Home » Posts tagged 'whole person care'
Tag Archives: whole person care

A lot more unites us in English dementia policy than divides us, potentially
It’s sometimes hard to see the big picture in the policy of England regarding dementia.
I don’t mean this in terms of the three key policy strands of the strategy, which is currently the Prime Minister’s Dementia Challenge. This extra layer was added onto the English dementia strategy, “Living well with dementia”, from 2009-2014.
There will be a renewal of this strategy next year. We currently don’t know what Government will be in office and power in 2015. But I am hoping the overall direction of travel will be a positive one. I would say that, wouldn’t I?
There are 3 dementia challenge champion groups, each focusing on 1 of the main areas for action: driving improvements in health and care, creating dementia friendly communities and improving dementia research.
But it is in my political philosophy to encourage a pro-social approach, not a fragmented one.
I’d like to see people working together. This can all too easily be forgotten in competitive tendering for contracts.
And things can be just as competitive in the third sector as for corporates.
This is the clinical lead for dementia in England, Prof Alistair Burns, who has oversight over all these complicated issues.

But we need to have a strong focus for the public good, especially as regards looking after the interests of people living with dementia, and their closest including all caregivers. State-third sector initiatives can work brilliantly for particular outcomes, such as encouraging greater sharing of basic information about dementia, but all concerned will hopefully feel that the people whose interests we want to protect the most benefit from a plural space with many stakeholders.
There is definitely a huge amount which has been achieved in the last few years. I do definitely agree with Sally Greengross, Chair of the All Party Parliamentary Group for dementia, that we should really take stock of what has worked and what hasn’t worked so well in the last five years, in our wish to move forward.
I say this, as it has come to my attention while reviewing the current state-of-play in policy and in research that there are potentially problematic faultlines.
1. One is diagnosis.
On the one hand, some people feel that we are under diagnosing dementia, and that there are people languishing in England waiting for a diagnosis for weeks or months.
Chris Roberts, himself living with a dementia, and a greater advocate for people living with dementia, often warns that it is essential that, despite the wait, that the diagnosis is correct.
I know of someone else in the USA who has battled on for years while waiting for a diagnosis of dementia, despite having symptoms of dementia.
On the other hand, there are concerns, particularly if teams in primary care are financially incentivised for doing so, that there might be a plethora of over diagnosed cases.
The concern here is that there might be alternative interests for why such people might be diagnosed, such as being recipients of compounds from drug companies which attach to proteins in the brain, and which might be useful in diagnosing dementia.
Or we are building a ‘new model army’ of people who are ageing, but being shoehorned into the illness model because of their memory problems?
2. Another is potential ‘competition’ between dementia charities.
Essentially, all dementia charities in England want the same thing, and will need to attract an audience through various ‘unique selling points’ through that awful marketing terminology.
But in the next few years we may see commissioning arrangements change where the NHS may involve the third sector doing different complementary rôles, such as advising and providing specialist nursing, in the same contractual arrangement.
The law might force people to work together here.
3. Another is the ‘cure versus care’ schism.
This debate has accelerated in the last few years, with the perception – rightly or wrongly – that cure – in other words the drive to find a magic bullet for dementia – is vying for attention with care. This narrative has a complicated history in fact, in parallel with moves in the US which likewise have overall seen a trend towards some people wishing for a ‘smaller state’.
But claims about finding a cure for dementias have to be realistic, and, while comparisons can be made with HIV and cancer about the impact of a cure has for absolving stigma potentially, such a debate has been done incredibly carefully.
For example, attention for cures and collaboration between Pharma and ‘better regulation’ constitute a diversion of resources away from care, potentially. In the NHS strategy for England, with social care on its knees, a drive towards personalised medicine on the back of advances from the Human Genome Project can end up looking vulgar.
I’ve also seen with my own eyes how the ‘cure vs care’ schism has seen different emphases amongst different domestic and international dementia conferences, with some patently putting people with dementia in the driving seat, and some less so (arguably).
4. Another is the exact emphasis of ‘dementia friendly communities’.
It is impossible to object to the concept of inclusivity and accessibility of communities, with recognition of the needs of people living with the various dementias.
But the term itself is possibly not quite right; as Kate Swaffer says, a leading international advocate on dementia, you would never dream of ‘black friendly communities’ or ‘gay friendly communities’ as a term.
Another issue is what the precise emphasis of dementia friendly communities is: whether it is an ideological ‘nudge’ for companies and corporates to enable competitive advantage, or whether it is driven by a more universal need to enshrine human rights and equality law.
As Toby Williamson from the Mental Health Foundation mooted, the need for an employer to make reasonable adjustments for cognitive disAbility is conceptually and legally is actually the same as the need for an employer to build an access ramp for a person who is in a wheelchair and physically disabled?
There can also be a problem in who wishes to be “the dominant stakeholder”. Is it the person with dementia? Or unpaid caregiver? Or paid carer? Or professional such as CPN, physio, OT, speech and language therapist, neurologist, physician or psychiatrist? Is it a dementia adviser or specialist nurse?
If we are to learn the lessons from the Carers’ Trust/RCN “Triangle of Care”, it is essential to learn from all stakeholders in the articulation of a personalised care and support plan? I feel this is important in whole person care if we are to have such plans in place, which recognise professional pro-active clinical help, in trying to assist in avoidable admissions to hospital.
But here we have to be extremely careful. An admission to hospital or appearance at A&E should not always be sign of ‘failure’ of care in the community.
5. Yet another source of division is that we all do our own things.
This is problematic, if we do our own things. We end up being secretive about which people we’re talking to. Or which conferences we’re going to.
Or if countries don’t talk to each other, even if they have similar aims in diagnosis, and post-diagnostic care and support (including the global dementia friendly communities policy). Or if we don’t share lessons learnt (such as, possibly, the beneficial impact of treating high blood pressure on dementia prevalence in one country).
Or if certain people become figureheads in dementia. But no man is an island.
I still feel that there’s a lot more that unites us than divides us.
Anyway, I’ll leave it to people on the frontline, and in communities, much more able than me, to work out what they want.

The time is now right to promote specialist nurses in ‘dementia friendly communities’
There was a time when the GP used to be at the heart of a person’s community, as well as ‘delivering care’. For some people, there is no such thing as society, and the community consists of high street brands, banks and services (such as police or fire).
I’ve spent some time thinking about the implementation of the ‘dementia friendly community’ policy in a number of jurisdictions. It really has struck me how, for whatever political reasons, nurses are not perceived to be the heart of dementia friendly communities in England.
This, I feel, is a great tragedy. I don’t deny there are about a hundred different causes of a dementia, people’s social circumstances will differ (it is not uncommon for a female widower to develop a dementia while very lonely), cultural differences exist (for example in the rôle of the family in those of an Asian background), there are different rates of progression, and so on.
On receiving a diagnosis, I think support services in dementia should be much stronger than now. What is all too commonplace is a travesty. People don’t know where to turn to for basic information about clinical aspects, or wider aspects about living in the community.
As the dementia progresses, in the later stages, a focus will be to keep the person out of hospital wherever possible. Clearly, support and care in the community need to be funded properly.
A ‘crisis’ for a person living with dementia is where a ‘stressor’ causes that person no longer to be able to cope with living in his or her usual environment. There could be a number of causes of that, but it’s noteworthy that many of them are in fact medical. I disagree a specialist nurse in dementia is necessarily a job for a community psychiatry nurse (“CPN”), as the workload of such nurses tends to be very big.
But seeing a rôle for a CPN is not a trivial one, as I’m a fully signed up devotee of ‘parity of esteem’ where mental health is not seen as the ugly sister of physical health. For that matter, social work practitioners, who often find themselves at the heart of mental capacity decisions and safeguarding issues, should be on an equal footing too with other professionals.
I said to Chris, a friend of mine living well with dementia recently, “GPs will even be in a good position to coordinate information”.
I was in fact repeating words from a GP.
Chris, “So why don’t they?”
In certain respects, in designing a system you wouldn’t wish to start from here.
Without the focus on ‘budgets’ which do not necessarily deliver the ‘right kind’ of choice for the person with the health and care matters, it’s important that people with dementia have rights to a personal care plan, which is responsive to that person’s needs in real time. Knowing someone’s background is particularly essential in people with Alzheimer’s disease where longer term memories may be more intact. Knowing someone as a person is of course at the heart of personhood, through maybe a ‘life story’.
I don’t think it should be a ‘luxury’ of people with dementia following them after diagnosis through the system. I think, in fact, it should be an essential aspiration. It’s really important that somebody can cross off inappropriate medications, such as perhaps antipsychotics, on a drug chart if the person with dementia might not benefit.
It might help if a dementia specialist companion could spot problems in overmedicated people for blood pressure, for example. These individuals might become at risk of falls (and subsequent bone fractures if living with osteoporosis). Or somebody may be developing constipation or a stinging urine, becoming acutely confused. Dementia is not simply caused by conditions of old age, but frail individuals can do particularly bad when coming into contact with hospitals.
In the scenario that a person with dementia at any stage does need to go into hospital, it would help enormously if there could be continuity of care between the community and hospital. People with all types of dementia can find unfamiliarity, in people and environments, extremely mentally distressing, and this can be detrimental to their physical health (taking a whole person care approach). There are few people better than paid carers, with pay above the national minimum wage, and not on zero hour contracts, and unpaid caregivers including friends and family, to inform on these care plans, but the person living with dementia is the one for whom the plan is being designed.
All staff clearly need to be informed and skilled about dementia, and it is vital that resources are put aside for the adequate training of the workforce. The workforce themselves want this.
It won’t be a surprise to you to learn that I see specialist nurses in prime position to offer a huge deal to the implementation of whole person care for dementia from the next Government?
I think my views are broadly consistent with a number of places. A number of reports across jurisdictions have been important in establishing the direction of travel for acute hospital care: e.g. “Dementia care in the acute hospital setting: issues and strategies: a report for Alzheimer’s Australia” (Alzheimer’s Australia, June 2014), “Spotlight on dementia care: a Health Foundation Improvement Report” (Health Foundation, October 2011), and the Royal College of Nursing’s report “Commitment to the care of people with dementia in hospital settings” (RCN, January 2013).
Examples of appropriate clinical leads, as the RCN themselves recognise, are “Admiral nurses” from the charity @DementiaUK, Alzheimer Scotland dementia specialist nurses, dementia champions in Scotland, and ward champions. Merely having ‘dementia advisors’ will be a case of the bland and ill informed leading the bland, on the other hand.
Like many other ‘once in a lifetime opportunities’, if we get this right the service could be vastly improved. I am confident that, if given the proper funding to make this happen, and strong leadership cascades downwards, the next Government will rise to this challenge.
Andy Burnham at the Fabian Society explaining a need for ‘whole person care’
Andy Burnham MP was invited to speak at an event called ‘Together’ on the subject of his Fabians pamphlet of the same name. This video was taken at the Labour Party Conference 2014.
Here he gives a vigorous defence of the proposed policy, not unique to this jurisdiction, on ‘whole person care’. In England, however, it will mean the formation of a National and Health Care Service. It therefore has profound policy implications.
Health and social care are ‘better together’, but a new government should still be cautious in delivery

Being cautious does not mean not changing things.
But for any change you have to take the key people with you.
For people who come into contact with the National Health Service or social care, the services are currently too bitty. It’s quite difficult to navigate your way through them.
There are further structural problems with how the service is organised for the NHS.
Ideally, there should be a consensus amongst members of political parties in doing something about the private finance initiative, or moving towards abolition of the purchaser-provider split?
Also, if ‘reconfigurations’ of NHS entities are deemed necessary, great thought should be put into the best clinically-driven as well as health economy method of doing so, involving meaningful engagement with persons and patients.
GPs, the backbone of the NHS, who are essential in providing a ‘proactive’ service for both health and illness, should not have their attention diverted into political attacks denigrating their value or into wondering whether their practices will have to shut.
With the default option now competitive tendering, this has generated a need for people who are savvy at making pitches and knowing the law. This is clearly a push of resources away from frontline care, the deliverers of which are expected to do ‘more for less’.
A brave Government will therefore have to organise better communication between the health and social care systems, and the person or patient.
It will also have to make technical adjustments to the law which currently puts competition law above clinical need (see for example the issue of mergers.)
Previous Governments in England have been great ‘reformers’, for example the Gladstone tenure.
Indeed, this Coalition inflicted a 493 page Act of parliament which had three aims: turbo boost a market, turbo boost getting rid of financially distressed hospitals, and pumping resources into an economic regulator.
This Act of parliament, accompanied by a £2 bn ‘reorganisation’, had nothing to do with patient safety. Indeed, the only clause in the Act acts to abolish the National Patient Safety Agency.
The new Government will have to be brave about funding.
For a Government of socialist flavour, this will mean avoiding at all costs compulsory personal budgets which are the shoo-horn for neoliberalism; and avoiding co-payments, which end up being a tax on the ill.
The focus of the new Government should be offering a pleasurable experience for any person using health and social care services, such that each member of the public is treated as an unique individual.
That individual is not merely a ‘collection of problems’, but has a past, present, and future, and interacts with his or her own social networks, community and environment.
The discussion to be had will at stage have to be a serious one, and there will be a need to engage the mainstream media in such a way that they evidently have had enthusiasm for (over Douglas Caswell, UKIP or Nigel Farage).
So the next Government is likely to introduce integrated or whole person care, but this should be clinically driven. Serious thought should be making each pound of healthcare spending go as far as possible, but ultimately there should be an acknowledgement that you get what you pay for.
And furthermore an ‘unsustainable’ NHS does not merely mean a NHS you wish to starve of adequate funds.
The NHS and social care systems do contain outstanding, hardworking professionals, and with the correct leadership the NHS can continue to be the ‘envy of the world’.
Hundreds of thousands of people are marching to London for September 6th to show just that.

‘Whole person care’ has been done by family doctors for years. We do not need yet more managerial silos.
“No matter how busy you are, you must take time to make the other person feel important.” -Mary Kay Ash
People living with dementia are generally not kept ‘in the loop’ about major decisions in the running of their health and social care services.
Whereas some politicians clearly see some capital in promoting dementia, it is hard to distinguish whether this is a genuine interest in dementia or a need to act as a broker for the pharmaceutical multinationals.
Likewise, ‘whole person care’ has all the makings of a great slogan, raising expectations beyond a reality. The concept is, irrespective of funding mechanisms in various jurisdictions, is that you see beyond a list of clinical diagnoses.
You ‘take notice’ of a person when they’re not ill; this has become a very potent concept with realisation that many people live with conditions but are not symptomatic of any illness. And more than ‘taking notice’, you actively help with issues that can help with wellbeing (such as lifestyle, advice about enforcement of legal rights, good quality housing, access to appropriate benefits, proper design of the environment.)
My working definition of ‘personhood’ is somewhat more basic than that of Carl Jung and Tom Kitwood, whose feet I should never wish to tread on intellectually. But my definition is simply that any person living well is at ease with his or her own past, present and future, and his or her environment including community.
In my view, therefore, it is refutable that there are sources of expertise for whole person care outside the medical profession, including unpaid carers, nurses, occupational therapists, physiotherapists and speech and language t harpists, as well as other persons with dementia.
Health and social care in England currently feels like fragmented different worlds, with a complete lack of communication between them. The lack of continuity of care leads to operational problems in offering health and social care. And if you reduce people to a list of diagnoses, you ignore the past of that person.
For example, a concert pianist might have rather different views about developing rheumatoid disease in his fingers than a building site construction worker has about developing the same disease in his.
What is driving the cost of the NHS budget in England, however, in England is technology not the ageing population; half of England’s current NHS budget goes to people below the age of 65 (Iliffe and Manthorpe, 2014).
There is an important how it could be delivered. An anticipated problem is that how the ‘integrator’ will include services including the private sector as well as possibly community care units; in this rôle the integrator ends up subcontracting services, potentially subverting the original ethos of the CCG process. This is a recipe for fast tracking resources away from the State to the private sector, highly dependent on corporates acting like ‘good citizens’.
Certainly, electronic patient records shared between entities would help.
But there is a temptation, and indeed danger, that ‘whole person care’ becomes a wish list for multinational corporations; e.g. “big is best” and implementation of massive IT projects. Focusing on a person’s beliefs, concerns and expectations, however, has been done successfully for decades by many family doctors, who have been subject to the same principles of regulation over confidentiality and disclosure as relevant to IT systems. By this I mean family doctors who spent ages talking to persons and their families in various environments such as home visits, rather than doctors in modern general practice guillotined by the seven minute time slot.
The current UK Labour opposition is wishing to implement ‘whole person care’ in its next government, and it of course it remains to be seen whether they will be given a mandate for doing so.
But, if so, policy has a delicate balance to run between recognising specialist clinical care in dementia, e.g. through Admiral nurses, in England, and not creating new “silos”, e.g. whole person care nurses in dementia.
Creation of new silos from management and management consultants, apart from all else, encourages insurance-based funding mechanisms for single diseases rather than mechanisms which encourage fair treatment of the whole person in an equitable way.
The strength about the ‘whole person care’ construct is that persons have their physical health, social care and mental health needs considered in the round, with an understanding that comorbities can act both ways: physical illness can cause mental illness, and vice versa.
Whilst it might seem like an experiment in England, and could not have come at a worse time for the NHS with campaigners feeling that changes in health policy are essentially a rouse for backdoor privatisation, the approach of ‘whole person care’ is particularly relevant to dementia, and other jurisdictions, for example California, have already made good progress with it.
Could the “social impact bond” help to improve services in dementia care?
This blogpost first appeared on the ‘Living well with dementia’ blog yesterday.
It’s impossible to ignore the occasional spate of reports of ‘care home scandals’, including Winterbourne View and Orchid View.
Whilst a direction of travel might be to advance people living ‘successfully’ as long as possible independently, there’ll be some people for whom a care home might be appropriate. There are particular aims of policy designed to support living well with dementia, such as combating loneliness and providing meaningful leisure activities, which can possibly be achieved through high quality care homes.
It’s pretty often that you hear of social care being “on its knees”, due to drastic chronic underfunding. A concern about attracting investment from the private sector is that this will help to accelerate the lack of financial resource allocation from the State. And yet this is the opposite to the argument of resources ‘leeching’ out of the public sector into the private sector.
In terms of the ‘business model’, there are concerns that, to maximise shareholder dividend, staff will not be incentivised to ‘care well’, if they are barely meeting the requirements of the national minimum wage. Whilst the employer emphasises ‘flexibility’ of zero hours contracts, for many such contracts are symbolic of a lack of commitment for sustained employment by the employer.
So the idea of bonds being used to prop up dementia care, currently one of the three big arms of the Prime Minister’s Dementia Challenge, has gained some momentum, for example here. Bonds are effectively “IOUs“, and concerns remain for them as in the private finance initiative – such as who actually benefits, the prolonged threat of penalty for not being able to meet your loan repayments, the issue of who decides the outcomes by which performance will be assessed, and who actually manages or controls the enterprise.
Social Impact Bonds (SIBs) are depicted as “a way of enabling innovation, creating flexible contracts around social outcomes and providing linked investment“. But for some, they are a vehicle for enabling ‘privatisation by stealth’.
The current Labour opposition officially is trying to distance itself from any mechanisms promoting the privatisation of the NHS, and yet it is known Chris Ham and Norman Lamb wish to publish a report imminently on the possible use of SIBs in policy under the auspices of the King’s Fund.
This is the title slide of Hazel Blears’ presentation for the Alzheimer’s Show on Friday.

And here is a section of her talk.
[apologies for the sound quality]
Hazel has a strong personal attachment to campaigning on dementia, and is particularly interested and influential in the direction of travel, not least in her rôle as Vice Chair of the All Party Parliamentary Group on dementia, a cross party group made up of MPs and Peers with an interest in dementia.
Andy Burnham MP, Shadow Secretary of State for Health, has made it clear that it is his firm and settled intention to repeal the Health and Social Care Act (2012). The current Prime Minister’s Dementia Challenge is to come to an end officially in March 2015.
Dementia UK set up some time ago its innovative ‘Admiral Nurses’ scheme, to provide specialist nurses who could help people with dementia and family carers to improve the quality of life of people with dementia and family carers.
Burnham has also let it be known that he intends to subsume social care within the NHS under the construct of ‘whole person care’. Whichever various formulations of ‘whole person care’ you look at, you tend to find a ‘care coordinator’ somewhere. The exact job description of the care coordinator, nor indeed which specialisms might be best suited to accomplish this rôle, is somewhat unclear presently.
But it is all too common to hear of people being diagnosed with dementia being ‘lost in the system’, sometimes for years without follow up.
A “care coordinator” might help to boost access to the following services: emotional support, enable short breaks for people with dementia and anyone in a caring role, promote nutritious meals, ensure medications are given on time, ensure the correct medications have been subscribed (for example avoiding antipsychotic medications in individuals who might be unsuited to these), advice about suitable housing (including downsizing), ensure all physical commodities are properly medically managed; and so the list goes on.
I feel it’s pretty likely there’ll be a ‘first mover advantage‘ effect for any entity which takes up this coordination rôle in dementia care. But the tension between this and the Opposition’s policy is palpable: one cannot talk of this entity being ‘the first to enter the market’, as many wish (and expect) Labour to abolish the internal market in health care.
Such a coordinating entity could well be a recipient of a SIB – but is this like the PFI of social care? PFI by and large has an incredibly negative press amongst members of the general public.
But on the other hand, is it vindictive to prevent a social enterprise from pitching from such a service? If that entity has the technical ‘know how’ to run operations nationally competently and at a reasonable price, would that be preferable to the State running such services when projects such as NHS IT and universal credit have not gone terribly well?
In our jurisdiction, private companies can hide easily being a corporate veil, and are for example currently not readily accountable through freedom of information legislation. This is despite numerous requests to Jeremy Hunt in parliament about parity in disclosure requirements from both private and public providers.
And the track record of some outsourcing companies in the private sector, it is said, has been terrible.
Jeremy Hunt and Norman Lamb are currently in control of NHS and care policy, but there might be a fundamental change in direction from the next Government.
Or there might not be.

Could the “social impact bond” help to improve services in dementia care?
It’s impossible to ignore the occasional spate of reports of ‘care home scandals’, including Winterbourne View and Orchid View.
Whilst a direction of travel might be to advance people living ‘successfully’ as long as possible independently, there’ll be some people for whom a care home might be appropriate. There are particular aims of policy designed to support living well with dementia, such as combating loneliness and providing meaningful leisure activities, which can possibly be achieved through high quality care homes.
It’s pretty often that you hear of social care being “on its knees”, due to drastic chronic underfunding. A concern about attracting investment from the private sector is that this will help to accelerate the lack of financial resource allocation from the State. And yet this is the opposite to the argument of resources ‘leeching’ out of the public sector into the private sector.
In terms of the ‘business model’, there are concerns that, to maximise shareholder dividend, staff will not be incentivised to ‘care well’, if they are barely meeting the requirements of the national minimum wage. Whilst the employer emphasises ‘flexibility’ of zero hours contracts, for many such contracts are symbolic of a lack of commitment for sustained employment by the employer.
So the idea of bonds being used to prop up dementia care, currently one of the three big arms of the Prime Minister’s Dementia Challenge, has gained some momentum, for example here. Bonds are effectively “IOUs“, and concerns remain for them as in the private finance initiative – such as who actually benefits, the prolonged threat of penalty for not being able to meet your loan repayments, the issue of who decides the outcomes by which performance will be assessed, and who actually manages or controls the enterprise.
Social Impact Bonds (SIBs) are depicted as “a way of enabling innovation, creating flexible contracts around social outcomes and providing linked investment“. But for some, they are a vehicle for enabling ‘privatisation by stealth’.
The current Labour opposition officially is trying to distance itself from any mechanisms promoting the privatisation of the NHS, and yet it is known Chris Ham and Norman Lamb wish to publish a report imminently on the possible use of SIBs in policy under the auspices of the King’s Fund.
This is the title slide of Hazel Blears’ presentation for the Alzheimer’s Show on Friday.
And here is a section of her talk.
[apologies for the sound quality]
Hazel has a strong personal attachment to campaigning on dementia, and is particularly interested and influential in the direction of travel, not least in her rôle as Vice Chair of the All Party Parliamentary Group on dementia, a cross party group made up of MPs and Peers with an interest in dementia.
Andy Burnham MP, Shadow Secretary of State for Health, has made it clear that it is his firm and settled intention to repeal the Health and Social Care Act (2012). The current Prime Minister’s Dementia Challenge is to come to an end officially in March 2015.
Dementia UK set up some time ago its innovative ‘Admiral Nurses’ scheme, to provide specialist nurses who could help people with dementia and family carers to improve the quality of life of people with dementia and family carers.
Burnham has also let it be known that he intends to subsume social care within the NHS under the construct of ‘whole person care’. Whichever various formulations of ‘whole person care’ you look at, you tend to find a ‘care coordinator’ somewhere. The exact job description of the care coordinator, nor indeed which specialisms might be best suited to accomplish this rôle, is somewhat unclear presently.
But it is all too common to hear of people being diagnosed with dementia being ‘lost in the system’, sometimes for years without follow up.
A “care coordinator” might help to boost access to the following services: emotional support, enable short breaks for people with dementia and anyone in a caring role, promote nutritious meals, ensure medications are given on time, ensure the correct medications have been subscribed (for example avoiding antipsychotic medications in individuals who might be unsuited to these), advice about suitable housing (including downsizing), ensure all physical commodities are properly medically managed; and so the list goes on.
I feel it’s pretty likely there’ll be a ‘first mover advantage‘ effect for any entity which takes up this coordination rôle in dementia care. But the tension between this and the Opposition’s policy is palpable: one cannot talk of this entity being ‘the first to enter the market’, as many wish (and expect) Labour to abolish the internal market in health care.
Such a coordinating entity could well be a recipient of a SIB – but is this like the PFI of social care? PFI by and large has an incredibly negative press amongst members of the general public.
But on the other hand, is it vindictive to prevent a social enterprise from pitching from such a service? If that entity has the technical ‘know how’ to run operations nationally competently and at a reasonable price, would that be preferable to the State running such services when projects such as NHS IT and universal credit have not gone terribly well?
In our jurisdiction, private companies can hide easily being a corporate veil, and are for example currently not readily accountable through freedom of information legislation. This is despite numerous requests to Jeremy Hunt in parliament about parity in disclosure requirements from both private and public providers.
And the track record of some outsourcing companies in the private sector, it is said, has been terrible.
Jeremy Hunt and Norman Lamb are currently in control of NHS and care policy, but there might be a fundamental change in direction from the next Government.
Or there might not be.
Dementia care in the whole person care age
The Australian jurisdiction have recently provided some helpful inroads here.
The narrative has changed from one of incessantly referring to people living with dementia as a ‘burden’ on the rest of society. For example, to push a sense of urgency that we have an ‘ageing population timebomb’, the cost of the ageing people with dementia flies completely in the face of other public health campaigns which emphasise, for example, “dementia is not a natural part of ageing”.
“The NHS as a whole and individual hospitals recognise that dementia is a significant, growing and costly problem for them” is the opening gambit of the Alzheimer’s Society “Counting the cost” report.
An easy to use online resource, Valuing People from Alzheimer’s Australia has been developed in collaboration with community aged care providers who have helpful in stablishing a person centred approach to service delivery.
Person centred care is a development to provide ervices provided in a way that is respectful of, and responsive to, the preferences, needs and values of people and those in the care and support network.
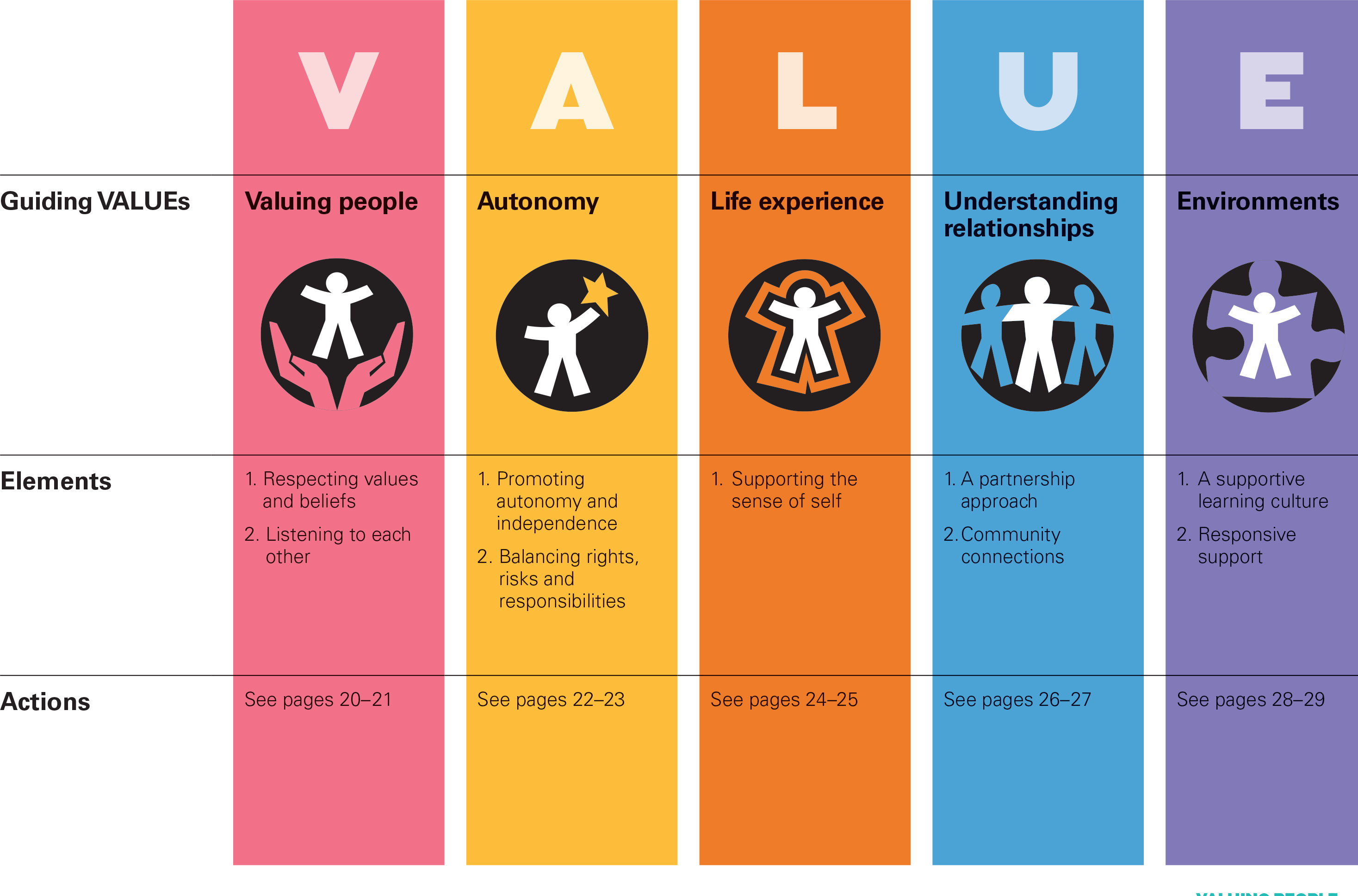
I cannot recommend this resource highly enough. The main source is here.
In fact, it summarises succinctly the conclusions I came to after my exploration of personhood in my book ‘Living well with dementia’. The late great Prof Tom Kitwood said of personhood, “It is a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being. It implies recognition, respect and trust”.
If a Labour government is elected on May 8th 2015, the first necessary step is to legislate for the repeal of the Health and Social Care Act (2012) and to enact new legislation to allow for integrated packages provided they are justified by clinical outcome. For this to happen, it will be necessary for Labour to undergo a ‘conscious uncoupling’ from all the baggage of EU competition law. For this, it is essential also that the UK government is able to carve out provisions from the investor protection clauses and/or the rest of the EU-US free trade treaty (TTIP).
The “whole person care model” has become attractive to those who wish to break down silos between different physical health, mental health and social care “silos”. It has been worked up in various guises by various parties.
A helpful construct is provided in the document, “Healthcare for complex populations: the power of whole-person care models” originally published by Booz & Company in 2013.
A major problem with dementia care, however it is delivered, is that it is full of divisions: public vs private care, fragmented vs national care, competitive vs integrated models. Operating in silos can’t work because of the nature of the dementias: the mood and cognition of a person with dementia profoundly affects how they might interact with the outside world, for example perform activities in the outside world. And we know that taking part in leisure activities can promote a good quality of life.
Their model is, though, a useful starting point.

Dementia cannot be only addressed by the medical model. In fact, it is my sincere belief that it would be highly dangerous to put all your eggs in the physical health basket, without due attention to mental health or social care. For example, last week in Stockholm, the international conference on Parkinson’s disease, a condition typified by a resting tremor, rigidity and slowness of movement, which can progress to a dementia, often is found to have as heralding symptoms changes in cognition and mood.
So it’s pretty clear to me that we will have to embark on a system of multidisciplinary professionals who could all have a part to play in the wellbeing of a person with dementia, depending on his or her own stage in life, and ability or need to live independently. “Care coordinators” have traditionally been defined incredibly badly, but we do need such an identity to navigate people with dementia, and actors in the care and support network, through the maze.
“Care collaborators” in their construct are very wonkily articulated, like “pre-distribution”, but the concept is not stupid. In fact it is very good. One idea is that people with dementia could act as support as other people with dementia, for people on receiving a diagnosis of dementia. The rationale for this is that people living with long term conditions, such as for example recovery from alcoholism, often draw much support from other people living with other long term conditions, away from a medical model. There needs to be safeguards in the system to safeguard against a lot of unpaid goodwill (which currently exists in the system.)
Informatics would have a really helpful rôle here, being worked up in telecare and assistive technology. But even simple disruptions such as a person living with dementia at risk of falling from problems with spatial depth perception being able to ‘hot email’ a care coordinator about perceived problems could trigger, say, an early warning system. And with various agents in the provision of care being involved in differing extents it will be up to NHS England to work out how best to implement a single accountable tariff. Falls are just the sort of ‘outcome metric’ which could be used to determine whether this policy of ‘whole person care’ for people living with dementia is working. And, even though everyone ‘trots it out’, the performance on avoided hospital admissions could be put into the mixer. It’s already well recognised that people with dementia can become very disoriented in hospital, and, and despite the best efforts of those trying to improve the acute care pathway, people with dementia can often be better off away from hospital in the community. But it’s imperative that care in the community is not a second-rate service compared to secondary care, and proper resourcing of community whole person care is essential for this before any reconfiguration in acute hospital services.
But the private sector has become such a ‘bogey term’ after arguably the current Government overplayed their hand with the £3bn Act of parliament which turbo-boosted a transfer of resource allocation from the public to private sector. Any incoming government will have to be particularly sensitive to this, as this is a risk in strategy for the NHS.
In October 2005, Harold Sirkin, Perry Keenan and Alan Jackson published a highly influential article in the Harvard Business Review entitled “The hard side of change management“. Whilst much play has in fact been made of politicians having to be distant from running the NHS, a completely lubricous line of attack when it is alleged that Jeremy Hunt talks regularly to senior managers and regulators in the NHS, the benefits of clear political leadership from an incoming Labour government are clear.
Andy Burnham MP has already nailed his colours to the mast of ‘whole person care’ on various occasions, and it is clear that the success of this ambitious large scale transformation depends on clear leadership and teamwork from bright managers. Take for example the DICE criteria from Sirkin, Keenan and Jackson:

But this is perfectly possible from an incoming Government. The National Health Service has a chance to lead on something truly innovative, learning from the experience of other jurisdictions such as Australia and the USA.
As alluded to in the new resource from the Alzheimer’s Australia, this cultural change will require substantial ‘unfreezing’ from the current mindset for provision of care for people with dementia. It will require a change in explicit and implicit sources of knowledge and behaviours, and will need to be carefully brought about by learning from the successes and failures of pockets of implementation.
The whole project’s pretty high risk, but the rewards for people living with dementia, and members of the care and support network, are potentially vast. But it does require the implementation of a very clear vision.
[First posted on the 'Living well with dementia' blog]

A large scale cultural national transformation is needed to drive whole person care in dementia
I’ll be blunt. It’s my dream for the #NHS to run a proactive not reactive service, promoting the whole person living well with dementia.
The Australian jurisdiction have recently provided some helpful inroads here.
The narrative has changed from one of incessantly referring to people living with dementia as a ‘burden’ on the rest of society. For example, to push a sense of urgency that we have an ‘ageing population timebomb’, the cost of the ageing people with dementia flies completely in the face of other public health campaigns which emphasise, for example, “dementia is not a natural part of ageing”.
“The NHS as a whole and individual hospitals recognise that dementia is a significant, growing and costly problem for them” is the opening gambit of the Alzheimer’s Society “Counting the cost” report.
An easy to use online resource, Valuing People from Alzheimer’s Australia has been developed in collaboration with community aged care providers who have helpful in stablishing a person centred approach to service delivery.
Person centred care is a development to provide ervices provided in a way that is respectful of, and responsive to, the preferences, needs and values of people and those in the care and support network.
I cannot recommend this resource highly enough. The main source is here.
In fact, it summarises succinctly the conclusions I came to after my exploration of personhood in my book ‘Living well with dementia’. The late great Prof Tom Kitwood said of personhood, “It is a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being. It implies recognition, respect and trust”.
If a Labour government is elected on May 8th 2015, the first necessary step is to legislate for the repeal of the Health and Social Care Act (2012) and to enact new legislation to allow for integrated packages provided they are justified by clinical outcome. For this to happen, it will be necessary for Labour to undergo a ‘conscious uncoupling’ from all the baggage of EU competition law. For this, it is essential also that the UK government is able to carve out provisions from the investor protection clauses and/or the rest of the EU-US free trade treaty (TTIP).
The “whole person care model” has become attractive to those who wish to break down silos between different physical health, mental health and social care “silos”. It has been worked up in various guises by various parties.
A helpful construct is provided in the document, “Healthcare for complex populations: the power of whole-person care models” originally published by Booz & Company in 2013.
A major problem with dementia care, however it is delivered, is that it is full of divisions: public vs private care, fragmented vs national care, competitive vs integrated models. Operating in silos can’t work because of the nature of the dementias: the mood and cognition of a person with dementia profoundly affects how they might interact with the outside world, for example perform activities in the outside world. And we know that taking part in leisure activities can promote a good quality of life.
Their model is, though, a useful starting point.
Dementia cannot be only addressed by the medical model. In fact, it is my sincere belief that it would be highly dangerous to put all your eggs in the physical health basket, without due attention to mental health or social care. For example, last week in Stockholm, the international conference on Parkinson’s disease, a condition typified by a resting tremor, rigidity and slowness of movement, which can progress to a dementia, often is found to have as heralding symptoms changes in cognition and mood.
So it’s pretty clear to me that we will have to embark on a system of multidisciplinary professionals who could all have a part to play in the wellbeing of a person with dementia, depending on his or her own stage in life, and ability or need to live independently. “Care coordinators” have traditionally been defined incredibly badly, but we do need such an identity to navigate people with dementia, and actors in the care and support network, through the maze.
“Care collaborators” in their construct are very wonkily articulated, like “pre-distribution”, but the concept is not stupid. In fact it is very good. One idea is that people with dementia could act as support as other people with dementia, for people on receiving a diagnosis of dementia. The rationale for this is that people living with long term conditions, such as for example recovery from alcoholism, often draw much support from other people living with other long term conditions, away from a medical model. There needs to be safeguards in the system to safeguard against a lot of unpaid goodwill (which currently exists in the system.)
Informatics would have a really helpful rôle here, being worked up in telecare and assistive technology. But even simple disruptions such as a person living with dementia at risk of falling from problems with spatial depth perception being able to ‘hot email’ a care coordinator about perceived problems could trigger, say, an early warning system. And with various agents in the provision of care being involved in differing extents it will be up to NHS England to work out how best to implement a single accountable tariff. Falls are just the sort of ‘outcome metric’ which could be used to determine whether this policy of ‘whole person care’ for people living with dementia is working. And, even though everyone ‘trots it out’, the performance on avoided hospital admissions could be put into the mixer. It’s already well recognised that people with dementia can become very disoriented in hospital, and, and despite the best efforts of those trying to improve the acute care pathway, people with dementia can often be better off away from hospital in the community. But it’s imperative that care in the community is not a second-rate service compared to secondary care, and proper resourcing of community whole person care is essential for this before any reconfiguration in acute hospital services.
But the private sector has become such a ‘bogey term’ after arguably the current Government overplayed their hand with the £3bn Act of parliament which turbo-boosted a transfer of resource allocation from the public to private sector. Any incoming government will have to be particularly sensitive to this, as this is a risk in strategy for the NHS.
In October 2005, Harold Sirkin, Perry Keenan and Alan Jackson published a highly influential article in the Harvard Business Review entitled “The hard side of change management“. Whilst much play has in fact been made of politicians having to be distant from running the NHS, a completely lubricous line of attack when it is alleged that Jeremy Hunt talks regularly to senior managers and regulators in the NHS, the benefits of clear political leadership from an incoming Labour government are clear.
Andy Burnham MP has already nailed his colours to the mast of ‘whole person care’ on various occasions, and it is clear that the success of this ambitious large scale transformation depends on clear leadership and teamwork from bright managers. Take for example the DICE criteria from Sirkin, Keenan and Jackson:
But this is perfectly possible from an incoming Government. The National Health Service has a chance to lead on something truly innovative, learning from the experience of other jurisdictions such as Australia and the USA.
As alluded to in the new resource from the Alzheimer’s Australia, this cultural change will require substantial ‘unfreezing’ from the current mindset for provision of care for people with dementia. It will require a change in explicit and implicit sources of knowledge and behaviours, and will need to be carefully brought about by learning from the successes and failures of pockets of implementation.
The whole project’s pretty high risk, but the rewards for people living with dementia, and members of the care and support network, are potentially vast. But it does require the implementation of a very clear vision.
[First posted on the 'Living well with dementia' blog]

“There’s more to a person than the dementia”. Why personhood matters for future dementia policy.
“Dementia Friends” is an initiative from the Alzheimer’s Society and Public Health England. In this series of blogpost, I take an independent look at each of the five core messages of “Dementia Friends” and I try to explain why they are extremely important for raising public awareness of the dementias.
There’s more to a person than the dementia.
In 1992, the late Prof Tom Kitwood founded Bradford Dementia Group, initially a side-line. Its philosophy is based on a “person-centred” approach, quite simply to “treat others in a way you yourself would like to be treated”.
A giant in dementia care and academia, I feel he will never bettered.
His obituary in the Independent newspaper is here.
Personhood is the status of being a person. Its importance transcends medicine, nursing, policy, philosophy, ethics and law even.
Kitwood (1997) claimed that personhood was sacred and unique and that every person had an ethical status and should be treated with deep respect.
A really helpful exploration of this is found here on the @AlzheimerEurope website.
Personhood in dementia is of course at risk of ‘paralyis by analysis’, but the acknowledgement that personhood depends on the interaction of a person with his or her environment is a fundamental one.
Placing that person in the context of his past and present (e.g. education, social circumstances) is fundamental. Without that context, you cannot understand that person’s future.
And how that person interacts with services in the community, e.g. housing associations, is crucial to our understanding of that lived experience of that person.
All this has fundamental implications for health policy in England.
Andy Burnham MP at the NHS Confederation 2014 said that he was concerned that the ‘Better Care Fund’ gives integration of health services a ‘bad name’.
It is of course possible to become focused on the minutiae of service delivery, for example shared electronic patient records and personal health budgets, if one is more concerned about the providers of care.
Ironically, the chief proponents of the catchphrase, “I don’t care who is providing my care” are actually intensely deeply worried about the fact it might NOT be a private health care provider.
Person-centered care is an approach which has been embraced by multi-national corporates too, so it is perhaps not altogether a surprise that Simon Stevens, the current CEO of NHS England, might be sympathetic to the approach.
Whole-person care has seen all sorts of descriptions, including IPPR, the Fabians, and an analysis from Sir John Oldham’s Commission, and “Strategy&“, for example.
The focus of the National Health Service though, in meeting their ‘efficiency savings’, has somewhat drifted into a ‘Now serving number 43′ approach.
When I went to have a blood test in the NHS earlier this week, I thought I had wandered into a delicatessen by accident.

But ‘whole person care’ would represent a fundamental change in direction from a future Government.
Under this construct, social care would become subsumed under the NHS such that health and care could be unified at last. Possibly it paves the way for a National Care Service at some later date too.
But treating a person not a diagnosis is of course extremely important, lying somewhat uneasily with a public approach of treating numbers: for example, a need to increase dementia diagnosis rates, despite the NHS patient’s own consent for such a diagnosis.
I have seen this with my own eyes, as indeed anyone who has been an inpatient in the NHS has. Stripped of identity through the ritualistic wearing of NHS pyjamas, you become known to staff by your bed number rather than your name, or known by your diagnosis. This is clearly not right, despite years of professional training for current NHS staff. This is why the campaigning by Kate Granger (“#hellomynameis”) is so important.
It is still the case that many people’s experiences of when a family relative becomes an inpatient in the National Health Service is a miserable one. I have been – albeit a long time ago – as a medical student on ward rounds in Cambridge where a neurosurgeon will say openly, “He has dementia”, and move onto the next patient.
So the message of @DementiaFriends is a crucial one.
Together with the other four messages, that dementia is caused by a diseases of the brain, it’s possible to live well with dementia, dementia is not just about losing your memory, dementia is not part of normal ageing, the notion that there’s more to a person than the dementia is especially important.
And apart from anything else, many people living with dementia also have other medical conditions.
And apart from anything else, many people living with dementia also have amazing other skills, such as cooking (Kate Swaffer), fishing (Norman McNamara), and encouraging others (see for example Chris Roberts’ great contributions to the community.)
References
Kitwood, T. (1997).Dementia reconsidered: the person comes first. Open University Press.
