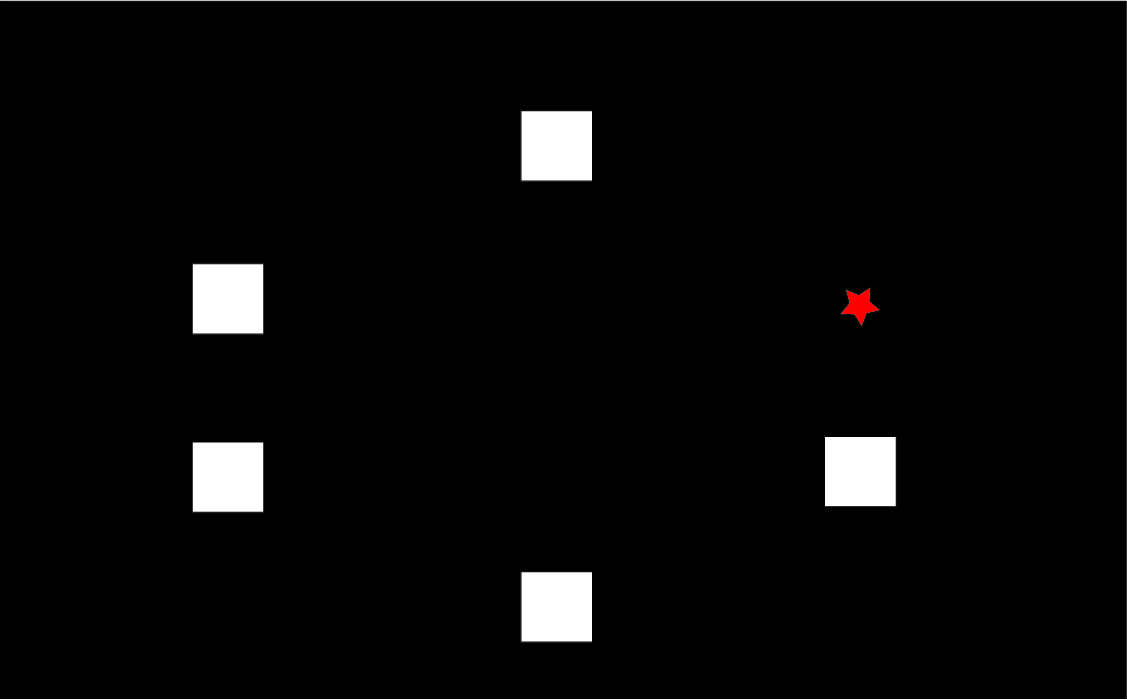
After showing you all the shapes, I then present to you a shape and ask you to identify the box in which it was first presented.

Cambridge Cognition in welcoming the Draft National Plan to Address Alzheimer’s disease in my opinion set out entirely correctly the advantages of this computerised testing battery; including fast, not culturally biased, not heavily loading on language, norm-referenced, culturally unbiased, and easy-to-use.
The reasoning behind it being sensitive to early Alzheimer’s disease – but what about mild cognitive impairment?
To understand why the narrative for the test being so attractive in early Alzheimer’s disease, you have to understand that this test has been found to be sensitive to functions of particular brain areas. If you chop out bits of the brain near the front of the head (frontal cortex) or near the ear (temporal cortex), performance on this task is impaired, as Prof Adrian Owen showed when he was a post-doctoral fellow (paper here). With hindsight, perhaps Owen should have looked at the effects of other brain areas further back in the brain, such as the parietal cortex, which are also now thought to be important in memory for spatial cues.
A consistent finding has been loss of brain cells in the “entorhinal cortex”, in the temporal cortex, early in Alzheimer’s disease (see for example here). Therefore, that the paired associates learning test should identify memory problems in early Alzheimer’s disease immediately makes intuitive sense.
But the issues I feel are much more complicated, and I wish Cambridge Cognition well in clarifying them.
If it’s not Alzheimer’s disease, what else could be causing the memory problems?
One possibility is “mild cognitive impairment”. It is described, for example on the authoritative Mayo Clinic website, that:
“Mild cognitive impairment (MCI) is an intermediate stage between the expected cognitive decline of normal aging and the more serious decline of dementia. It can involve problems with memory, language, thinking and judgment that are greater than normal age-related changes. If you have mild cognitive impairment, you may be aware that your memory or mental function has “slipped.””
David Hart, Senior Business Development Manager of Cambridge Cognition, kindly sent Dr Peter Gordon the rationale for the use of the CANTAB task by Dr Andrew Blackwell, their Chief Scientific Officer (as produced on Peter’s blog here).
Cambridge Cognition concede that distinguishing between MCI and Alzheimer’s Disease “is difficult”, but this is a distinction that must be arrived at otherwise a test potentially will give “false positives” – but no test is perfection, and it basically is impossible to strive for perfection. What we all trying avoid is where a test for possible dementia itself is expensive followed by a further expensive investigation to show the original result was a false positive – or as the Express euphemistically called it recently, “Dementia diagnosis proved wrong by new super scanner”. (It is important to state clearly here that no details are given how a diagnosis had been arrived at previously for Ros Davies.)
To give them credit, Cambridge Cognition cite the Chandler et al. (2008) paper, but the full citation of this is “Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association Volume 4, Issue 4, Supplement , Pages T551-T552, July 2008″ – i.e. it is a supplement of abstracts not full papers. This particular abstract can be viewed here.
It is hoped that this full study will have been published elsewhere, and if so Cambridge Cognition will need to update their website with the full paper. Notwithstanding this, the numbers of individuals in each group are disappointingly low: there are seventeen with putative MCI and twelve with putative Alzheimer’s disease.
Is this task actually sensitive and specific?
However, the discussion by Dr Andrew Blackwell and colleagues in his 2004 paper is useful. I have more than a passing interest in that paper as the main author on that paper was one of my PhD supervisors at Cambridge, Prof John Hodges. John has also kindly written one of my three Forewords for my book, “Living well with dementia” to be published on January 14th 2014.
Blackwell remarks correctly that this task has been used to distinguish between unipolar depression and Alzheimer’s disease in Rachel Swainson’s study. But is this enough? I looked to the previous Beats study in “geriatric depressive”, and there was nothing forthcoming there. How confident can one be that only early patients with Alzheimer’s disease, and not those severely depressed or with an underactive thyroid, will perform abnormally on the PAL? Personally, I’m not at all confident yet, despite the Swainson study, but these fears can easily be allayed with a sensitivity/specificity study of much higher power.
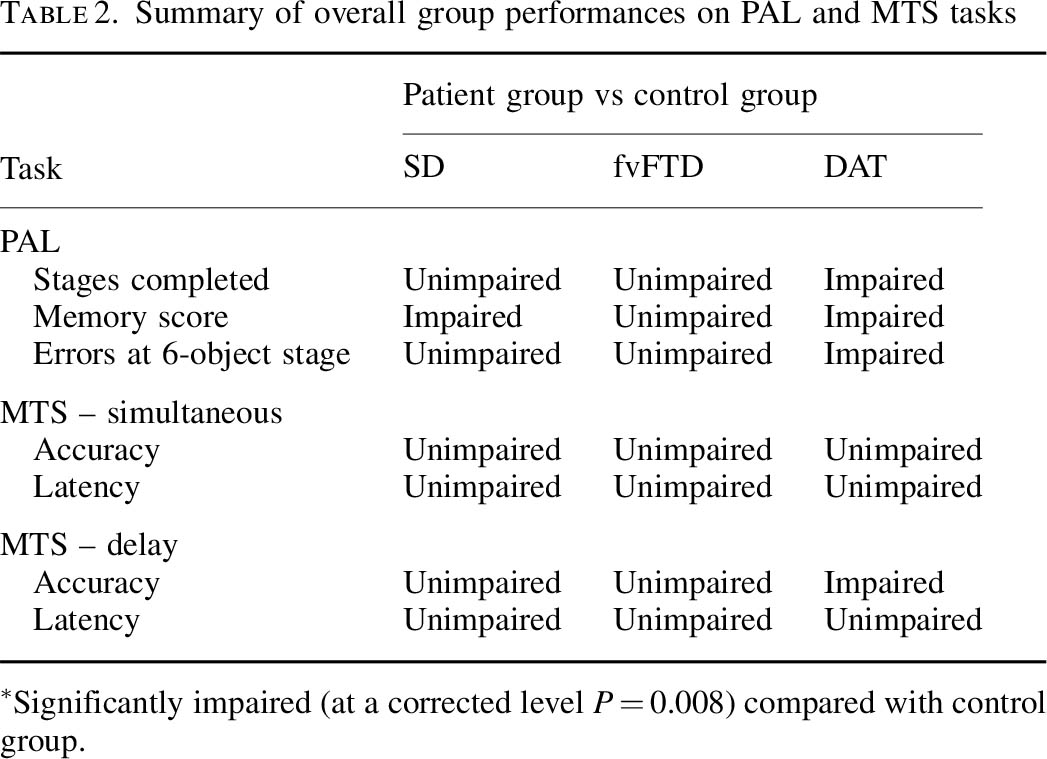
Blackwell is however correct in citing my study with Dr Andy Lee in that patients with semantic dementia and behavioural variant frontotemporal dementia are relatively unimpaired, though the clinical presentations of the frontotemporal dementias can be quite clearly different in the clinic from Alzheimer’s disease. Completing the double dissociation, I did find that the behavioural variant of frontotemporal dementia did present with rather specific risk-taking decision-making of its own.
But in the meantime the comparison with frontotemporal dementias is useful.
Nonetheless, this approach is being rolled out.
On 28 June 2013, the use of CANTABmobile was described as follows:
“The Guildford and Waverley Clinical Commissioning Group (CCG) is leading the use of an innovative new iPad-based memory assessment system as part of a national push to decrease dementia diagnosis waiting times and streamline the referral process. Accessed through NHS medical professionals, CANTABmobile enables GPs to test a patient’s episodic memory through an easy to use and administer 10-minute cognitive assessment.”
The CANTAB paired associates learning test is pictured under the heading “intuitive touchscreen interface”. if you go to “download information” on this page.
It was covered in the national media here: for example Victoria MacDonald’s report (this page provides a criticism of another report by Victoria MacDonald this time over Prof Brian Jarman’s proposed HSMR data by NHS Consultant, Dr Jacky Davis).
So what does this task test?
In understanding how the task works in reality, I found a paper where Prof Ed Bullmore and colleagues put individuals with Alzheimer’s disease and control subjects performing the task into a scanner really helpful. Bullmore and colleagues frontloaded their discussion with the following comment:
“Independent of the level of difficulty, the majority of subjects in both groups activated a network of brain regions, including the anterior cingulate, lateral, and medial occipitoparietal and frontal cortices, during successful encoding and retrieval.”
This is interesting as it doesn’t point to the usual suspects of the narrative, i.e. the entorhinal cortex and other parts of temporal lobe. Even Andrew Blackwell had described how the damage to the entorhinal cortex might possibly account dor deficits on the paired associates task:
“The transentorhinal region is a complex transitional area located between the entorhinal region proper and the adjacent temporal isocortex. It has been suggested that damage to this site in early [Alzheimer's disease] disrupts reciprocal connections with the hippocampal formation and that this disruption underlies deficits in episodic memory.”
But on reflection is this wholly a surprise? Ed Bullmore and colleagues from their results, also from Cambridge, discuss that the lateral parietal activations reported during episodic memory tasks are thought to reflect recognition processes and retrieval processing of spatial information. Medial parietal activity has been proposed to underlie imagery and retrieval success.
I don’t feel it’s altogether surprising given what is known about the build-up of pathology in Alzheimer’s disease, either. The authors of one study looking at this report that:
“[18F]FDDNP-PET signal was significantly higher across widespread cortical regions in subjects with poorer neuropsychological test performances. Strong correlations were seen in the entorhinal, orbitofrontal, and lateral temporal cortices, temporoparietal and perisylvian language areas, parietal association cortices, and much of the dorsolateral prefrontal cortex.”
But the Sahakian lab elsewhere did find something was up with the parts in “the hippocampus and associated structures”, i.e. the structures in the temporal lobe, in this task.
But that study was only comparing MCI with normal controls. It did not include patients with Alzheimer’s disease. This is relevant, if you happen to believe that MCI ‘predates’ Alzheimer’s disease, as the authors of that study clearly do:
“Later in the course of the transition from MCI to clinical Alzheimer’s disease, functioning of the MTL deteriorates further to an extent that such compensatory activity is no longer possible. The hyperactivity in early MCI might then represent a possible predictor or biomarker of the progression to Alzheimer’s disease.”
But in the real world this is far from clear.
However, the evidence of progression of MCI (mild cognitive impairment) to DAT is currently weak. It might be attractive to think that MCI is a preclinical form of dementia of Alzheimer Type, but unfortunately the evidence is not there to back this claim up at present: only approximately 5-10% and most people with MCI will not progress to dementia even after ten years of follow-up (Mitchell and Shiri-Feshki, 2009). Drug companies have been trying hard to push the identification of “biomarkers”, possibly subtle psychological ‘deficits’, scan results or changes in substances in the fluid surrounding the brain (or cerebrospinal fluid). It is no accident that psychological testing and biomarkers were heavily promoted in David Cameron’s G8 dementia speech in Lancaster House at the end of last year.
In summary, I don’t think it can be taken as red that entorhinal cortex problems are causing the observed deficits in the CANTABmobile paired associates learning task.
Conclusion
Overall, my personal view is that the deficits on the CANTAB paired associates learning task are real in early Alzheimer’s disease, but possibly not for the reasons felt by some in their groups. Above all, I don’t care as such, as long as greater numbers of people benefit from a correct diagnosis of Alzhemer’s disease, but I do feel that the logic in their reasoning has gone a bit awry.
My academic viewpoint is utterly irrelevant actually, as above all I wish the whole of the medical profession well in their “war against dementia”.
I’d be the first to admit I’ve got it wrong. I am simply raising the issues in a constructive way that I hope is beneficial for the public interest.
But Dr Mitul Mehta, Reader in Neuroimaging at the IoP, does have his concerns.

The G8 dementia Summit: the comparison with the botched NHS reforms is striking

This week, to great fanfare, the G8 hosted its summit on dementia. Indeed, that the G8 were discussing a single condition was indeed remarkable. That they were joining forces to consider working together on this inspired hope.
What was unforgiveable was the sheer volume of myths about dementia which were pedalled though by the media. Prof Alistair Burns to his credit gave an answer in an interview by Emily Maitlis explaining how dementia prevalence rates appeared to be falling, in response to the backdrop set up by media memes such as ‘timebomb’. Many were left extremely angry on account of the lack of balance, completely distorting the picture such that any idea of someone ‘living well with dementia’ became a rarity.
What was not expected was a sanitisation of advanced dementia, but even there there was not a discussion of end of life care. In fact, there generally was no discussion of a minimum safe level of health and social care in any of the countries. The media pushed hard ‘a cure for dementia by 2025′, which major Alzheimer’s societies had signed up to. The claim is complete and utter rubbish, as there are over a hundred different types of dementia; the public were unashamedly being sold a pup.
The English health system, the National Health Service, has an obsession with ‘efficiency’. So much so it will happily fork out to pay one for one junior doctor covering all the general medical hospital every night for a week, and that junior doctor doesn’t stop all night. Sometimes that junior doctor will be expected to cover the wards too. Cover by nurses can be equally ‘lean’ during the weekends too.
The obsession with measuring ‘I want good care’ and regulation is akin to a teacher who has forgotten to teach but can set regular assessments. When the system is set up to run everything with much less doing a lot more, it’s possible something has got to give. And this is of course precisely what happened at Mid Staffs.
And yet out of the blue there appeared a 493 page document ultimately called the Health and Social Care Act (2012) which had nothing to do with this most important point about patient safety. There is not even a single clause to do with patient safety (unless you include the clause abolishing the National Patient Safety Agency). The medical Royal Colleges were not involved. The BMA was not involved. And yet the Act of parliament, outsourcing and privatising the NHS, is just what the Corporate ordered.
This is what is known in the (business) trade as an ‘opportunity cost’ where money and efforts could have been better spent elsewhere. In this particular case, despite a promise of ‘no top reorganisation’, there was a £3bn reorganisation.
When attending a medical ward, you have to go to the sick patient first. You have to prioritise. If there had to be an unannounced reform of the NHS, outsourcing it was not the priority. The latest survey even shows that the public don’t especially like private providers doing NHS work.
Likewise, the priority for dementia care should have been investment in the social capital of caring. Too often carers are embattled with the biological, financial and legal considerations of caring. Many carers are themselves on zero-hours contracts. The G8 dementia summit was a great opportunity to confront that.
It didn’t. Instead, with alarming synchrony, the G8 leaders came together to sing off the corporate script. Vivienne Parry with effortless ease choreographed a seemingly spontaneous discussion about well rehearsed arguments for the need for ‘big data’, global data sharing, genomics, and personalised medicine, for much of the day. Prevention was of course discussed, but this is of course intimately wound up with the collection of information about the person, and the use of that other pet subject, biomarkers.
And more research is not better research, in the same way bigger information is not better information. If research monies are diverted into data analysis, genomics and personalised medicine, these monies will be diverted away from research into caring for example. One wonders whither the ‘cure for dementia’ will actually go, unless they have another fifteen years to look at slowing the progression of Alzheimer’s disease. The evidence that cholinesterase inhibitors, a class of drugs used to treat symptomatically memory and attention problems in Alzheimer’s disease, has a beneficial effect on slowing disease progression is as low as it possibly can be after nearly 20 years of expensive research in this area.
The G8 summit, like the Health and Social Care Act, was ‘corporate capture’ at its best, so if you’re angry, well done, that is the appropriate emotional reaction! If you were wondering if you’d accidentally missed the discussion of carers and how they would be involved until 2025, don’t worry, you hadn’t. They weren’t there.
The day the corporates captured the global dementia policy
This blogpost first appeared on the ‘Living well with dementia’ blog.
The setting for today’s #G8Dementia Summit was in Lancaster House, London.
 Many thanks to Beth Britton, Ambassador for Alzheimer’s BRACE and campaigner, Anna Hepburn at the Department of Health, and Dr Peter Gordon, Consultant and expert in dementia, for helping understand, with the excellent livestream from the Department of Health, what challenges might be in store for global dementia policy in the near future.
Many thanks to Beth Britton, Ambassador for Alzheimer’s BRACE and campaigner, Anna Hepburn at the Department of Health, and Dr Peter Gordon, Consultant and expert in dementia, for helping understand, with the excellent livestream from the Department of Health, what challenges might be in store for global dementia policy in the near future.
My account is @dementia_2014
The final G8 Summit Communique is here.
The G8 Summit Declaration is here.
There’s a bit of a problem with global dementia policy. The patients, carers, families, businesses, corporate investors, charities, media, academics (including researchers) politicians, all appear to have different opinions, depending on who you speak to.
Peter Dunlop, a man with dementia of Alzheimer type, received a standing ovation after his speech. He had explained his reactions on receiving a diagnosis, and how he has tried to continue enjoying life. He had been a Consultant Obstetrician and Gynaecologist.
Peter Dunlop: “I continue to enjoy life and fishing” – Moving testimony that a good life with #dementia is possible! #G8dementia — Alzheimer Europe (@AlzheimerEurope) December 11, 2013
Peter Dunlop had a standing ovation from #G8dementia – NEVER underestimate the power of the lived experience of dementia — Beth Britton (@bethyb1886) December 11, 2013
The people with dementia who appeared did indeed remind the audience, including Big Pharma, why they were there at all. Trevor Jarvis talks about person-centered care and need for doctors to fully understand the disease. What an eloquent gentleman. #G8dementia — Romina Oliverio (@RominaOliverio) December 11, 2013
And that there was more to life than medications: AE Chair Heike von Lützau-Hohlbein highlights role of self-help movement and successful advocacy work #G8dementia — Alzheimer Europe (@AlzheimerEurope) December 11, 2013
And this was sort-of touched on even by the Prime Minister:’Today is about three things: realism, determination and hope.’ @David_Cameron #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
And personhood was not completely lost on David Cameron MP:’… this is about allowing people to live well with dementia, and with dignity’ @David_Cameron #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
And this was indeed music to the ears of people like me, and countless of persons with dementia, their carers, friends and relatives, for example:
Cameron: It’s not just about finding a cure, it’s also about helping people with dementia to lead more fulfilling lives. #G8dementia — DeNDRoN (@nihrdendron) December 11, 2013
Elephant in the room according to @marcwort is the number of people with #dementia in developing countries #G8dementia — Alzheimer Europe (@AlzheimerEurope) December 11, 2013
And the carers were listening carefully too..! listening for David Cameron to tell us some good news for those living with dementia now #G8dementia — Dementia Skills (@Dementiaskills) December 11, 2013
There was some concern aired that the volunteers and charities would been seen as a valid alternative for a properly supported health and social care system. Whilst everyone agreed that ‘dementia friends’ and ‘dementia friendly communities’ were worthy causes, everyone also agreed that these should not replace actual care.
Please don’t defer the responsibility to volunteers and charities – health and social care need to step up #G8dementia #DAACC2A — DAA Carers Action (@DAAcarers) December 11, 2013
Part of the aim of today was to foster of culture of diminishing stigma. And yet the media had been full of words such as ‘cruel disease’, ‘robs you of your mind’, ‘horrific’. So the politicians seem conflicted between this utter armageddon and wishing to destigmatise dementia, with generally pitiful results.
Some of the language in the last 24 hours has indeed been truly diabolical. I took a break to watch the main news item on the BBC, and Fergus Walsh was heading up the main item on dementia with extremely terrifying language.
#G8dementia I was going to keep track of how many times the word “Fight” was used today. I have long since lost count! #militarymetaphors — Peter Gordon (@PeterDLROW) December 11, 2013
But the Summit kept on reverting to the ‘real world’, pretty regularly though.
A pervasive theme, brought up by many health ministers and other interested parties, was how dementia carers themselves needed supported. Dr Margaret Chan even later in the day spoke about a new online resource for carers, which would be fantastic.
“Dementia carers also need our support.” Dr Chan @WHO #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
‘We’re going to develop an online resource to help carers.” Dr Margaret Chan @WHO #G8dementia This is indeed brilliant news. — Living Well Dementia (@dementia_2014) December 11, 2013
An aspect of why this situation had arisen was not really explained. Prof Martin Rossor, Honorary Consultant for the Dementia and Cognitive Disorders unit at Queen Square, described the dementia issue as ‘a wicked problem’ on the BBC “You and Yours”. However, Dr Margaret Chan from WHO was much more blunt.
“This is yet another case of market failure.” Dr Margaret Chan @WHO #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
Big Pharma had failed to ‘come up with the goods’, despite decades of trying. Dr Chan: In terms of a cure (for #dementia), or even treatments that can modify the disorder or slow its progression, we are empty-handed — WHO (@WHO) December 11, 2013
But few speakers were in any doubt about the societal impact of dementia, though much of the media resorted to scare tactics as usual in their messaging.
London-G8HealthMinisters on dementia. One of the most important challenges for ageing societies.Huge human,social and economic impact.#OECD — Yves Leterme (@YLeterme) December 10, 2013
The speakers on the whole did not wish to discuss how care for people could be reconfigured. The disconnect between the health and social care systems is clearly a concern in English policy. And indeed this was even raised.
Integrated approach for the delivery of services bridging health and social care is needed, says @yleterme #G8dementia — Alzheimer Europe (@AlzheimerEurope) December 11, 2013
All was not lost regarding wellbeing.
Hazel Blears, Labour MP for Salford, explained how her mother was living with dementia, so it was vital that policy should do everything it could do to help people live with dementia.
“We need to find the evidence for non-pharmacological interventions as well.” @HazelBlearsMP #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
I first met the Salford Institute for Dementia, a brand new account, for the first time, which was one of the highlights of my day.
Salford Institute for Dementia launched to use research to improve the lives of people with dementia #G8dementia http://t.co/BgDw3X9Xw9 — Inst for Dementia (@InstforDementia) December 11, 2013
Although not pole position compared to ‘cures’ and ‘disease modifying drugs’, it was clear that the #G8summit were keen to support assistive technology, telecare and telemedicine. This could be in part due to the generous research grants from various jurisdictions for innovation, or it could be a genuine drive to improve the wellbeing of persons living with dementia.
‘Homecare is arguably one of the best means of care because of quality of life – we should all think of innovative ways to keep ppl at home’ — Anna Hepburn (@AnnaHepburnDH) December 11, 2013
At just before lunchtime, I suddenly “twigged it”.
I must admit I was angry at myself for having been “slow on the uptake”.
I now understand what this ‘data sharing’ drive is about. It’s for DNA genomic collaboration to develop personalised treatment. #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
As it was, the discussion appeared to swing periodically between two ends of an extreme during the course of the day. At one end, the discussion was about ‘big data’ and ‘open data’ sharing.
Vivienne Parry , then said how she preferred the term ‘safe data’ to ‘open data’, but Twitter was at that point awash with queries as to whether a rose by any other name would smell as sweet?
@vivienneparry has hit the nail on the head; ‘unsafe’ data sharing could be perceived as reducing risk for corporate investors. #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
People conceded the need for persons and patients voluntarily to contribute to these data sets, and for international organisations such as WHO to attempt to formulate standardised harmonised templates for these data. At the other end, people were very keen to talk about genetic information, presumably DNA, being the subject of DNA genomics data scrutiny at a personal level.
Also, the discussion itself swung from personal tales (such as Beth Britton’s) to a discussion of looking at societal information as to what sorts of data clusters might show ‘susceptibility’ in their genetic information decades before the onset of clinical dementia. Big data, like 3D printers, has been identified as ‘the next big thing’ by corporates, and it’s no wonder really that big data should of interest to big Pharma corporates.
Having failed spectacularly to have produced a cure or disease-modifying drugs across a number of decades, Pharma are left with two avenues. One is that they look at the individual response to therapy of drugs at a single case level using radio-active binding studies (radio-ligand binding studies), and monitor any slowing of build-up of abnormal protein in the brain as a response to treatment. How much this actually benefits the patient is another thing.
Or Big Pharma can build up huge databases across a number of continents with patient data. Researchers consider this to be in the public interest, but patients are clearly concerned about the data privacy implications.
Here, it was clear that Big Pharma could form powerful allies with the charities (which also acted as patient groups):
“Data sharing is absolutely essential to make the advances needed across the world.” Harry Johns, Alzheimer’s Association #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
And of course this agenda was very much helped by Sir Mark Walport being so enthusiastic about data sharing. Having been at the Wellcome Trust, his views on data sharing were already well known though.
“There are concerns about ‘Big Data’ around the world.” Sir Mark Walport CSO #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
If it were that regulators could allow data sharing more easily, justified presumably on public policy grounds such that freedom of information was more important than data protection according to the legal doctrine of proportionality, this plan could then considerably less risky for corporate investors wishing to invest in Big Pharma.
Andrea Ponti from JP Morgan gave this extremely interesting perspective, which is interesting given the well known phenomena of ‘corporate capture’ of health policy, and ‘rent seeking behaviours’ of corporates.
The G8 have a great opportunity to altering the risk and return ratios, important for investors.” Andrea Ponti @jpmorganfunds #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
It has been argued that waiting for valid consent from the patients would take too long, so presumed consent is more of a practical option. However, this ethically is an extremely tricky argument. The Pharma representatives were very keen to emphasise the ‘free flow’ of data, and the need to ‘harmonise regulation'; but they will be aware that this will requiring relaxing of the laws of more than one country.
And so, during the course of the day, the agenda of Big Pharma became clear. They intended to be tough on the lack of cure for dementia, and tough on the causes of that cure. Some might say, that, as certain anti-patent drugs come to the end of their patents, they have suddenly converged on this idea to tackle dementia, as it is a source of profitability to enhance shareholder dividend. They now need new business models to make it succeed (and various charities and research programmes which benefit from this corporate citizenry might be able to make it work too.)
“We have introduced approaches which encourage personalisation and individualisation of care.” Madame Marisol Touraine #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
But during the course of the day those ‘pesky’ tweets about person-centred care kept on coming…
As #G8Dementia summit about to start – see the person not the diagnosis with @SCIE_socialcare award winning film http://t.co/PJ58m6xWB9 — Andrea Sutcliffe (@Crouchendtiger7) December 11, 2013
Some of the tales were truly heart-breaking.
“I lost friends. Well I say friends. If they can’t cope with a diagnosis of dementia, they’re not really friends.” @BethyB1886 #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
But I was happy because Beth was happy at the reception of her film. She is so utterly passionate, and totally authentic, about the importance of her father who had dementia. It was a privilege for us to see how well the film had been received by all there at the #G8summit.
Our montage film, featuring people with dementia & carers (inc me), well received at #G8dementia — Beth Britton (@bethyb1886) December 11, 2013
And those pesky tweets kept on coming…!
Watch our award winning #SocialCareTV film ‘Getting to know the person with #dementia‘: http://t.co/tivbpYkb8Z — SCIE (@SCIE_socialcare) December 11, 2013
But indeed there was a lot to be positive about, as research monies if well spent could provide a cure or disease-modifying drugs. Big Pharma and the researchers know that they are not only trying to tackle the big one, the dementia of the Alzheimer type, but also other types such as the vascular dementias, frontotemporal dementias and diffuse Lewy body disease.
EU announces Horizon 2020 call dementia & neurodegenerative disease in 2014/2015 €1.2 billion #G8dementia @isgtw @martinrossor — DeNDRoN (@nihrdendron) December 11, 2013
Beth’s input today was invaluable.
“I would really like to make a plea, on behalf of the delegates, for non-pharmacological interventions. Thank you.” @BethyB1886 #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
And Dr Peter Gordon loved it!
@bethyb1886 and @HazelBlearsMP well said, both of you. We need balance in our approach. Your voices matter so much #foryourfolk — Peter Gordon (@PeterDLROW) December 11, 2013
But the best comment of the day must certainly go to Dr Margaret Chan, a V sign to those obsessed with Big Data spreadsheets and molecular biologists looking at their Petri dishes:
‘We’re going to develop person-centred care, not talk about people as collections of organs or diseases’ Dr Margaret Chan @WHO #G8dementia — Living Well Dementia (@dementia_2014) December 11, 2013
In summary…
It smelt like a corporate agenda.
It looked like a corporate agenda.
It sounded like a corporate agenda.
And guess what?
Related articles
- The G8 Dementia Summit cannot just be about “Pharma-friendly communities” (livingwelldementia.org)
- All stick and no carrot? How much diagnosis, but how much actual care, of dementia? (livingwelldementia.org)
- The #G8Dementia Summit – hopefully a chance for real campaigners, not an international trade fair (livingwelldementia.org)
- Dementia cure ‘within our grasp’, says David Cameron (standard.co.uk)

The #G8Dementia Summit – a curious lack of a person-centred approach in the research strategy

David Cameron should be given credit for making ‘dementia’ the topic for discussion of the G8 on 11th December 2013. But the event runs the risk of being a trade fair for the pharmaceutical industry, becoming increasingly desperate to prove their worth in dementia and society.
However, it is widely acknowledged that cholinesterase inhibitors, drugs that boost levels of acetylcholine in the brain to improve attention and memory, have a modest effect if that in the majority of patients with early dementia of the Alzheimer type (‘dementia of the Alzheimer type’). There is no robust evidence that they slow down disease progression in humans from human studies of patients.
Many senior academic experts feel conversely that there has been insufficient attention put into interventions that actually do help people to live well with DAT. Such interventions include improving the design of the home, design of the built environment (including signage and pavements), non-statutory advocacy, dementia-friendly communities, assistive technology and ambient living innovations.
On Wednesday 4th December 2013, a ‘research summit’ was held for the press for “research into dementia”. The main focus of this research summit was how can one best predict who will get dementia or when, do we even know what causes dementia yet, what “cures” are there in the pipeline, what can be done to prevent dementia, what obstacles are pharmacological researchers facing, does Pharma have sufficient resources, and what needs to be done to make the Dementia Summit a success.
The focus of this ‘summit’ into ‘research into dementia’ was not living well with dementia, which is a gobsmacking tragedy for all those involved in promoting living well with dementia.
What is overwhelmingly absent is a ‘person centred approach’ which has been a major force for good in contemporary dementia care in England.
The panel members, according to the brief, were: Dr Doug Brown, Director of Research and Development, Alzheimer’s Society; Prof Nick Fox, Professor of Neurology, MRC Senior Clinical Fellow, Institute of Neurology, University College London; Prof Simon Lovestone, Professor of Old Age Psychiatry, Director of NIHR Biomedical Research Centre for Mental Health at the South London and Maudsley NHS Trust and Institute of Psychiatry, King’s College London and Lead for the Translational Research Collaboration in Dementia (a network of 6 centres established by the NIHR); Prof Peter Passmore, Professor of Old Age Psychiatry, Queen’s College Belfast and Lead for Dementia for The British Geriatrics Society; and Dr Eric Karran, Director of Research, Alzheimer’s Research UK.
To show how little there was on wellbeing, and discussing innovative ways to allow people to live well with dementia, here’s the official write up from the BMJ this week:
“Nick Fox, professor of neurology and a Medical Research Council senior clinical fellow at the Institute of Neurology at University College London, said, “We should be asking the G8 collectively to double the research spending on dementia within five years.
“And I think there is a lovely equitable way of looking at this. We ask the G8 countries to commit 1% of their dementia costs to add another doubling of research spending within 10 years.”
Brown said the aims of the research were to enable more accurate and timely diagnosis of dementia; to create disease modifying treatment to try to stop, slow, or reverse the condition; and to find drugs to treat the symptoms. Most importantly, he said, researchers needed to understand how dementia developed to enable the risk to be reduced and onset of dementia to be prevented or at the very least delayed. “If we could delay the onset by five years we could probably cut the numbers of [people with] dementia in half,” he said.
Fox said that past trials of treatments had concentrated on people with symptoms of the disease, which was “like trialling chemotherapy when people are already in a hospice.” Now, he said, treatments were beginning to be tested in people who were at higher risk of dementia because they had a family history or other genetic risk factors or because scans had shown early features of the disease.
Scans and other techniques could then be used to track the effects of treatment before symptoms appeared. “Only if we can identify people where we can see whether our therapies are having an effect will we ever make progress,” Fox said.
Peter Passmore, professor of old age psychiatry at Queen’s College Belfast and the British Geriatrics Society’s lead on dementia, said that as more was known about the mechanism of dementia, researchers were looking at drugs licensed for other conditions that might impinge on those mechanisms. “That’s cheaper drug development: those drugs are off patent,” he said.”
Many thanks to @sam4wong for sharing this with us on Twitter this morning.
Sadly, this representation of research for #G8dementia has taken on more of an appearance of a corporate international trade fair, which is a crying shame. This is, ironically, in the week that the World Trade Organization has apparently agreed its first-ever global deal aimed at boosting commerce.
A trade fair (trade show, trade exhibition or expo) is an exhibition organised so that companies in a specific industry can showcase and demonstrate their latest products, service, study activities of rivals and examine recent market trends and opportunities. In contrast to consumer fairs, only some trade fairs are open to the public, while others can only be attended by company representatives (members of the trade, e.g. professionals) and members of the press, therefore trade shows are classified as either “Public” or “Trade Only”. However, the G8 next week would be at considerable risk of being hijacked by market forces, if it were not for the valiant efforts of the Department of Health and people who have devoted their lives to raising dementia awareness too. Trade fairs are helpful for marketing of products to a wider audience.
James Murray-White (@sky_larking) is a film-maker, and campaigns perennially for raising dementia awareness. James announced yesterday that he was proud to be part of a central network of dementia ‘activists’ on Twitter, but had just reported on the same media network that he had recently been refused ‘press accreditation’ for #G8dementia.
Earlier this year, filmmakers and scientists came together at this event to increase the public understanding of dementia. This event comprised series of short films about dementia, curated by Murray-White, will precede a discussion with researchers from the University of Bristol and other institutions supported by @AlzheimersBRACE, a local charity that funds research into Alzheimer’s disease and other forms of dementia. Panel speakers included: Professor Seth Love (Professor of Neuropathology); Laura Palmer (South West Dementia Brain Bank Manager); James Murray-White (filmmaker).
However, all is not lost, by any means. Beth Britton (@BethyB1886) will be participating in a short film for #G8dementia. Prof Alistair Burns (@ABurns1907), the Clinical Lead for Dementia in England, has written of Britton:
“Beth Britton has been a breath of fresh air in the discussions and debates around dementia. She brings a clarity of thought and originality of ideas which I have always found very refreshing and helpful when considerations and discussions of the importance of people with dementia and their carers are concerned. She has a unique writing style and a gifted ability to convey ideas and experiences”
Beth is one of the U.K.’s leading campaigners on dementia. Her experience of supporting her father, who was living with dementia, and her professional background, give her unparalleled insight into effective ways of campaigning for change, it is widely felt.
There are people who are simply interested in individuals with people – the person not the drug. For example, Lucy Jane Masters (@lucyjmasters) is a dementia nurse specialist, advocating for change, an educator, and primarily passionate about that person with dementia and those who care for him or her.
Alistair has for long time emphasised the importance of “a timely diagnosis”, rather than an “early diagnosis”. This is very much in keeping with the notion that the potential diagnosis should be offered at a time personally appropriate to any particular individual. Alistair also believes, in his rôle as part of NHS England, that there should be a reasonable level of “post-diagnosis support”. Academics generally agree that the tenure of Alistair as the National Lead for Dementia in England has been a very successful experience for all involved.
There are few people as inspirational too as Norman McNamara, who has campaigned tirelessly to dissolve the stigma which can surround dementia. He can be very easily found on Twitter for example (@NormanMcNamara). McNamara has written poignantly about his own personal experiences of ‘living with dementia’.
Sally (@nursemaiden) was a senior nurse, but likewise now promotes heavily wellbeing in dementia, with her father with dementia of the Alzheimer type having passed away on 1st September 2012.
And it truly is an international ‘effort': Kate Swaffer (@KateSwaffer) in Australia – who has just met up with Gill Phillips who advocates ‘paths to personalisation’, has written brilliantly about her experiences of the dementia diagnosis.
Indeed, it would not be hyperbolic to say that many people have given up much free time into the world of the dementias, as a vocation. Lee (@dragonmisery) has produced an incredible information provision website for carers of people with dementia, and this has advanced the policy plank promoting choice and control in wellbeing.
Twitter has been particularly successful at giving people a voice at last. Charmaine Hardy (@charbhardy) is one of the most prominent members of this very close community. Her profile reveals that her husband, whom she adores, has a rare dementia known as primary progressive aphasia. Anyone following Charmaine knows exactly the emotional intensity of someone caring for somebody with dementia.
Likewise, Thomas Whitelaw (@TommyNTour) has literally been ‘on tour’ talking with amazing authentic emotion, affectionately, about his mother, Joan Whitelaw, who had been living with dementia.
So why such a focus on pharmacology?
Why so little on ‘person centred care’?
This glaring omission of person centred care in #G8 dementia apart from representations below is utterly embarrassing and humilating for the thousands of researchers and practitioners who work in this area. @MrDarrenGormley‘s award-winning blog is a most useful introduction to this area.
And, although deeply enmeshed in the English health policy which has sometimes been far from controversy, the efforts of the Department of Health itself have been most impressive.
Anna Hepburn (@AnnaHepburnDH) is Digital Communications Manager for Social Care at the Department of Health. Anna is well known to be genuinely interested in the views of people living with dementia, and those closest to them.
Anna remarked recently,
“When people with dementia and their partners were invited to the Department of Health recently, there was one simple statement that stuck in my mind: “We are still people”. It came as a bit of a shock coming from one of the articulate and funny people gathered round the table. But it says it all about the misconceptions and stigma surrounding dementia.”
Anna Hepburn continued,
“On 18 November, I had the privilege of meeting more people with dementia, as well as current and former carers of people with dementia, who came to London to make short films to show at the G8 dementia summit. This is so we can bring their voices – and the reality of dementia – into the room on 11 December.”
But as a result of the research summit and other efforts from the media and select researchers, the headlines have been rather sensational and sadly all too predictable, viz:
“Unprecedented breakthrough in the hunt for a dementia drug within ‘five years'” (Independent)
“G8 ministers warned to prepare for global dementia ‘time bomb’” (Times)
“Monthly injection to prevent Alzheimer’s in five years” (Telegraph)
“Jab to slow Alzheimer’s ‘is just five years away': Monthly treatment could be given a decade before symptoms” (Daily Mail)
“Dementia cases ‘set to treble worldwide’ by 2050” (BBC)
The last one has been the most difficult for real experts in the research community with real knowledge of the problems facing international research.
On the other hand, Mr Jeremy Hughes, chief executive of the UK’s Alzheimer’s Society, according to that final BBC report cited above, said: “Dementia is fast becoming the biggest health and social care challenge of this generation.”
“We must tackle dementia now, for those currently living with the condition across the world and for those millions who will develop dementia in the future.”
There has been much media interest in improving diagnosis rates in England, driven more by the dementia charities than public health physicians or GPs. Whilst undoubtedly a ‘cure’ for dementia would be wonderful, it is rarely reported that dementia rates are in fact considered to be dropping. Medical doctors such as Dr Peter Gordon (@PeterDLROW; a NHS Consultant Psychiatrist) and Dr Martin Brunet (@DocMartin68; a NHS General Practitioner) have been invaluable as “thought leaders” in forging ahead with an evidence-based approach to this complex issue, cutting through the media garb and spin (and promotional copy).
Very recently in the prestigious New England Journal of Medicine, it was reported that, “Although demographics will drive an increase in the number of dementia cases, recent reports — generally based on population-based community studies or survey data — point to declining age-specific prevalence or incidence rates among people born later in the first half of the 20th century”
You can follow live digital coverage of the G8 dementia summit on the Dementia Challenge site on 11 December 2013. Well done to all those involved, particularly the grassroots campaigners, Anna Hepburn, and the Department of Health!

Are individuals living with dementia “recipients” of care?
Language is very important. Only this week, the media was stuffed full of talk of dementia being a ‘horrible disease’, and people ‘suffering’.
A recent Telegraph article cited, “Health Secretary Jeremy Hunt says it is “utterly shocking” that only half of people suffering from dementia are being formally diagnosed.”
Society has a certain image of dementia. It really is no use denying that this image is horribly negative, and feeding on this fear can be low-hanging fruit for raising funds through charity.
In this scheme of thinking, those with the dementia are only viewed through the prism of their illness, and this is often reduced to the image of its last and most tragic phases.
It is as if as soon as a diagnosis of a progressive dementia is made, the person in question, it is perceived by the rest of society, automatically becomes incapable of taking any autonomous decisions, loses his/her personality and identity and immediately needs to be cared for.

In reality, however, this illness can develop quite slowly: between the moment when it is diagnosed and the terminal phase, there may be years of development. Moreover, people living with the illness can rarely have the opportunity to express their thoughts and feelings about it: there is communication about them, but only rarely with them. The individual sadly disappears behind the blanket label of an illness.
The term “suffering”, however, sounds negative, and does not support the concept of “personhood”, and certainly does not fit with a philosophy of “hope” and “wellness”.
The way the NHS has latterly been structured as a market also reinforces this customer-supplier master-servile relationship. Dementia care is a ‘service’ you can pay for, with or without a personal health budget.
The dominant notion itself that the need of people with dementia to socialise should be met by “services” is disempowering, for the concept of service incorporates the notions of “providers” and “recipients”; of the “helpers” and “the helped”, of “us” and them”.
These notions further perpetuate the stigmatising assumption that people with dementia are only able to participate in relationships as “receivers”, and that relating to them is a problem for those who do not have the disease: they further advance the widespread perception that people with dementia are, essentially, a “burden” on their families and society.
This term “burden” can perhaps help validate the ‘burden’ some caregivers experience, but should not be assumed and should be avoided when speaking in generalities such as public presentations.
This language and terminology are in desperate need of change, and the prevailing perception of people past the first stages of dementia as just receivers of care, and users of services, needs drastic reframing.
The truth is that, as the symptoms of the disease progress, people with dementia can still play an active role in society, if provided with support, and this support can very often be provided by fellow citizens, rather than by professionals paid to deliver a service.
The purpose of person-centred language is to recognise the impact of language on thoughts and actions, to ensure language does not diminish the uniqueness and intrinsic value of each person.
Personhood is pivotal. This is the standing or status that is bestowed upon one human being by others in the context of relationship and social being. It implies recognition, respect and trust.
The aim is to create the positive conditions where the person can live without stigma; where people are treated with warmth and authenticity, listened to without judgment and are given opportunity for self-expression.
There are, however, ways to ‘reframe’ this debate.
Framing is a fast developing concept, as much in communication sciences as in other disciplines. This is partly due to the fact that it is a rather flexible approach that lends itself to many applications.

When there is a question relating to knowing how a particular subject is presented, in the media for instance, framing immediately springs to mind.
Instead of painting the illness as a homogenous and unchanging totality, it would be preferable to place the accent on its progressive and developmental nature.
One can put the accent on continuing to be a real person despite the decline due to the illness: acknowledge the personality, the identity and the life journey of those with a progressive dementia.
One can also develop empowerment and social inclusion with people with a progressive dementia. Such individuals are more than passive and dependent consumers of help and care services. They have resources that should be mobilized. The principle of inclusion implies that society is composed of all its citizens. However, this needs competent leadership.
Let those who living with dementia speak. It will provide others with one of the most powerful counter-examples in relation to the current dominant image, which often makes the individual disappear behind his/her illness.
Let your respect for those living with the dementia be obvious in what you have to say.
It is useful also never to forget that people with Alzheimer’s disease also have their own life story, their own personality and character. This is because their long-term memories are relatively preserved, due to a phenomenon first characterised by the French neurologist Ribot in the 1880s. Enable these aspects to be expressed too.
Those who disseminate messages, especially via texts designed to influence people, may deliberately choose a frame that the reader is supposed to pick up and appropriate so as to henceforth view reality in this way.
Given that frames form part of any culture, many of them are common to both the sender and the recipient of a given message.
The question of whether framing is a conscious process remains open to discussion: how far will the writer of a given text deliberately choose a frame that serves his own interests?
As we approach the G8 leading on the subject of what is important in dementia diagnosis, research and care, it is all the more important that we frame the discussion properly.
There are so many stakeholders in English dementia policy, it can be quite uncertain know where the current dementia policy has come from.
David Cameron has often argued that ‘it is not where you’ve come from, it’s where you’re going to’. If one of the goals is destigmatising dementia in society, how we articulate the present debate today is vital to our progress tomorrow.
This means not talking about ‘horrible’ and ‘suffering’ in a way as to encourage ‘moral panic’.
This means treating people with dementia, living at all stages with any particular condition, with the dignity they deserve; this will enormously help carers too.
