Home » Posts tagged 'Clare Gerada'
Tag Archives: Clare Gerada
My medical career finished along ago, but the GMC FTP procedures for ill doctors are still far too dangerous

One of the ways that the General Medical Council will try to pin you down is if you appear blasé in any sense about your own behaviour, or lack insight into its repercussions.
I have a psychiatrist in West London who oversees my recovery. I am a barn door alcoholic now in recovery. One of the wisest things he has ever said to me is that it is impossible to ignore the distress I caused to friends, family and others. I think about this every day of my life in fact. It has left an indelible trace on Google, which I do not wish to forget. That’s why I have never asked for it to be removed.
I get upset that the BBC considers my tragic case of erasure from the Medical Register as ‘entertainment’. Behind this titillating story was someone who was in massive distress, and to some extent continues to be in distress.
I have learnt the General Medical Council (GMC) is only doing its job. Reports, like the latest damning one by Civitas on how the GMC treats sick doctors badly, come and go. And nothing really changes.
But I remember all too well what happened to me. I repeat that I find my behaviour then, as a different person, disgusting and unacceptable. But things came to a head when I was blue-lighted in at the beginning of June 2007 with an asystolic cardiac arrest which I was very lucky to be resuscitated out of. I then spent six weeks in a coma. I was fighting for my life, with drips, a central line, and the full army of Intensive Care machinery. The Consultant at the Royal Free warned people I was not expected to leave the hospital. I was clearly a very sick man.

My late father came to visit every day when I was learning how to walk and talk again at the National Hospital for Neurology and Neurosurgery. That’s where I had spent six happy months, while healthy, learning about general neurology and dementia. It’s where I developed a lifelong interest in neurodegenerative disease, which pervades through my post-doctoral fellowship at the Institute of Neurology thereafter, my mention in the Oxford Textbook of Medicine, and my own book on wellbeing in dementia.
I am happy now that, having learnt how to walk and talk, I was invited to the Alzheimer’s Association International Conference in Copenhagen last month, and I went to the Alzheimer’s Show in Manchester and London this year. My friends include people living with dementia, and they tell me what’s important in policy now.
I remember though the days of having to hide my name on blogposts or my Twitter account. I remember how I was frightened to show myself in public in the last few years. I remember how my circle of friends completely collapsed, though I am happy with the very small number of very close friends I have now. I still continue to get trolled, like no tomorrow, with words like “Disgusting” and “How do you live with yourself?”
I do also remember how the General Medical Council took years with their investigations. I remember the torrent of newspaper articles explaining how likely it would be I would be struck off. I remember thinking how this was an inglorious end to my ten years training to be a Doctor, a profession which I still feel honoured to have been in once.
But the General Medical Council protracts out their investigations. The GMC never got round to appointing a clinical supervisor (very odd) even though my independent clinical examiners had concluded that I had a severe alcohol problem. So it rumbled on for a few years with my mental health in free fall. Dynamite.
This is extremely risky – dangerous – for the sick doctor. If you lack insight or if you’re in denial you can be finished (as indeed the numbers of people reported to have committed suicide while waiting for their Fitness to Practise sessions show).
I remember how I totally ‘lost it’ in 2005 a year before my final hearing. I had long left a medical job, but I just fell apart while still waiting for my GMC hearing. I went on a massive bender sat alone sobbing into my drink in a pub in Notting Hill very close to Portabello Road, ended up being sectioned, and then was suspended by the GMC.
A year after I was erased, with no job and no family or friends virtually, my life really did take a nosedive. I sat in pubs all day from opening time to closing time. I was done for drunk and disorder offences.
But I woke up after a six week coma, newly disabled, but with a new purpose. I did three books on postgraduate medicine, and I became regulated by the Solicitors Regulation Authority. I have three degrees, my Bachelor of Law, my Master of Law, and my Master of Business Administration, as well as my pre-solicitor training.
I didn’t get very far when I bothered going up to Manchester for my restoration application. The GMC hadn’t bothered to do a basic conflicts session, so the meeting was adjourned after one day. My friend Martin Rathfelder made it to support me. He like Jos Bell and Kate Swaffer are true friends.
It’s a miracle that I didn’t have a relapse being in the City where I had been with my late father, where I was erased, with plenty of bars and restaurants, with plenty of memories. It’s like you’re being set up to fail by the GMC – or else they are incredibly incompetent when it comes to dealing with people with mental health issues.
But I did get as far as asking the panel if I could hold the hearing in public this time. I want to explain to the whole world why and how alcohol destroyed my life, and caused distress to others.
I think the GMC did the right thing in getting rid of me from the medical profession, but I am still bemused why one consultant in West London asked me to sort it out by giving me a phone number of the Priory, did not refer me to Occupational Health, and did not offer me sick leave. I am bemused why various consultants described me as looking dishevelled and alcoholic, and yet allowed me to finish my medical jobs in London, without referring me to Occupational Health.
By the time I was erased, the GMC had been given five reports from five independent doctors stating clearly that my primary problem was a severe alcoholic dependence disorder, and that I desperately needed help.
I never received this help until the NHS saved my life a year later.
The GMC will wish to ‘win their case’ and I strictly speaking am not allowed to bring any of this up in case it reaks of bitterness.
The GMC opposed my application to explain all this and my recovery in public. The panel rejected the GMC’s case.
In my view, Clare Gerada’s “Practitioner Health Programme” is a necessary lifeline for those are sick Doctors, and who fall under the London jurisdiction.
Prof Gerada is a true inspirational NHS leader.
Needless to say, I’ve never had an alcoholic drink for more than seven years, since my coma. I’m one of those guys who has no off switch after one drink, such that I’ll either end up in A&E or in a police cell.
My case will now be held in Manchester beginning August 20th 2014. If you want to begin to understand how sick doctors cope, or do not cope, please feel to come along.
My experience of being a sick Doctor

“Anything can happen to anybody at any time.”
This one principle does guide what I think about people and health.
It’s what I think when a friend of mine living with dementia suffers a bereavement. It’s what I think when a friend of mine gets told he has bladder cancer.
It’s also how I come to rationalise my six week coma in 2007 due to acute bacterial meningitis. I was rushed into the intensive care unit of the Royal Free Hospital Hampstead, having been resuscitated successfully by somebody I used to work with in fact. He knows who he is.
His team stopped me fitting in an epileptic seizure. His crash team got a pulse back on their third cycle of jumping down on my chest after I had been flatlining in cardiac asystole. He managed to put a tube down me as I had stopped breathing.
I then spent six weeks in a coma, and my mother and late father came to visit me every day in intensive care, and in the neurorehabilitation unit (Albany Ward) at the National Hospital for Neurology and Neurosurgery, London (a hospital in which I had worked in 2002 in a rotation which included an interest of mine, dementia).
I am now living with physical disability. I can now walk, and I remember my protracted time in a wheelchair. I remember people’s reactions to you in the street. I remember how ‘available’ black cabs would simply drive past. I was, in effect, taught how to work again by inpatient and community physiotherapy.
Due to my meningitis, I could barely speak; the “speechies” helped me with that. I had difficulty planning a cup of tea; the “OTs” helped me with that.
I can relate to all the current NHS concerns how you become stripped of identity in the modern NHS: you become a bed number, or at best a surname.
But in many ways, as my late father kept reminding me shortly before his own death in November 2010, that meningitis in a way saved my life.
I then engaged properly with the NHS as a patient. I used to see my GP regularly.
As a medical student, I had felt as if I was too busy to see my own GP. Big mistake.
As a young house officer in hepatology, I used to be surrounded with very pleasant patients; but for whom I had to perform an abdominal paracentesis, as they were often bright yellow due to liver failure (but awaiting a liver transplantation).
I slowly became alcoholic and isolated. I have often been asked when did I start to drink heavily. This is very difficult for me to place, as most people like me go through a phase of problem drinking.
My official diagnosis for the alcoholism is severe alcohol dependence syndrome in remission. I have now not drunk alcohol for seven years. I know I am an alcoholic as it is unsafe for me to have an alcoholic drink. If I have an alcoholic drink, I would either end up in A&E or in a police cell. I am incapable of having a social drink.
Receiving a medical diagnosis for my mental health condition, in my particular case, helped me to rationalise the cause of my problems which had caused so much distress to others including especially my mother and late father.
I was listening to LBC last night and the presenter was joking that he had a listener rung up “I am an alcoholic. I haven’t had a drink for 35 years.” But seriously folks, it is like that.
I am now regulated by the legal profession. I spent 9 years at medical school, doing my basic degrees for medicine and surgery, and my PhD in the early diagnosis of frontal dementia. As a junior in the medical profession, walking around as the most junior member pushing the Consultant’s trolley and writing in the notes, the thought that you might be ill did seem an alien one.
And yet I was extremely ill. For all people in addiction, there becomes a time when you are in complete denial and lack complete insight. That’s when it is impossible for you to be regulated.
I also have a lot of sympathy for the regulators who regulate people who I think can be best be described as a “dry drunk patients” – i.e. they spend months or even years dry before relapsing. They are, I feel, “living by the seat of their pants”, or “whiteknuckling” it.
The alternative is recovery – where you are not merely abstinent, but where you embrace a life which is utterly content, but in the absence of your addiction of choice.
I indeed find this hard to explain to people who have never experienced addiction. I do not wish to compete with ‘patient leaders’, or think tanks who go on and on and on and on about patient involvement.
But I do wish to recommend to you, if you are in their catchment area, the Practitioners Health Programme (PHP). An incredible ambition of Prof Clare Gerada, the programme is a lifeline to doctors who are ill. It’s been shown in numerous numerous surveys that an ill doctor under-functions as much ‘use’ as a doctor who is completely out of the service. I would simply say to anyone who is ill in the medical profession, put your own health ahead of your career. Your patients deserve that too. Do not be blinded by your own career. I am proud to attend regularly PHP.
I don’t do much apart from hundreds of blogs for the SHA, or campaigning for people living with dementia. But I am at least at last content.
Update: I (Dr Shibley Rahman) was returned to the GMC Register for the UK 26 August 2014. I had been in recovery from alcohol since the onset of my coma due to meningitis in June 2007.

Living well with dementia: diet not drugs?

There is no cure for dementia currently. The available treatment strategies offer mainly symptomatic benefits. Thus, strategies to prevent or delay onset of dementia by changes in lifestyle factors, such as diet, are therefore important, given finite resources. There is no doubt it’d be wonderful if, after many many years of trying, there might be a breakthrough.
But physicians and politicians have a responsibility to the general public to be honest about what is genuinely achievable. It’s in the interests of charities and research groups which depend on income for their research to raise money for a cure; or in the interests of those research groups wishing to raise money for research which appears linked to that somehow. It’s in the interest of Big Pharma-ceutical companies to raise money for their research funds; and they have a legal duty to their shareholders too. The public appreciate a truthful debate about what might work; and where a lot of monies would in fact would be better spent elsewhere.
It’s certainly low hanging fruit for politicians to support this worthy cause.
However, the scant attention to living well with dementia in many statements, in contrast to drug treatments, is very telling. The Department of Health will, however, be livestreaming the #G8dementia summit proceedings later this week. Details are here.
Not all dementia occurs in the elderly. Nonetheless, it is possible that health problems related to aging (including dementia of the Alzheimer type) are projected to add to the high clinical, social, and economic burden of caring for persons with dementia.
The Mediterranean diet has been associated with reduced risk for a wide range of age-related conditions such as stroke, type 2 diabetes, cardiovascular disease, and all-cause mortality. The traditional Mediterranean diet refers to a multinutrient dietary profile characterized by high intake of fruits, vegetables, cereals, and legumes; low consumption of saturated fats with olive oil as the main source of fat; moderate consumption of fish; low to moderate intake of dairy products (in the form of yogurt and cheese); low consumption of red meat and meat products; and moderate amount of alcohol (especially wine) usually consumed during meals.
Recently, a number of peer-reviewed pieces in the reliable academic literature have presented evidence for an association between a Mediterranean-type diet and decreased risk of dementia. Findings from prospective studies suggest that greater adherence to Mediterranean diet may be associated with slower cognitive decline and reduced risk of Alzheimer disease. In the light of these findings, it has been suggested that improving adherence to the Mediterranean diet may delay or prevent the onset of dementia.
A really helpful review was published by Lourida and colleagues earlier this year in the “Epidemiology” journal (Jul;24(4):479-89). Twelve eligible papers (11 observational studies and one randomized controlled trial) were identified, describing seven unique cohorts.
Despite methodological heterogeneity and limited statistical power in some studies, there was a reasonably consistent pattern of associations. Higher adherence to Mediterranean diet was associated with better cognitive function, lower rates of cognitive decline, and reduced risk of Alzheimer disease in nine out of 12 studies, whereas results for mild cognitive impairment were inconsistent.
Published studies suggest that greater adherence to Mediterranean diet is associated with slower cognitive decline and lower risk of developing Alzheimer disease. Further studies would be useful to clarify the association with mild cognitive impairment and vascular dementia. Long-term randomised controlled trials promoting a Mediterranean diet may help establish whether improved adherence helps to prevent or delay the onset of Alzheimer disease and dementia.
Only today, leading doctors warned the Government the battle against dementia should focus on the benefits of a Mediterranean diet rather than ‘dubious’ drugs. In an open letter to the Health Secretary, they said persuading people to eat fresh fruit and vegetables, nuts, fish and olive oil was ‘possibly the best strategy currently available’ for preventing Alzheimer’s and other memory-robbing diseases.
The letter’s signatories include Prof Clare Gerada, the former chairman of the Royal College of General Practitioners, and Dr David Haslam, chairman of the National Obesity Forum.
It reads:
‘We hope this crisis can be seen as an opportunity towards a real policy change, namely towards a Mediterranean diet, rather than towards the dubious benefits of most drugs.’
It goes on to say the evidence ‘strongly suggests’ that improvements to lifestyle will have a ‘far greater effect’ on the rising tide of dementia than drugs.
The call comes as dementia experts from the G8 countries prepare to travel to London for a summit hosted by the Prime Minister.
Dr Simon Poole, the GP who organised the letter, said: ‘It is all about looking at what pharmaceutical companies can do, which is actually not very much.
‘They talk up their medicine and then it is very often a damp squib. We want some sort of focus on prevention. Educating all generations, including our children, in the importance of a good diet in maintaining health in old age is a project which will take years, but is absolutely essential.’
‘We are calling upon policymakers to not only support the care and treatment of those who are already suffering from dementia, but to make significant investments in work which will see benefits beyond the period of one or two parliaments.’
There has also been a focus on individual components of the Mediterranean diet, such as [omega]-3 fatty acids or olive oil as the main source of monounsaturated fats. Although the advantages of Mediterranean diet are relevant for non-Mediterranean populations, it is often argued that studies are not always comparable because there are substantial differences in dietary composition among countries.
A more detailed examination reveals this is perhaps especially true for fatty acids. Although olive oil is the hallmark of Mediterranean diet, differences in the origin of monounsaturated fats or cooking style (eg, baked vs. fried) could partly explain these inconsistencies. Studies comparing types of olive oil concluded that compared with refined oil, virgin olive oil (rich in phenolic content) has additional anti-inflammatory and antioxidant properties beneficial to cellular function and cardiovascular health.
The Mediterranean diet may exert its effects on cognitive health through multiple biological mechanisms. Relationships with reduced risk of coronary heart disease, hypertension, diabetes, dyslipidemia, and metabolic syndrome have been observed, and these conditions have also been associated with mild cognitive impairment, vascular dementia (a dementia associated with general factors affecting the cardiovascular system such as smoking, cholesterol, diet, family history), or disease of the Alzheimer type.
Sticking to this Meditteranean diet may also facilitate metabolic control because it has been related to improved insulin sensitivity and glucose metabolism. Insulin is a chemical acting in the body which can affect our metabolism – it is an important “hormone” for us.
Furthermore, “oxidative stress” increases with age and results in “oxidative damage”—a state often observed in the brain of patients with Alzheimer disease. Typical components of the Mediterranean diet (namely fruits, vegetables, wine, and virgin olive oil) are rich in antioxidants such as vitamin C and E, carotenoids, and flavonoids. Decreased oxidative stress found in people adhering to a Mediterranean-type diet could partially explain their lowered risk for dementia.
And there’s a plausible biological mechanism for all this. Brain cells (neurone) are protected against oxidative stress by specialist chemicals, called “neurotrophins” (basic proteins) such as the brain-derived neurotrophic factor. There is some evidence that Mediterranean diet may increase plasma brain-derived neurotrophic factor concentrations. Inflammatory processes have also been suggested for Alzheimer pathogenesis. Higher concentrations of C-reactive protein, a nonspecific marker of inflammation, have been associated with increased risk for cognitive decline, Alzheimer disease, and vascular dementia, whereas better adherence to Mediterranean diet has been associated with lower levels of C-reactive protein.
Access to medicine has become a really important issue in the NHS. Already we are getting stories of rationing in the NHS emerging during the period of this Government (such as varicose veins stripping), so it is not particularly surprising if drugs which do have modest effect on memory for dementia are not a top priority. Encouraging people to learn about diet and how this might prevent thinking problems is therefore a worthy aim, as it might actually work better than many of the drugs ‘on offer’. Senior doctors have advised this approach in fact.
Just because it’s not coming from Big Pharma with their massive marketing budgets doesn’t mean it’s a dead duck.
Related articles
- Healthy diet ‘may prevent dementia’ (skynews.com.au)
- Mediterranean Diet is the Key to Preventing Dementia (medindia.net)
- How To Live Longer: Mediterranean Diet Proven To Help Women Live Past 70 (medicaldaily.com)
- Dementia fight must focus on diet, say experts (yorkshirepost.co.uk)
Should Doctors and Nurses act as surrogate immigration officials?
 Anyone can get very ill at any time.
Anyone can get very ill at any time.
This issue is also about recognising mutual obligations and responsibilities, and looking after all our futures.
Would you like to be a British citizen abroad in France and being refused treatment?
Nonetheless, the British media has been relentless in presenting the ‘dogwhistle’ politics of immigration, rather than having an open, honest or complete debate about the NHS privatisation enacted by this Government.
Jeremy Hunt MP says today:
Having a universal health service free at the point of use rightly makes us the envy of the world, but we must make sure the system is fair to the hardworking British taxpayers who fund it.
This current Government, it has been argued, has been extremely divisive, setting off able-bodied people against disabled citizens, employed people against unemployed, and so it goes on.
The ludicrous farce of this latest announcement, of cracking down on “health tourism”, is that similar announcements have been made before. In the meantime, Hunt has been forced to apologise for a tweet when faced with legal action, and there has been talk of an impending crisis in acute medicine.
Today’s announcement will again see Ministers facing renewed claims that GP surgeries are being turned into “border posts”.
In its three years in power the government has a poor record on announcing policies that sound good but prove to be completely unworkable
(shadow health minister Liz Kendall, previously)
The Chair of the Royal College of General Practitioners, Prof Clare Gerada, has previously warned that:
“GPs must not be a new ‘border agency’ in policing access to the NHS. While the health system must not be abused and we must bring an end to health tourism, it is important that we do not overestimate the problem and that GPs are not placed in the invidious position of being the new border agency.”
Today, the Department of Health is publishing the first comprehensive study of how widely migrants use the NHS. These independent findings show the major financial costs and disruption for staff which result from a system which will be substantially reformed in the interests of British taxpayers. Just because they are ‘independent’ findings does not necessarily mean they are very accurate, as any observer of the “output” of the OBR will tell you.
Previous estimates of the cost to the NHS have varied, but this latest attempt research reveals the cost may be significantly higher than all earlier figures.
To tackle this issue and deter abuse of the system, the #omnishambles Government is proposing the following now:-
- introducing a simpler registration process to help identify earlier those patients who should be charged.
- looking at new incentives so that hospitals report that they have treated someone from the EEA to enable the Government to recover the costs of care from their home country.
- introducing a new health surcharge in the Immigration Bill to generate income for the Government (but it is unlikely this money will go into frontline patient care, as indeed the £2.4bn “efficiency savings” have not been returned either);
- appointing Sir Keith Pearson as an independent adviser on visitor and migrant cost recovery;
- identifying a more efficient system of claiming back costs by establishing “a cost recovery unit”, headed by a Director of Cost Recovery;
Andy Burnham MP, Labour’s Shadow Health Secretary, responding to Jeremy Hunt’s announcement on overseas visitors’ and migrants’ use of the NHS, said:
We are in favour of improving the recovery of costs from people with no entitlement to NHS treatment. But it’s hard not to conclude that this announcement is more about spin than substance. The Government’s own report undermines their headline-grabbing figures, admitting they are based on old and incomplete data. Instead of grand-standing, the Government need to focus on delivering practical changes. Labour would not support changes that make doctors and nurses surrogate immigration officials.
For a video of Andy Burnham MP responding to this latest report, please go here.
Furthermore, it appears that what Hunt won’t say about migrants is that British expatriates might make much heavier use of the NHS than any other visitors (and accordingly they should pay.)
A recent report by the European Commission concluded that so-called benefits tourism was “neither widespread nor systematic”.
As for most countries, residency not nationality primarily determines eligibility for healthcare treatment.
With the Conservative Party finding themselves ‘squeezed’ by UKIP in the run-up to the European elections, this could provide an useful smokescreen for the disaster in acute care which the Conservatives have somehow single-handedly generated.
However, the “benefits tourism” narrative of the Conservatives and UKIP was dealt a heavy blow by the emergence of this information, which the BBC’s Norman Smith tweeted earlier last week:
 Last week’s announcement by Jeremy Hunt on loneliness was panned in a widespread manner by many professionals.
Last week’s announcement by Jeremy Hunt on loneliness was panned in a widespread manner by many professionals.
Maybe for the Conservatives there is ‘no such thing as Society’ after all?
Overseas visitors and migrant use of the NHS: extent and costs
Time to rate how Doctors are treated in the NHS?
Sir Gus O’Donnell said famously, “If you treasure it, measure it”. This is happening in the medical profession too, with a policy drive that the best people to rate the NHS are the users of the service. These are the patients (or “customers” if you’re that way inclined). The ‘Friends and Family Test’ has come under fierce criticism, not surprising given that it has never been subject to proper analytical rigour, and the criticisms of it have been well rehearsed elsewhere. There is a fundamental difference in assessing your hospital stay, compared to “Trip Advisor”, but it is all part of the information revolution. Information, according to people interested in innovation like me, is not the same as knowledge, and not all information is useful. Whilst the corporates, who introduced their love for Big Data to the rest of the world are fully aware there is a lot of redundant, useless data, and the importance of certain datasets need to be explained carefully, this has completely passed the NHS by. The introduction of the vascular surgery rates was held by some to be a shambles, due to the poor explanation of these data as well as data inaccuracy. Forgetting the fact that certain fields in vascular surgery (e.g. abdominal artery aneurysm repairs for aneurysms diameter > 6.5 cm are considered riskier than sclerosing varicose veins, for example), or that safety is a team activity (though the root cause of a problem can be identified to a single reason), the data explosion is envisaged as empowering patients and persons with ‘choice’.
Enter the market. Jeremy Hunt continues to dodge completely the question why private sector entities under freedom of information legislation introduced by a Labour government are not under obligation to disclose data because of their ‘commercial interest’. As they are not public bodies, they are not amenable to judicial review either. Moving swiftly on, choice is supposed to empower the patient with information. How is that possible, that a patient will be equally fluent as a Doctor of about 7 years’ standing who has achieved registration with the General Medical Council? Very good question. Is it the case that vascular surgeons have a need to improve their mortality data because they are now operating (quite literally) in a free (pseudo)market? No, categorically not. The Royal Colleges of Surgeons and the General Medical Council are responsible for general professional training and higher specialist training standards in surgery. Doctors are increasingly seen as employees in a business case, with Trusts salami-slicing how much they want to spend on staff to achieve their efficiency savings as mandated by Sir David Nicholson and the Department of Health. They are that respect no more essential than an import of horsemeat for lasagna to improve the profitability of a venture capital investment. Registered Doctors are professionals though, and legal.
It has been noted that trust in GPs has plummeted from 70% to 30% since the implementation of the Health and Social Care Act (2012)? I, for one, would quite like to rate how management consultants conducted this important strategic implementation. This £3bn reorganisation had a critical piece of legislation, the “section 75 regulations”, which produced competitive tendering as the default option. The first set of Regulations were so bad they had to be withdrawn. The Medical Royal Colleges, the BMA and RCN all say the Act won’t work. The first rule of strategic implementation is that you involve all the stakeholders and engage in a realistic conversation about what is intended to be achieved, how, why, or when. None of this happened. That is why I award the Department of Health, despite what can be best described as “shuttle diplomacy” by Earl Howe, a big fat result thus:
 And why has trust in GPs plummeted? Is it anything to do with the fact the media and politicians have been force-feeding the public with stories that GPs opted out of out-of-hours some time ago, and they got a deal which was quite lucrative? Or is it because there are now anecdotal reports of GPs having to advise non-NHS care to their patients in the hope that they can jump a lengthy NHS queue? It is very hard to tell. But certainly it is true that GPs have become first in the firing line for the NHS reforms. They in fact opposed the reforms, with clear leadership by Prof Clare Gerada, Chair of the Royal College of General Practitioners. The Government PR went into overdrive that “GPs are at the heart of commissioning”, the ‘clinical commissioning groups’, but this was obviously never the intention. CCGs are merely a vehicle for holding funds and assessing risk in a pooled population, in a manner of ‘statutory insurance schemes’. This has always been the case, and always will be. For all the talk of ‘entrepreneurial GPs’, the public do not appear to warm to the idea of GPs as businessmen (and GPs do not particularly wish to represented as businessmen). Germane to this is the “dual agent” problem, very well known in insurance markets. That is the idea that no person can have “two masters”, without a significant conflict of interest: this might be for example a GP’s professional duty to his or her patient, and his or her duty to the people who ultimately provide the funding. This issue of trust is possibly bound to get worse, as ‘scandals’ are drip fed to the media of a system in distress. The reason this score is nothing to do with Prof Gerada is because Prof Gerada, as the new “NHS SOS” book explains (edited by Dr Jacky Davis and Prof Ray Tallis), was one of the few NHS leaders to have a clear vision and have the charisma to set this out in confidence, a textbook example of a “charismatic leader”, who deservedly was one of the hundred most influential individuals in health. And, very clearly, she appeared to be representing patients as well as GPs.
And why has trust in GPs plummeted? Is it anything to do with the fact the media and politicians have been force-feeding the public with stories that GPs opted out of out-of-hours some time ago, and they got a deal which was quite lucrative? Or is it because there are now anecdotal reports of GPs having to advise non-NHS care to their patients in the hope that they can jump a lengthy NHS queue? It is very hard to tell. But certainly it is true that GPs have become first in the firing line for the NHS reforms. They in fact opposed the reforms, with clear leadership by Prof Clare Gerada, Chair of the Royal College of General Practitioners. The Government PR went into overdrive that “GPs are at the heart of commissioning”, the ‘clinical commissioning groups’, but this was obviously never the intention. CCGs are merely a vehicle for holding funds and assessing risk in a pooled population, in a manner of ‘statutory insurance schemes’. This has always been the case, and always will be. For all the talk of ‘entrepreneurial GPs’, the public do not appear to warm to the idea of GPs as businessmen (and GPs do not particularly wish to represented as businessmen). Germane to this is the “dual agent” problem, very well known in insurance markets. That is the idea that no person can have “two masters”, without a significant conflict of interest: this might be for example a GP’s professional duty to his or her patient, and his or her duty to the people who ultimately provide the funding. This issue of trust is possibly bound to get worse, as ‘scandals’ are drip fed to the media of a system in distress. The reason this score is nothing to do with Prof Gerada is because Prof Gerada, as the new “NHS SOS” book explains (edited by Dr Jacky Davis and Prof Ray Tallis), was one of the few NHS leaders to have a clear vision and have the charisma to set this out in confidence, a textbook example of a “charismatic leader”, who deservedly was one of the hundred most influential individuals in health. And, very clearly, she appeared to be representing patients as well as GPs.
Anyone who wishes to defend the NHS is accused of protecting a ‘national religion’. And yet the NHS is accused of being ‘monolithic’, ‘inefficient’, ‘dangerous’, ‘expensive’, and every negative adjective under the sun. Politicians are responsible for this deprofessionalisation of key non-managerial workers in the NHS, with talk of ‘it doesn’t matter who provides my care as long as it is the…’ (a saying which in the legal and medical sectors has increasingly been completed with the word “cheapest”). Every conceivable thing is blamed for the pressures under which the NHS functions; such as the “burden of the ageing population” and the equally pathetic and untrue myth that high-quality healthcare is dependent on expensive equipment. Tell that to the cardiologist who can discern an early diastolic murmur with a pulmonary hypertensive ‘heave’ due to a crappy £20 stethoscope, not a £5000 portable digital echocardiogram machine. The number of lies in the drive to make the NHS attractive financially to outsourcers and privatisers has been breath-taking. In view of this, isn’t it time perhaps we either rate how Doctors are actually treated in the NHS, or time to turn the tables and rate our NHS management and politicians?
So what of social enterprises and the NHS? Corporate social responsibility and marketing revisited.

Milton Friedman’s famous maxim goes as follows:
“there is one and only one social responsibility of business – to use its resources and engage in activities designed to increase its profits so long as it stays within the rules of the game, which is to say, engages in open and free competition without deception or fraud.”
The history of social enterprise in fact extends as far back to Victorian England (Dart, 2004; Hines, 2005). The worker cooperative is one of the first examples of a social enterprise. Social enterprises prevail through- out Europe, and are most notable in the form of social cooperatives, particularly in Italy, Spain and increasingly France (Mancino and Thomas, 2005).
More recently, Clare Gerada, the Chair of the Royal College of General Practitioners, yesterday on BBC’s “The Daily Politics”, stated the following:
“Privatisation is the moving of State resources into the for full profit or non-profit sectors. And – the previous debate is that ‘if you don’t pay for therefore it’s not privatisation – it is privatisation. The profit that Specsavers or Harmoni make, they will not go back into the State: they will go straight into the shareholders.”
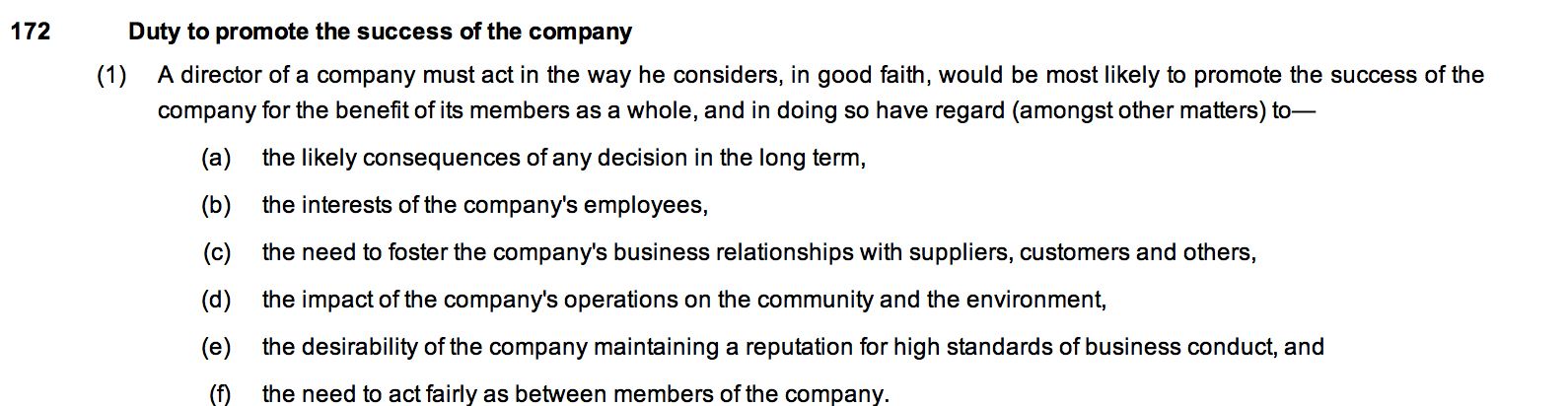
Currently, the position in English law is that the directors of every private limited company in law, whether they are called ‘social enterprises’ or not, have a statutory duty to the environment and stakeholders of their company. This is embodied in s.172 Companies Act (2006):
In an article by Rachel C. Tate, provocatively entitled, “Section 172 Companies Act 2006: the ticket to stakeholder value or simply tokenism?”, Tate argues as follows that stakeholder interests do not trump the interests of the company, i.e. to make profit. Interestingly. s.172 has no corollary in the common law.
“As highlighted, s172(1) formally obliges directors to consider stakeholder interests during the decision-making process. Yet, it is crucial to note that shareholder interests remain paramount. The interests of non-shareholding groups are to be considered only insofar as it is desirable to ‘(…) promote the success of the company for the benefit of its members.’17 A director will not be required to consider these factors beyond the point at which to do so would conflict with the overarching duty to promote company success. Stakeholder interests have no independent value in the consideration of a particular course of action.19 In addition, no separate duty or accountability is owed to the stakeholders included in the section.Thus, the duties of nurturing company success and having regard to the listed interests ‘(…) can be seen in a hierarchal way, with the former being regarded more highly than the latter.’21 Consequently, it would be wrong in principle to view s172 as requiring directors to ‘balance’ shareholders and stakeholder interests.22 These views are supported by industry guidance published on the effects of s172.”
“Social enterprises” are actually very hard to define. According to the United Kingdom (UK) government’s Department of Trade and Industry (2002), in the era of Tony Blair and Patricia Hewitt, a social enterprise is:
“a business with primarily social objectives whose surpluses are principally reinvested for that purpose in the business or in the community, rather than being driven by the need to maximise profit for shareholder and owners’”
Therefore, in theory, social ends and profit motives do not contradict each other, but rather have complementary outcomes, and constitute a ‘double bottom line’.
Nonetheless, the UK Government website contains a list of possible entities which could be described as ‘social enterprises’, namely:
- limited company
- charity, or from 2013, a charitable incorporated organisation (CIO is the new legal structure for charities)
- co-operative
- industrial and provident society
- community interest company (CIC)
- sole trader or business partnership
Note that in one of the vehicles, the limited company, as stated above, the primary duty of the directors is to promote success of the company. And that can be a “social enterprise”. Furthermore any contracts supplied to social enterprises can still still meet the definition of ‘privatisation’ above, not least because social enterprises are considered not to be wholly in the public sector (for example this EU definition, link here, where “Social enterprises are positioned between the traditional private and public sectors.”). Social enterprises do not meet the definition of what is typically in the public sector, by reference to the European System of Accounts 1995, link here. It is striking that the EU concede that one feature of social enterprises is a “significant level of risk”, so one has to question the long-term wisdom of competitive tendering contracts increasingly to social enterprises. Indeed, given that directors of English private limited companies are supposed to have due regard to wider “stakeholder” factors, one has to wonder quite what the point of the Public Services (Social Value) Act 2012 is. “Third Sector” magazine on 9 October 2012 reported that this enactment was not going that well:
“The Public Services (Social Value) Act could end up as a missed opportunity and more work needs to be done to encourage its use by commissioners and procurement professionals, delegates at the Labour Party conference heard. The act became law in March and places a duty on public bodies in England and Wales to consider “economic, social and environmental wellbeine in connection with public service contracts’! But at a fringe event hosted by the local infrastructure body Navca and the think tank ResPublica in Manchester, Hazel Blears, vice-chair of the All-Party Parliamentary Group on Social Enterprise, said she was concerned that many local authorities would not give it the attention it deserved.”The wording is weak,”she said.”If they had to ‘take account of social value, that would have been a harder position.””
There has been concern that in social enterprises, whilst the external environment may be given prominence, the internal environment may suffer (Cornelius et al., 2008):
“Since many social enterprises exist predominantly to address social ends (one key feature of the triple bottom line), it could be argued that the prevalence of their CSR policy and practice require close investigation. Emanuele and Higgins (2000) con- tribute to this agenda by challenging the assumption that non-profit organisations can offer comparatively lower wages, because they are more pleasant places to work. The authors emphasise that employees in this sector are often second income earners, and therefore are less concerned with lower wages and reduced benefits more characteristic of the private sector. They highlight how the voluntary sector is often a job entry point for new employees, who later move on to other sectors offering more fringe benefits, better financial security and healthcare programmes. They conclude with the assertion that ‘‘we must begin to exert the same pressure for ‘corporate responsibility’ among non-profit employers, as we demand in the private sector’’ (Emanuele and Higgins, 2000: 92), implying that the social enterprise sector needs to treat its employees better. Distinguishing between external and internal CSR may be beneficial, with social enterprises clearly focusing upon serving communities and overlooking crucial internal human resource issues.”
Grimsby “Care Plus” has been, in fact, highly commended in the UK Social Enterprise Awards (link here). The national competition, organised by Social Enterprise UK, recognises excellence in Britain’s growing social enterprise sector. And yet it was recently reported that, “More than 800 staff employed by the Care Plus Group – which provides adult health and social care across North East Lincolnshire – are in consultation over cuts to their pay and conditions.” Lance Gardner, the Chief Executive of the organisation, is reported as saying, “There is a lot of goodwill here. Our staff go that extra mile for their patients and have a passion for caring. They would not want to see them suffer. I do not want to take our goodwill for granted.”
The story of what happened between UNISON and Circle Hinchingbrooke is of course well known now (link here):
“Christina McAnea, head of health at Unison, said Circle could “cream off nearly 50% of the hospital’s surpluses” which would make it “virtually impossible to balance the books”.
“This is a disgrace. Any surpluses should be going directly into improving patient care or paying off the hospital’s debt, securing its future for local people – not ploughed into making company profits.
“Instead patients and staff are facing drastic cuts. The hospital was already struggling, but the creep in of the profit motive means cuts will now be even deeper. And it is patients and staff that will pay the price.””
Of course, ‘corporate social responsibility’ (“CSR”), abbreviated to ‘people, planet, profit’ somewhat tritely, has clashed before with marketing, so it is no wonder that businesses should wish to look ‘socially responsible’ to seek competitive advantage. Corporates have long been criticised for using diversity as a marketing ploy, e.g. putting in their promotional literature photos of employees in wheelchairs to demonstrate they are disabled-friendly. Pitches from social enterprises are likely to come with them ‘a feel good factor’ in competitive tendering, and of course any pitch which complies with adding social value in keeping with the new legislation is perfect “rent-seeking” fodder. But at the end of the day they are a range of entities seeking to make money which does not necessarily get fed back into frontline care, but used to generate a surplus aka profit. In an outstanding essay by Anna Kim for the 8th Ashbridge Business School MBA award, the author writes:
“Many critics believe that most of so-called CSR activities are nothing but a deceptive marketing tool, such as greenwashing. Can British American Tobacco be a ‘responsible’ cigarette manufacturer? Is Nestle really moving towards social values, or simply trying to wash its image around the baby milk and other ethical issues by putting a Fairtrade label on its 0.2% of coffee product line? From the green policy of oil giants BP and Shell to the childhood obesity research fund of McDonald’s, the list of controversial CSR examples is not exhaustive.”
So what of social enterprises and the NHS – remember Milton Friedman and Clare Gerada….
References
Cornelius, N., Todres, M., Janjuha-Jivraj, J., Woods, A., and Wallace, J. (2008) Corporate Social Responsibility and the Social Enterprise, Journal of Business Ethics, 81, pp. 355–370.
Dart, R. (2004) The Legitimacy of Social Enterprise’, Nonprofit Management and Leadership ,14(Summer), pp. 411–424.
Department for Trade and Industry (2002) Social Enterprise: A Strategy for Success, available at http://www.seeewiki.co.uk/~wiki/images/5/5a/SE_Strategy_for_success.pdf .
Hines, F. (2005) Viable Social Enterprise – An Evaluation of Business Support to Social Enterprises’, Social Enterprise Journal, 1(1), pp. 13–28.
Mancino, A. and Thomas, A. (2005) An Italian Pattern of Social Enterprise: The Social Cooperative, Nonprofit Management and Leadership, 15(3), pp. 357–369.
So what of social enterprises and the NHS?

People, planet, profit
What of social enterprises and the NHS?
Milton Friedman’s famous maxim goes as follows:
“there is one and only one social responsibility of business – to use its resources and engage in activities designed to increase its profits so long as it stays within the rules of the game, which is to say, engages in open and free competition without deception or fraud.”
The history of social enterprise in fact extends as far back to Victorian England (Dart, 2004; Hines, 2005). The worker cooperative is one of the first examples of a social enterprise. Social enterprises prevail through- out Europe, and are most notable in the form of social cooperatives, particularly in Italy, Spain and increasingly France (Mancino and Thomas, 2005).
More recently, Clare Gerada, the Chair of the Royal College of General Practitioners, yesterday on BBC’s “The Daily Politics”, stated the following:
“Privatisation is the moving of State resources into the for full profit or non-profit sectors. And – the previous debate is that ‘if you don’t pay for therefore it’s not privatisation – it is privatisation. The profit that Specsavers or Harmoni make, they will not go back into the State: they will go straight into the shareholders.”
Currently, the position in English law is that the directors of every private limited company in law, whether they are called ‘social enterprises’ or not, have a statutory duty to the environment and stakeholders of their company. This is embodied in s.172 Companies Act (2006):
In an article by Rachel C. Tate, provocatively entitled, “Section 172 Companies Act 2006: the ticket to stakeholder value or simply tokenism?”, Tate argues as follows that stakeholder interests do not trump the interests of the company, i.e. to make profit. Interestingly. s.172 has no corollary in the common law.
“As highlighted, s172(1) formally obliges directors to consider stakeholder interests during the decision-making process. Yet, it is crucial to note that shareholder interests remain paramount. The interests of non-shareholding groups are to be considered only insofar as it is desirable to ‘(…) promote the success of the company for the benefit of its members.’17 A director will not be required to consider these factors beyond the point at which to do so would conflict with the overarching duty to promote company success. Stakeholder interests have no independent value in the consideration of a particular course of action.19 In addition, no separate duty or accountability is owed to the stakeholders included in the section.Thus, the duties of nurturing company success and having regard to the listed interests ‘(…) can be seen in a hierarchal way, with the former being regarded more highly than the latter.’21 Consequently, it would be wrong in principle to view s172 as requiring directors to ‘balance’ shareholders and stakeholder interests.22 These views are supported by industry guidance published on the effects of s172.”
“Social enterprises” are actually very hard to define. According to the United Kingdom (UK) government’s Department of Trade and Industry (2002), in the era of Tony Blair and Patricia Hewitt, a social enterprise is:
“a business with primarily social objectives whose surpluses are principally reinvested for that purpose in the business or in the community, rather than being driven by the need to maximise profit for shareholder and owners’”
Therefore, in theory, social ends and profit motives do not contradict each other, but rather have complementary outcomes, and constitute a ‘double bottom line’.
This is the EU definition (link here):
Social enterprises are positioned between the traditional private and public sectors. Although there is no universally accepted definition of a social enterprise, their key distinguishing characteristics are the social and societal purpose combined with an entrepreneurial spirit of the private sector. Social enterprises devote their activities and reinvest their surpluses to achieving a wider social or community objective either in their members’ or a wider interest.
However, they note that social enterprises have a “significant level of risk“. The fact that a ‘social enterprise’ is not a public body means that it lacks full accountability through legal mechanisms such as freedom of information requests or judicial review (provided time limits are observed), which is an issue that the law will have to confront at some stage; how amenable is the law to address questions of private companies forming essentially public functions?
Nonetheless, the UK Government website contains a list of possible entities which could be described as ‘social enterprises’, namely:
- limited company
- charity, or from 2013, a charitable incorporated organisation (CIO is the new legal structure for charities)
- co-operative
- industrial and provident society
- community interest company (CIC)
- sole trader or business partnership
However, a page from ‘Social Enterprise Scotland’ is much more helpful in describing the different entities, and what criteria might embrace all social enterprises (link here; ht: Martin Rathfelder @SocialistHealth). However, it should be noted that the approach of social enterprises in Scotland is not exactly the same as that in England. In England, a useful definition of what a “co-operative” is has provided by the Communities and Local Government Committee recently (link here), but the Committee interestingly note a ‘paralysis of decision-making’ if there are too many stakeholders with dissenting views (this will be a valid criticism of any organisation):
“A genuine co-operative model would draw together both the ‘consumers’ and ‘producers’ of public services, and enable the users of services to participate in service production and delivery. The reciprocity a public service co-operative offers to its consumers could generate tangible economic advantages at local level when the profits could be distributed amongst members as dividends and/or recycled back to the communities to support further public services, resulting in a sustainable accumulation of social and pecuniary capitals and substantially reduced reliance of citizens on state-funded models.”
Note that in one of the vehicles, the limited company, as stated above, the primary duty of the directors is to promote success of the company. And that can be a “social enterprise”. Furthermore any contracts supplied to social enterprises can still still meet the definition of ‘privatisation’ above, not least because social enterprises are considered not to be wholly in the public sector (for example this EU definition, link here, where “Social enterprises are positioned between the traditional private and public sectors.”). Social enterprises do not meet the definition of what is typically in the public sector, by reference to the European System of Accounts 1995, link here. It is striking that the EU concede that one feature of social enterprises is a “significant level of risk”, so one has to question the long-term wisdom of competitive tendering contracts increasingly to social enterprises. Indeed, given that directors of English private limited companies are supposed to have due regard to wider “stakeholder” factors, one has to wonder quite what the point of the Public Services (Social Value) Act 2012 is. “Third Sector” magazine on 9 October 2012 reported that this enactment was not going that well:
“The Public Services (Social Value) Act could end up as a missed opportunity and more work needs to be done to encourage its use by commissioners and procurement professionals, delegates at the Labour Party conference heard. The act became law in March and places a duty on public bodies in England and Wales to consider “economic, social and environmental wellbeine in connection with public service contracts’! But at a fringe event hosted by the local infrastructure body Navca and the think tank ResPublica in Manchester, Hazel Blears, vice-chair of the All-Party Parliamentary Group on Social Enterprise, said she was concerned that many local authorities would not give it the attention it deserved.”The wording is weak,”she said.”If they had to ‘take account of social value, that would have been a harder position.””
There has been concern that in social enterprises, whilst the external environment may be given prominence, the internal environment may suffer (Cornelius et al., 2008):
“Since many social enterprises exist predominantly to address social ends (one key feature of the triple bottom line), it could be argued that the prevalence of their CSR policy and practice require close investigation. Emanuele and Higgins (2000) con- tribute to this agenda by challenging the assumption that non-profit organisations can offer comparatively lower wages, because they are more pleasant places to work. The authors emphasise that employees in this sector are often second income earners, and therefore are less concerned with lower wages and reduced benefits more characteristic of the private sector. They highlight how the voluntary sector is often a job entry point for new employees, who later move on to other sectors offering more fringe benefits, better financial security and healthcare programmes. They conclude with the assertion that ‘‘we must begin to exert the same pressure for ‘corporate responsibility’ among non-profit employers, as we demand in the private sector’’ (Emanuele and Higgins, 2000: 92), implying that the social enterprise sector needs to treat its employees better. Distinguishing between external and internal CSR may be beneficial, with social enterprises clearly focusing upon serving communities and overlooking crucial internal human resource issues.”
Grimsby “Care Plus” has been, in fact, highly commended in the UK Social Enterprise Awards (link here). The national competition, organised by Social Enterprise UK, recognises excellence in Britain’s growing social enterprise sector. And yet it was recently reported that, “More than 800 staff employed by the Care Plus Group – which provides adult health and social care across North East Lincolnshire – are in consultation over cuts to their pay and conditions.” Lance Gardner, the Chief Executive of the organisation, is reported as saying, “There is a lot of goodwill here. Our staff go that extra mile for their patients and have a passion for caring. They would not want to see them suffer. I do not want to take our goodwill for granted.”
The story of what happened between UNISON and Circle Hinchingbrooke is of course well known now (link here):
“Christina McAnea, head of health at Unison, said Circle could “cream off nearly 50% of the hospital’s surpluses” which would make it “virtually impossible to balance the books”.
“This is a disgrace. Any surpluses should be going directly into improving patient care or paying off the hospital’s debt, securing its future for local people – not ploughed into making company profits.
“Instead patients and staff are facing drastic cuts. The hospital was already struggling, but the creep in of the profit motive means cuts will now be even deeper. And it is patients and staff that will pay the price.””
This, unsurprisingly, has led UNISON to warn of the potential dangers of enterprises, specifically (this link):
“Social enterprises have been heralded as a ‘third way’ between private and state provision, combining the innovation, entrepreneurship and flexibility associated with the former with the public ethos and public interest of the latter. For some the expansion of social enterprise into mainstream services is an important part of policies for moving away from the state’s role in directly providing services and will help to improve them. For others this leads to the fragmentation of service provision, the incursion of private sector providers, the undermining of unions and central bargaining and a likely reduction in the public accountability of those services.”
Of course, ‘corporate social responsibility’ (“CSR”), abbreviated to ‘people, planet, profit’ somewhat tritely, has clashed before with marketing, so it is no wonder that businesses should wish to look ‘socially responsible’ to seek competitive advantage. In the modern philosophy, of ‘value creation’, as discussed for example by Juscius and Jonikas (2013), value can only exist in the context of any company (whether called a “social enterprise” or not) in its wider environment. This is shown in the Fig. below.
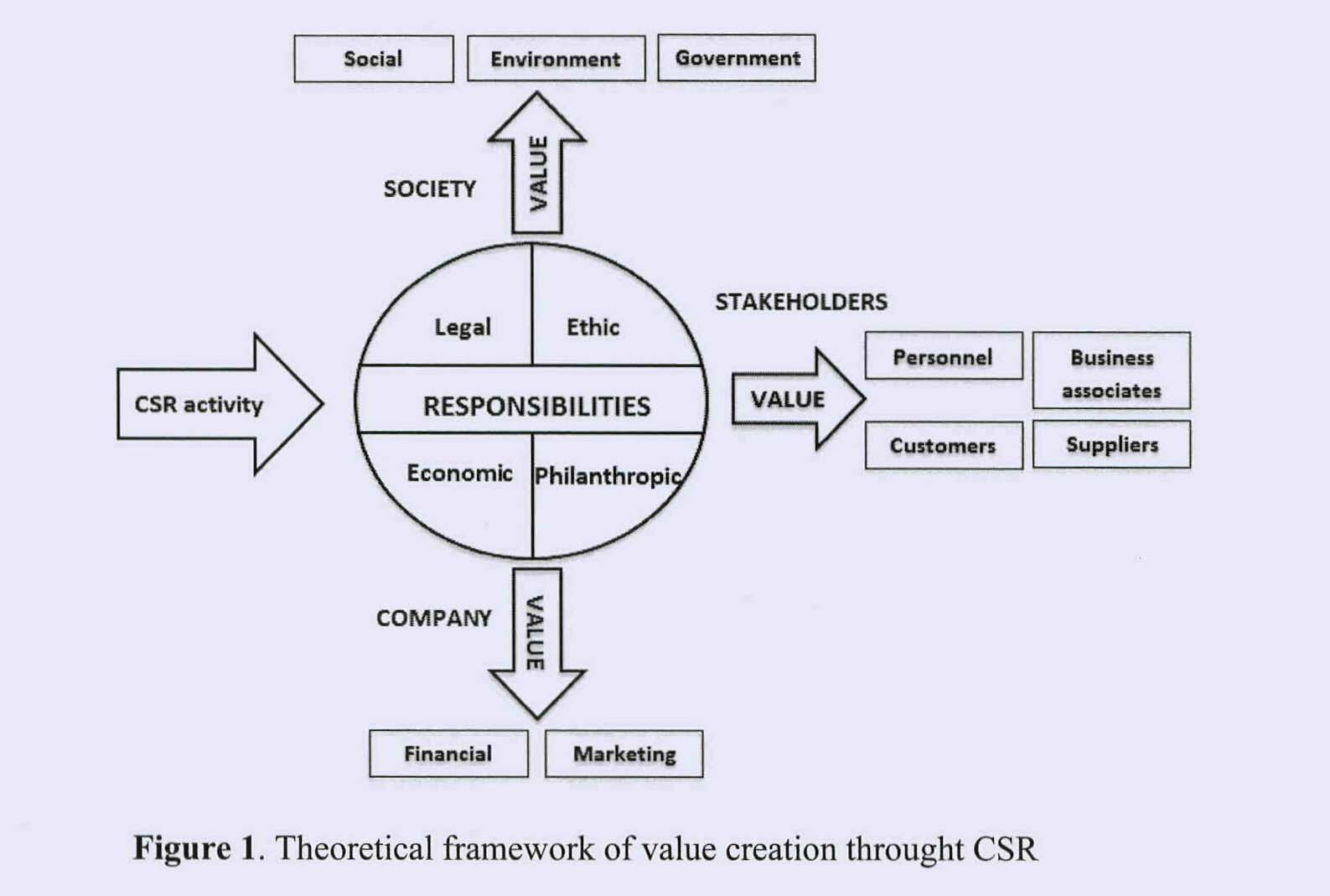
FIG. Theoretical framework of value creation through CSR (details in text.)
Corporates have long been criticised for using diversity as a marketing ploy, e.g. putting in their promotional literature photos of employees in wheelchairs to demonstrate they are disabled-friendly. Pitches from social enterprises are likely to come with them ‘a feel good factor’ in competitive tendering, and of course any pitch which complies with adding social value in keeping with the new legislation is perfect “rent-seeking” fodder. But at the end of the day they are a range of entities seeking to make money which does not necessarily get fed back into frontline care, but used to generate a surplus aka profit. In an outstanding essay by Anna Kim for the 8th Ashbridge Business School MBA award, the author writes:
“Many critics believe that most of so-called CSR activities are nothing but a deceptive marketing tool, such as greenwashing. Can British American Tobacco be a ‘responsible’ cigarette manufacturer? Is Nestle really moving towards social values, or simply trying to wash its image around the baby milk and other ethical issues by putting a Fairtrade label on its 0.2% of coffee product line? From the green policy of oil giants BP and Shell to the childhood obesity research fund of McDonald’s, the list of controversial CSR examples is not exhaustive.”
So what of social enterprises and the NHS – remember Milton Friedman and Clare Gerada….
References
Cornelius, N., Todres, M., Janjuha-Jivraj, J., Woods, A., and Wallace, J. (2008) Corporate Social Responsibility and the Social Enterprise, Journal of Business Ethics, 81, pp. 355–370.
Dart, R. (2004) The Legitimacy of Social Enterprise’, Nonprofit Management and Leadership ,14(Summer), pp. 411–424.
Department for Trade and Industry (2002) Social Enterprise: A Strategy for Success, available at http://www.seeewiki.co.uk/~wiki/images/5/5a/SE_Strategy_for_success.pdf .
Juscius, V, Jonikas, D. (2013) Integration of CSR into value creation chain: conceptual framework, Inzinerine Ekonomika-Engineering Economics, 24(1), pp. 64-70.
Hines, F. (2005) Viable Social Enterprise – An Evaluation of Business Support to Social Enterprises’, Social Enterprise Journal, 1(1), pp. 13–28.
Mancino, A. and Thomas, A. (2005) An Italian Pattern of Social Enterprise: The Social Cooperative, Nonprofit Management and Leadership, 15(3), pp. 357–369.

It's time we spoke about the "friends and family test"

Friends and family test
Mr David Cameron introduced ‘the friends and family test’ (FFT) at the beginning of this year. However, the FFT is based on a model developed to test satisfaction with consumer products. Clare Gerada, Chair of the Council of the Royal College of GPs, rightly questioned whether friends and family are proper judges of the NHS in all its complexity:
“The NHS isn’t Facebook, and healthcare isn’t a commodity like eating in a restaurant. And we must make sure that we don’t confuse issues around the NHS such as shortages, with the care that patients get from the staff that look after them.”
Dr Kailash Chand from the BMA Council likewise posited,
“Who can disagree with that?”.
Prof Peter Lynn, an expert on survey methodology from Essex University, says the findings may be unreliable.
“I have concerns about whether the friends and family test will actually provide data that allows meaningful comparisons of the performance of trusts – partly because of reliance on a single rather vague question and partly because hospitals will vary in how they approach patients and encourage them to answer the question.”
The government insists the test will give everyone a clear idea of where to get the best care, without piling costs on trusts. It says by checking on the NHS choices website, people will be able to see which trusts are in the normal range, those among the best and those among the worst.
Meanwhile, in a different sector, owners of pubs, restaurants, hotels and bars are all too familiar with “TripAdvisor”, which is loved and loathed in equal measures.TripAdvisor, which claims to have 75 million online reviews, allows people to post anonymously and without even proving they have been to the place in question. Getting a high or low rating can make or break a business. Chris Emmins of KwikChex, which investigates online reviews, believes there are as many as ten million fake reviews on the site by ‘trolls’ – someone who posts a deliberately provocative message with the intention of causing maximum disruption – who are either disgruntled former employees or rival businesses.
Emmins said:
“It’s war out there. Getting a top rating is crucial and yet one bad one-star review can hit the ratings so hard that it takes 20 five-star reviews to get the rating back.”
This is a wider example of the phenomenon called “shilling” in marketing. A shill, also called a plant or a stooge, is a person who publicly helps a person or organization without disclosing that he has a close relationship with that person or organisation. “Shill” typically refers to someone who purposely gives onlookers the impression that he is an enthusiastic independent customer of a seller (or marketer of ideas) for whom he is secretly working. The person or group who hires the shill is using crowd psychology, to encourage other onlookers or audience members to purchase the goods or services (or accept the ideas being marketed). Shills are often employed by professional marketing campaigns, and there is a danger that, like the original FFT has been imported, the practice of “shilling” could be imported too. Shilling is illegal in many circumstances and in many jurisdictions, because of the potential for fraud and damage, however, if a shill does not place uninformed parties at a risk of loss, but merely generates “buzz,” the shill’s actions may be legal. For example, a person planted in an audience to laugh and applaud when desired, or to participate in on-stage activities as a “random member of the audience,” is a type of legal shill.
