Home » Posts tagged 'NHS'
Tag Archives: NHS

Does Jeremy Hunt wish to ‘save the NHS’? Most definitely not.
There is nothing more embarrassing than for hardworking clinicians in the NHS and practitioners in social care than to hear of Jeremy Hunt going to New York to lay the groundwork for a transatlantic trade deal or to go to international conferences to preach to others on patient safety. Whether the longest serving Secretary of State for Health chooses to admit or not, and he doesn’t, there is nothing to boast about in 20 hour trolley waits, or people being asked to sit in a toilet or corridor before being given a hospital bed. If the definition of patient safety is that nobody has died unnecessarily yet, then expectations are indeed very low. Indeed, Sir Robert Francis, whom Hunt used to quote all the time, now says another Mid Staffs is “inevitable”.
To be honest, this is the perfect storm which prominent campaigners, including junior doctors, themselves have been warning about. It might seem beyond ludicrous that Jeremy Hunt can shamelessly say that the performance of the NHS is ‘unacceptable’, but as far as he is concerned he is not responsible for the performance of the NHS. And the purpose of the 2012 Health and Social Care Act (2012) was not to promote the highest quality clinical care – symptomatic of that is the fact in the 500 pages of legislation the legislation found time to devote only one clause to patient safety, and that was to abolish the National Patient Safety Agency. The legislation instead was put in place to turbo-boost the transfer of NHS services to the private sector. This is – wait for it – the definition of ‘privatisation’. It also provided legislation for clinical commissioning groups, where is no statutory mandate for clinical skill. These clinical commissioning groups, which are even definite in size of population in law, are merely insurance entities which happen to reside in the public sector, assessing the potential risk of illness in a certain geography. In other words, this highly contentious Act of parliament, on which billions of £ were ultimately spent in a top-down reorganisation that nobody as such voted for, laid down the infrastructure for harmonisation between the public sector and the private sector for the ultimate piecemeal sell off of the NHS.
The ultimate issue that successive governments have had to face for the last three or four decades has been a desire not to go ‘public’ about transferring the NHS to the private sector, so that the NHS simply becomes a badge for the state deliverer of services, not the state provider. In an ideal world, Jeremy Hunt MP does not even want to be involved with anything to do with the NHS. Hunt, and many others of the same ideological ilk, would be perfectly happy for different providers, e.g. Capita, Virgin, G4S, in some corporate plutocracy to run the NHS using the NHS logo if need be.
Jeremy Hunt’s faux disdain at the performance of the NHS is completely understandable, if one realises that Hunt thinks the public will blame the fact the NHS is in the public sector rather than him for the poor performance of the NHS. And, to be fair to him, there are people who ring up local radio phone shows to say that the problems of the NHS are entirely due to mismanagement, the fact that the general public take no responsibility for their own health (a completely irrelevant argument if someone is born with a congenital disease such as heart problem or lung problem). And, furthermore, more in the post-facts milieu, the hope is that nobody can discern fact from fiction. In other words, with the help of a compliant media, the general public can be manipulated into thinking that the root cause of the NHS being overloaded is entirely due to the immigrant population. There is no discussion of non-indigineous doctors or other healthcare professionals in this utopia, just ‘small talk’, albeit dangerous UKIP pillow talk, of an aspiration of Jeremy Hunt to reverse decades of the NHS being propped up by foreign clinicians to train ‘home grown’ doctors. Mainsteaming British Doctors for British patients has never been easier.
But back to the fundamental issue of why I believe Jeremy Hunt does not care about the performance of the NHS is that his thinking rests on three assumptions. And, whilst a sizeable number of people in parliament think the same way as him, the likelihood of a cross-party commission on the NHS will come to the conclusion that some form of privatisation of the NHS, whether in terms of co-payments, vouchers or full blown increase in capacity of private insurance providers, will occur, rubber-stamped by all the political parties (except for some this time). It might, for example, be seductive for irritable, cranky people to ‘charge drunk people for attending A&E’, but think about the actual practical implementation of this policy – by what measure would you define the tipping point from ‘quite tipsy’ to ‘quite drunk’? Is it, for example, either feasible or desirable that healthcare professionals, including GPs, to carry Visa card or passport readers in addition to their numerous other duties?
A number of assumptions can possibly be made about this current Government and recent ones too:
1. There is no distinction between private and public providers in the NHS.
2. The Government believes in a ‘small state’ and low taxation.
3. The NHS is expected to make efficiency savings in keeping with an austerity approach.
That there is no distinction between private and public providers in the NHS is why Jeremy Hunt resents being in a centre of a tsunami about junior doctors’ pay. In an ideal world, he would like there to be complete harmonisation between private and public sectors, so that doctors could come and go as they wish in terms of employment. This is entirely the drive for the 24/7 NHS, which is why Jeremy Hunt is do keen to promote any fake research news coming out of the BMJ to further his ideology. You do not need to be an expert in sophisticated mathematical modelling techniques to realise that if you were to stretch out the already woefully inadequate resources for a 5-day elective service into a 7-day one the consequences on patient safety would be diabolical. What, furthermore, is quite incredible is for the current Department of Health to be so oblivious to the fact there already exists a 7-day emergency service running at full throttle, hence their need to spend valuable resources in making further metrics to measure A&E performance by.
Where junior doctors can come and go as they please, like where consultants can come and go as they please, or where nurses come and go as they please, is a strategy which is the direct opposite to the public sector keeping its workforce loyal, wellbeing promoted and well educated, and being contained budget-wise in terms of salaries. We already know that the agency spend has become out of control, due to poor planning of the Department of Health over many years, and to the weird hybrid private-NHS market we currently have. And all this is to ignore completely that private providers take no responsibility for, financially or otherwise, for the education and training of the workforce the vast majority of which start in the NHS. This is entirely in keeping in why Hunt is so intensely relaxed about applications for nursing training going through the floor after his devastating nursing bursary initiative – Hunt does not ideologically believe the Government should be safeguarding against a minimum body of doctors, nurses or allied health professionals in the workforce. The problem now of course for him now is #Brexit unless it looks like he can poach staff from the Asian subcontinent; but word is spreading fast how bad the working conditions of the English NHS are.
2. Unfortunately, the Conservatives and Liberal Democrats were able to converge on the ideology behind the Health and Social Care Act 2012 and the mirage that economic competition would drive up clinical quality because of the robustnesss in their belief in the small State. This does not envision the State to be a supportive thing to promote the health and wellbeing of its citizens, including so that they can be healthy enough to be in ‘gainful employment’ and be ‘productive’. This instead pre-supposes that everybody wishes to pay very low taxes, somehow living in a world where public services are still magically working well. But this falsehood is very easy to put in place if the main political parties are able to blame a ‘common enemy’ for all of their problems, e.g. immigrants. Such politicians want to divorce the link between improved public services and paying for them, which is why the Conservatives invest so much effort into depicting the Labour Party as incompetent (whereas the national debt under the 7 years of Conservatives has ballooned way above the previous 13 years of Labour).
Unfortunately, a hypothecated tax for the NHS would necessitate a debate about hypothecated taxes for everything else such as national security or education, and is well known to be yet another ‘zombie policy’ which won’t go away. Finally, whilst the Government gives the impression that the debacle in social care, causing delayed transfers of care from hospitals to care packages in the community, is seen as a ‘local authority’ not national problem, say for example through the ‘precept’ or the Surrey referendum, the impression is reinforced that social care is out of control, and its catastrophic state impacting on the performance of the NHS is nothing which can be reversed essentially.
3. Stephen Dorrell MP already has said that the NHS efficiency savings, first proposed by the management consultants, McKinseys have never successfully been tried before – and indeed many blame this drive for efficiency and for ‘foundation trust’ status to be at the heart of how disasters at Mid Staffs and other Trusts happened. It is a plain fact that if budgets are under enormous strain in providing a skeleton workforce (e.g. one junior doctor to cover all the medical wards in one large teaching hospital AND cover the cardiac arrest bleep), and to pay massive unconscionable private finance initiative payments (a form of a Corporate Wonga), something will have to give. There might be a temptation for such cuts to be hidden by commissioners and managers in mental health, despite all the Twitter infograms and rhetoric about ‘parity of esteem’ – unless of course there happens to be a spike in uncontrollable demand for mental health beds or suicides. So far, all the main English political parties have been very loyal to ‘efficiency savings’ – but this is essentially ‘austerity’, and a political choice for the NHS not an economic one.
If the ultimate aim is to increase transfer of public assets to private entities (the definition of privatisation), keeping the NHS at a low unsafe level of funding reinforces the impression the NHS is ‘unsafe in public hands’. That is why rolling coverage by the BBC of ‘specials’ of a NHS and social care system at breaking point might lead people to blame the public funding of the NHS, not Jeremy Hunt. This is of course fully intended, so that the green light can be given for a blatant privatisation of the NHS.
The correct conclusion, of course, is that the NHS has been chronically underfunded for years, and no Government wishes to admit they want to privatise the NHS as it’s so politically toxic.

Many Labour MPs are on suspended sentence – and they know it

It’s impossible to escape the conclusion that the failed coup (and it wasn’t even that in the end) did quite a lot of damage to the perception of Labour. At a time when the UK was reaching an existential crisis, as to whether it should be a Union or part of it, Hilary Benn made himself into a political Archduke Ferdinand and precipitated world war within Labour. Benn Junior’s legacy was a real “* you” to the membership, given that it is ubiquitously accepted that the general public will always punish divided parties as a rule of Newtonian classical dynamics.
The post-truth era for Jeremy Corbyn had of course begun long before his second election as Labour’s elected leader. It’s no mean feat for Rafael Behr or James O’Brien to continue their boring whingeing about Corbyn all the time, but to give them credit they need to pay their mortgages. But other people need a Labour government. The meme ‘Britain needs a strong opposition’ laying the blame at Corbyn of course is completely laughable given the torrent of abuse at Corbyn from all of the mainstream media, whether it’s on the inclination of his bowing in official ceremonies, the lack of singing at the National Anthem, or the alleged refusal to kneel and kiss at the Privy Council inauguration ceremonies.
Corbyn does not have the Twitter following with the magnitude of Donald Trump. He would not wish to boast about ‘expanding his arsenal’ either (pardon the unintentional pun about the Holloway Road in Islington). Nor is he best friends with Vladimir Putin. Talking of which, all of the pseudo-commentators who were spitting bullets at Corbyn’s morality seem to have gone deadly quiet about Trump’s ‘locker room’ banter, did you notice?
For all the talk about strong leadership, Jeremy Corbyn is no Adolf Hitler, Donald Trump or Nigel Farage. It’s hard to disagree with his ten pledges, which include the ‘bread and butter’ for many of us on the left wing of politics. Take for example the pledge ‘full employment and an economy that works for all’. George Osborne’s legacy, possibly not meriting a CBE, was to produce one giant ‘gig economy’, with workers having desperately and deliberately poor employment rights, many on zero hour contracts, and many being topped up with ‘working tax credits’ (hence becoming the ‘working poor’). Unsurprisingly, this has done very little to tackle the poor productivity of the UK in general, and the poor tax receipts have been a shocker for running public services safely.
A second pledge is impossible to disagree with. That is, “Secure our NHS and social care”. The emphasis of the current Conservative government has been a traditional one of ‘getting more bang for your buck’ and the euphemistically termed “delivery”, but the crisis in social care has been due to a toxic combination of imposition of private markets and lack of funding matched to demand since 2010. Even Conservative MPs are concerned about the parlour state of social care, which is also having a cost in the economy in people of working adult working age being unable to lead independent lives because of the need to care for “dependents”, for example people living with dementia with substantial caring needs. For a very long time, A&E departments nationally have been unable to meet their targets, and delayed discharges have gone through the roof. But this is not headline stuff due to a corrupt mainstream media – hellbent on their character assassination of Jeremy Corbyn.
No poll, even up until the night of Donald Trump’s eventual election, had predicted accurately the scale of the Republican victory. The general public are continuously being told about the unelectability of Jeremy Corbyn, however, even though British pollsters have a formidably catastrophic recent polling record, for example in the EU referendum or the 2015 general election. No amount of fiasco is too large to displace the vitriolic attacks on Corbyn, whether that be the failure of privatised rail services, the corruption of captains of industry for well known high street brands, an ability to curb the excesses of unconscionably paid people, and so on. But Corbyn himself would be the last person to bank on a three full terms with him as Prime Minister. He is currently 67 – not being ageist, but he would be over 80 if he completed three full terms for Labour. The succession planning for Tony Blair was an unmitigated disaster, reputedly because many of the successors did not want to ‘succeed’ taking up profitable jobs elsewhere.
Talking of which, Jamie Reed is doing himself and Labour simultaneously a favour. There is more of a chance of a pig landing on Mars, than there is a chance of Reed winning in the strongly Brexit seat of Copeland. It is a fact that Labour cannot triangulate itself into making itself very pro European Union for the benefit of many in Scotland and London, while also being anti European Union for very many in England. Whilst there are a few with extreme opinions such as ‘send Muslims back’, there are some who hold the opinion that EU workers are ‘stealing the jobs’ of indigenous citizens due to being able to work at lower salary rates. Theresa May MP has been consistently unable to stick to immigration targets, and Hilary Benn MP would have been better off campaigning on this than sticking the political knife into Jeremy Corbyn? It’s pretty unlikely that Theresa May will be able to deliver on both exiting completely out of the single market and exempting itself from free movement of people, meaning that there’ll be a lot of disappointed people around.
The LibDems have already made their bed, which they intend to lie in. The possibility of another Tory-LibDem coalition beckons (particularly if Kezia Dugdale keeps up her triumphant work of Armageddon in the Scottish labour vote; this catastrophe long predates the Corbyn factor). They in case are not the party of the 52% or the 100%, but the 48%.
I suspect people who claim to want a ‘strong opposition’ want nothing of the sort. They are prepared to continue to undermine Jeremy Corbyn at all costs in 2017, and are fully prepared to see Theresa May secure a mandate for a hardline exit from the European Union.
Jeremy Corbyn for the time being has taken back control of the Labour Party, but his strategy has paradoxically been to make himself not dependent on others to the point of being isolationist. But the strength for Labour will be, as always, when the whole works for the collective good, and is larger than the sum of individual parts. If some people with big egos don’t feel they wish to suffer the indignity of losing under Corbyn for their own beliefs, and want to leave, that can only be interpreted as a good thing. If they can offer constructive criticism as leading Commons select committees, that I suppose is good potentially too. Strictly isn’t bad either.
But if they’re just going to whinge holding onto minor London seats, or larger, they’re better off getting out for the sake of all of us.
Some thoughts on Jeremy Hunt

I’m a card carrying socialist. I don’t know whether I’m a Marxist Trot, but my views are in keeping in what most people would view as for the public good but not in a way dictated by markets free or otherwise.
Not that it matters, but I’ve always voted Labour. The defining event for me was in fact going to Margaret Thatcher’s last ever Prime Ministers Questions. I lived mainly in London in 1990, a stone’s throw away from Leicester Square – and I remember the Poll Tax riots and the tail end of the Thatcher government vividly. I remember the politics of the 1980s vividly, as a child, and I committed never to vote Tory again. I fulfilled that promise, as it happens.
It’s well known I’ve spent far longer as a NHS patient, with an adult onset physical disability as a result of meningitis in my mid 30s, than as a practising junior doctor, though I remember my time as a junior doctor with disproportionate affection. Hospitals for me provoke mixed emotions – I survived a six week coma in one, I saw my father have the cardiac arrest team around him before he did in the same hospital as it happens, and it’s one where I have much goodwill for their ‘dementia friendly’ approach given my current interest as an academic physician in dementia predominantly.
I am not a ‘celeb blogger’ – but then again I loathe the media, and the media hate me. I tweeted recently that ‘I don’t believe a word that Jeremy Hunt says’ – this is on the basis of how his legal team had emphasised he had never imposed the NHS #juniordoctors contract despite him saying on numerous occasions he was imposing it.
But the thing to remember for me is that Jeremy Hunt as such does not ‘act alone’. He went into Theresa May’s first cabinet reshuffle expecting to be dropped like a lead balloon – hence the lack of lapel on his jacket – but he emerged happily in situ. So Jeremy Hunt is fallible – he expected to be sacked.
He sincerely believes what he does – which I think is ‘liberalising the market’, ensuring that Mid Staffs never happens again, producing a workforce less dependent on immigration, and so on.
As it happens, I profoundy disagree with his view on the NHS. I dislike the fact he rarely comments on the idea that provider competition has not improved quality in the NHS, how he has a total blindspot for the social care profession, how he seems in total denial about the catastrophic finances of the NHS, how his electronic IT programme is way off track, and so on.
But again I wonder to what extent this lack of trust in him is entirely his fault. For example, I don’t think the BMA acted par excellence, and I myself wondered how on earth these strikes were not impacting on patient quality or safety. But then again if it’s the case that NHS Providers and NHS hospitals can send out strongly worded letters with impunity then that is that.
The General Medical Council don’t appear to wish to comment much on rota gaps, and general morale, or how #juniordoctors might refuse to sign a contract if they feel uncomfortable, and so on. I’m not in fear of the Council, it’s just I have nothing much to do with them. My personal view is that they could have been far more respect and responsive of the patient safety views of doctors, that’s all.
It says in our code of conduct that if we feel uncomfortable about resources we should say so. Some of us have repeated this ad nauseam – so now what?
I like James Titcombe hugely. I find the story of Joshua incredibly fertile in what we could do for learning from mistakes from the future. But, despite the best will in the world, if Katrina Percy refuses to resign having won once a HSJ award that’s where we are. If I can live with a mistake for the rest of my life, and others don’t, so be it.
I like Deb Hazeldine equally hugely. I can’t even begin to imagine what she feels everyday.
I enjoy my work which is basically advocating for people with dementia. As a carer myself, I am interested in that too. But I know my boundaries. Me ‘hating’ Jeremy Hunt will achieve nothing – he is doing his job albeit with a workforce some of which want to emigrate.
Cuts and low morale I think are a threat to patient safety – but if the General Medical Council feel comfortable with that in their remit, nor with giving proper support to Chris Day’s whistleblowing case, there’s not much many of us can do about it.
I don’t actually ‘hate’ Jeremy Hunt. He MUST, I’m sure, know that the NHS and social care need more money, the workforce largely don’t trust what he says, doctors in India no longer wish to work in the UK whether or not he needs them, and so on.
But it’s Jeremy Hunt – too surreal to fail.

Owen Smith MP must surely have been aware that the NHS is being rapidly privatised?

David Cameron himself slammed “top-down” reorganisations, before introducing a £3bn reorganisation of his own.
The changes which seem to fragment the system and introduce a number of new elements, such as the purchaser-provider split, Foundation Hospitals, were many changes under New Labour. And they did not cohere, and ultimately led to the Health and Social Care Act (2012). That of course is a massive fear of what Owen Smith MP would do to lay the foundation slabs for a future demonic Conservative government, despite his current poetic words.
This issue is beyond party politics, and not even about Owen Smith’s doomed leadership bid.
Not even about my support of any one Labour leadership candidate, or another.
I was unable to get a word in edgeways on a popular radio show about this last night, but I did get a chance to rebut fully a previous caller, by the name of John Redwood MP, Conservative MP for Wokingham. He claimed that there had been “no secret plan” to privatise the NHS, and that the Conservatives had been vocal critics of “Labour’s PFI”.
The “private finance initiative” was started in 1992 under John Major, and continued with much more force under Tony Blair from 1997 onwards. It was exasperating that this is still barely talked about by followers of New Labour as it was continued by the Coalition under George Osborne in 2010-5.
This ‘off budget accounting’ of PFI under New Labour was brought in at a time to address the poor physical infrastructure of the NHS. The risk was transferred to the public sector, while all the reward went to the finance sector. You can even trade in PFI units in the City.
The effect of this substantial privatisation technique? Firstly, due to the ‘corporate wonga’ nature of the loan repayments for these PFI hospitals money for safe staffing is driven to the bone. It is therefore effectively investing in shiny buildings and the City and disinvesting in people and skills in the NHS.
And back to John Redwood.
And, if there had been no “secret plan”, why was it then that John Redwood and Oliver Letwin in 1988 published a document for the Centre for Policy Studies called, “Britain’s biggest enterprise – ideas for radical reform of the NHS”.
On reflection, I actually agree with John Redwood MP.
This plan was far from secret.
And the conclusion could not be more blatant.
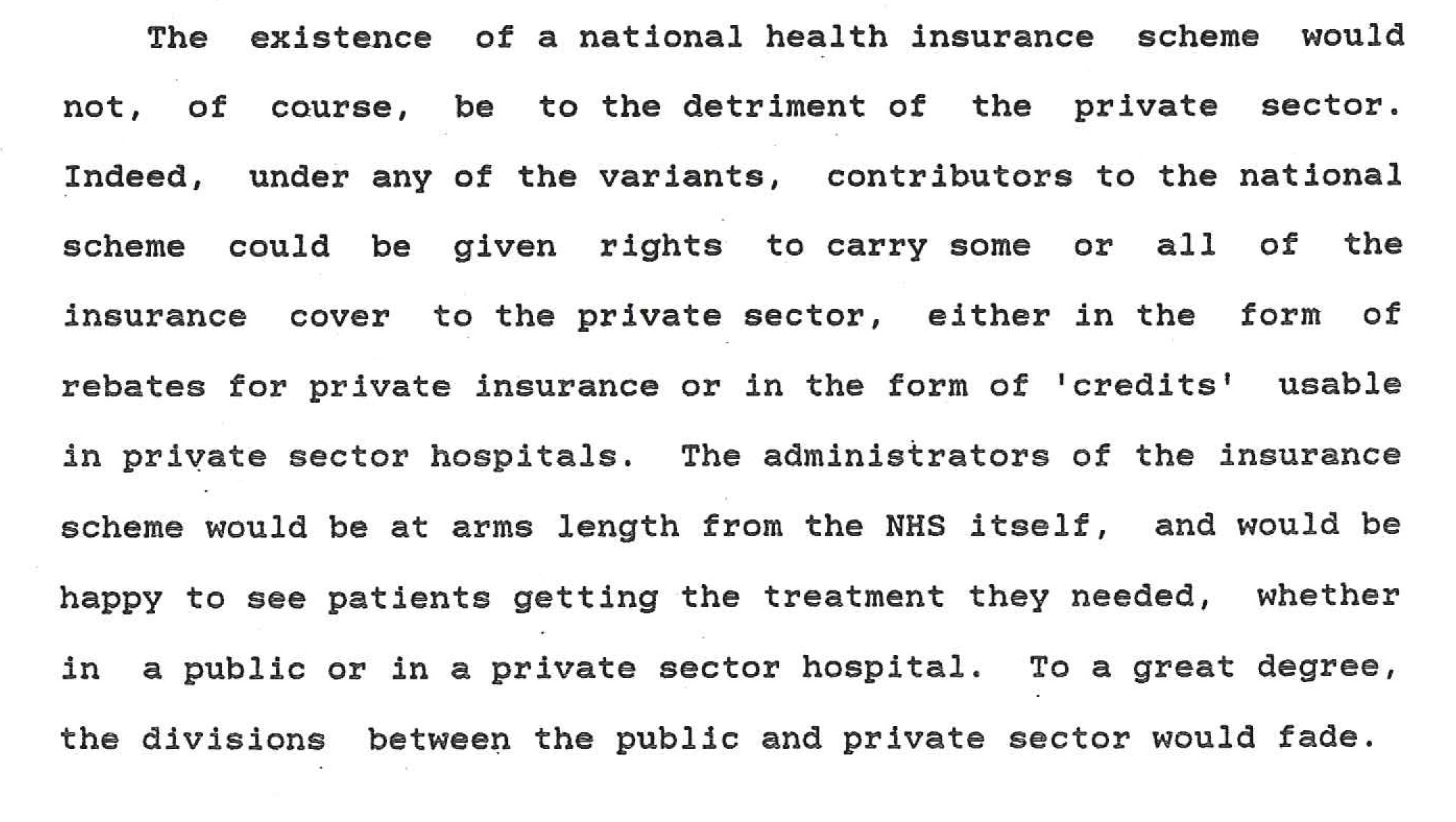
The Conservatives persist with the lie that privatisation is ‘not happening’ and yet boast of how things would be much more ‘efficient’ if the NHS were privatised.
The depth of this deception to the general public is completely laid bare by private companies providing NHS services hiding behind the NHS logo not their own corporate logo.
And you can still buy this from Amazon – authored by now Conservative Peer, Lord David Willetts, from 1993, the ‘golden era’ of John Major PFI.
A Guardian article yet again yesterday outed the lie there had not been any privatisation.
The ‘public face’ of the Conservatives is that they are ashamed of privatisation, whilst propelling it at full force. For Owen Smith MP or any others to argue that they were unaware that they were letting the NHS progress on this privatisation road is either deeply negligent or massively fraudulent, as the facts speak otherwise.
The Conservatives rely on the fact that there’s no ‘big bang’ flotation of the NHS, like the ‘Tell Sid’ campaign of privatising British Telecom in the 1980s.
Of course, the notion of the ‘privatisation of the NHS’ is deeply unpopular. People who are “experts”, like Christine Lagarde, Mark Carney and George Osborne, warning about economic armageddon delivered a #Brexit vote, were utterly rejected in the #EUref, reflecting perhaps the contempt that the City is held by some voters.
This contempt is not superficial – it is an endophenotype of how investment bankers crashed the economy, and yet nurses on their pay freeze or low paid teachers or the disabled are somehow meant ‘to pay for it’.
And then the next trick is to avoid defining what privatisation is. All privatisation is is transferring assets from the public sector to the private sector.
This is completely in keeping with other mutterings elsewhere from the Conservative Party – as described in “Opening the oyster: the NHS reforms in England” by Dr Lucy Reynolds and Prof Martin McKee (Clinical Medicine, Journal of the Royal College of Physicians) April 2012.
“According to a glossy brochure summarising the conference held last October, Britnell told his audience: “GPs will have to aggregate purchasing power and there will be a big opportunity for those companies that can facilitate this process … In future, the NHS will be a state insurance provider, not a state deliverer.” He added: “The NHS will be shown no mercy and the best time to take advantage of this will be in the next couple of years.””
(David Cameron’s adviser says health reform is a chance to make big profits, 14 May 2011, Guardian)
And remember Oliver Letwin MP, John Redwood’s co-author of the pamphlet above?
“Oliver Letwin has reportedly told a private meeting that the “NHS will not exist” within five years of a Conservative election victory. The Shadow Chancellor said that the health service would instead be a “funding stream handing out money to pay people where they want to go for their healthcare”, according to a member of the audience. The remarks, which have been furiously denied by Mr Letwin, were last night seized on by Labour pecks evidence of the Tories’ true intentions towards the NHS. It is not disputed that Mr Letwin met a gathering of construction industry representatives in his constituency of Dorset West on 14 May. During the meeting he urged the group of around six local businessmen to work together to win contracts for a new PFI hospital to be built in Dorchester. Mr Letwin then astonished his audience, however, by saying that within five years of a Conservative election victory “the NHS will not exist anymore”, according to one of those who were present.”
(“Letwin: NHS will not exist under Tories”, Andy McSmith, 6 June 2004, Independent)
It is simply up to the Conservatives and New Labour to defend this blatant policy, rather than lying to the public about it.
I’ve mentioned one technique which has delivered poor value for the taxpayer (the poor value for money to subsidise shareholder profit is an onrunning Conservative and New Labour theme; it is no accident that the privatisation of the NHS was conceptualised by Andrew Lansley like the privatisation of the utilities).
But there are many other techniques – and they’ve all been attempted/completed.
For example, the privatisation of auxiliary services – e.g. chemists, cleaners, lab staff.
Or, the selling off of NHS property (including buildings and land).
Or, the rampant outsourcing of NHS services/contracts to private sector (Health and Social Care Act 2012, section 75).
The components of the NHS privatisation jigsaw have been put in place by Tony Blair’s re-introduction of the internal market, and the introduction of the purchaser-provider split. (Tony Blair had originally won a mandate to get rid of the internal market, which had been advanced in statutory instruments such as the NHS and Community Care Act, but actually in the end ended up amplifying it. It is argued that Frank Dobson tried to stem the advance of the private market, but his work was thwarted in this respect by Alan Milburn)
And we know from New Labour’s watch, that the rush for Foundation Trust status, including financial competitive autonomy, means that some clinical services went down the pan. New Labour don’t like talking about Mid Staffs much for good reason.
There is no evidence that the private sector in producing clinical services is any more efficient.
In fact, there’s substantial evidence that there’s massive reduplication of unnecessary work, as that can cause repeated billing.
And it was a farcical situation when under a previous Government a merger could not take place which would have been for the benefit for providing better quality clinical services, as it breached competition law.
And the mere act of funnelling everything through private contracts, consequent to 2012 (and laid in place from the New Labour NHS Act 2007 and Public Contracts Regulations 2006), has seen a massive amount of extra paid work for corporate lawyers in litigation and other dispute work.
What is even more incredible is that a ‘serious’ Labour leadership candidate could have been unaware of this.
If the Right of the Labour Party want to throw their toys out of the pram, and split, and not support democracy or the vast majority of the membership of the Labour Party, they’re welcome to leave.
But – parliament is ultimately about sending delegates who represent the public’s feelings, not representatives of a big slick corporate marketing machine.
And look what happened to the SDP in the 1980s.
Privatisation timeline
It is necessary to refer to the Adam Smith document by Pirie and Butler (entitled “The health of the nations – solutions to the problem of finance in the health care sector”) which charted all of this – in 1988.
Phase I 1988 – 1997 Thatcher/Major Abolition of District Health Authorities
“Perhaps a better candidate for abolition or reform, however, would be the tier ofDistrict Health Authorities”
The NHS internal market, and purchaser-provider split
“There must be more of an internal market within the NHS — that those units and districts with excess capacity or with some particular expertise should be more able to market their services to others who need them.”
Phase II – Blair and Brown (1997-2010) Payment by results, Foundation Trust hospitals and HRG diagnosis-related groups systems
“With a direct charging mechanism, with hospitals as cost centres, and with the use of management budgeting techniques by which each service provided by a hospital can be properly costed, such an I internal market could be vibrant.”
Use of private sector hospitals to clear NHS waiting lists for elective surgeries
“Private hospitals, undertaking 400,000 operations per year, have a number of special strengths: they are particularly experienced at hip replacements, for example, because many older people who have saved to make their retirement comfortable happily spend the money on going private rather than waiting for two years or more in the public sector. Buying in such operations from the private sector — with NHS patients going to private hospitals for their treatment, but continuing to receive it free of charge — could be a cost effective way of clearing the waiting lists.”
PFI It is of course remarkable that in an article called “Private equity pioneer”, the impact of Michael Queen is laid bare. The timing of this is particularly noteworthy, predating the Blair government commencing 1997.
“CEO of 3i Michael Queen on his accountancy roots and how private equity can help develop world infrastructure. As chief executive of 3i, a FTSE 100 company and one of the world’s leading international private equity groups, Michael Queen is one of the most influential business people in Britain. In his 23 years with the firm, Queen has notched up many successes. Working his way through a variety of roles including finance director, he led the firm’s growth capital business and founded its infrastructure investment arm. In the mid-1990s, he found time to pioneer the NHS private finance initiative (PFI) which kick-started hospital building in the UK for the first time in decades. Recently, as CEO, he’s turned a £2bn debt in 2009 into £350m currently, built some £2bn in cash reserves and led a restructure of the group’s private equity business. And he’s just won the ICAEW’s Outstanding Achievement in Corporate Finance Award for his major contribution to UK business, entrepreneurship and the economy. But none of these are the moments that have defined his career. That was getting a position as an accountancy trainee with Coopers & Lybrand.”
As Andrew Sparrow outlined in an article last year in the Guardian,
“George Osborne, the chancellor, is pressing ahead with private finance initiative (PFI) projects on a multibillion-pound scale despite having dismissed the infrastructure funding mechanism as “discredited” when he was in opposition, research has revealed. A report on Channel 4 News shows 61 PFI projects, worth a total of £6.9bn, have been taken forward since the general election. This is despite claims that private sector borrowing costs currently make PFI particularly poor value for money.”
The Health of Nations had provided:
“The private sector may also be able to help in terms of raising capital for new facilities. In areas where medical treatments have been contracted out, one of the first actions of the private sector providers is commonly to scrap existing buildings and equipment and start afresh with facilities that are less costly to maintain and more pleasant to work in. Sale and leaseback arrangements might well be a good way of raising capital for the public hospital and simultaneously contracting out certain forms of care, such as long-stay care, which the private and charitable sectors might be better able to provide anyway. Contracts with private consortia to design, build, and operate complete hospital units on behalf of the Service would seem to be a logical extension of present practices. In addition, they could provide aninteresting source of new approaches to medical care.”
Phase III – Cameron/Clegg (2010 – present day) Formation of the NHS National Commissioning Board
“Making the Service less political may help to solve some of these problems. At national level, it might be better to run the NHS through a board which, like other nationalized industries, does not include the direct involvement of government ministers and does not allow their day-to-day involvement in the running of the industry, but is ultimately responsible to them.”
Monitor and the licensing of CCGs (or “HMUs”)
“With the management of the NHS switched over to HMUs instead of Regional and District Health Authorities, national supervision of the HMUs will be necessary. A ministerial body will license each HMU and specify the standards which they are required to attain. It will also have the responsibility of ensuring that the levels of service reach those required. It will publish the criteria and compare the performance of HMUs across the country. If the HMUs make use of sub-contractors for certain aspects of health care, these, too, will be required to attain what are deemed to be the appropriate standards.”
“Perhaps one of the most exciting new ideas, however, is the concept of management by contract, which works well abroad and is just now being tried out within the NHS.” “contracts can be of any duration, though five years is a workable minimum” “In this new version, however, it is the managers who are under contract, rather than the front-end service workers. The skills needed to run each function come not from in-house managers but from outside experts, hired under a contract of finite duration. They must achieve whatever targets are negotiated and agreed at the beginning of the contract, or risk losing their work to a competitor.”
2012-2013 Outsourcing of South-East London & Northwest Healthcare Trust
“Contracting out the management of an entire hospital, including the medical services, could lead to greater opposition, but on, the other hand it might be seen as a lifeline to units that are threatened with closure because of demographic changes, smallness or obsolescence.”
Choose and Book (“AQP”) with CCGs funded by PHBs (“vouchers”)
“In more radical versions of the idea, however, patients are given a wider choice about the NHS doctor and hospital they want to treat them, and the average per caput health expenditure represented in the voucher actually follows them when they choose.”
Introduction to CCGs (Clinical Commissioning Groups) funded by PHBs Abroad, in the Netherlands, “unintended consequences” of PHBs have now been described. The “Health of Nations “provides:
“Fundamentally, HMOs offer a complete health care delivery service to groups of individuals in return for a fixed and prepaid annual premium. A group, such as a group of employees contracted into the HMO by a company, pays a premium on joining the scheme, and for that the HMO guarantees to provide each member with all the GP and hospital care that may be needed in each case. The scheme managers will in turn contract with the doctors and hospitals they need in order to provide this whole-care service.”
The CCGs use the PHBs to contract with GPs of CCG member practices & purchase hospital and other secondary care through competitive tendering or through Choose and Book (“AQP”)
“For example, we might break down the NHS delivery system in a particular city or area, transforming it into a series of competing whole-care delivery plans on the HMO model, whose budgets were allocated on a per-patient basis rather than from a DHA grant, and who contracted with their own doctors and bought in the necessary hospital treatment from the private or public sectors.”
The insurance risks for CCGs are highlighted
“However, difficulties remain. There are still no obvious structures presently in existence within the NHS which would provide the nucleus around which new HMO-style systems could be grown. Some group — managers or doctors — have to accept the risk that they can deliver a complete health care service within the per caput budget, and neither group currently working inside the NHS is likely to accept that new challenge with much pleasure. In fact, staff at all levels would be worriedby the prospect of their service being divided into competing units.”
Patient choice will not extend to consultation over exchanging universal tax-funded NHS coverage for an insurance-based healthcare
“Even if a new structural arrangement could be devised, there would be the problem of how to allocate residents to each of the new plans. A free individual decision to stay with the present structure or opt for the new plan might be dangerous in the initial stages at least, because those in most need of treatment might self-select. Thus, it would be a case of compulsorily transferring patients from the existing structure into the new plans, which again might not be a popular proposal. Any move to explore the possibilities of how best to do this, however, would undoubtedly meet loud objections against using NHS patients as guinea-pigs for some new organizational theory.“
Phase IV Cameron/Clegg (2012-5) Abolition of SHA & PCT management superstructure
“The key to reform of the NHS, as in education, lies in reorganization of its management structure. In place of the Regional Health Authorities and the District Health Authorities there should be management bodies which have every incentive to spend resources in ways which are cost effective and attractive to patients. These bodies should be funded from taxation and should have the responsibility of proving a full health care service for patients. They should distribute resources to general practitioners at the primary level, and to hospitals and consultants at the top. They will be, in effect, Health Management units (HMUs).”
CCGs as statutory health insurance? The idea of CCGs as “insurance schemes” has been previously mooted. The ‘pooling of risk’ is explicitly referred to in the Department of Health’s Health and Social Care Bill (2011) impact assessment thus:
“CCG Size: There is no consensus on a minimum size to handle the financial risk.2 5 Inter-GP relations and peer review are strong forces and can counter the effects of higher statistical risk in smaller CCGs for many services. However, while some high risk services are best covered at a more regional level, risks could be shared by CCGs grouping together to form their own risk pools.”
Meanwhile, the “Health of Nations” provided,
“The public sector HMUs, taking responsibility for total health care of NHS patients, are not too far removed in structure from private insurance and management bodies. The funds for premiums are publicly provided, but the same competition and incentives operate, and the same choices are made available.”
PHBs as the basis of calculation of the funding allocated to CCGs
“The HMUs themselves will have to provide total health care on the basis of an average annual allocation per patient. They will have the incentive to make sure they get value for money from the GPs who subscribe to them, and for the hospital and consultancy work they obtain for their patients.”
Performance management of GPs and hospitals by CCGs
“They will have the incentive to make sure they get value for money from the GPs who subscribe to them, and for the hospital and consultancy work they obtain for their patients.”
Situation of GPs once CCGs are authorised
“The HMUs will be licensed non-profit bodies responsible for the total health care ofthe patients registered with their doctors. They will be management bodies, drawingupon the existing skills of health managers.” (p.32) “The HMUs will be required to buy hospital and specialist services for their patients as required” “The payment and monitoring of their GPs will be part of the task of HMUs, and will be performed in ways which ensure value for money. Cost details of GP work will be compared, and action taken where necessary to improve efficiency. HMUs will be vigilant in the selection of specialist and hospital services for their patients. They will be concerned to provide these on the most cost-effective basis they can, because the less they pay for each service, the more services they ‘will be able to offer to patients’ and the more attractive will be the rewards they can offer to personnel. The HMUs will not operate on a simple least-cost basis, but on a most cost-effective basis. Patients and their GPs will have the choice to move to an HMU whose services are more attractive, and will take with them the state’s allocation per patient. It will be very much in the interest of the Health Management Units to lower the cost per patient by timely preventive work and early diagnosis by regular check-ups. The move to HMUs will have a dramatic effect on the costs and the efficiency of hospital treatment. As hospitals go to independent management they will have to cost each service and will need to be aware of precise cost information. They will be very much more flexible in their management and method of operation. Pay scales will be more flexible and will be negotiated on a local basis instead of the rigid system of national scales and procedures. It is doubtful if restrictive practices in operation at present in the NHS will survive the changeover. There will be an incentive towards efficiency and flexibility, as well as to specialization. In some areas it is quite possible that HMUs will send their patients to the private sector for some categories of service and treatment. Where private clinics offer better value than state hospitals, there will be every incentive for them to do so. What certain hospitals do in particularly effective ways they will be able to sell widely, leading to the expansion of what each does well. The result will be for a new partnership of private and public medicine, with the services of each available to NHS patients on the basis of their comparative efficiency. An early result of the switch to HMUs will be the development of specialist low-cost treatments. Existing NHS hospitals and new intermediate facilities will have every incentive to develop methods of treatment which can bring economical results. Again, the example of other advanced countries and the private sector in Britain suggests that new methods will be pioneered which involve shorter hospital stays, more localized services, more preventive medicine, and a generally less costly style of care. The incentive will be there with HMOs seeking to provide health care efficiently. HMUs and hospitals will be able to undertake new capital projects with a combination of central grants and monies raised or saved locally. Funds from the private sector might well be attracted to areas which promise a saving on current expenditures. GPs acting singly or in groups will have the incentive to add facilities, perhaps leased from their HMUs, in order to compete with the cost of more expensive hospital services. Some of the work which now has to be done in hospitals will move out to smaller and lower cost treatment centres, some in the surgeries of doctors.”
Abolition of GPs’ Minimum Practice Income Guarantee announced October 2012
“The proportion of remuneration which derives simply from having patients on their books will disappear, leaving payment only by results.”
Patients and their GPs will have the choice to move to an HMU whose services are more attractive, and will take with them the state’s allocation per patient.
“It will be important to prevent HMUs from selecting patients by picking the one’s which cost least to treat. HMUs will be required to accept patients who register with their doctors, without any selection permitted other than on the basis of optimum size of the HMU. Even here, where patients are refused because an HMU is at its optimum, waiting lists will have to be established with new patients admitted in order of application as places become available.”
CCGs as a vehicle for increasing uptake of private sector hospital care and other commercial services
“In some areas it is quite possible that HMUs will send their patients to the private sector for some categories of service and treatment. Where private clinics offer better value than state hospitals, there will be every incentive for them to do so. What certain hospitals do in particularly effective ways they will be able to sell widely, leading to the expansion of what each does well. The result will be for a new partnership of private and public medicine, with the services of each available to NHS patients on the basis of their comparative efficiency.”
GP incentive scheme?
“GPs acting singly or in groups will have the incentive to add facilities, perhaps leased from their HMUs, in order to compete with the cost of more expensive hospital services. Some of the work which now has to be done in hospitals will move out to smaller and lower cost treatment centres, some in the surgeries of doctors.”
CCG funding
“The basis of funding will be the annual health allocation for each patient registered Health Maintenance Organizations is largely avoided by keeping patients with their present GP. The resources go to the HMU selected by the doctor, although the ultimate choice lies with the patient, who can change HMO by going to a doctor registered with another one. The resources are thus directed to the HMOs which are most favoured by doctors and patients.”
PHBs calculated with demographic weighting
“The size of the average health allocation will be set each year, and there will be pressures to keep up with an advancing standard of living. A major difference is thatthere will be internal competition, with some HMOs managing to offer a greater range of services than others do on the same per caput budget. There will be the option available to vary the health allocation for each patient according to the local health costs. Geography will play a part, but so will the age pattern of the population. It may be desirable to vary the allocation by category of patient, on the grounds that older patients are more expensive to care for. This is not different in degree from varying the central funding for each age group of child in the education system.”
Personal health budget (partial roll-out now commencing) as allocations calculated for individuals which the individuals can transfer from public to private sector providers (from CCGs to insurance companies selling NHS top-up insurance)
“Under this idea, each individual would receive from the state a health voucher, equivalent in value to the average per caput sum that is presently spent on providing health care. The voucher can be used towards the purchase of private health insurance or exchanged for treatment within the public sector health system. Through this mechanism, the state honours its assumed obligation to ensure that everyone has access to health services. Those who opt into private insurance can use the voucher to pay their premiums, and the insurance companies then collect the cash value of the voucher from the government. This guarantees that everyone can afford at least a basic level of insurance cover, and (perhaps more importantly) it allows each individual a choice between different insurers and insurance packages, no matter how rich or poor they might be. However, people who decide that health care is particularly important to them are free to add to the amount covered by the voucher and thus purchase more expensive forms of insurance, perhaps covering more unlikely risks or providing superior standards of comfort or convenience. The voucher does not force people into private insurance, although it certainly makes the option of going private instantly available to everyone. Those who want to use the state service will continue to receive it, their voucher being their ticket to free treatment just as their national insurance number is at the moment. Under the more modest voucher proposals, that is the end of the story, the NHS continuing much as before — though perhaps losing some customers to the private sector that has suddenly become so much more affordable to all. In more radical versions of the idea, however, patients are given a wider choice about the NHS doctor and hospital they want to treat them, and the average per caput health expenditure represented in the voucher actually follows them when they choose. Thus, the pressure of competition is introduced in the public sector as well, because those doctors and hospitals which are popular with patients will be taking in more vouchers and thus getting a larger share of the government’s health budget. There are strong incentives to improve standards of care and to regard the patient more as a paying customer who must be satisfied.”
CCGs as transitional structures leading to unification of the NHS with the private healthcare industry
“Perhaps the greatest advantage lies in the flexibility of the new system. In place of the rigid demarcation between a public health service which does what it can on a take-it-or-leave-it basis, and a private system for the rich which offers choice and competition, the distinction between the two is blurred. They begin to overlap, each on the territory of the other. “
CCGs as insurance mechanisms
“The public sector HMUs, taking responsibility for total health care of NHS patients, are not too far removed in structure from private insurance and management bodies. The funds for premiums are publicly provided, but the same competition and incentives operate, and the same choices are made available.” “This convergence is one of the most attractive features of the change which HMUs will bring. The HMU principle lays the groundwork and the basis for further changes at a later stage, but it brings its benefits immediately. Most of the groups involved in health care stand to gain from its introduction, the patients most of all. It is from realities such as this that change is made possible.”
Phase V Here are the new resources to be brought into the healthcare system that the 2010 White Paper mentioned: payments to private health insurance companies from private individuals to pay for their healthcare, as in the USA. PHBs have been created in the form of transferable vouchers which can be spent on a pooled basis through CCGs or transferred to supplement a purchased top-up insurance policy. Such top-up policies are already being marketed intensively in England as the insurance industry prepares for the Transition planned by the DH.
“At present in the UK, car drivers are required to have a motor insurance policy that compensates other people in the event that they cause damage or injury in an accident. Similarly, it is argued, we could meet the health needs of everyone without the need for the government itself to provide health services through the NHS, simply by requiring that all individuals have medical insurance cover for a range of services that are deemed to be the acceptable minimum standard of health care. Of course, those who wished to have a superior standard of service could take out a more extensive policy: there would be no Objection to individuals insuring themselves for additional or more costly services, as long as the basic requirements are met.” “A key advantage of the universal private insurance approach is that individuals have much more choice and that the insurers and health care providers face far more competition than the NHS faces at present. Although people are obliged to have a minimum level of medical insurance cover, they can shop around between insurers and decide which provides the best value for their premium money. Because there is competition, they can decide which insurer’s particular package of services is most suited to their individual needs, instead of having to accept the standard service provided by the NHS. In addition, they can spend more on their health care, if they judge it worthwhile, than is presently spent on their behalf by the government, so new resources will be brought into the health care system.” “Under this idea, each individual would receive from the state a health voucher, equivalent in value to the average per caput sum that is presently spent on providing health care. The voucher can be used towards the purchase of private health insurance or exchanged for treatment within the public sector health system.” “The actual provision of health care services in such a system of universal private medical insurance would be undertaken by private sector doctors and hospitals, and the nationalized health sector in the shape of the National Health Service would lose its reason for existence.”
Owen Smith MP is doing a great disservice by pretending to be the ‘controlled opposition’ to the privatisation of the NHS, when there are great NHS campaigners who have vociferous about this for years.
As such it won’t matter – as I bet my life Owen Smith MP won’t win the Labour leadership.

From my vantage point as a junior doctor, I can tell you the NHS is not in a good place


When Jos Bell, experienced campaigner for the NHS, says she wept at the end of yesterday’s march, you know two things. First of all, it was an amazing event. Secondly, there is something very wrong with the NHS.
In my brief time on the wards, I witnessed how the Hammersmith A&E department ‘functioned’. And how Addenbrookes managed its acute take. And also the daily chaos in Northwick Park. It was pretty unpleasant training, covering the acute medical unit and all the medical wards at night simultaneously, with the cardiac arrest bleep. I note with some mirth the eventual fate of those hospitals. I am glad I am not the only one who had his doubts.
A decade ago, I am still technically a junior doctor, as is anyone technically below Consultant level in hospital medicine. What I do know from my vantage point on the GMC Medical Register is how to produce and share research and learning about living better with dementia and to enjoy it. I get considerable pride in what I do, which is ultimately to improve the quality of life of people with dementia and carers. This was acknowledged in my BMA Best Book of the Year Award 2015, though I think the NHS is saturated with competitions and award ceremonies.
The NHS is really not in a good place – and nor is social care. I don’t think I’ve ever known a peaceful time in the politics of the NHS, but the current Secretary of State, Jeremy Hunt MP, is uniquely bad. I share his anger with how bad things got at Mid Staffs, but it is also the case that the place has been a reputational nightmare to recruit at ever since.
The safety at weekends does not require a highly paid NHS manager to work out. You have a skeleton staff trying to do their best in what is already a seven day service. With so many Trusts in deficit, I look forward to the day when the staff to bed ratio is the same at the weekends as it is during the week, and Hunt has to concede that he cannot achieve this with the same number of staff just doing ‘different things’. It is utterly unacceptable that he has whipped the general public into a frenzy such that members of the public are now frightened to seek medical help at the weekend: if a doctor on the GMC register did that, he’d be heavily disciplined. For politicians, a seat at the House of Lords beckons instead.
But it is not Hunt’s operational ineptitude which gives me most distress. It’s just that he seems to have complete and utter contempt for the staff in the NHS. He reckons that professional people who’ve done at least five or six years unpaid before qualified are being ‘misled’ by the BMA, implying that they are too stupid to make up their own mind about the new terms of their contract.
This lack of investment in people, while simultaneously siphoning off money in payment of PFI loan repayments, is evident too in the lack of pay rise for many nurses. The wider picture is certainly concerning. George Osborne MP is clearly involved in the fire sale of State assets, and this has included NHS tangible property, so it will be natural for him to think what else he can transfer to the private sector to make his books balance.
Being fixated on the deficit, which he has not fixed by 2015 as promised, means that he has not be able to address the mess in social care funding. Social care is on its knees, and it is not acceptable that there are people languishing in hospital who literally can’t escape even once discharged.
The NHS is not going to be ‘saved’ by gimmicks with hashtags into quality mightier than the sword on Twitter. It, like social care, is going to be saved with proper funding and investment for the future – not with a view to selling it off at some later date.
So, in full solidarity, this mess has been a long time coming, and I fully support the junior doctors (of which I am one, technically). It will not be understood by well paid journalists in their ivory towers necessarily, and certain high profile people need to concede some lack of progress in ‘curing’ the NHS.
Labour now must prove that the NHS is safe in their hands

I’ve lost count of the number of times when the UK Labour Party have stated ‘only 24 more hours to save the NHS’. As somebody who has always voted for Labour in fact since 1992, I take no pleasure in saying that Labour now must prove that the NHS is safe in its hands.
If you believe that the NHS is a cherished institution, or even a ‘sacred cow’, with massive public goodwill, it might seem strange that the Secretary of State for health, Jeremy Hunt MP, plays so fast and loose with junior doctors’ pay. A reason that Jeremy Corbyn MP, the current leader of the opposition and leader of the Labour Party, is so despised, apart from not turning up to gala rugby matches or singing the national anthem, is that he has effectively torn up the rule book. It’s no longer a case of ‘balancing the books’ – and let’s face it Osborne has been dramatically unsuccessful in even doing that – but it’s a case of making sure the customer doesn’t get ripped off from rail privatisation or has a decent living wage.
A favourite line of attack for Progress, the think tank which caters well for Labour believers who believe in modernity, is that ‘money does not grow on trees’. This is of course a full throated lie when you factor in that George Osborne himself got out the printing press recently, and did rather well out of it.
It has been convenient to misquote Liam Byrne MP as ‘there’s money left’ to perpetuate the idea of ‘living within your means’. That is except for the investment bankers who were not living within their means, and had to suffer the indignity of one trillion pound of a State bailout to help subsidise their lavish bonuses and more.
The austerity in the NHS is better known as ‘efficiency savings’, except here money is leaking like a sieve. The Conservative mantra that you need a successful economy is utterly fraudulent when you finally acknowledge that national debt since 2010 has gone through the roof. It also becomes hollowed out when you consider the high number of NHS foundation trusts running a deficit, because they have not been – take a deep breath – given enough money to run the NHS.
This was of course the biggest lie about the word ‘sustainability’ which many came to know as code as ‘we don’t want to afford it’. This means that it became a tough public choice that we didn’t want to afford the pay of nurses or junior doctors, but we could somehow afford the unconscionable loan repayments to the City for shiny new PFI buildings.
The lack of ability of Labour, like the Conservatives, to do something about the private finance debt, not just talk about it in a public accounts committee, is staggering. The current crisis in agency staffing could have been totally avoided with better planning.
Jeremy Corbyn wishes to give an apology for the Iraq War. But this is not the only apology that Labour needs to make over policy, although other apologies are less serious. For ages, Labour peddled the myth that quality between autonomous foundation trusts could be driven up through competition. To acquire ‘foundation trust status’, NHS hospitals had to reach targets, and even if NHS CEOs ultimately failed they could move onto other equally lucrative posts.
To make the financial books balance however, it is sadly the case the legacy was that some Trusts did not run their operations safely. The issue of lack of planning, in an unsocialist way, also is evident in the way in which Labour embraced independent sector treatment centres; the argument ‘to increase capacity to deal with demand’ was an entirely synthetic one, given that the NHS has been increasing significantly in demand since 1946.
So it is quite possible that the election of Jeremy Corbyn as leader of Labour is a stop to ‘more of the same’. This entirely depends on how much Corbyn’s private views are tempered by his shadow cabinet, and Corbyn has tried to bring dissenters into his tent to manage the situation in the same way Abraham Lincoln had many years ago.
To give Burnham credit, there was the beginning of a discussion of bringing health and social care together. Such discussions have nonetheless failed to reconcile how an universal NHS system can be bolted onto a means-tested social care system. The relics of personal budgets, which also have been identified as a practical way of devolving cuts and rationing, continue in policy, and have been furthered rather than extinguished by recent legislation.
Labour itself did much to wreck social care with privatisation, and, whilst we have had relentless cuts in social care funding in recent years which have also affected the way in which the NHS works, the problems started a long time before 2010. But Labour has for me much to prove on the NHS. It’s a long time since ‘the spirit of 45′, but Labour cannot just function as a shrill shroud waving protest party. It needs to have, at last, a sensible debate about all these matters which have been festering for far too long.

The electoral arithmetic potentially could turn out good for the NHS
Be in no doubt. This is a very complicated UK general election.
It’s pretty likely that the SNP will gain a huge number of seats in the Westminster parliament. Many of us sadly forecast this. Jim Murphy and Kesia Dugdale were not the people to inspire the Scottish electorate to a good representation. At the time, it was pretty clear that many would go back to their constituencies and prepare for a hung parliament.
The situation is this. Ed Miliband wants a coalition with the SNP over his dead body. He has ruled out ‘a deal’, although this does not exclude lots of mini-deals to get a minority Labour government legislation through. A critical test for a Labour minority government will be whether the SNP can support a Labour government on a case-by-case basis. The economy clearly presents a problem, but many people feel that Ed Balls is ‘the weakest link’. Allowing for eased austerity and boosting consumer confidence and demand might be good for a weak recovery in the UK, and certainly the Green Party and the SNP should like to establish this.
The Liberal Democrats clearly fancy themselves as tempering the Government on preventing a lurch to the left or right. However, the credentials of the current Government are not much to brag about. National debt has gone through the roof. With the Coalition’s policies, a ‘fair society’ is not evidenced by the decimation of English law centres (aka access to justice). If Nicola Sturgeon becomes the Deputy Prime Minister of the United Kingdom, she is exercising her democratic right to be a force within UK politics, given that it was also an exercise of democracy that Scotland did not become independent.
Both the Green Party and SNP talk the talk on wanting a public-run NHS, and the proof of the pudding is in the passing of legislation. Both political parties are expected to be keen to reverse the Health and Social Care Act (2012), getting rid of the toxic sections 75 and 76 which makes competitive tendering a must if there’s more than one bidder. Given that Nick Clegg is keen to apologise for tuition fees, it is possible that Norman Lamb, if given a rôle in government as an experienced care minister, might support integration. Integration is a ‘must’ to make Andy Burnham’s “whole person care” work, bringing together a national health and care service, with pooled budgets, integrating physical, mental and social care. There are potential advantages in having a Liberal Democrat influence on health and care policy now, parking aside previous differences, on securing funding for the future for 2015-20 and giving prominence to mental health and parity of esteem.
In terms of personalities, it is going to be incredibly tough. But you can bet your bottom dollar that Nick Clegg will want to leave the scene, as there is animosity between him and Labour, and the feeling’s entirely mutual. Many Labour members also want him to lose his seat in parliament to a very good Labour candidate in Sheffield Hallam. Nick Clegg might not want to be physically there if Ed Miliband is Prime Minister, and Miliband takes the lead in scrapping the Bedroom Tax and the Health and Social Care Act (2012).
The alternative is pretty dreadful – of a Conservative government propped up by any party which wants a referendum on Europe, i.e. UKIP. Another toughie is going to be Trident, but it is likely that the majority of the Conservative Party, Labour Party and Liberal Democrats will vote against others such as the Greens or SNP on such a vote, whipped or not.
The structure and function of a possible Labour minority government is complicated, but there is actually a possibility that the relationship is a more meaningful relationship that the current Coalition. The electorate, strangely enough, might be producing a best possible outcome.

Two Titanic democratic deficits are colliding: Scotland and the NHS

Two huge democratic deficits are about to collide: what the general public feel about the NHS and the action of governments, and also the government of Scotland.
The Health and Social Care Act (2012) did not have a single clause on patient safety. It did not speak to Mid Staffs.
Remember when David Cameron promised ‘no top down reorganisation’?
It did, however, contain a very nifty clause, distinct from the legislation which had preceded it, providing a massive legal threat to those NHS contracts which did not go out to competitive tender in section 76(7).
It was clear that this legal threat was not innocent at all, as previous experience from the Netherlands had been very costly.
I reviewed back in January 2013 that in the Netherlands, a year previously, competition law authorities fined the national GP association £6.4 million for trying to prevent the same situation as has been allowed to develop in Sweden, rural areas unserved by primary care services (reported in the British Medical Journal).
This legal pincer grip continues to have sharp teeth. Earlier this year, it was reported that a complaint by private healthcare operators had been upheld against Blackpool CCG on the basis of ‘insufficient choice’.
A lot of damage has done in the English health policy in the name of competition and choice. The idea was that competition would drive up quality and drive down costs. Because of the nature of the oligopolistic market, as would be predicted, this has not happened.
This competition policy has been aggressively pimped in the academic journals as a ‘success’ for New Labour’s health policy between 1997-2010, and together with the public private initiative and TTIP formed an unholy mess.
The privatisation of social care in England is well known to have been a disaster, an explosive mixture of austerity, outsourcing and privatisation opportunities and poor employment bargaining.
In England yesterday, the current Prime Minister framed low taxes as ‘a moral decision’. Low taxes means, however, theoretically less money you contribute to the running of public services such as the NHS, and more you can spend elsewhere for example on private health insurance.
And it has all being elegantly through: the ability to take your pension as a lump sum encourages the free movement of capital into private industry too.
The SNP have now got a clear lead in the polls, and the tendency has been for this to be under-reported in England, emphasising instead that the Conservatives and Labour are ‘neck and neck’.
Whatever the claim and counterclaim, Scotland made a clear departure from the English pro-privatisation legislation back in 2011, and is set to complete the current phase of devolution with a Scotland Bill to be presented to parliament later this year.
As a Guardian newspaper report in 2011 revealed,
“The rhetoric may be strident, but Scottish Government ministers at least practice what they preach. Across a whole range of areas, public versus private sector, telehealth, pooling health and social care and streamlining management, the devolved government has adopted a markedly different approach for the NHS in Scotland. And although that health service had long been administered separately from that in England, it was the creation of the Scottish Parliament in 1999 that made this increasing divergence politically possible.”
So a critical question becomes would the SNP be willing to vote on non-Scottish issues such as the NHS?
The answer, as of January 2015, appears to be “yes”.
Sturgeon explains:
“On health, for example, we are signalling that we would be prepared to vote on matters of English health because that has a direct impact potential on Scotland’s budget. So, if there was a vote in the House of Commons to repeal the privatisation of the health service that has been seen in England, we would vote for that because that would help to protect Scotland’s budget.”
In exchange, the SNP viewed in public during the referendum campaign that Scottish independence as producing a sustainable financial budget for the NHS, hence the smirks from Sturgeon when Nigel Farage claimed that Scotland gets a relatively good deal from “the Barnet Formula”.
Labour’s policy is for the NHS to be the “preferred provider”, but only in January 2015 the English NHS achieved its “biggest-ever privatisation of its services in a deal worth up to £780m intended to help hospitals tackle the growing backlogs of patients waiting for surgery and tests.”
But this policy does not go as far as the SNP one. For a start, the Labour policy still retains the failed quasi-market and purchaser-provider split.
The anti-austerity arguments run that if you ease off the rate of austerity then you can encourage consumer-led growth, increasing tax revenues, and encouraging a recovering economy.
The direct parallel of this is the austerity-induced ‘efficiency savings‘ in the NHS, an austerity narrative which has seen some English NHS hospitals running unsafe staffing in the aim of balancing budgets, because neoliberal parties do not wish to entertain funding the NHS properly.
The freeze on pay in nurses, therefore, looks ideologically driven, as opposed to using pay to incentivise performance of staff as in any other industry. Also, national policy appears to give the impression that nurses are immune from any recovery in the economy due to this imposed austerity, which is a crying shame.
Of course, the trade off for a more public NHS in England might be Scottish independence, but some feel the most pertinent moral argument is here that Westminster should not be governing over Scotland anyway if has few or no MPs.
Unbelievably, two democratic deficits have collided: one to do with the NHS and one to do with Scotland.

Party politics may be failing the NHS and care, but democracy isn’t
There is a sense of the ‘unfinished revolution’ as Philip Gould might have put it. UK politics perhaps feels like ‘work in progress’, or ‘just in time’, to borrow management speak.
The pre-match build up has been quite exhilarating. The seleb nature of politics is exemplified that Alex Salmond is still box office despite Nicola Sturgeon being the head of the party. And that Ed Miliband wants a knock-out with David Cameron, even though David Cameron doesn’t wish to attend the weigh-in.
I have for ages railed against the consumerist nature of politics, thinking that you have to road test and focus group your offerings. It is often joked that John Major MP’s government was the first New Labour government, but here we see the seeds of a policy which has become quite controversial – the private finance initiative.
Whilst ‘PFI’ has undoubtedly helped to rebuild a physical infrastructure for the NHS which is to be welcomed, there’s no doubt that it is an accounting trick of sorts, and has a ‘buy now pay later’ feel for it.
Previous Labour and Tory governments have not been good at managing the negotiations for PFI, and it is the taxpayers who ultimately lose out.
Anyway, the lack of pay increases in the nursing profession nor the number of acute NHS Trusts in deficit did not warrant a mention in George ‘You’ve never had it so good’ budget speech.
Who really runs Britain? This is a question that Robert Peston, son of a Labour peer, asked not so long ago. The problem is that, as far as the NHS is concerned, we are not being given much of a choice.
We’re being given no choice about the implementation of personal budgets. We’re being given no choice about PFI loan repayments. We’re being given no choice about the £20 billion ‘efficiency savings’ aka cuts.
The ultimate in exercise of democracy is supposed to be your vote. The late Tony Benn made a great play of the fact all of us could exercise a democratic vote, even if we did not have sufficient money to buy influence as in corporate lobbying.
But this vote is only as good as the choice on offer. We are presently not being given a choice as to whether we would pay more taxes to see social services not cut to the bone.
Many of us feel that we were not given much choice about the eye watering contracts which were shunted across to the private sector in the lifetime of previous governments.
There remains a dearth of skilled opinions and ‘thinking’ about the NHS aside from some exceptional independent people. There remains no skilled socialist health association apart from a small body of middle-old age people who do not generate policy in a democratic manner and who have little influence on any of the political parties.
Only platforms, it seems such as ‘Our NHS’, are able to put their neck over the parapet, but I feel this is not enough. I feel some sympathy for the National Health Action Party, which is able to take the bull by the horns; but even they will be the first to admit they will have to fight hard to get elected representatives in parliament.
I would like to be able to support something such as the NHS Reinstatement Bill, for example I would love to see somebody responsible for the running of the NHS, but my humblest submission is that another top down reorganisation of the NHS would be traumatic.
But we would be deluded to expect that another reorganisation of some sort is unlikely. The change required in combining health and care, even if it is cost neutral somehow, cannot be labelled as anything other than ‘radical’.
Rather like being a consumer for music, however, I prefer making up my own soundtrack on Spotify, rather than buying whole albums. However, there aren’t any tracks from UKIP which I am interested in.
Party politics, I believe, are failing the majority of people in Britain. There seems to be little link between what people want and what people actually get, irrespective of ‘broken promises’, and this appears to be especially the case now for the NHS and care.
For example, the Liberal Democrats are now unashamedly campaigning on mental health when their cuts, albeit implemented locally, have seen social care truly on its knees.
The ultimate farce will be when a sizeable number of SNP MPs are weighed up against Labour losses, to see whether the Tories, UKIP, the Democratic Unionist Party, Greens and National Health Action Party can provide a ‘government of minorities’ to form a government.
It may not even be a coalition, nor ‘supply and confidence’ – it might simply be vote by vote.
And are we expected to run the NHS on the basis of this?

The Liberal Democrats and UKIP should pledge to repeal the Health and Social Care Act
Ed Miliband, Andy Burnham, and the whole of Labour have pledged robustly that a direction to repeal the Health and Social Care Act (2012) will be made in the first Queen’s Speech of a new Labour Government.
It is said that David Cameron and Nigel Farage are to be issued with a joint challenge to declare that they will rule out any attempt to repeal the ban on foxhunting if they form a pact in the event of a hung parliament.
Evan Harris on 6 March 2012 identified the impact that the Lansley legislation would have to turbo-boost marketisation and privatisation of the NHS.
He warned Liberal Democrat colleagues not to touch it with a bargepole:
“It has no friends among even the non-party-political royal colleges, and has no mandate in those areas where it goes beyond the coalition agreement. The political impact will be to retoxify the Tory brand – which they are welcome to do, of course –, but also, by association, to damage the Lib Dems.”
The assurances given by Lord Clement Jones have turned out to be hollow:
“In putting down amendments, we have no hostility to competition as such, merely a desire to make use of the opportunities that the TFEU and European competition law offer member states to avoid the NHS being treated like a utility, such as gas and electricity.
Under the EU treaties, Article 106 of the Treaty on the Functioning of the European Union states:
“Undertakings entrusted with the operation of services of general economic interest … shall be subject to the rules contained in this Treaty, in particular to the rules on competition, insofar as the application of such rules does not obstruct the performance, in law or in fact, of the particular tasks assigned to them”.
Member states have certain discretion as to which services are services of general economic interest. By ensuring healthcare services for the purposes of the NHS are services of general economic interest and that the “task” of co-operation between services is “assigned” to the healthcare providers, it should be possible to provide some protection from less desirable aspects of competition law.”
This year saw Cambridgeshire and Peterborough NHS Foundation Trust awarding G4S Integrated Services a £3.9 million contract to provide domestic cleaning, portering and catering support across its property portfolio. The three year agreement, with the option to extend for a further year, will see G4S initially delivering services to 34 sites across Peterborough and Cambridgeshire, with further locations likely to be added in the future. Cleaning will be provided across the contract, with additional portering services and catering support at some specific sites.
Privatisation does not require a complicated definition. It’s simply the transfer of public sector resources into the private sector. Even the late Sir Keith Joseph, widely thought to be “brilliant” by the late Margaret Thatcher herself, and who was thought to be the principal “architect” of Thatcherism, ended up trying to keep afloat businesses in the public sector rather than privatise them. This was during his time as Secretary of State for Trade and Industry.
There is generally a feeling that the Coalition government, a joint enterprise between the Conservatives and the Liberal Democrats, went much further in privatising the NHS than the Thatcher government even dared to. And the worst aspect of this was there was absolutely no inkling that this would happen. There was no mention of this even in the Coalition Agreement of 2010.
There is no official policy by UKIP on the NHS yet.
This is absolutely staggering. The late Tony Benn used himself to warn people against voting for people who are ‘false prophets’. UKIP seem alarmingly reluctant to acknowledge the number of people from black asian minority ethic background who actually work for the NHS and bring value to it everyday.
It is now felt that there is quite a high chance of a ‘hung parliament’, although Labour activists are desperate to fight for a Labour government at Westminster with a healthy majority. It appears that the mainstream right-wing press have given up the ghost, in the form of David Cameron.
It is curious why the Conservative Party haven’t ditched their leader, like they did famously in 2010, but the most parsimonious explanation is that it would make sense to find a new leader after the expected catastrophe of the 2015 election. Ditching Cameron now might mean that they would have to ditch a new leader further in 2015. Besides, the Conservatives and Liberal Democrats have become a tried and tested product as far as the City are concerned.
The current Government, and people who sail with her such as BoJo, have fiercely defending the City’s interests in Europe as far as banker bonuses are concerned. They have resisted the ‘Mansion Tax’, which is widely thought to be introduced by Ed Balls as Chancellor in the first Budget of a Labour Government, as a windfall tax to produce a cash injection into the NHS. Furthermore, the City still has lucrative contracts in the form of the private finance initiative which have yet to be renegotiated properly from this Government; and also they have been very successful in promoting social impact bonds, the PFI equivalent for social enterprises, with the current Government which has used mutualisation to Trojan horse rent seeking in response to Mid Staffs.
Certain dividing lines have now got to be laid for the sake of the public good.
I feel that it is essential that David Cameron, Nick Clegg, and Nigel Farage are to be issued with a joint challenge to declare that they will rule out any attempt to resist the repeal of the Health and Social Care Act (2012).
Nigel Farage, for all his faux socialist credentials, seems unseen to resist formally the privatisation of the NHS; in fact his henchmen over the years have prided themselves on the ‘efficiency’ of the private sector, despite the growing allegations of fraud and inefficiency from the outsourcing companies used by the current government to deliver the smaller State.
Nick Clegg not only has a PR problem; he has a major issue with the content of what the Liberal Democrats stand for. It is widely known that there is discontent about his party’s ‘differentiation’ policy, which has seen the Tories and the Liberal Democrats telling the voters why each other party is clearly unfit for government. The charge sheet against the Liberal Democrats, including a weak economy (not enough till receipts from income tax to fund public services), demolition of legal aid, privatisation of NHS, misery for a mass of disabled citizens through botched welfare reforms, is substantial.
As a minority party, the Liberal Democrats would be asked to repeal the Health and Social Care Act (2012) which is possible but simply weird. It is clear that the Liberal Democrats, Conservatives and UKIP are clearly capable of running the NHS into the ground.
A lot of energy was put into fighting the Liberal Democrats on the toxic firestorm hospital closure clause, clause 119, which the Liberal Democrats were instrumental in protecting. Norman Lamb, for all his soothing words, has been the Minister of State in office while social care has imploded; the social care budget has not been ring fenced, coincidentally, since 2010.
There was a popular joke on Twitter this year that turkeys joked, “It’s like humans voting for UKIP”.
David Cameron, if he is still leader in 2015, or whoever is in charge of that toxic brand, will clearly be in no position to repeal the Health and Social Care Act (2012). The least worst option is that the Liberal Democrats and UKIP should pledge not to resist the repeal of the Health and Social Care Act (“Act”), but the hope is that a strong Labour government will have renewed vigour in assessing the political weather. Even better, they should pledge to repeal the Act.
That is, the component of the private sector in the mixed health and care economy has gone way too far. The health and care sectors should never be run anywhere for the benefit for shareholders offering care in 15 minute slots or below the minimum wage. The health and care sectors should not be so fragmented as they are now. People should be collaborating with each other to offer excellent clinical care, not competing with each other.
The vote is the most critical weapon of influence any of us has. Even more than ever, it is vital that it is used wisely.
