Home » Posts tagged 'Decisions'
Tag Archives: Decisions

Decisions in different types of dementia
Decisions are fundamental to our lives.
Decision making is a fundamental and complex skill which is crucial at any age. We all have to face decisions regarding their health care, medical treatment, retirement, housing, transport, and finances, for example.
We not only have to consider the benefit of a decision for their current living situation, but also to anticipate the consequences of decisions of such actions in the nearer and farer future. We need to hold the decision in my memory for long enough to think through strategically the options, and be able to action an outcome.
Everyday life requires numerous and fast decisions. Often these decisions have an uncertain result. Wrong decisions may thus have severe consequences in several domains.
Disturbances in an ability to make decisions or to anticipate the possible consequences of decisions can result in massive problems.
In the last decade in cognitive neuroscience and cognitive neurology, there has been an increasing interest to investigate neural basis of decision-making abilities and disturbances both in healthy subjects and to people where there has been some disruption.
But we have been able to build up a coherent picture of this using neuropsychological and neuroimaging techniques.
An assessment of cognitive deficits in neurodegenerative diseases has focused so far almost entirely on memory, language, attention, visuospatial perception and executive functioning (Gleichgerrcht et al., 2010).
In the past decade, however, the study of decision-making in these conditions has increased, prompting the development of new tasks that have enabled this cognitive process to be readily assessed. In clinical practice, it is not uncommon to find early persons with behavioral-variant frontotemporal dementia (bvFTD) who, to a considerable extent, are intellectually unimpaired, while relatives and caregivers depict a strikingly different picture: they claim that these patients show severe changes in their behaviour and real-life decision-making skills (e.g. Rahman et al., 1999; Manes et al., 2011).
The literature has so able to identify the orbitofrontal, anterior cingulate, and dorsolateral prefrontal cortices as being critical to decision-making (Rosenbloom, Schmahmann and Price, 2012).
A schematic view of the important neural substrates proposed by Rahman and colleagues (Rahman et al., 2001) is shown in Figure 1.

Rahman and colleagues showed that patients with behavioural variant frontemporal dementia exhibited a profile of risk-taking, not impulsive, behaviour in decision-making, suggestive of dysfunction in the ventromedial prefrontal or orbitofrontal cortex. Kloeters and colleagues (Kloeters et al., 2013), fourteen years later, published results showing that atrophy in the orbitofrontal cortex and amygdala correlated with performance on the Iowa Gambling Task used in their study to examine decision-making.
A large proportion of human cognitive social neuroscience research has focused on the issue of decision-making thus far.
Impaired decision-making is a symptomatic feature of a number of neurodegenerative diseases, but the nature of these decision-making deficits depends on the particular disease.
Once you’ve met one person with dementia, you’ve met one person with dementia. Each person with dementia will have a cognitive profile according how far progressed the condition has reached, and the extent to which functional problems are perceived. This might depend on the likely diagnostic category in which a patient living with dementia finds himself or herself.
Examining the qualitative differences in decision-making impairments associated with different neurodegenerative diseases provides potentially valuable information regarding the underlying neural basis of decision-making.
A good account of decision-making in different neurological conditions including dementia is provided by Brand, Labudda and Markowitsch (2006).
Figure 2 shows a schematic view of some of the key processes.

The features of their model are as follows.
General problem solving strategies, also stored in long-term memory, need to be recalled in order to evaluate which strategy seems to be appropriate in order to decide advantageously. The recall of this information, including personal autobiographical experiences and general strategies that have been developed during life, is triggered and controlled by executive components, for example cognitive flexibility.
In working memory, the features of the current decision and the retrieved information from long-term memory are combined to generate or initiate a current decision strategy that guides the decision.
In this process, “somatic markers”, which means biasing signals from the body or mental representations of them, can also guide the selection of an appropriate strategy. The decision itself leads to positive or negative feedback (e.g., gain or loss of a specific amount) that activates an bodily autonomic response.
The feedback – or the somatic markers, which are the results of the emotional feedback – can also result in an alteration of the information stored in long-term memory as well as – in a more direct way – the representation of somatic markers associated with comparable decisions.
The comparison of the profiles of decision making in different conditions, which can cause dementia, are arguably helpful in predicting what the person with dementia might expect. Several studies have reported altered decision-making in Parkinsons’s disease (Perretta et al., 2005) and pathological gambling has been found in Parkinsons’s disease patients with L-Dopa medication (Weintraub et al., 2006) attributing a key role to the chemical dopamine in taking risky decisions.
Recent studies also investigated decision-making in Huntington’s disease and found that learning and memory processes, rather than motivational processes, are responsible for decision-making deficits in this group (Busemeyer and Stout, 2002).
Hampton and O’Flaherty (2007, some years ago, mapped out the neural substrates of reward-related decision making with functional MRI. They identified that the combined signals from three specific brain areas (anterior cingulate cortex, medial prefrontal cortex, and ventral striatum) were found to provide all of the information sufficient to decode subjects’ decisions out of all of the regions studied.
These findings appear to implicate a specific network of regions in encoding information relevant to subsequent behavioral choice. Evidence for the important role of the orbitofrontal cortex and the amygdala in decision-making particularly under ambiguous conditions comes from a recent study by Hsu and colleagues (Hsu et al., 2005)).
Dementia of the Alzheimer type (DAT), the cause of the most cases of dementia worldwide, is typically characterised by typical structural, neurochemical and cognitive changes as the disease progresses.
Pathological changes in mild DAT affect primarily the medial temporal lobes and limbic structures (e.g., entorhinal cortex, hippocampus), and then extend to the association cortices of the frontal, temporal and parietal lobes (Braak and Braak, 1991).
Ha and colleagues have argued that the changes in DAT fundamentally alter the frames of reference for making decisions (Ha et al., 2012).
The study by Delazer and colleagues further highlighted important differences in decision-making between mild DAT patients and healthy controls (Delazer et al., 2007). Findings from the study by Sinz and colleagues are consistent with the notion that decisions under ambiguity as well as decisions under risk are impaired in mild DAT (Sinz et al., 2008). It may thus be expected that patients with mild DAT have difficulties in taking decisions in everyday life situations, both in cases of ambiguity (information on probability is missing or conflicting, and the expected utility of the different options is incalculable) and in cases of risk (outcomes can be predicted by well-defined or estimable probabilities).
The legal instrument to assess capacity through the Mental Capacity Act (2005) is very blunt. Characterising an ability of a person living with dementia to make optimal decisions is essential for giving confidence to that person (and those closest to him and her) that such risks are being managed appropriately.
It is likely that the implementation of the Mental Capacity Act will come under increasing scrutiny, in parallel with advances in decision-making research in cognitive neuroscience and cognitive neurology.
References
Braak, H., Braak, E. (1991) Neuropathological staging of Alzheimer-related changes, Acta Neuropathologica (Berl), 82, pp. 239–259.
Brand, M., Labudda, K., Markowitsch, H.J. (2006) Neuropsychological correlates of decision-making in ambiguous and risky situations, Neural Netw, 19(8), pp. 1266-76.
Busemeyer, J. R., Stout, J. C. (2002) A contribution of cognitive decision models to clinical assessment: Decomposing performance on the Bechara gambling task, Psychological Assessment, 14, pp. 253–262.
Delazer, M., Sinz, H., Zamarian, L., Benke, T. (2007) Decision-making with explicit and stable rules in mild Alzheimer’s disease, Neuropsychologia, 45(8), pp. 1632-41.
Gleichgerrcht, E., Ibáñez, A., Roca, M., Torralva, T., Manes, F. (2010) Decision-making cognition in neurodegenerative diseases, Nat Rev Neurol, 6(11), pp. 611-23.
Ha, J., Kim, E.J., Lim, S., Shin, D.W., Kang, Y.J., Bae, S.M., Yoon, H.K., Oh, K.S. (2012) Altered risk-aversion and risk-taking behaviour in patients with Alzheimer’s disease, Psychogeriatrics, 12(3), pp. 151-8.
Hampton, A.N., O’Doherty, J.P. (2007) Decoding the neural substrates of reward-related decision making with functional MRI, Proc Natl Acad Sci U S A, 104(4), pp. 1377-82.
Hsu, M., Bhatt, M., Adolphs, R., Tranel, D., Camerer, C. F. (2005) Neural systems responding to degrees of uncertainty in human decision-making, Science, 310, pp. 1680–1683.
Kloeters, S., Bertoux, M., O’Callaghan, C., Hodges, J.R., Hornberger, M. (2013) Money for nothing – Atrophy correlates of gambling decision making in behavioural variant frontotemporal dementia and Alzheimer’s disease, Neuroimage Clin, 2, pp. 263-72.
Manes, F., Torralva, T., Ibáñez, A., Roca, M., Bekinschtein, T., Gleichgerrcht, E. (2011) Decision-making in frontotemporal dementia: clinical, theoretical and legal implications, Dement Geriatr Cogn Disord, 32(1), pp. 11-7.
Rahman, S., Sahakian, B.J., Hodges, J.R., Rogers, R.D., Robbins, T.W. (1999) Specific cognitive deficits in mild frontal variant frontotemporal dementia, Brain, 1999, 122 (Pt 8), pp. 1469-93.
Rosenbloom, M.H., Schmahmann, J.D., Price, B.H. (2012) The functional neuroanatomy of decision making, J Neuropsychiatry Clin Neurosci, 24(3), pp. 266-77.
Sinz, H., Zamarian, L., Benke, T., Wenning, G.K., Delazer, M. (2008) Impact of ambiguity and risk on decision making in mild Alzheimer’s disease, Neuropsychologia, 46(7), pp. 2043-55.
Weintraub, D., Siderowf, A. D., Potenza, M. N., Goveas, J., Morales, K. H., Duda, J. E., Moberg PJ, Stern MB. (2006) Association of dopamine agonist use with impulse control disorders in Parkinson disease, Archives of Neurology, 63, pp. 969–973.

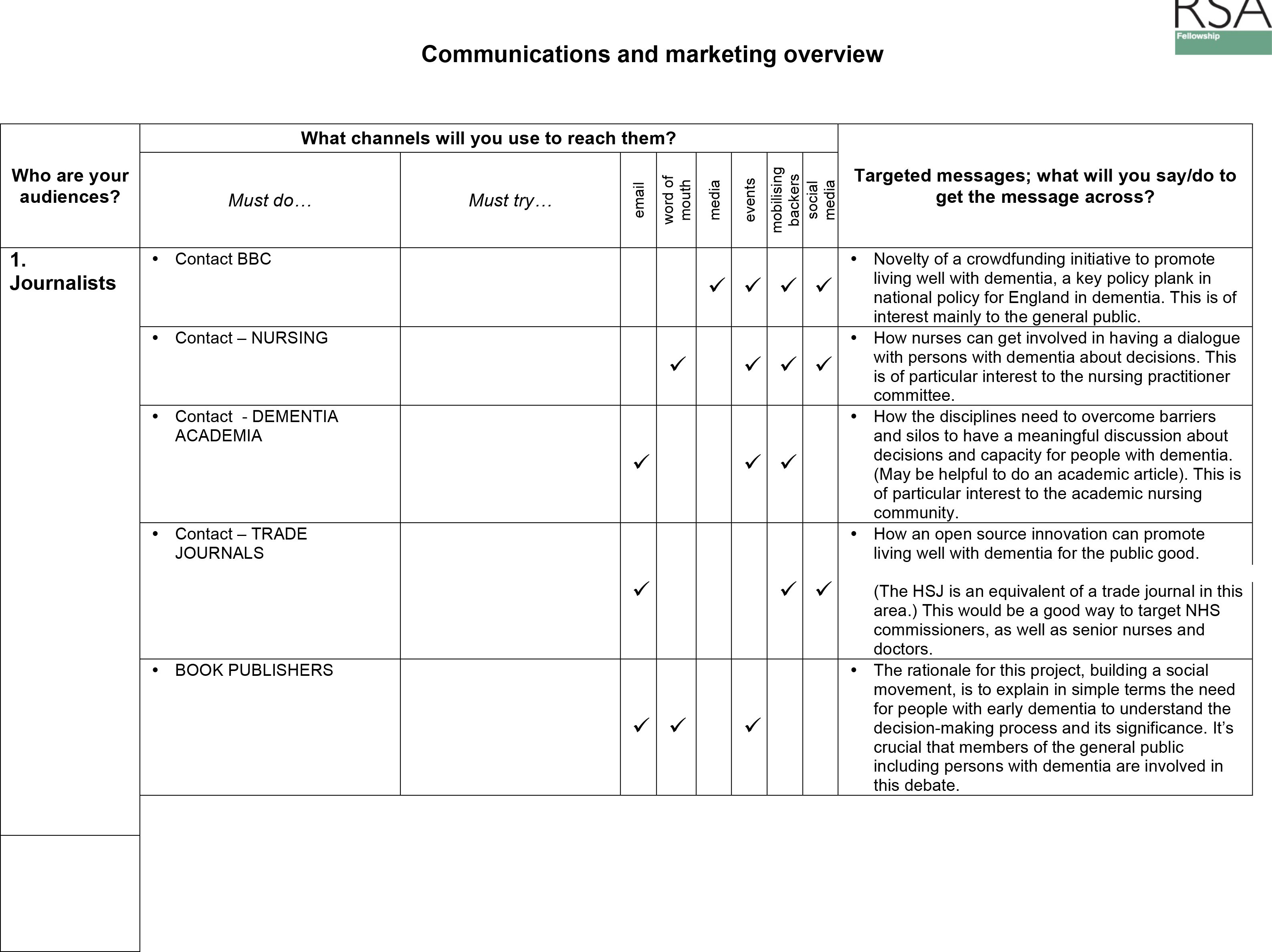
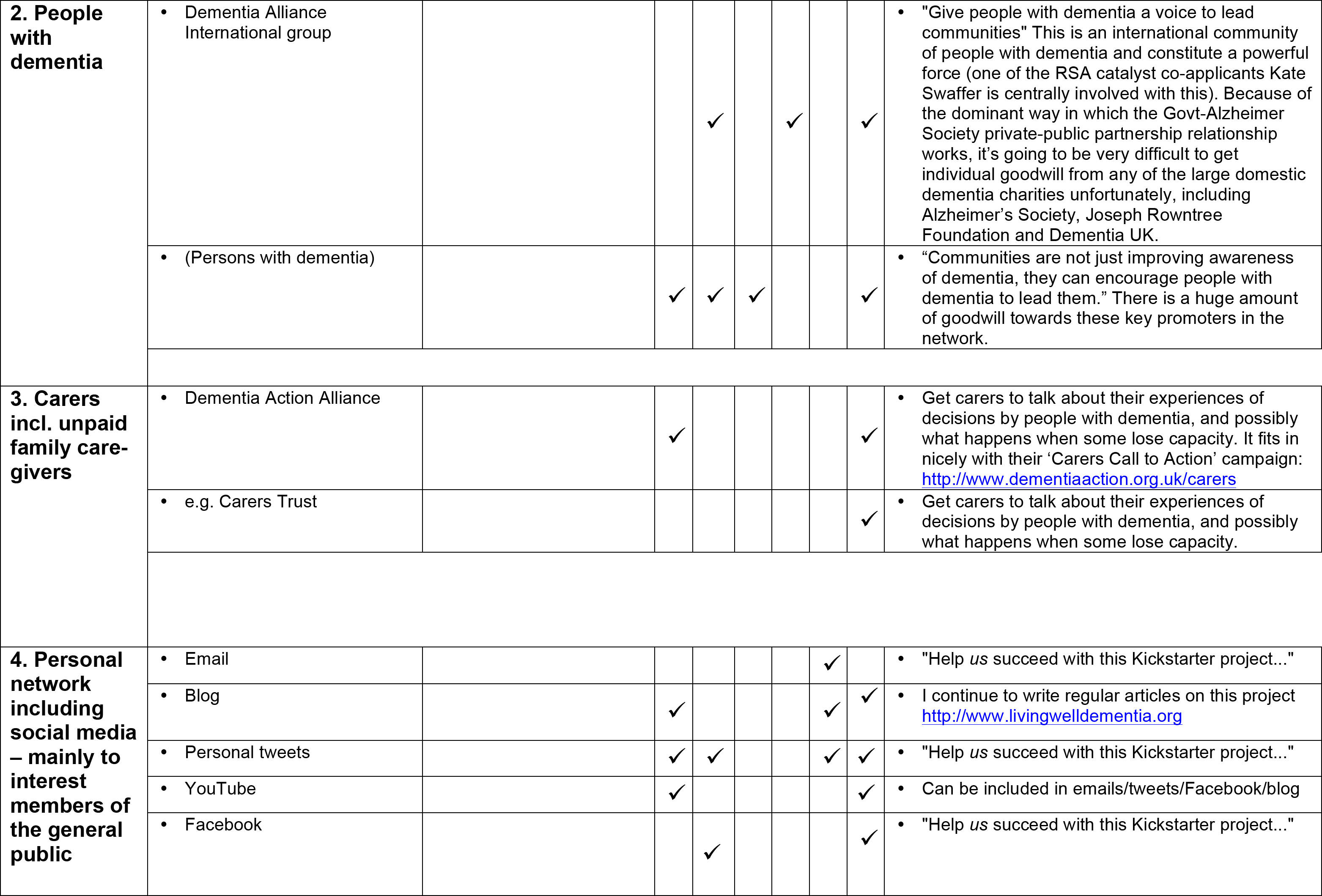
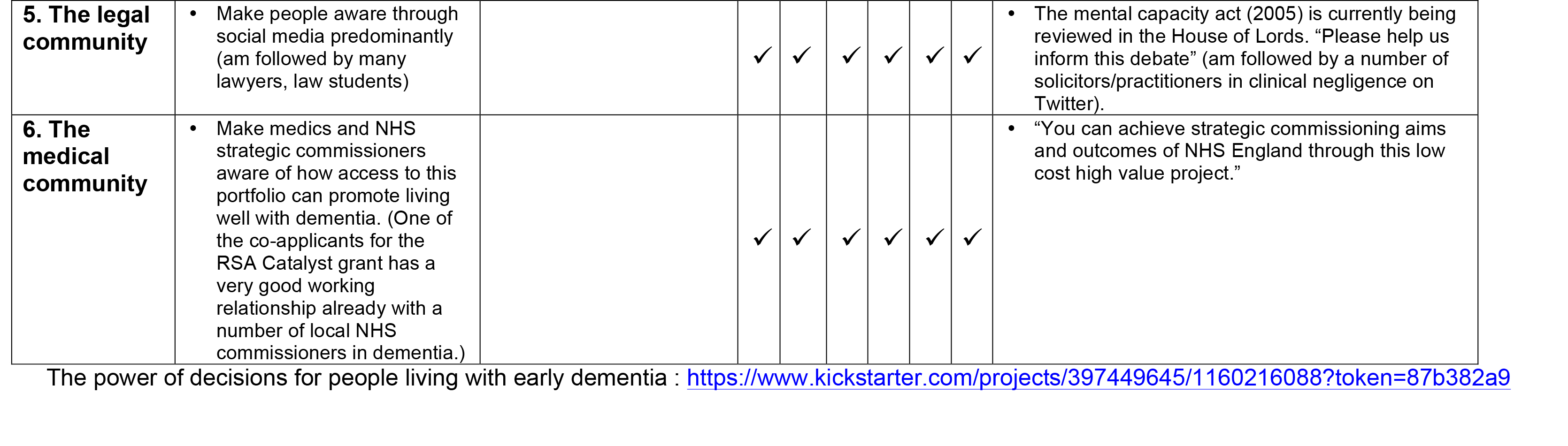
My marketing campaign brainstorming session at the RSA this morning for ‘decisions in dementia’.
We were joined by top marketing consultants this morning to advise on our crowdsourcing campaign.
The draft details of my crowdsourcing campaign, to raise awareness of decisions, the importance of decisions in dementia, and how decisions can possibly be influenced, are here on my Kickstarter page.
This campaign is not live yet.
Most marketing strategists will agree that creating customer value is fundamental to both profit-seeking companies and nonprofit organizations.
Indeed, creating superior customer value is a necessary condition for a company securing a niche in a competitive environment, not to mention a leadership position in the market.
A price signal is information conveyed, to consumers and producers, via the price charged for a product or service, thus providing a signal to increase supply and/or decrease demand for the priced item.
A large focus of our discussions was ‘market segmentation’.
Market segmentation is a marketing strategy that involves dividing a broad target market into subsets of “targets” who have common needs and priorities, and then designing and implementing strategies to target them.
Market segmentation strategies may be used to identify the target “backers”, and provide supporting data for positioning to achieve a marketing plan objective.
As a result, I might develop product differentiation strategy, so that the website I am designing fulfils diverse needs, such as for people with early dementia, journalists or NHS commissioners.
One of the leading consultants advised that for my particular project, and this is a difficulty any product-oriented kickstarting campaign, that “content is King”.
He advised me that a big problem with my pitch is that the figures asked for seemed very ‘budget’. I think, in fairness, he was concerned about my project looking too “bargain basement”.
Too cheap or too expensive can both be off-putting.
We’ve been advised to maximise use of all marketing channels, and to synchronise properly rewards to the different market segments.
This all seems very sensible.
But it’s all the same very exciting.
I hope to get hold of the makers of this short animation, based in Serbia, I think so that they can make a short animation on the importance of decisions for people living with dementia (for a stated revised budgetary cost of my output of crowdfunding campaign.)
This is by the way how I intend to maximise use of marketing channels (some details redacted.)

I have not set out to build a social movement, but I want to do this for persons with early dementia
I received this message last night.

The thing is, I don’t buy into the profoundly negative imagery of the media, including memes such as “crippling”, “horrific”, “timebomb” and “explosion”.
Whilst some people, and caregivers, are undeniably “suffering”, you can’t expect all people to agree with this particular narrative at all times, I feel.
One of the things I’ll never forget was when my Ph.D. supervisor, Prof John Hodges, received a complaint about me doing neurocognitive assessments in a person with frontal dementia back in 1997.
This type of dementia, commoner in an age group below 60, is characterised by a personality and behavioural change early on, often in the absence of deficits in thinking such as memory or perception. You need an account from someone very close to that person with dementia, as the person himself or herself can have no insight into the changes.
I remember saying to the wife of a young man with this type of dementia, “I would never have guessed that he had a dementia”. This comment had upset her very much, and by that stage I was years into my medical training.
This one event is something I’ve never forgotten in the 16 years subsequently.
I remember I literally didn’t sleep for a week, and I was profoundly upset by this. But it does lie to the heart of some of my reservations about the term ‘dementia friendly communities’. There are some people for whom you would not be able to tell they were living with dementia.
I understand the focus on memory problems in the general media, as this can be a dominant presentation in typical Alzheimer’s disease, the commonest form of dementia. But memory is only one of the cognitive functions we have.
What unites all people with dementia is that the law makes a verdict on whether they are able to make decisions. This is called legal capacity.
Decisions impact on many aspects of life, such as working out how to spend your money, or which treatment to go for in hospital.
And capacity is very topical. Not only is the House of Lords seeking to update the Mental Capacity Act (2005), but also neuroscientists currently want to know what members of the public think about their research on decisions.
This is therefore not about denying compassion or dignity for all persons with dementia. It’s about redressing a power balance, where I feel people who’ve just received a diagnosis of dementia might learn something constructive about dementia, decisions and science of how to influence decisions.
This is profoundly about having a discussion with persons with dementia.
I’ve been on the receiving end of ‘look at my website’ and I find it intensely nauseating. But I wish my website, which I intend to build with funds from a crowdfunding campaign and scientific grant bodies, to allow persons with dementia to think about their own decisions.
It’s well known in the science of decisions for example that some ‘bad’ decisions can be avoided by not following ‘hot impulses’ or following the ‘herd effect’.
So here is my explanatory video:
Whilst I have been urged to make this campaign so that ‘it touches every person with dementia’, I do also want a grown up conversation without dumbing down any of the concepts.
A lot of feedback has concentrated on the ‘social movement’ aspect of it, but I should like to say whilst I say I would like to build one, I really mean it’s important for me personally that this gathers some momentum.
And I think it will from initial feedback from persons with dementia, and even people involved in the NHS and social care.
All too easily dementia policy can have more regard to marketing and tokenism, which lends itself to commissioning ‘tick box’ culture. My campaign is not for them.
And I’ve got a bit of a shock for some people – I am determined to make a big success of it.
@legalaware @theRSAorg amazing idea – we need to do more of this in the nhs
— Pollyanna Jones (@PollyannaJones) April 2, 2014
@legalaware @tommyNtour @dementia_2014 Great video, great idea. Need more openness- dementia isn’t going to go away, so embrace opportunity
— #HelloMyNameis Pip (@pippa_dolittle) April 3, 2014
very proud of friend & colleague @legalaware who has started this important campaign in dementia wellbeing: http://t.co/2y9dmTJkW2 please RT
— James Murray-White (@sky_larking) April 2, 2014
@legalaware I have been trying to convince people the nhs needs it’s own kickstarter platform for a while. Will be great to see if it works
— Pollyanna Jones (@PollyannaJones) April 2, 2014
@legalaware @dementia_2014 looks like a really exciting project.
— Rebecca Wassall (@Bexmoxon) April 8, 2014

My plans for a crowdfunding campaign to empower decisions in people with early dementia
The power of decisions for people living with early dementia
This project is dedicated to all persons living with dementia, carers and caregivers, all other people touched by dementia past present or future, and more.
The need
Decisions are crucial to our lives. Every person is unique.
A person’s ability to make decisions is defined legally as his or her “capacity”.
The brain is fascinating. It’s also incredibly complex. Neuroscience is beginning to work out how decision-making is affected in people with early dementia.
We’ve been told by many people who’ve been diagnosed with dementia that they’re interested in how the brain makes decisions.
Dementia can happen to anyone, but we should be motivated as all members in society to encourage people with dementia to live as well as possible.
Every individual with dementia is different. There are about a hundred different types of dementia.
The aim of this project is to build a social movement to empower people living with early dementia to think about decision-making. It’s about explaining the science of decisions in early decision. This is also about inviting people including those with dementia to think about their decision-making in an exciting way, and to participate in ways of influencing them for the better.
Our idea
This project is to design a website for all to enjoy, but including people who’ve been newly diagnosed with dementia.
This will provide exciting videos about why decisions are so pivotal in understanding dementia. We hope to produce exciting creative films to explore this topic by asking a professional filmmaker, James Murray-White, with a known interest in dementia and a proven record in film making.
We will design our website is so that they can understand the science of what a dementia is and how it affects decisions. It’ll also have an interactive blog.
The website will build on the RSA’s “Social Brain” findings in “Steer” (2010), but will also make use of cutting-edge research such as Daniel Kahneman’s “Thinking fast and slow”.
People with the earliest stages of dementia can think about their decisions.
People will know about it through my Twitter (@legalaware). We’ll also set up a special new Twitter account to promote the project.
The future
People with dementia can also tell neuroscientists what they feel they should be researching, and tell lawyers what they think about “capacity”.
They can get directly involved in policy making without any middle men, in keeping with the RSA’s philosophy and values.
With being empowered to make better decisions, people with early dementia can also lead communities. They would be not just be “involved” in communities which are “friendly” to them.
We’re also hoping that as the project establishes itself it will provide a core offering in NHS packages for people living well with dementia, a key national policy priority.
Who’s behind it?
Our team consists of three people.
1. Dr Shibley Rahman FRSA – academic in dementia, with book chapters, a book, original research papers and keen blogger on dementia http://www.livingwelldementia.org
2. Dr Marian Naidoo FRSA – dementia specialist in dementia-friendly communities
3. Kate Swaffer – a person living with dementia in Adelaide, Australia; Chair, Dementia Advisory Committee at Alzheimer’s Australia; Volunteer; a powerful advocate for people living with dementia, whose blog already has a powerful international outreach.
Rewards
Please support this project.
We are trying to raise £2500.
The ‘rewards’ for participating are awesome.
Backers will get
1. For up to 50 people: £5 or more
A special name mention/shout-out on the website,
2. For up to 30 people: Pledge £15 or more
a special limited edition e-book by the authors explaining decisions, the science of how decisions are affected in early dementia, and what all people might do to influence their decision-making
3. For up to 30 people: Pledge £15 or more
a special limited edition attractive mug so that you can demonstrate your personal involvement with this project; price includes postage and packing
4. For up to 30 people: Pledge £20 or more
a special limited edition attractive T-shirt so that you can demonstrate your personal involvement with this project; price includes postage and packing.
5. For up to 30 people: Pledge £25 or more
a special limited edition attractive tote bag so that you can demonstrate your personal involvement with this project; price includes postage and packing
6. For up to 30 people: Access to special privileged areas of the website for £40 or more pledges
- we are offering access through a special username and password unlimited access to certain protected parts of the website
- there will be special information sheets about the science of decisions and early dementia, and how they can be influenced; with special access to other resources such as videos or blog articles.
- this may be especially of interest to NHS commissioners.
6. For up to 20 people: Mentions in my new book ‘Living better with dementia’ for £30 or more pledges
I have already written a well-received book on ‘Living well with dementia’ which has very good reviews. I am offering exclusively mentions for up to 20 people involved in this project special mentions in my follow-up book ‘Living better with dementia’.
7. For up to 30 people: Invitations to a special workshop afternoon for £30 or more pledges
In our special-invite only workshops, we’ll be presenting the science of decisions, and be discussing how these are affected in early dementia, and what we know from the science about what can be done to influence them.
8. Recognition as a sponsor – pledges of £100 or more
We’ll proudly recognise your contribution on our website for a year and in our promotion of this initiative, which could include in NHS commissioning rounds.
The future
A chance to shape policy through NHS strategic commissioning decisions.
Risks and challenges
We feel that this is an incredibly exciting project, concentrating on what people with early dementia can do, rather than what they cannot do.
The main risk is that our website, described above, fails to explain the importance of decisions in early dementia. We hope as well experienced authors we’ll do a very good job of it though.
But we hope the resources will have been written in a way that is easily accessible, and inclusive by experts with considerable experience in this area.
We will instruct a proficient designer of websites, with a proven track record, to make the website for us.
Our project is all about people working together.
That brings challenges to make sure enough people feel engaged, but our experience from our involvement in social media (e.g. @legalaware with 11000 followers), interested people love being engaged.
We have put our time and effort into these projects because we believe in people getting involved – with each other, with their community, with making things better.
FAQ
The RSA’s curated area on Kickstarter selects the best new ideas to help tackle social problems that its 27,000 Fellows are looking to deliver. I’m an RSA Fellow and have been selected to be a part of this. ?Visit www.kickstarter.com/pages/rsa to see more RSA-backed projects and find out more about the RSA.
Thank you.

Why I’m on a mission to explain the science of decisions to people living with mild dementia
As a person who is physically disabled, and who has a speech impediment due to a meningitis from 2007, I am more than aware of how people can talk down to you in a patronising way.
It’s why I am very sensitive about language: for example, even with the best intentions in the world, “dementia friendly communities” conjures up an intense feeling of ‘them against us’.
It’s really important to not do anything which can cause a detriment to any group of people.
If you happen to be living with a condition which could cause you to have difficulties, this is especially important.
A “dementia” might be a disability under the Equality Act, and the person you’re speaking to might not obviously to you be living with a disability – it’s a ‘so-called invisibility’.
But – I’m deadly serious this. People shouldn’t be judged on what they can’t do. We all have failings of some sort. People should be encouraged for what they can do whenever possible. I don’t, likewise, consider the need for policy to embark on ‘non-pharmacological interventions’ as if what I’m talking about is second fiddle: living well with dementia is a complete philosophy for me.
In any other disability, you’d make reasonable adjustments. I see the need to explain how decisions are made to people with dementia as absolutely no different, both under the Equality Act (2010) and morally for a socially justice-oriented nation.
The excitement about how ‘decisions’ are made was recently described in the book by Prof Daniel Kahneman, “Thinking fast and slow”.
How we hold information for long enough to weigh up the pros and cons fascinates me.
Kahnemann, and others, feel that there are two systems.
System 1 is fast; it’s intuitive, associative, metaphorical, automatic, impressionistic, and it can’t be switched off. Its operations involve no sense of intentional control, but it’s the “secret author of many of the choices and judgments you make”. System 2, on the other hand, is slow, deliberate, effortful. Its operations require attention. (To set it going now, ask yourself the question “What is 13 x 27?”

Kahneman is a hero of mine as in 2002 he was awarded the Nobel Prize for economics, but he is essentially a cognitive psychologist.
In 2001, I was awarded a PhD from Cambridge for my thesis in decision-making in frontal dementia. I was the first person in the world to demonstrate on a task of decision-making that people with frontal dementia are prone to make risky decisions, despite having very high scores on standard neuropsychological tests and having full legal capacity.
Now, one coma later following my meningitis, I have done my postgraduate studies in law, and I have become fascinated by the rather arbitrary way in which our law has developed the notion of mental capacity, based on our ability to make decisions.
People with dementia can lose their ability to make decisions, so decision-making is a fundamental part of their life. As neuroscience and law straddle my life, I should like to make it my personal mission to explain the science of decision-making to people with full capacity, and who happen to have a diagnosis of dementia.
I am all in favour of a world sympathetic to the needs of people living with dementia, but this requires from us as a society much greater literacy in what the symptoms and signs of dementia are. I am not convinced we’re anywhere near that.
In the meantime, I think we can aim to put some other people in the driving seat, and they rarely get put in the driving seat: yes, that’s right, it’s time to engage people with mild dementia in the scientific debate about how decisions are made.
Many decisions are subconscious. That’s what marketing people manipulate to make loadsamoney.

It is actually very hard to tell whether this Government’s actions are a result of a fundamentally libertarian ideology, or whether there is simply no ideology at all – they simply wish to allow their “corporate friends” to make lots of money (which as such is not an ideology). The screw-up over plain packaging in cigarettes can be interpreted at a number of different levels. One is how plausible transparency in the Government is: whilst the evidence concerning Lynton Crosby himself (and his company) is unconvincing, the lengths that international tobacco companies might go through in influencing public health policy are interesting. It could be argued that tobacco companies are simply not keen on regulation, but that does not stop Philip Morris initiating legal action at the drop of the hat. There are wider subtler inherent contraindications in the analysis of the power of the State and its rôle in public health too which will cause problems ultimately. A strong undercurrent has been the notion of “choice”, typified by Tim Kelsey’s approach to the use of data in decision-making of patients, or “customers of the NHS” as called by some. The idea that “regulation is bad” is of course fully consistent with a political philosophy from the Conservative Party, and while the Labour Party could rightly be accused of a somewhat authoritarian, “nanny state” tinge to its last attempt at office and power, the idea of the “public good” continues to gather much support in many jurisdictions.
The government has actually now mutualised its “Nudge” unit, but “Nudge” was the future once. The centrality of using behavioural insights to the Coalition government is such that it entered formal written agreement between the Conservative and Liberal parties, in the foreword by the two party leaders and their juniors:
“There has been the assumption that central government can only change people’s behaviour through rules and regulations. Our government will be a much smarter one, shunning the bureaucratic levers of the past and finding intelligent ways to encourage support and enable people to make better choices for themselves”.
Nudge is an interesting foray into consumer behaviour, and part of the problem in this is that human beings are often irrational (and certainly will make suboptimal decisions on the basis of dodgy data.) Consumer behaviour is ultimately determined by cognitive processes, such as perception, selective attention, and memory, which is why the approach to “big data” fails inherently to capture individual differences. This is a problem in planning public policy, but why should the field of marketing and economics be so interested in packaging if it does not matter? The actual evidence provides that product packaging is an important tool for suppliers to communicate with consumers.1 Tobacco manufacturers have effectively used cigarette pack design, colours, and descriptive terms to communicate the impression of lower tar or milder smoke while preserving taste “satisfaction”. Smokers’ beliefs about a given product are likely to be shaped in part by the descriptors, colours, and images portrayed on the pack and in related marketing materials.
In the US jurisdiction, “The Framework Convention on Tobacco Control” (Article 11) calls for a ban on misleading descriptors in an effort to address consumer misperceptions about tobacco products. New regulations contained in the Family Smoking Prevention and Tobacco Control Act of 2009 (FSPTCA) prohibit tobacco companies from labelling cigarette packs with terms such as light, mild, or low after June 2010. However, experience from countries that have removed these descriptors suggests that cigarette marketers manage to circumvent the intended goal of the regulation by using different terms, colours, or numbers to communicate the same messages. Specifically, recent research has shown that consumers in the United Kingdom and Canada, which have removed “light” and “mild” descriptors, perceive cigarettes in packs with lighter colours as less harmful and easier to quit compared to cigarettes in packs with darker colours. Colour is a good example of non-verbal marketing signal, which has an important influence on our daily lives. The underlying emotions that colours evoke have been cultivated since birth and vary depending on age, geographic location, and gender (e.g. blue for boys, pink for girls). Colour, it affects, affects our moods and feelings, and research suggests that it has a physical effect as well, influencing the hormones that control our emotions.
Studies have shown that color:
- Increases brand recognition by up to 80%
- Improves readership as much as 40%
- Increases comprehension by 73%
- Can be up to 85% of the reason people decide to buy
Bansal-Travers, O’Connor, Fix,and Cummings (Am J Prev Med 2011;40(6):683–689) showed 193 participants array of six cigarette packages (altered to remove all descriptive terms) and asked to link package images with their corresponding descriptive terms. Participants were then asked to identify which pack in the array they would choose if they were concerned with health, tar, nicotine, image, and taste. Participants were more accurate in matching descriptors to pack images for Marlboro brand cigarettes than for unfamiliar Peter Jackson brand (sold in Australia). Smokers overwhelmingly chose the “whitest” pack if they were concerned about health, tar, and nicotine. Smokers in the U.S. associate brand descriptors with colours. Further, white packaging appeared to most influence perceptions of safety.
Tobacco studies indicate that health-related information in cigarette advertising leads consumers to underestimate the detrimental health effects of smoking and contributes to their smoking-related perceptions, beliefs, and attitudes. Paek and colleagues (Paek et al., 2010) examined the frequencies and kinds of implicit health information in cigarette advertising across five distinct smoking eras covering the years 1954-2003. Most notably, a majority of the cigarette ads portrayed models smoking, lighting, or offering a cigarette to others. Rooke and colleagues (Rooke et al., 2010) investigated how tobacco displays are used at the point of sale (PoS) as an important means for the tobacco industry to communicate with consumers. With regulations prohibiting PoS displays recently having come into force in Ireland, this is an increasingly important issue. Over 100 retailers were visited, with interviews taking place on site. Information was gathered on the type and size of tobacco display, who was paying for the display, requirements and incentives, and visits by industry representatives. The majority of retailers had gantries provided by tobacco companies. A minority of these were fitted with automated dispensers called retail vending machines. Attractive lighting and colour were often used to highlight particular products. Wakefield and colleagues (Wakefield et al., 2002) investigated the role of pack design in tobacco marketing. A search of tobacco company document sites using a list of specified search terms was undertaken during November 2000 to July 2001. Many smokers are misled by pack design into thinking that cigarettes may be “safer”. There is a need to consider regulation of cigarette packaging.
The World Health Organization applauded Australia’s law on plain packaging noting that “the legislation sets a new global standard for the control of a product that accounts for nearly 6 million deaths each year” The Cancer Council of Australia hailed the passing of the legislation, stating, “Documents obtained from the tobacco industry show how much the tobacco companies rely on pack design to attract new smokers….You only have to look at how desperate the tobacco companies are to stop plain packaging, for confirmation that pack design is seen as critical to sales.” Don Rothwell, professor of international law at the Australian National University, noted that Philip Morris was pursuing multiple legal avenues. The Notice of Arbitration under the bilateral investment treaty between Hong Kong and Australia has a 90-day cooling off period after which the case would most likely be sent to the International Centre for Settlement of Investment Disputes in Washington. He stated that Philip Morris was most likely aiming for the Australian Government to back down, or failing that, to sue for compensation. He said the questions to decide are whether the legislation means that Australia would acquire property by the imposition of these rules and if this legislation is a legitimate public-health measure. Gavin Allen of the Daily Mail newspaper reported that the Philip Morris lawsuit could cost the Australian government “billions”. He also noted that the Australian law is being closely watched by other governments in Europe, Canada and New Zealand. In 2005, the World Health Organization urged countries to consider plain packaging, and noted that Bhutan had banned the sale of tobacco earlier in 2011.
As the latest row over the role of big money in politics hit Downing Street, Paul Burstow, who was a health minister until September last year, said Crosby should either quit or be sacked by Cameron after it emerged that his lobbying firm works for global tobacco giant Philip Morris. Other Liberal Democrats also made clear they were furious and would fight to ensure Crosby was removed from any role in which he could influence health or any other coalition policy. Amid the growing furore, the Tory chairman of the all-party select committee on health, former health secretary Stephen Dorrell, announced that his committee would look into why the government had changed its mind on the question of cigarette packaging.
This is a very serious issue. The Observer editorial was devoted to it this morning.
As the Smokefree Action Coalition points out, cigarettes are the only legal product sold in the UK that kill their consumers when used exactly as the manufacturer intends. Even if the government remains unconvinced of the wisdom of plain packaging, an alliance of MPs, charities and health experts and the Faculty of Public Health disagree, as does the public. A YouGov poll in February found that 64% of the public is also in favour. So why the sudden U-turn?
The tobacco giants are spending £2m in a campaign against standardised packaging. Critics also point out that the industry has its very own Trojan horse inside Number 10, in the shape of Australian Lynton Crosby, the Conservatives’ general election co-ordinator. Hours after the decision to postpone plain packaging, it emerged that Crosby’s company, CTF, has been advising Philip Morris Ltd in Britain since November. Now there are calls for an inquiry. As the lacklustre bill on lobbying moves through parliament, Deborah Arnott, chief executive of the health charity Action on Smoking and Health, rightly says: “David Cameron has called political lobbying the ‘next big scandal waiting to happen’. Happen it has, right in 10 Downing Street.” Tory MP and GP Dr Sarah Wollaston, who also campaigns for price controls on alcohol, aptly tweeted: “RIP public health. A day of shame for this government; the only winners big tobacco, big alcohol and big undertakers.”
“There is another fundamental contradiction in nudging, particularly in the context of the declared intent to increase a sense of individual responsibility outlined by the Prime Minister. Whilst there may be an attempt to provide at least token interference transparency to preserve the possibility of exposing a ‘nudge too far’, this also underlines how far this process is from one that encourages greater learning about problems and how the individual might take on some responsibility for their management. Behaviouralism directs us away from building the renewed sense of personal and social responsibility the Coalition government has set out as fundamental to its mission.”
Therein lies the rub perhaps. While promoting “individual choice” through nudges, the policy has inadvertently discouraged personal responsibility, and especially responsibility for other members of the community. The critical problem is that the whole is not the sum of its constituent parts, and while FA Hayek’s “The Road to Serfdom” was hailed by Margaret Thatcher (whose remark was passionately argued by the Bishop of London at her funeral to have been misquoted), cognitive neuroscience acknowledges that individuals often make the “wrong” choices – wrong for them individually, and also wrong for society. Many decisions are unconscious, and indeed that is what the whole of the profit-generating marketing industry is devoted to manipulating. But the fact that these decisions are unconscious tells you exactly what is fundamentally incorrect about the libertarian analysis. People don’t know why they’re making certain decisions: they are not in control at all. The advertisers are. And more importantly, they cannot learn from their decision-making process. Public health, for all its possible faults, is firmly against this philosophy.
References
Paek HJ, Reid LN, Choi H, Jeong HJ. (2010) Promoting health (implicitly)? A longitudinal content analysis of implicit health information in cigarette advertising, 1954-2003. J Health Commun. 2010 Oct;15(7):769-87. doi: 10.1080/10810730.2010.514033.
Rooke C, Cheeseman H, Dockrell M, Millward D, Sandford A. Tobacco point-of-sale displays in England: a snapshot survey of current practices. Tob Control. 2010 Aug;19(4):279-84. doi: 10.1136/tc.2009.034447. Epub 2010 May 14.
Wakefield M, Morley C, Horan JK, Cummings KM. (2002) The cigarette pack as image: new evidence from tobacco industry documents. Tob Control. Mar;11 Suppl 1:I73-80.
Bansal-Travers, M, O’Connor, R, Fix, BV, Cummings, KM (2011) What Do Cigarette Pack Colors Communicate to Smokers in the U.S.? Am J Prev Med 2011;40(6):683– 689
