Home » Posts tagged 'policy'
Tag Archives: policy

A wellbeing economics prism to ‘dementia friendly communities’

There has been some startling consensus over the national political settlement, including as it applies to English dementia policy.
There has generally been cross-party agreement about personal budgets, even though the ‘direction of travel’ from the UK Labour Party is to favour a ‘rights based approach’ to advance choice and control rather than merely though a financial budget.
There are good reasons not to put many eggs into the personal budget basket for dementia; these include how the range of ‘products and services’ for dementia can be in places rather underdeveloped, and the formidable potential safeguarding issues for certain vulnerable individuals living with dementia.
Another consensus is to be found in wellbeing, or living well.
I was struck by a recent recommendation from the first ever report by the All Party Parliamentary Group on Wellbeing Economics, entitled “Wellbeing in four policy areas” (published September 2014):
“Health and Wellbeing Boards should bring together public health professionals, Clinical Commissioning Groups, GPs, and other stakeholders to develop strategies for ‘whole person care’ which effectively integrate mental and physical health.”
Unknown to me, they had been doing great work even prior to the last UK election. Their ultimate aim, unsurprisingly, is to make wellbeing into a pervasive policy strand that straddles across all areas of life.
This ‘wellbeing prism‘ has impacted on various areas of policy, I suspect, in the past, like ‘The Big Society’. I have always felt that the ‘dementia friendly communities’ policy in England, heralded in the Prime Minister Dementia Challenge, although clearly having some roots in the Japanese ‘caravans’ ‘befriending’, fits well into the ‘Big Society’ ethos.
One of the problems with both ‘dementia friendly communities’ and the ‘Big Society’ has been whether the civic sense of solidarity might diminish statutory obligations.
I have witnessed the problems with this, first hand, in writing my book ‘Living better with dementia: champions for enhanced communities’ which I hope to publish next year. The same tensions exist in statutory obligations in the form of equality and human rights law, and statutory entities, and non-statutory community-driven ones there too.
As the O’Donnell Report puts it, wellbeing:
‘leads us to place greater weight on the human factors that explain the big differences in wellbeing, but that tend to be pushed to the margins in traditional policy making’.
There has been some focus on how we need an ‘alternative measure to GDP’. Cynics unsurprisingly argued that such a measure might inevitably gather political momentum given the problems we have had with economic growth in the last few years.
But the general arguments from the APPG on wellbeing economics make an enormous amount of sense to me. Julian Huppert is the current MP for Cambridge, and I dedicated my current book to his mother Prof Felicia Huppert, Professor of Wellbeing at Cambridge. Julian is, to my knowledge, on the APPG on wellbeing economics.
The next parliament, I hope, will see a continuation of a focus on wellbeing in policy. As pointed out in their first report, there is considerable overlap with the wellbeing field and that of the ‘social determinants of health’.
In my next book, I continue with analysing this overlap, using housing as an example. Housing is clearly an area which impacts upon the quality of life of people living well with dementia, not just from architectural perspectives of design, but also how spaces are organised to facilitate personal interaction.
Similarly, planning in the built environment is important, with considerations of inclusivity and accessibility.
These are all ‘desirable’ (or even ‘essential’?) attributes of the ‘dementia friendly communities’.
Unpaid caregivers and paid carers, like professionals, are vital in the social capital of these communities too.
It is said elsewhere that while there has been a strong focus on GDP-style economics the lack of focus on wellbeing means that we do not touch upon many policy areas, such as strife caused by marital breakdown.
I feel that this touches upon another tension of dementia policy, this time at a global level.
We know, for example, loneliness is an important source of emotional morbidity for people who have received a probable diagnosis of dementia all around the world.
Also, jurisdictions have been encouraging the aspiration of people living with dementia to live independently; in other words, not institutionalised in some form, as long as possible. This, I think, is intuitively right, so long as it is not perceived as a ‘failure’ if somebody does need the support and care provided from an institution.
There are some people who believe that the ‘successful ageing’ and ‘ageing in place’ movements have overplayed their hand; with cynics pointing out they fit nicely into the ‘small state’ narrative, a rather individualistic narrative, which takes little account of our cohesion as a society.
But this I genuinely think would be to analyse the issue too much but with one important proviso.
That proviso is that I don’t think you can value people simply in terms of their economic productivity.
I refer to this ‘equality of wellbeing’ even in my Introduction to my new book. Such equality of wellbeing throws a different light on equality driven by a purely economic sense.
In summary, in reference to the first ever report from the APPG in wellbeing economics, as the next Government and the Civil Service turn their minds into thinking about wellbeing and health policy, it will be forefront in their minds that we are about to embark on a huge behavioural change bringing together the NHS and social care.
This transformative change to ‘whole person care’ will bring great opportunities, I feel, as well as formidable challenges, not least funding considerations at a local and national level.
But I feel like the current Government, and like future ones hopefully, that a focus on wellbeing is desirable. O’Donnell is reported to have said, “If you can measure it, cherish it!”
Ideally, it would be nice to have some form of metric to see whether wellbeing interventions have any effect. I am mindful of the excellent work by Prof Sube Banerjee and colleagues on DemQoL, but others exist. And of course we should not want to end up where we started: in a target driven culture which hits targets but misses the point (as famously phrased by Sir David Nicholson).
There might be desirable effects of such metrics, though. They could be formally put into grants for research for living well with dementia; to see whether some activities are more beneficial in care homes, where there is a high proportion of people living with dementia often, than others.
The Baroness Sally Greengross asked me to put in a chapter on arts, music and creativity in my current book; so I did.
But, as the new APPG report on dementia this year rightly discusses, such a metric could be used to incentivise the use of the arts and creativity to improve the quality of life of individuals in society. And I have no doubt whatsoever that arts and creativity are a linchpin of dementia friendly communities too.
The APPG in dementia earlier this year, under Sally’s leadership, urged the importance of high quality commissioning in post-diagnostic support for dementia.
If we have more a ‘joined up’ approach to commissioning and policy, in parallel with the breaking down of silos needed for ‘whole person care’, I think England can consolidate its formidable lead in the ‘dementia friendly communities’ policy in the world.
Other jurisdictions might even follow suit.
Recommended reading:
Gus O’Donnell (Chair) – and Angus Deaton, Martine Durand, David Halpern and Lord Richard Layard(2014). Wellbeing and Policy. London: Legatum Institute. Accessible at: http://www.li.com/docs/default-source/commission-on-wellbeing-and-policy/commission-on-wellbeing-and-policy-report—march-2014-pdf.pdf?sfvrsn=2
Wellbeing in four policy areas: Report by the All-Party Parliamentary Group on Wellbeing Economics (September 2014). Accessible at: http://b.3cdn.net/nefoundation/ccdf9782b6d8700f7c_lcm6i2ed7.pdf
All-Party Parliamentary Group on Dementia assesses progress of the National Dementia Strategy for England
2014 report: The National Dementia Strategy: Change, progress and priorities
Accessible at: http://www.alzheimers.org.uk/site/scripts/download_info.php?downloadID=1447

George Osborne’s “duty of candour”

I’m pretty certain that George Osborne is actually quite a nice guy.
I know of people who know people who’ve had dealings with him on a chat-chat level. And apparently he’s perfectly harmless.
George Osborne’s one job was to run the UK economy. And he’s failed at that.
The LibDems had a job to deliver to deliver ‘a strong economy and fair society’. Add in the murder of English legal aid, we can confidently say the LibDems failed on their side of the bargain.
It doesn’t matter which particular metric you wish to use. The only good soundbites came from the rose garden soundbites from the Office for Budget Responsibility in 2010 informing us of the shiny uplands.
But it turns out that the incline of the uplands was steeper than we first thought. Osborne kept on telling us this was due to the Eurozone crisis. This is the same Eurozone crisis which has suddenly disappeared with one us being one of the ‘best performing economies’ in the G20.
Osborne’s pitch is that he needs just a little more time, as the famous Reet Petite song goes. He needs to ‘finish the job’ to put the UK back ‘on the path to prosperity’. This is the “long term economic plan”.
Except… the long term economic plan is not working. A record number apparently in employment with really bad income from as receipts? How did that happen?
Was it something, perhaps, to do with a record number on low security “zero hour contracts”, topped up with tax credits, who do not end up paying much income to the State?
The Conservative (Ronald Reagan) doctrine of a small state is creepy. The drastic diet of an ‘over bloated’ State has left a State which is anorexic – and which is dangerously fragile.
The Coalition’s anorexic state is consequently far from resilient. Most reasonable people agree that the anorexic State would simply be unable to cope with the Conservatives’ further planned cuts in the next term of office.
This is not the “shock doctrine” of Greece. It is a reality of something happening in the UK not seen since the 1930s.
The current Government has successfully relaunched the ‘duty of candour’. The duty of candour, about being open in the NHS when a mistake is made, already existed in the regulatory codes of the clinical professionals.
And again – it’s not actually the legal instrument as drafted which is the main problem (though there are problems here). It’s whether anyone is observing them properly: see for example ‘wilful neglect’ (section 44 Mental Capacity Act), national minimum wage, or deprivation of liberty safeguards.
Osborne does not want to come even close for apologising for the record debt, the colossal borrowing, the poor living standards, or the fact that his plan to pay off the deficit has been tragically bad.
I don’t know whether this is a pride thing, but in the real world it has a knock on effect for whether you can pay for health and care. We know the social care budget has been on its knees for years.
Many NHS Trusts are in deficit. This can’t be due to the nurses, most of whom have not experienced a pay rise for years. It may be due to the salaries of top CEOs in the NHS who have to ‘deliver’ on metrics which do not necessarily reflect high quality care (e.g. the ‘four hour wait’). Or it could be due to paying off the loan prepayments for PFI under successive governments.
I really like members of the NHS campaigning parties, but discussions about the NHS have to be linked with the discussions of the state of the economy. It’s an elephant in the room.
Likewise, for all of the slagging off of the Efford Bill, I can guarantee that the statutory instrument UKIP would like to introduce would be far more controversial.
UKIP at least do entertain a discussion on leaving Europe and European law, sort of, even if they do not have any plans for the UK economy.
The Efford Bill was seen in some quarters as ‘the trojan horse for privatisation’, and I can see how interpretation of the clauses might result in this conclusion. I think a problem the Efford Bill was ‘reverse engineering’ to comply with EU competition law – i.e. clauses which perhaps sound as if they’re providing exemptions from EU law, but nobody actually knows.
Not even the best legal minds in the country, of which I am not one, know.
But the EU is founded on free movement of people. Tick – I remember working as a junior in NHS hospitals in London, and simply the day to day operations of these Trusts would have been impossible without the hard work of staff nurses predominantly from India and the Philippines.
And it is also founded on free movement of capital.
There is a genuine feeling of ‘I wouldn’t start from here’ for NHS campaigners in NHAP and Keep our NHS Public. They certainly want to go to a NHS inspired by Nye Bevan which had never heard of section 75 or TTIP.
But it is impossible to have this debate in the absence of a discussion of Europe. It’s impossible to have a debate on the NHS in the absence of a wider debate on the economy.
Russell Brand and Nigel Farage may be grandstanding, but on the face of it they seem to be coming from different places, and with huge followings.
This all matters as it is highly unlikely a Labour-UKIP coalition could be made to work on the NHS, given we know such little about what accommodations UKIP might make on EU competition law or the economy.
We don’t know whether UKIP supports ‘efficiency savings’ however.
All of this is not a leading to a conclusion of ‘Vote Labour’. Labour has not overtly apologised for some thorny apsects of NHS policy, in the same way that Osborne has not apologised over the economy. But it does seem to have apologised for a lot – like letting the market in too far – but curiously not PFI?
I am particularly mindful that there are some ‘real’ experts in NHS policy who are far more experienced and wiser than me. I am also in strong admiration of campaigners wherever they hail from; many of whom have experience of seeing patients regularly.
I never see patients unless they’re friends of mine; and that’s purely for social reasons.
But the next Government’s policy on the NHS will be severely affected by the mistakes of the current Government, part of which ironically has a catchphrase ‘strong economy, fair society’.

An overview of my book ‘Living better with dementia: champions for enhanced communities”.
I hope you find this overview of my book ‘Living better with dementia: champions for enhanced communities’ useful.
It is written by me.
And the Forewords are Prof Alistair Burns, the England clinical lead for dementia, Kate Swaffer (Alzheimer’s Australia, Dementia Alliance International, and University of Wollongong, Australia), Chris Roberts (Dementia Action Alliance Carers Call to Action, Dementia Alliance International), and Dr Peter Gordon (Consultant Psychiatrist in dementia and cognitive disorders, NHS Scotland).
It will primarily assess where we’ve got to, along with other countries, in improving diagnosis and post-diagnostic care, and assess realistically the work still yet to be done.
My thesis will articulate why the ‘reboot’ of the global “dementia friendly communities” must now take account of various issues to be meaningful. It will argue for a difference in emphasis from competitive ‘nudge’ towards universal legal and enforceable human rights promoting dignity and autonomy.
It will also argue that dementia friendly communities are meaningless unless there is a shift in the use of language away from ‘sufferers’ and ‘victims’, while paying tribute to the successful “Dementia Friends” initiative.
It will, further, argue that dementia friendly communities are best served by a large scale service transformation to ‘whole person care’, and provide the rationale for this. A critical factor for enhancing the quality of life of people living better with dementia will be to tackle meaningfully the social determinants of health, such as housing and education.
The thesis will also argue that dementia friendly communities must also value the behaviours, skills and knowledge of caregivers in wider support networks. This is essential for the development of a proactive service, with clinical specialist nursing input deservedly valued, especially given the enormous co-morbidity of dementia.
This title will be published by Jessica Kingsley Publishers, in early 2015.
Chapters overview
Chapter 1 provided an introduction to current policy in England, including a review of the need for a ‘timely diagnosis’ as well as a right to timely post-diagnostic care. This chapter also provided an overview of the current evidence base of the hugely popular “Dementia Friends” campaign run by the Alzheimer’s Society and Public Health England, to raise awareness about five key ‘facts’ about dementia. It was intended that this campaign should help to mitigate against stigma and discrimination that can be experienced by people living with dementia and their caregivers.
Chapter 2 comprised a preliminary analysis of stigma, citizenship and the notion of ‘living better with dementia’. This chapter explained the urgency of the need to “frame the narrative” properly. This chapter also introduced the “Dementia Alliance International” which has fast become a highly influential campaigning force by people living with dementia for people living with dementia.
Chapter 3 looked at the various issues facing the timely diagnosis and post-diagnostic support of people living with dementia from diverse cultural backgrounds, including people from black, Asian and ethnic minority backgrounds, people who are lesbian, bisexual, gay or transsexual, and people with prior learning difficulties.
Chapter 4 looked at the issue of how different jurisdictions around the world have formulated their national dementia strategies. Examples discussed of countries and continents were Africa, Australia, China, Europe, India, Japan, New Zealand, Puerto Rico and Scotland.
Chapter 5 looked at the intense care vs care debate which has now surfaced in young onset dementia, with a potentially problematic schism between resources being allocated into drugs for today and resources being used to fund adequately contemporary care to promote people living better with dementia. An example was discussed of how the policy of ‘Big Data’ had gathered momentum across a number of jurisdictions, offering personalised medicine as a further potential compontent of person-centred care. This chapter also considered the impact of the diagnosis of younger onset dementia on the partner of the person with dementia as well. A candid description was also given about the possible sequelae of the diagnosis of young onset dementia on employment, caregivers, and in social isolation.
Chapter 6 focused on delirium, or the acute confusional state, and dementia. It considered the NICE guidelines for delirium, and the pitfalls in considering the relationship between delirium and dementia in English policy.
Chapter 7 was the largest chapter in this book, and took as its theme care and support networks. An overview of how patient-centred care is different from person-centred care was given, and how person-centred care differs from relationship-centred care. The literature inevitably has thus far focused on the ‘dyadic relationship’ between the person with dementia and caregiver, but a need to enlarge this to a professional in a ‘triangle of care’ and extended social networks was further elaborated and emphasised. Finally, the importance of clinical specialist nurses in ‘dementia friendly communities’ was argued, as well as the Dementia Action Alliance’s “Carers Call to Action”. Different care settings were described, including care homes, hospitals – including acute hospital care, and intermediate care.
Chapter 8 considered eating for living well with dementia. This chapter considered enforceable standards in care homes, including protection against malnutrition or undernutrition. The main focus of the chapter was how people with dementia might present with alternations in their eating behaviour, and how the mealtime environment must be a vital consideration for living better with dementia.
Chapter 9 looked at a particular comorbidity, incontinence. The emphasis was on conservative approaches for living well with dementia and incontinence. Other issues considered were the impact of incontinence on personhood per se, and the possible impact on the move towards an institutional home.
Chapter 10 argued how the needs for people living better with dementia would be best served by a fully integrated health and social care service. This chapter provided the rationale behind this policy instrument in England. The chapter also considered various aspects of what would be likely to make ‘whole person care’ work, including data sharing, collaborative leadership, care-coordinators, responsible and accountable ‘self care’, and the multi-disciplinary team. This chapter also considered how it was impossible to divorce physical health from mental health and social care, and explained the intention of the longstanding drive towards ‘parity of esteem’ in English policy.
Chapter 11 considered the importance of the social determinants of health. A focus of this chapter was on education, and its impact on a person living with dementia. However, the main focus of this chapter was housing, including ‘dementia friendliness, downsizing, and green or public spaces.
Chapter 12 considered whether ‘wandering’ is the most appropriate term. The main emphasis of this chapter were the legal and ethical considerations in the use of ‘global positioning systems’ in enhancing the quality of life of persons with dementia and their closest ones.
Chapter 13 considered a number of important contemporary issues, with a main emphasis on human rights and “rights based approaches”. While there is no universal right to a budget, the implementation of personal budgets was discussed. The chapter progressed to consider a number of legal issues which are arising, including genetic discrimination in the US jurisdiction, dementia as a disability under the equality legislation in England, and the importance of rights-based approaches for autonomy and dignity. Finally, the issue of engagement was considered.
Chapter 14 was primarily concerned with art and creativity. This chapter took as its focus on how living with dementia could lead to art and creativity, and how the cultural needs of people living with dementia could best be furnished through laughter, poetry and art galleries or museums. This focus also looked at the exciting developments in our understanding of the perception of music in people living with dementia, and how music has the potential to enhance the quality of life for a person living well with dementia.
Chapter 15 looked at the triggering of football sporting memories in people living well with dementia. This chapter considered the cognitive neuroscience of the phenomenon of this triggering, and presented a synthesis of how the phenomenon could be best explained through understanding the role of emotional memory in memory retrieval, how autobiographical memories are represented in the human brain usually, the special relevance of faces or even smells such as “Bovril”.
Chapter 16 looked at the impact of various innovations in English dementia policy, giving as examples including service provision (such as the policy on reducing inappropriate use of antipsychotics or the policy in timely diagnosis) and research. This chapter also contemplated the principal factors affecting how innovations can become known, and what ultimately determines their success.
Chapter 17 looked at how leadership could be promoted by people living with dementia. This chapter considered who might lead the change, where and when, and why this change might be necessary to ‘recalibrate’ the current global debate about dementia. This chapter considered how change might be brought about from the edge, how silos might be avoided, the issue of ‘tempered radicals’ in the context of transformative change to wellbeing as an outcome; and finally how ‘Dementia Champions’ are vital for this change to be effected.
Please note that Beth is not endorsing this book – this image is entirely separate and is taken from the main event for G8 dementia – we’re all proud of Beth’s work meanwhile!


The chapter on art, music and creativity for my new book on living better with dementia
The following are the journal references for my chapter on art, music and creativity for my book “Living better with dementia: champions for enhanced friendly communities”. Please do let me know if you wish to have any further academic papers cited. And also please do let me know if you wish local initiatives or innovations to be featured in my chapter, and I will do my best to include them if appropriate.
Very many thanks.

Amaducci L, Grassi E, Boller F. Maurice Ravel and right-hemisphere musical creativity: influence of disease on his last musical works? Eur J Neurol. 2002 Jan;9(1):75-82.
Basaglia-Pappas S, Laterza M, Borg C, Richard-Mornas A, Favre E, Thomas-Antérion C. Exploration of verbal and non-verbal semantic knowledge and autobiographical memories starting from popular songs in Alzheimer’s disease. Int Psychogeriatr. 2013 May;25(5):785-95. doi: 10.1017/S1041610212002359. Epub 2013 Feb 7.
Beard, R.L. Art therapies and dementia care: A systematic review 2012 11: 633-656.
Bisiani L, Angus J. Doll therapy: a therapeutic means to meet past attachment needs and diminish behaviours of concern in a person living with dementia–a case study approach. Dementia (London). 2013 Jul;12(4):447-62. doi: 10.1177/1471301211431362. Epub 2012 Feb 15.
Blood AJ, Zatorre RJ. Intensely pleasurable responses to music correlate with activity in brain regions implicated in reward and emotion. Proc Natl Acad Sci U S A. 2001 Sep 25;98(20):11818-23.
Budrys V, Skullerud K, Petroska D, Lengveniene J, Kaubrys G. Dementia and art: neuronal intermediate filament inclusion disease and dissolution of artistic creativity. Eur Neurol. 2007;57(3):137-44. Epub 2007 Jan 10.
Camic PM, Chatterjee HJ. Museums and art galleries as partners for public health interventions. Perspect Public Health. 2013 Jan;133(1):66-71. doi: 10.1177/1757913912468523.
Camic PM, Tischler V, Pearman CH. Viewing and making art together: a multi-session art gallery-based intervention for people with dementia and their carers. Aging Ment Health. 2014 Mar;18(2):161-8. doi: 10.1080/13607863.2013.818101. Epub 2013 Jul 22.
Camic PM, Williams CM, Meeten F. Does a ‘Singing Together Group’ improve the quality of life of people with a dementia and their carers? A pilot evaluation study. Dementia (London). 2013 Mar;12(2):157-76. doi: 10.1177/1471301211422761. Epub 2011 Oct 31.
Chakravarty A. De novo development of artistic creativity in Alzheimer’s disease. Ann Indian Acad Neurol. 2011 Oct;14(4):291-4. doi: 10.4103/0972-2327.91953.
Crutch SJ, Isaacs R, Rossor MN. Some workmen can blame their tools: artistic change in an individual with Alzheimer’s disease. Lancet. 2001 Jun 30;357(9274):2129-33.
Eekelaar, C., Camic, P. M., Springham, N. Art galleries, episodic memory and verbal fluency in dementia: An exploratory study. Psychology of Aesthetics, Creativity, and the Arts, Vol 6(3), Aug 2012, 262-272.
Fletcher PD, Clark CN, Warren JD. Music, reward and frontotemporal dementia. Brain. 2014 Oct;137(Pt 10):e300. doi: 10.1093/brain/awu145. Epub 2014 Jun 11.
Fletcher PD, Downey LE, Witoonpanich P, Warren JD. The brain basis of musicophilia: evidence from frontotemporal lobar degeneration. Front Psychol. 2013 Jun 21;4:347. doi: 10.3389/fpsyg.2013.00347. eCollection 2013.
Fornazzari LR. Preserved painting creativity in an artist with Alzheimer’s disease. Eur J Neurol. 2005 Jun;12(6):419-24.
Gjengedal E, Lykkeslet E, Sørbø JI, Sæther WH. ‘Brightness in dark places': theatre as an arena for communicating life with dementia. Dementia (London). 2014 Sep;13(5):598-612. doi: 10.1177/1471301213480157. Epub 2013 Mar 13.
Gold K. But does it do any good? Measuring the impact of music therapy on people with advanced dementia: (Innovative practice). Dementia (London). 2014 Mar 1;13(2):258-64. doi: 10.1177/1471301213494512. Epub 2013 Jul 26.
Gordon N. Unexpected development of artistic talents. Postgrad Med J. 2005 Dec;81(962):753-5.
Gross SM, Danilova D, Vandehey MA, Diekhoff GM. Creativity and dementia: Does artistic activity affect well-being beyond the art class? Dementia (London). 2013 May 22. [Epub ahead of print]
Guétin S, Portet F, Picot MC, Pommié C, Messaoudi M, Djabelkir L, Olsen AL, Cano MM, Lecourt E, Touchon J. Effect of music therapy on anxiety and depression in patients with Alzheimer’s type dementia: randomised, controlled study. Dement Geriatr Cogn Disord. 2009;28(1):36-46. doi: 10.1159/000229024. Epub 2009 Jul 23.
Hafford-Letchfield T. Funny things happen at the Grange: introducing comedy activities in day services to older people with dementia–innovative practice. Dementia (London). 2013 Nov;12(6):840-52. doi: 10.1177/1471301212454357. Epub 2012 Jul 9.
Holland AC, Kensinger EA. Emotion and autobiographical memory. Phys Life Rev. 2010 Mar;7(1):88-131. doi: 10.1016/j.plrev.2010.01.006. Epub 2010 Jan 11. Review.
Hsieh S, Hornberger M, Piguet O, Hodges JR. Neural basis of music knowledge: evidence from the dementias. Brain. 2011 Sep;134(Pt 9):2523-34. doi: 10.1093/brain/awr190. Epub 2011 Aug 21.
James IA, Mackenzie L, Mukaetova-Ladinska E. Doll use in care homes for people with dementia. Int J Geriatr Psychiatry. 2006 Nov;21(11):1093-8.
Janata P. The neural architecture of music-evoked autobiographical memories. Cereb Cortex. 2009 Nov;19(11):2579-94. doi: 10.1093/cercor/bhp008. Epub 2009 Feb 24.
LaBar KS, Cabeza R. Cognitive neuroscience of emotional memory. Nat Rev Neurosci. 2006 Jan;7(1):54-64. Review.
Lazar A, Thompson H, Demiris G. A systematic review of the use of technology for reminiscence therapy. Health Educ Behav. 2014 Oct;41(1 Suppl):51S-61S. doi: 10.1177/1090198114537067.
Mezirow J. (2000) Learning to think like an adult. In J. Mezirow and Associates, Learning as transformation: Critical perspectives on a theory in process. (pp. 3-33). San Francisco: Jossey Bass.
Miller BL, Boone K, Cummings JL, Read SL, Mishkin F. Functional correlates of musical and visual ability in frontotemporal dementia. Br J Psychiatry. 2000 May;176:458-63.
Miller BL, Cummings J, Mishkin F, Boone K, Prince F, Ponton M, Cotman C. Emergence of artistic talent in frontotemporal dementia. Neurology. 1998 Oct;51(4):978-82.
Miller, B.L., Yener, G, Akdal, G. (2005) Artistic patterns in dementia, Journal of Neurological Sciences (Turkish), vol. 22(3), pp. 245-249.
Mitchell G, McCormack B, McCance T. Therapeutic use of dolls for people living with dementia: A critical review of the literature. Dementia August 25, 2014 1471301214548522.
Mitchell G, McCormack B, McCance T. Therapeutic use of dolls for people living with dementia: A critical review of the literature. Dementia (London). 2014 Aug 25. pii: 1471301214548522. [Epub ahead of print]
Mitchell G, Templeton M. Ethical considerations of doll therapy for people with dementia. Nurs Ethics. 2014 Sep;21(6):720-30. doi: 10.1177/0969733013518447. Epub 2014 Feb 3.
Omar R, Hailstone JC, Warren JE, Crutch SJ, Warren JD. The cognitive organization of music knowledge: a clinical analysis. Brain. 2010 Apr;133(Pt 4):1200-13. doi: 10.1093/brain/awp345. Epub 2010 Feb 8.
Pezzati R, Molteni V, Bani M, Settanta C, Di Maggio MG, Villa I, Poletti B, Ardito RB. Can Doll therapy preserve or promote attachment in people with cognitive, behavioral, and emotional problems? A pilot study in institutionalized patients with dementia. Front Psychol. 2014 Apr 21;5:342. doi: 10.3389/fpsyg.2014.00342. eCollection 2014.
Ramachandran, VS, Hirstein, (1999) The science of art: a neurological theory of aesthetic experience. Journal of Consciousness Studies (6), no.6-7, pp.15-51.
Rankin KP, Liu AA, Howard S, Slama H, Hou CE, Shuster K, Miller BL. A case-controlled study of altered visual art production in Alzheimer’s and FTLD. Cogn Behav Neurol. 2007 Mar;20(1):48 61.
Roe B, McCormick S, Lucas T, Gallagher W, Winn A, Elkin S. Coffee, Cake & Culture: Evaluation of an art for health programme for older people in the community. Dementia (London). 2014 Mar 31. [Epub ahead of print]
Salimpoor VN, Benovoy M, Longo G, Cooperstock JR, Zatorre RJ. The rewarding aspects of music listening are related to degree of emotional arousal. PLoS One. 2009 Oct 16;4(10):e7487. doi: 10.1371/journal.pone.0007487.
Seeley WW, Matthews BR, Crawford RK, Gorno-Tempini ML, Foti D, Mackenzie IR, Miller BL. Unravelling Boléro: progressive aphasia, transmodal creativity and the right posterior neocortex. Brain. 2008 Jan;131(Pt 1):39-49. Epub 2007 Dec 5.
Stevens, J 2012, ‘Stand up for dementia: performance, improvisation and stand up comedy as therapy for people with dementia; a qualitative study’, Dementia, vol. 11, no. 1, pp. 61-73.
Takahata K, Saito F, Muramatsu T, Yamada M, Shirahase J, Tabuchi H, Suhara T, Mimura M, Kato M. Emergence of realism: Enhanced visual artistry and high accuracy of visual numerosity representation after left prefrontal damage. Neuropsychologia. 2014 May;57:38-49. doi: 10.1016/j.neuropsychologia.2014.02.022. Epub 2014 Mar 11.
Takeda M, Hashimoto R, Kudo T, Okochi M, Tagami S, Morihara T, Sadick G, Tanaka T. Laughter and humor as complementary and alternative medicines for dementia patients. BMC Complement Altern Med. 2010 Jun 18;10:28. doi: 10.1186/1472-6882-10-28.
Tanaka, Y, Nogawa, H, Tanaka, H. (2012) Music Therapy with Ethnic Music for Dementia Patients, International Journal of Gerontology Volume 6, Issue 4, December 2012, Pages 247 257.
Topo, P, Mäki,O, Saarikalle, K, Clarke, N, Begley, E, Cahill, S, Arenlind, J, Holthe, T, Morbey, H, Hayes, K, Gilliard, J. Dementia October 2004 Assessment of a Music-Based Multimedia Program for People with Dementia vol. 3 no. 3 331-350
Woods RT, Bruce E, Edwards RT, Elvish R, Hoare Z, Hounsome B, Keady J, Moniz-Cook ED, Orgeta V, Orrell M, Rees J, Russell IT. REMCARE: reminiscence groups for people with dementia and their family caregivers – effectiveness and cost-effectiveness pragmatic multicenter randomised trial. Health Technol Assess. 2012;16(48):v-xv, 1-116. doi: 10.3310/hta16480.
Zeilig H. Gaps and spaces: representations of dementia in contemporary British poetry. Dementia (London). 2014 Mar 1;13(2):160-75. doi: 10.1177/1471301212456276. Epub 2012 Aug 17.

A powerful group led by persons with dementia may be just the disruptive innovation the world needs
This, rather than “The Golden Arches”, is fast becoming a symbol of hope.
The motor vehicle was supposed to be a major disruption for the horse and cart. Paper superseded parchment. The DVD long surpassed the audio cassette.
Progress and innovation, whatever your political philosophy, some might say is pretty inevitable.
In terms of technology, people have recently opined about three ‘industrial revolutions’, and “the shock of the new”.
Innovations can not just be about products. They can be about fundamentally a whole new way of doing things.
The traditional large charity for dementia model has its advantages. It, through economies of scale and large operational efficiencies, can implement large projects, liaise with governments, and have a lot of media backing in the implementation of their projects.
The down-side to this is that it can too easily suffocate innovation from small social enterprises. It can also pursue agendas which are biased in one particular direction.
One example is witnessed in the the appointment of the World Dementia Council.
This Council, quite strangely, does not include any representatives of persons with dementia or representatives of carers. If its primary purpose is to develop new innovations or drugs, they will need to know the efficacy of user adoption at some stage even from a management or industrial basis.
As it is, large charities, in promising to deliver new orphan drugs for dementia one day, can totally ignore the need for high quality research into living well with dementia. They can treat their associated persons with dementia as ‘subjects’ for future drug trials.
This is incredibly problematic and obstructive for those people with dementia – and their supporters including researchers – who wish to pursue an agenda of quality of life in dementia for current people living with dementia.
Even in the press bulletin for the first meeting of the World Dementia Council, dementia is referred to as a ‘timebomb’.

This is incredibly troublesome for some purists who note that the prevalence of dementia across two decades in England may in fact be falling, due to primary care managing successfully the vascular dementias.
So in this specific scenario – a timebomb it is not.
Of course, the ‘holy grail’ for drug companies, and large charities supporting them, is that there exists a ‘pre-dementia’ stage, of people without symptoms, who could be amenable for drug treatment later one day, or advice about lifestyle and risk factors.
Currently, the evidence for the feasibility of this approach is very poor, however.
But something quite amazing, and indeed “disruptive”, happened quite recently. To say it could be explosive for international policy is in fact an understatement.
The 29th International Conference of Alzheimer’s Disease International, entitled “Dementia: Working Together for a Global Solution” held on 1-4 May 2014 at San Juan, Puerto Rico, was beyond reasonable doubt a storming success.
The ADI welcomed Glenn Rees, current CEO of Alzheimer’s Australia, as its Chair-Elect. This is a highly significant appointment, and one which people who promote the living well with dementia philosophy extremely warmly welcome.
So what?
A plucky group of people with dementia emerged, gave talks, and presented cutting-edge research. It was no longer a case of ‘listening to people with dementia’, but rooms packed full of people mesmerised by original contributions from a totally different perspective.
One academic in stigma was overheard to say to a person with dementia: “You don’t look like a person with dementia.”
That person commented that the academic didn’t, either.
Dementia Alliance International is a non-profit group of people with dementia from the USA, Canada, Australia and other countries that seek to represent, support, and educate others living with the disease, and an organisaton that will provide a unified voice of strength, advocacy and support in the fight for individual autonomy and improved quality of life.
Membership in Dementia Alliance International is free and open to people with dementia only, in any country.
Membership is open to any person with dementia who would like to be part of a global community of others with dementia where members support and encourage each other to live well with dementia, or oin others in fighting against the stigma, isolation and discrimination of dementia.
In addition to the larger countries, there has been interest from Taipei, New Zealand, St Maartens, Spain, Puerto Rico, and Japan, to name but a few. Of course, such an initiative is immediately attractive to a lot of other people who have the cash, including world philanthropists who have some personal connection with dementia.
This group has even been ‘noticed’ by the larger corporates and corporate-like entities in dementia, but people close to this group report that they are desperate to keep their autonomy and identity, despite possible (legal) enticements.
They know that they are on the threshold of massively disrupting current policy. They know they won’t be one or two bums occupying seats on research panels of large charities any more, only.
They will be there now leading the pack.
1. ADI staff get recognition for their work.

2. Final panel on Sunday includes person with dementia from USA, Scott Russell.

3. Final Panel with Scott Russell.

4. Person with dementia from Puerto Rico, Julio, speaks out as keynote. He got the only standing ovation of the morning’s speakers.

5. The DAI team

6. Kate Swaffer, from DAI, before her presentation of her model, “Prescribed disengagement”


A person newly diagnosed with dementia has a question for primary care, and primary care should know the answer

Picture this.
It’s a busy GP morning surgery in London.
A patient in his 50s, newly diagnosed with Alzheimer’s disease, a condition which causes a progressive decline in structure and function of the brain, has a simple question off his GP.
“Now that I know that I have Alzheimer’s disease, how best can I look after my condition?”
A change in emphasis of the NHS towards proactive care is now long overdue.
At this point, the patient, in a busy office job in Clapham, has some worsening problems with his short term memory, but has no other outward features of his disease.
His social interactions are otherwise normal.
A GP thus far might have been tempted to reach for her prescription pad.
A small slug of donepezil – to be prescribed by someone – after all might produce some benefit in memory and attention in the short term, but the GP warns her patient that the drug will not ultimately slow down progression consistent with NICE guidelines.
It’s clear to me that primary care must have a decent answer to this common question.
Living well is a philosophy of life. It is not achieved through the magic bullet of a pill.
This means that that the GP’s patient, while the dementia may not have advanced much in the years to come, can know what adaptations or assistive technologies might be available.
A GP will have to be confident in her knowledge of the dementias. This is an operational issue for NHS England to sort out.
He might become aware of how his own house can best be designed. Disorientation, due to problems in spatial memory and/or attention, can be a prominent feature of early Alzheimer’s disease. So there are positive things a person with dementia might be able to do, say regarding signage, in his own home.
This might be further reflected in the environment of any hospital setting which the patient may later encounter.
Training for the current GP is likely to differ somewhat from the training of the GP in future.
I think the compulsory stints in hospital will have to go to make way for training that reflects a GP being able to identify the needs of the person newly diagnosed with dementia in the community.
People will need to receive a more holistic level of support, with all their physical, mental and social needs taken into account, rather than being treated separately for each condition.
Therefore the patient becomes a person – not a collection of medical problem lists to be treated with different drugs.
Instead of people being pushed from pillar to post within the system, repeating information and investigations countless times, services will need to be much better organised around the beliefs, concerns, expectations or needs of the person.
There are operational ways of doing this. A great way to do this would be to appoint a named professional to coordinate their care and same day telephone consultations if needed. Political parties may differ on how they might deliver this, but the idea – and it is a very powerful one – is substantially the same.
One can easily appreciate that people want to set goals for their care and to be supported to understand the care proposed for them.
But think about that GP’s patient newly diagnosed with dementia.
It turns out he wants to focus on keeping well and maintaining his own particular independence and dignity.
He wants to stay close to his families and friends.
He wants to play an active part in his community.
Even if a person is diagnosed with exactly the same condition or disability as someone else, what that means for those two people can be very different.
Once you’ve met one person with dementia, you’ve done exactly that: you happen to have met one person with dementia.
Care and support plans should truly reflect the full range of individuals’ needs and goals, bringing together the knowledge and expertise of both the professional and the person. It’s going to be, further, important to be aware of those individuals’ relationships with the rest of the community and society. People are always stronger together.
And technology should’t be necessarily feared.
Hopefully a future NHS which is comprehensive, universal and free at the point of need will be able to cope, especially as technology gets more sophisticated, and cheaper.
Improvements in information and technology could support people to take control their own care, providing people with easier access to their own medical information, online booking of appointments and ordering repeat prescriptions.
That GP could herself be supported to enable this, working with other services including district nurses and other community nurses.
And note that this person with dementia is not particularly old.
The ability of the GP to be able to answer that question on how best her patient can lead his life cannot be a reflection of the so-called ‘burden’ of older people on society.
Times are definitely changing.
Primary care is undergoing a silent transformation allowing people to live well with dementia.
And note one thing.
I never told you once which party the patient voted for, and who is currently in Government at the time of this scenario.
Bring it on, I say.

A need for much more effective regulation for dementia charities
All governments in the UK have recently thought about ‘reforming public services’, mostly in the context of public-private partnerships (PPP) or the private finance initiative (PFI). Third sector organisations, such as social enterprises and charities, especially large ones, are acting in increasingly private or even corporate ways.
Many feel that this has now become a dangerous policy issue in dementia in England.
There is much goodwill towards dementia as a cause, not least because there are 800,000 people living with dementia currently in the UK. On account of this, there should be a moral onus for fundraisers and politicians to act in the general interests of all people with dementia, and carers.
Take for example the report of the “Dementia Friends” initiative.
It is reported as, by 2015, 1 million people becoming Dementia Friends. The £2.4 million programme is funded by the Social Fund and the Department of Health. The scheme has been launched in England and the Alzheimer’s Society is hoping to extend it to the rest of the UK soon.
A newspaper article on dementia will now have a standard format. There’ll be the story itself, a bit about dementia, and invariably a bit about Dementia Friends. But the situation is very serious indeed. It wouldn’t be tolerated if all the discussions of groceries in newspapers or online media only made references to Sainsbury’s.
This is clearly problematic for other charities such as the Joseph Rowntree Foundation, who have their own longstanding friendship initiatives, but who have never publicly complained about this situation.
When the State goes into partnership with third sector organisations, the need for much more effective regulation in public-private partnerships is imperative.
This is what the OECD had to say about the issue in their document “Recommendation of the Council on Principles for Public Governance of Public-Private Partnerships May 2012″:
“Sound regulatory policy promotes the efficient functioning of regulatory agencies by ensuring that they operate under an appropriate and clear mandate, with the necessary independence from political influence and regulated subjects, that they are appropriately resourced and equipped, and that their decision-making is fully transparent and accountable,”
“Where PPPs are employed in the delivery of infrastructure facilities with natural monopoly characteristics, the role, design and organisation of regulators is important to secure value for money for the public sector and protect users and consumers. This role should be clear to all (staff, regulated entities and the community).”
“The appropriate sector regulator should consequently be consulted in the project design and subsequently monitor compliance with regulated service standards. This role is important not only in shaping the markets, but also with concrete issues such as service quality, profitability, tariffs and prices. Of particular interest in monopoly-like situations is the degree of profitability compared to the sector average using various benchmarks.”
There are good business management reasons why such entities are able to exert monopoly-like effects. Large organisations benefit from ‘economies of scales’, meaning that it is cheaper to do things in bulk. And large organisations can afford, say, to attend conferences, pay for posters, stand space, marketing pamphlets, etc.
It is simply impossible for smaller organisations to compete with this. For example, large charities are able to instruct commercial/corporate law firms to protect their logos and trademarks on intellectual property registers; and are able to exert competitive advantage that way.
And this was from Public Health England last year:
“The aim is to create a fully-integrated marketing programme which will help transform how the public thinks and feels about dementia, increase social connectedness and upskill society, so that people understand how they can help. It will encourage people to join the Dementia Friends programme, launched by Alzheimer’s Society, and invite businesses and communities to become dementia-friendly organisations.”
There’s been a whole plethora of cutbacks, which have thus far gone relatively unnoticed under the RADAR of the mainstream media. For example, it is reported that Essex County Council has just finalised plans to axe £200,000 funding for Mundy House, the only dementia day care centre in South Essex.
A number of people have told me in private that they cannot compete with the Alzheimer’s Society, but are increasingly having to find strategic partnerships with them otherwise they really would have no hope of competing in commissioning, even if they feel that their values and project are distinct.
The suboptimal nature of this sometimes bursts onto Twitter, where it can be difficult to have a highly managed media message. Tommy Whitelaw, well respected campaigner for carers’ voices, wished the Alzheimer’s Society to share his video, and these were some of the responses when the video wasn’t shared.
what on earth?Why won’t you RT a heartfelt film about carers/dementia, @alzheimerssoc ? Dementia doesn’t consider borders!  @tommyNtour
@tommyNtour
— #hellomynameisRachel (@StMHNurseRahs) March 31, 2014
@tommyNtour @alzheimerssoc : Are you saying that the issues highlighted in the film don’t apply to carers in England?
— joyce cavaye (@joycecavaye) March 31, 2014
For all of twelve hours I had forgotten about this major problem, until this reminded me:
“don’t bite the hand that feeds you” mantra keeping big dementia charities in the pocket of government? Not as influential as we think?
— Darren Gormley (@MrDarrenGormley) April 1, 2014
And a friend of mine on Facebook, who had been a longstanding supporter of the Alzheimer’s Society, and who himself/herself lives with dementia, complained last night that (s)he was very dillusioned about his/her views weren’t being listed to, amongst a plethora of other grievances about the current direction.
(S)he had just in fact read my survey about who were the winners and losers of the G8 Dementia survey according to about 90 of my followers on Twitter.
I think this situation is intolerable. I intend to write to the Alzheimer’s Disease International about my concerns, because we need a diversity and plurality in fundraising for all the dementias. I know that I already have the support of many who are equally concerned. All we need, I feel, is an open and transparent debate about what or who is calling the shots in English dementia policy.
And finally, this tweet has summed up my concerns. Thanks Bernadette.
@legalaware This was always the danger of ‘Big Society’ or PPP concept: some charities losing independence, some becoming the ‘chosen ones’.
— Bernadette Meaden (@BernaMeaden) April 1, 2014

My name is Shibley, and I’m addicted to buying my own book ‘Living well with dementia’
I’ve sat in more recovery sessions than you’ve had hot dinners….
.. possibly.
So I get a surge of dopamine whenever I receive yet more copies of my book from Amazon.
Worth every penny.

I am Shibley. and I’m addicted to buying my own book.

But I also have a weird habit of getting people I know to sign my copy of my book.
I get withdrawal symptoms from not having enough copies.
I also get tolerance – I need to have an increasing number of copies to get the same “kick” from my book.
Thanks enormously to the following ‘well wishers’, though, who have signed my book.
A huge thanks to Gill (@WhoseShoes) for her unflappable support of me and my book.
Here’s Gill’s blogpost.
And here we are!

I felt very happy to give a copy of my book to Prof Sube Banerjee, newly appointed Chair of Dementia at Brighton and Sussex Medical School. Sube has in fact been the lead for England for dementia – his work is quoted in my book, and I think he’s made an enormous contribution to the living well with dementia literature.

And what does the future hold for ‘living well with dementia’?
Other ‘signatories’ include:

I’ve known Lisa for yonks on Twitter. Lisa is one of the few people who’ve supported me through the bad times too.



But now you can ‘Look Inside’ to get a flavour of my book – as there is now a Kindle edition (thanks to Alice in my book publishers @RadcliffeHealth)
Here it is on Amazon.

Here is a sample chapter from my book ‘What is living well?’
‘Living well’ is not some bogus mantra for the hell of it. It is an ideological standpoint which serves to promote the dignity of our fellow citizens who happen to also have a clinical diagnosis of dementia.
And here are the “beautiful people” who came to my book launch at the Arlington Centre, Camden, one afternoon in February. I can’t believe that this wasn’t even a month ago now!

One of the happiest days, as well, was giving Joseph a copy of my book as a gift.

Joseph was in fact my carer when I could hardly walk or talk, when I was in physical recovery from meningitis on ITU (where I was unconscious in 2007).
And those were the days…

And THIS is the famous poppy.
This picture was taken by Twitter pal, @charbhardy, first amongst equals in the #dementiachallengers.

After I said I was buying my own copies, @KateSwaffer asked:

But Kate has read a copy of my book from cover to cover:
And as @Norrms says – how can ‘living well with dementia’ fail?

The David and Goliath problems of the English Dementia Charities
To be clear, I think the work of the Alzheimer’s Society is fantastic.
Since their restructuring, with the support of the Department of Health, they have done really important work in activities to do with dementia, not just Alzheimer’s disease.
Goliath (Hebrew: ????????,) is a a giant Philistine warrior defeated by the young David, the future king of Israel, in the Bible’s Books of Samuel (1 Samuel 17).
Britain’s energy market is said to be dominated by the Big Six gas and electricity suppliers. All markets need competition to function effectively, with genuine choice for consumers.
Mentions of the Alzheimer’s Society are extensive.
This is for example Hazel Blears on 16 December 2013:

And here is the recruitment drive of Jeremy Hunt, four minutes in into his speech at the G8 Summit in December 2013:
It really has become a gigantuan operation for smaller charities to compete also in the social media:

Last week, it was announced that staff at Marks & Spencer, Argos, Homebase, Lloyds Bank and Lloyds Pharmacy will attend special sessions to help them understand the needs of customers with dementia and support them better.
The Alzheimer’s Society makes clear that the drive towards ‘Dementia Friends’ forms part of the six-month progress report on the Prime Minister’s Challenge on Dementia.
And it has been a success we can all be proud of. Norman McNamara is also soldiering on with his “Dementia Friendly” Torbay initiatives.
As a result of commitments from various businesses regarding “Dementia Friends”, over 190,000 staff will become Dementia Friends – 60,000 from M&S, 70,000 from Lloyds Pharmacy, 50,000 from the Home Retail Group, which owns Argos and Homebase, and 11,500 from Lloyds Bank.
And yet ‘dementia friendship’ is a global initiative.
Supportive communities are well known in Japan. For example, Fureai kippu (in Japanese ?????? :Caring Relationship Tickets) is a Japanese currency created in 1995 by the Sawayaka Welfare Foundation so that people could earn credits helping seniors in their community.
An initiative from another charity, the Joseph Rowntreee Foundation, “York Dementia Without Walls” project looked into what’s needed to make York a good place to live for people with dementia and their carers.
They found that dementia-friendly communities can better support people in the early stages of their illness, maintaining confidence and boosting their ability to manage everyday life.
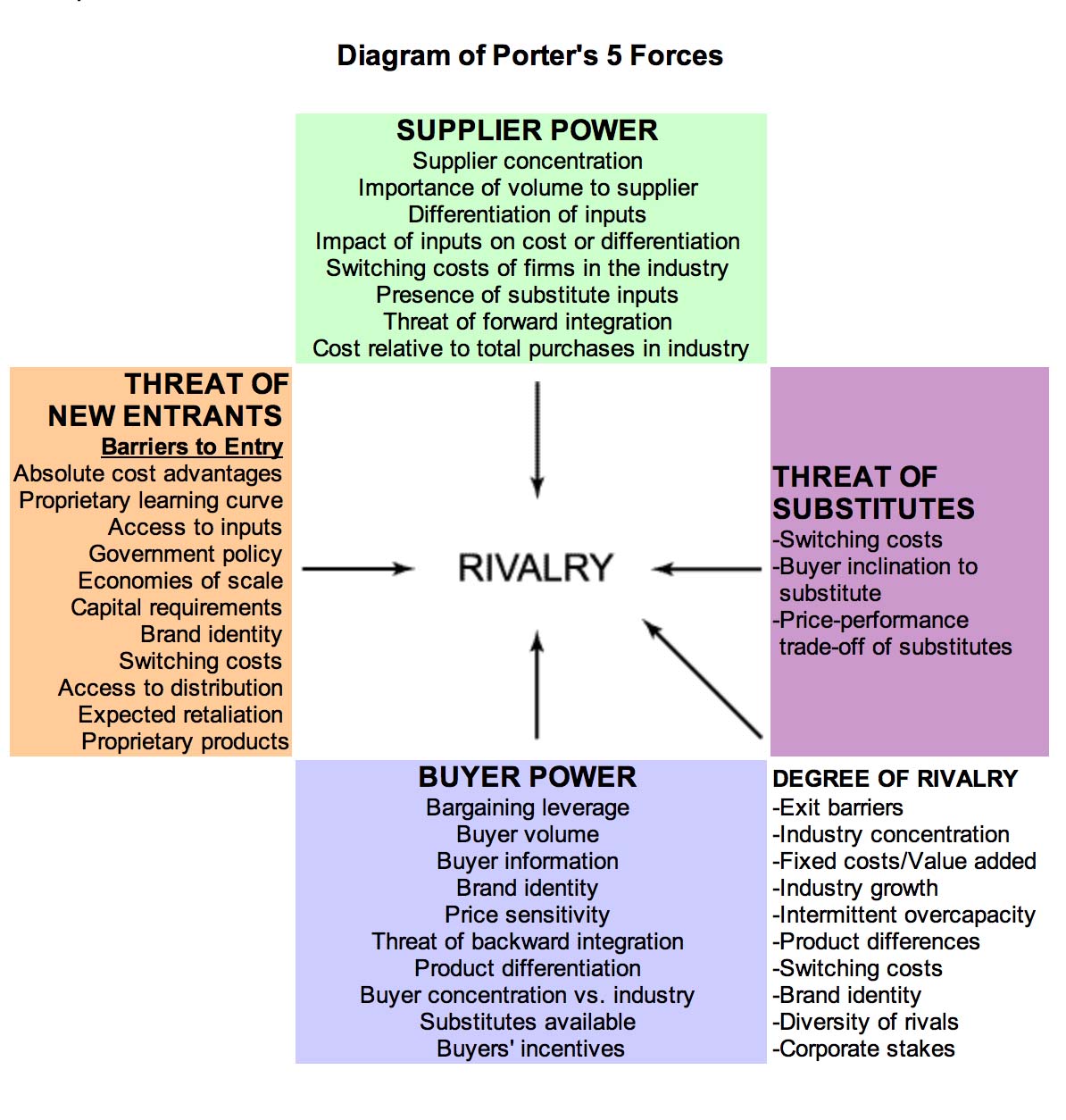
There are various reasons why it is so easy for the Alzheimer’s Society to ‘clean up’ in the dementia charity market in England.
These are helpfully summarised in this summary slide, derived from the work of Michael Porter, Bishop William Lawrence University Professor of Business Management at the Harvard Business School, USA.
The Alzheimer’s Society have protected their visual mark for “Dementia Friends” on the trademark register for the IPO, as trademark UK00002640312. It is protected under various categories. This is across various classes, including ‘gymnastic and sporting articles’.

It would have cost a lot for the Alzheimer’s Society plus the cost of instructing their lawyers, which are cited here as the big commercial/corporate law firm DLA Piper in Leeds. It’s simply impossible for smaller charities to compete resource-wise over this arm of intellectual property.
Currently, according to the UK trademark office, it costs £170 to apply to register a UK trade Mark if you apply on-line (£30 discount applies for on-line filings). This includes one class of goods or services. It is a further £50 for every other class you apply for.
And the pattern of news stories about dementia has now reached a consistent homogeneous pattern. For example, this story about Prunella Scales being diagnosed with dementia has a standard line with the word ‘suffering’ (“Fawlty Towers star Prunella Scales is suffering from dementia – but is determined not to let it stop her performing, her actor husband Timothy West has revealed.”)
But the language is not one of ‘living well with dementia’, consistent with other metaphors such as ‘timebomb’, ‘explosion’, ‘flood’ and ‘tide’.
And crucially it is very rare to have any other dementia charity named apart from the Alzheimer’s Society because of their strong brand presence inter alia.
There are other dementia charities in England, however.
BRACE is a registered charity that funds research into Alzheimer’s disease and other forms of dementia. Their role is to help medical science understand the causes of dementia, find ways of diagnosing it earlier and more accurately, and develop more effective treatments.
Dementia UK is a national charity, committed to improving quality of life for all people affected by dementia. They provide mental health nurses specialising in dementia care, called Admiral Nurses. And yet there have been cuts to the Admiral Nurses service.
On December 13th 2013, the Dementia Advocacy Network reported that they would be closing after 12 years of supporting independent advocates (this is the current link to their website.)
An article in the European Journal of Marketing (Vol. 29 No. 10, 1995, pp. 6-26), entitled “The market positioning of British medical charities” by Sally Ann Hibbert from Department of Marketing, University of Stirling, Stirling, Scotland, does throw some light on this issue.
Hibbert notes that clusters of people who donate to charities exist overall.
“Following on, the next highest scores are revealed for cancer and deaf charities, the former investing notably in education and research for cures, the latter focusing largely on treating the effects of deafness to improve the quality of life for people affected. This trend from preventive approaches to care services can be traced down through the charities on the vertical dimension to hospices, which are primarily carers.”
In the absence of a reliable marker through scans or psychology before symptoms, and in the absence of good treatments of dementia which stop the condition “in its tracks“, it was hard to make the pitch for molecular biology research and treatments. The industry was described as “ailing“.
That’s why it was so crucial to compare dementia to AIDS (see video above).
There is a legitimate concern that driving policy towards limited angles in this way could obscure the need for funding a grossly under-resourced community care services for dementia.
And living well with dementia is an appropriate policy plan for persons currently with dementia and their caregivers.
But specialist groups of people with dementia are beginning to emerge. For example, the “Dementia Action Alliance” is a non-profit dedicated to improving the quality of life for people living with the effects of dementia.
The DAA Carers Action (@DAACarers) also do incredible work .
Like the Government has been to provide an “equal playing field” for any qualified provider of NHS services, it is impossible to think that the playing field for raising money for dementia through charities and people such as the Purple Angels is anything like an “equal playing field”.
This is a major flaw in current policy, and could mean that there are some losers and some winners. This ‘zero sum gain’, simply, is not on I feel.
It is deeply concerning that “might is right”. We should try to work together.

Blurred lines in English dementia policy – privatisation in all but name
In case you don’t like the soundtrack, here are the slides.
To some extent, Europe resolved our dispute about whether we should aspire to an ‘early diagnosis’, or ‘timely diagnosis’ for dementia. The overall consensus from the European ALCOVE project was that a diagnosis should be timely, in keeping with the needs of the person with a dementia, his friends, his family or his carers.
This was an extremely helpful move in English policy, although the road had not been that clear.
One blurred line in the public was how dementia so massively became conflated with all memory problems in the elderly. Whilst it was argued that the memory problems in Alzheimer’s disease should no longer be passed off as ageing (and indeed there are strong cultural pressures elsewhere for calling dementia ageing), there was some concern from GPs that older people thought their memory problems were dementia because of the widespread media campaign. Many of these individuals were later to arrive at a diagnosis of minor cognitive impairment, underactive thyroid, or depression. Given that there are hundreds of different causes of dementia which can affect any part of the brain and brainstem (though they all tend to start off in different areas), it’s not altogether surprising that some of the dementias don’t present with memory problems at all.
The drive to make the diagnosis is almost certainly going to be affected by the policy from NHS England to achieve ‘ambitions’ for increasing dementia diagnosis rates. The evidence from the MRC study at Cambridge has demonstrated that this prevalence has in fact been falling over some decades, so there is serious concern that a drive to increase dementia rates will lead to a large number of false diagnoses in 2014. This is definitely one to watch, as a false diagnosis can lead to very serious harmful repercussions. Nonetheless, the number of people who have a MMSE in the region of 10-15 on initial diagnosis is, arguably, staggering, and blatant lack of diagnoses of more obvious presentations of diagnosis most people would agree is unacceptable.
The spotlight in G8, and certainly the presence of corporates there, will lead to increased scrutiny of those people who financially have much to gain from an early diagnosis. An early diagnosis may indeed lead to someone ‘accessing care’, even that care results from a personal health budget with treatments which are not proven clinically from the evidence. The direction of this particular plan depends how far individualised consumer choice is pushed in the name of personalisation. Genetics, neuropsychologists, and pharmaceutical private sector companies wishing to monitor the modest effects of their drugs on substances in the brain all stand to capitalise on dementia in 2014, much of which out of the NHS tax-funded budget. This of course is privatisation of the NHS dementia policy in all but name. One thing this Government has learnt though is how to make a privatisation of health policy appear popular.
Despite corners being cut, and the drive to do ‘more for less’, it will be quite impossible to avoid making a correct diagnosis in individuals thought to have a dementia in the right hands. A full work-up, though the dementia of the Alzheimer type, is the most common necessitates a history of the individual, a history from a friend, an examination (e.g. twitching could be associated with the motor neurone disease variant found in one of the frontotemporal dementias), brain scan (CT/MRI/PET), brain waves (EEG), brain fluid (cerebrospinal fluid), bedside psychology, formal cognitive psychological assessment, and even in some rarely a brain biopsy (for example for variant Creutzfeld-Jacob or a cerebral inflammatory vasculitis).
Analysis by paralysis is clearly not desirable either, but the sticking point, and a blurred line, is how England wishes to combine increasing diagnostic rates; and making resources available for post-diagnosis support; making resources available for the diagnosis process itself including counselling if advised. As the name itself ‘dementia’ changes to ‘neurocognitive impairment’ under the diagnostic manual DSM in 2015, the number of people ‘with the label’ is likely to increase, and this will be ‘good news’ for people who can capitalise on dementia. The label itself ‘neurocognitive impairment’ itself introduces a level of blur to the diagnosis of dementia itself.
The general direction of travel has been an acceleration of privatisation of dementia efforts, but this to be fair is entirely in keeping with the general direction of the Health and Social Care Act (2012). A major question for 2014 is whether this horse has now truly bolted?
