Home » Posts tagged 'Mid Staffs'
Tag Archives: Mid Staffs

How the acute medical take can generate into chaos for persons with dementia
The independent Future Hospital Commission was established by the Royal College of Physicians in March 2012 to find solutions to the current challenges facing the NHS – a rising number of acute admissions, the increasing number of patients who are frail, old, or who have dementia, patients with increasingly complex illnesses, systemic failures of care, poor patient experience, and a medical workforce crisis. The NHS leaflet on the 6Cs here. Even for the official 6Cs, powerful forces are at play in undermining the acute medical take. The ‘Good 6Cs’ can find themselves competing with the ‘Bad 6Cs’, which can determine the outcome of the acute general medical take. One year on after the publication of the last Francis Report on Mid Staffs, there appears to be common themes in what can go wrong.

1. Care
Care is described as a “core business”, perceiving each event with a patient as a transaction which is a potentially billable event.” Caring defines us and our work” indeed is true; as it defines to some extent how people get paid. Unfortunately, the way in which care goes wrong is pretty consistent in the narrative. For example, nurses may be too ‘posh’ to care. In this version, nurses who are too academic are incapable of caring for which there is little published evidence. The other more likely version is that junior nurses are “too rushed to care”. This is understandable, in that if there are ten people still waiting to be clerked in, it can be hard for all professionals to focus on taking a proper history and examination without cutting corners, for examination in completing an accurate neurological examination of the cranial nerves. However, the emergency room often cultivates a feeling of a conveyor belt, with a feeling of “Now serving number 5″. A patient experience is not going to be great if the doctor, nurse or AHP appears rushed in clerking in a patient. The patient feels more like they are in a sheep dip as “continuity of care” between different medical teams suffers.
2. Compassion
“Compassion is how care is given through relationships based on empathy, respect and dignity.” Again there is some irony in the same management consultants outfit recommending compassion by healthcare professionals, when the same professionals have recommended ‘efficiency savings’. Compassion in the NHS can of course be extremely difficult to deliver from the nurses remaining after there have been staff cuts, and the remaining nurses are having to work twice as fast ‘to beat the clock’, or a target such a “four hour target”.
3. Competence
“Competence means all those in caring roles must have the ability to understand an individual’s health and social needs.” This is of course is motherhood and apple pie stuff. The problem comes if the NHS ‘productivity’ is improved with lateral swapping of job rôles: that some functions are downgraded to other staff. Health care assistants might find themselves doing certain tasks which had been reserved for them. If there’s mission creep, the situation results of receptionists triaging a patient, rather a physician’s assistant doing a venflon. Competence of course cannot be delivered by untrained staff delivering an algorithm, as has been alleged for services such as NHS 111.
4. Communication
Communication is central to successful caring relationships and to effective team working. The overall “no decision about me without me” mantra of course has been made a mockery of, with unilateral variation of nursing and medical contracts (with adjustments to terms and conditions, and pay, of staff by NHS managers without any dialogue.) If you don’t communicate any errors in clinical care to the patient (reflected in the ‘lack of candour’ below), the patient and relatives are bound to leave with an unduly glossy version of events of the acute medical assessment. This can of course bias the outcome in the ‘Friends and Family Test’.
5. Courage
“Courage enables us to do the right thing for the people we care for, to speak up when we have concerns.” Take the situation where your Master (senior nurse) is wishing to implement a target, but you’re the one rushed off your feet with missing drug charts, no investigations ordered, no management plan formed as the patient was shunted out of A&E before the 4 hour bell started ringing? Are you therefore going to be able to speak out safely against your Master when your Master is the one who determines your promotion? If you’re made of strong stuff, and completely fastidious about patient safety, you might decide ‘enough is enough’ by whistleblowing. But the evidence is that whistleblowers still ultimately get ‘punished’ in some form or others.
6. Commitment
“A commitment to our patients and populations should be the cornerstone of what we doctors, nurses, and allied healthcare professions do, especially in the “experience of the patients.””. Of course, if you get a situation where junior staff are so demoralised, by media witch hunting, it could be that people are indeed driven out of the NHS for working for other providers, or even other countries. A commitment to the public sector ethos may have little truck if you’ve got more interest in ‘interoperability’, or ‘switching’, which are of course the buzzwords of introducing ‘competition’ into healthcare systems.
There can be some downright ‘yang Cs’ epitomising danger for the acute medical take and hospital.
7. Chaos
If for the sake of hitting a target, drug charts aren’t written up, investigations not ordered, an inaccurate management plan produced, that is no victory at all. This can only lead to chaos later down the line for nursing teams for ‘receiving wards’.
8. Crisis
When things get out of hand, some of the more hyperbolic allegations might conceivably happen. With people lose the plot, they are capable of anything. And if the system is too lean, and there’s a road traffic accident or other emergency, or there’s an outbreak of rotavirus amongst staff, there may be insufficient slack in the system to cope.
9. Cuts
Whilst patient campaigners have been right to emphasise that it’s more of a case of safe staffing rather than a magical minimum number, there’s clearly a number of trained staff on any shift below which it’s clearly unsafe for the nurses to deliver good nursing care. Cuts in real terms, even if that’s the same budget (just) for an increased numbers in an elderly population, can of course be a great motivator for producing unstable staffing, as the Keogh 14 demonstrated. That might be especially tempting if ‘financially strained’ NHS FTs are trying to balance their budgets in light of PFI loan repayments.
10. Collusion
This can affect a nurse’s ability to communicate problems with courage, if senior nurses are colluding with certain consultants in meeting targets. This means that medical consultants who are recipients of the non-existent drug charts, non-existent management plans, or non-existent investigation orders can probably take one or two weeks to ‘catch up’, but the ‘length of stay’ gets extended. Frontline staff can take the risks. But senior nurses can collude with the management to deliver ‘efficiency savings’ and promote themselves. That’s not fair is it?
11. Lack of Candour
This target-driven culture of the NHS, and excessive marketing of how wonderful things are, must stop. A lack of honest communication with the patient through candour can lead to patients never knowing when things go wrong. This is a cultural issue, and it may be legislated upon at some point in the future. But without this cultural willingness by clinical staff to tell patients when things have unnecessarily got delayed through the missing drug charts etc., they will only get to know of things going badly wrong.
12. Complaints
If things go badly wrong, they may generate complaints. These complaints may as such not matter if the system completely ignores complaints. For example, there has been only one successful judicial review against the PHSO since 1967. The recent review of the complaints process for NHS England has revealed how faulty the process is. There has been criticism of the clinical regulators in their ability to enforce patient safety too, particularly in light of Mid Staffs.
As you can see, the system is delicately balanced. If transparency is the best disinfectant, it’s time to reveal the other six Cs for a start? The most important thing of course may be Culture, the 13th C.
Being number 13, it may be worse than unlucky for some.
The 11 Cs – can we avoid another Mid Staffs one year after the last Francis Report?
This is the NHS leaflet on the 6Cs here.
Even for the official 6Cs, powerful forces are at play in undermining the acute medical take.
The 6Cs still, though, potentially form the ‘greater good'; that of the ‘ying Cs’.
But it’s how they engage with the 5 other ‘yang Cs’ which will determine whether there’s another Mid Staffs, more than one year on from the last Francis Report.
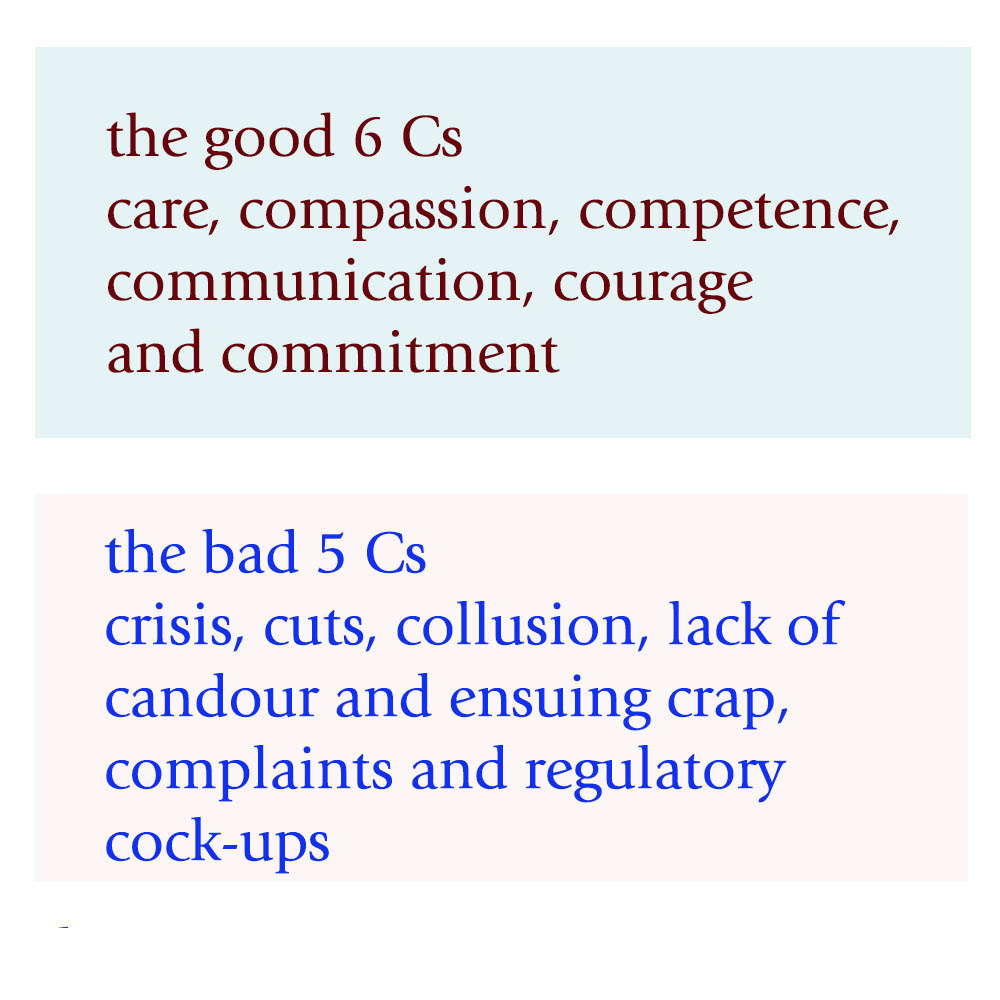
1. Care
Care is described as a “core business”, perceiving each event with a patient as a transaction which is a potentially billable event.” Caring defines us and our work” indeed is true; as it defines to some extent how people get paid. Unfortunately, the way in which care goes wrong is pretty consistent in the narrative. For example, nurses may be too ‘posh’ to care. In this version, nurses who are too academic are incapable of caring for which there is little published evidence. The other more likely version is that junior nurses are “too rushed to care”. This is understandable, in that if there are ten people still waiting to be clerked in, it can be hard for all professionals to focus on taking a proper history and examination without cutting corners, for examination in completing an accurate neurological examination of the cranial nerves. However, the emergency room often cultivates a feeling of a conveyor belt, with a feeling of “Now serving number 5″. A patient experience is not going to be great if the doctor, nurse or AHP appears rushed in clerking in a patient. The patient feels more like they are in a sheep dip as “continuity of care” between different medical teams suffers.
2. Compassion
“Compassion is how care is given through relationships based on empathy, respect and dignity.” Again there is some irony in the same management consultants outfit recommending compassion by healthcare professionals, when the same professionals have recommended ‘efficiency savings’. Compassion in the NHS can of course be extremely difficult to deliver from the nurses remaining after there have been staff cuts, and the remaining nurses are having to work twice as fast ‘to beat the clock’, or a target such a “four hour target”.
3. Competence
“Competence means all those in caring roles must have the ability to understand an individual’s health and social needs.” This is of course is motherhood and apple pie stuff. The problem comes if the NHS ‘productivity’ is improved with lateral swapping of job rôles: that some functions are downgraded to other staff. Health care assistants might find themselves doing certain tasks which had been reserved for them. If there’s mission creep, the situation results of receptionists triaging a patient, rather a physician’s assistant doing a venflon. Competence of course cannot be delivered by untrained staff delivering an algorithm, as has been alleged for services such as NHS 111.
4. Communication
Communication is central to successful caring relationships and to effective team working. The overall “no decision about me without me” mantra of course has been made a mockery of, with unilateral variation of nursing and medical contracts (with adjustments to terms and conditions, and pay, of staff by NHS managers without any dialogue.) If you don’t communicate any errors in clinical care to the patient (reflected in the ‘lack of candour’ below), the patient and relatives are bound to leave with an unduly glossy version of events of the acute medical assessment. This can of course bias the outcome in the ‘Friends and Family Test’.
5. Courage
“Courage enables us to do the right thing for the people we care for, to speak up when we have concerns.” Take the situation where your Master (senior nurse) is wishing to implement a target, but you’re the one rushed off your feet with missing drug charts, no investigations ordered, no management plan formed as the patient was shunted out of A&E before the 4 hour bell started ringing? Are you therefore going to be able to speak out safely against your Master when your Master is the one who determines your promotion? If you’re made of strong stuff, and completely fastidious about patient safety, you might decide ‘enough is enough’ by whistleblowing. But the evidence is that whistleblowers still ultimately get ‘punished’ in some form or others.
6. Commitment
“A commitment to our patients and populations should be the cornerstone of what we doctors, nurses, and allied healthcare professions do, especially in the “experience of the patients.””. Of course, if you get a situation where junior staff are so demoralised, by media witch hunting, it could be that people are indeed driven out of the NHS for working for other providers, or even other countries. A commitment to the public sector ethos may have little truck if you’ve got more interest in ‘interoperability’, or ‘switching’, which are of course the buzzwords of introducing ‘competition’ into healthcare systems.
There can be some downright ‘yang Cs’ epitomising danger for the acute medical take and hospital.
7. Crisis
When things get out of hand, some of the more hyperbolic allegations might conceivably happen. With people lose the plot, they are capable of anything. And if the system is too lean, and there’s a road traffic accident or other emergency, or there’s an outbreak of rotavirus amongst staff, there may be insufficient slack in the system to cope.
8. Cuts
Whilst patient campaigners have been right to emphasise that it’s more of a case of safe staffing rather than a magical minimum number, there’s clearly a number of trained staff on any shift below which it’s clearly unsafe for the nurses to deliver good nursing care. Cuts in real terms, even if that’s the same budget (just) for an increased numbers in an elderly population, can of course be a great motivator for producing unstable staffing, as the Keogh 14 demonstrated. That might be especially tempting if ‘financially strained’ NHS FTs are trying to balance their budgets in light of PFI loan repayments.
9. Collusion
This can affect a nurse’s ability to communicate problems with courage, if senior nurses are colluding with certain consultants in meeting targets. This means that medical consultants who are recipient of the non-existent drug charts, non-existent management plans, or non-existent investigation orders can probably take one or two weeks to ‘catch up’, but the ‘length of stay’ gets extended. Frontline staff might take the risks. But senior nurses might collude with the management to deliver ‘efficiency savings’ and promote themselves. That’s not fair is it?
10. Lack of Candour and Ensuing Crap
This target-driven culture of the NHS, and excessive marketing of how wonderful things are, must stop. A lack of honest communication with the patient through candour can lead to patients never knowing when things go wrong. This is a cultural issue, and it may be legislated upon at some point in the future. But without this cultural willingness by clinical staff to tell patients when things have unnecessarily got delayed through the missing drug charts etc., they will only get to know of things going badly wrong.
11. Complaints and Regulatory Cock-ups.
If things go badly wrong, they may generate complaints. These complaints may as such not matter if the system completely ignores complaints. For example, there has been only one successful judicial review against the PHSO since 1967. The recent review of the complaints process for NHS England has revealed how faulty the process is. There has been criticism of the clinical regulators in their ability to enforce patient safety too, particularly in light of Mid Staffs.
As you can see, the system is delicately balanced.
If transparency is the best disinfectant, it’s time to reveal the other five Cs for a start?
The most important thing of course may be Culture, the 12th C. If the culture is toxic, as happened in Mid Staffs, it may be hard to analyse the problem in terms of its root causes.
Why yesterday’s Care Bill debate matters to tomorrow’s decision about Mid Staffs

s. 118 is the contentious clause of the Care Bill.
An important question is of course whether the Labour Party, if they were to come into government in 2015, would seek to repeal this clause if enacted. The likelihood is yes. What to do about reconfigurations and reconsultations for NHS entities which are not clinically or financially viable is a practical problem facing all political parties. A practical difficulty which will be faced by all people involved in the TSA process between now and 2015 is that it is relatively unclear what Labour’s exact legislative stance on the future structural reorganisation of the NHS is, save for, for example, having strongly opposed the recent decisions over Lewisham (prior to the High Court and Court of Appeal.)
Draft recommendations for the future of Mid Staffordshire NHS Foundation Trust were published on Wednesday 31 July 2013 by the Joint Trust Special Administrators. Tomorrow will see the publication of the final proposals (and it is widely expected that interested parties will be informed about the outcome of the consultation process this evening.) Producing a long-term outlook for key services, including paediatrics, ICU and maternity, is going to have been a complicated decision-making process for all involved.
Stephen Dorrell MP, Chairman of the influential Health Select Committee, pointed out in the Care Bill debate yesterday afternoon that the competition debate about the NHS is usually presented as ‘binary’, and this is to some extent reflected in John Appleby’s famous piece for the King’s Fund on how there are both advantages and disadvantages of competition. What people agree on more or less is the need to move beyond fragmented care to an integrated approach in which patients receive high-quality co-ordinated services. The idea is that competition itself need not be a barrier to collaboration provided that the risks of the wrong kind of competition are addressed. This will involve considerable legislative manoeuvring in the future. In securing a more integrated approach, reflected also in Labour’s “whole person care” ultimately, commissioners are expected not be able to fund ever-increasing levels of hospital activity.
Trying to keep frail older people away from hospital, and to allow such individuals to live independently, has become an important policy goal. Trying to keep people in hospital for shorter stays is another key aspiration. Matching services to actual demand is a worthy aspect of any reconfiguration (and also providing the full range of relatively unprofitable emergency services locally.) All of these factors become especially important with the increasing numbers of older people in the population, some of whom have multiple and complex chronic conditions that require the expertise of GPs and a range of specialists and their team. “Integrated delivery systems” in other countries have previously embraced a model of multi-specialty medical practice in which GPs work alongside specialists, often in the same facilities. It is possible that this sort of approach will become more popular in future here in the UK. It is relevant to the NHS here, because of the need for specialists and GPs to work together much more closely to help patients remain independent for as long as possible and to reduce avoidable hospital admissions.
A frequent criticism has been that ‘competition lawyers should not be blocking decisions which are in the patients’ interest‘. The problem with this argument is that simple mergers may not actually be in the patients’ interest. While mergers to create organisations that take full responsibility for commissioning and providing services for the populations they serve have been pursued in Scotland and Wales, the benefits of this kind of organisational integration remain a matter of dispute.
It’s been mooted that stroke care in London and Manchester has been improved by planning the provision of these services across networks linking hospitals. They are reported ass “success stories”. For example, Manchester uses an integrated hub-and-spoke model that provides one comprehensive, two primary and six district stroke centres. Results include increasing the number of eligible patients receiving thrombolysis within the metropolitan area from 10 to 69 between 2006 and 2009.
The decision over the future of services in Staffordshire allows to put to the test the idea that health care teams can develop a relationship over time with a ‘registered’ population or local community. They can therefore target individuals who would most benefit from a more co-ordinated approach to the management of their care. For example, a “frail elderly assessment service” might well to act as a one-stop assessment for older people and take referrals from a wide range of sources to better meet the needs of the frail elderly. The ‘new look’ services in Mid Staffs could become a ‘test bed’ for seeing how information technology (IT) could be best used. IT could, in this way, support the delivery of integrated care, especially via the electronic medical record and the use of clinical decision support systems, and through the ability to identify and target ‘at risk’ patients
A clinician–management partnership that links the clinical skills of health care professionals with the organisational skills of executives, sometimes bringing together the skills of purchasers and providers ‘under one roof’, might become more likely in future. This might be particularly important for ensuring that patient safety targets are actually met in clinical governance, and corrective action can be initiated if at any stage deemed necessary. The engagement of actual patients would be very much in keeping with Berwick’s open organisational learning culture. Of course the Care Bill cannot set top-down commands for organisational culture and leadership. It was interesting though that these were discussed in yesterday’s debate. Effective leadership at all levels will be necessary to focus on continuous quality improvement. A collaborative culture will be needed which emphasises team working and the delivery of highly co-ordinated and patient-centred care.
So the future of Mid Staffs clearly represents an opportunity for the NHS, not a threat; it would be helpful if politicians of all sides could rise to the occasion with maturity and goodwill.
Fears and smears – wilful inattention from healthcare journalists?
In an article today in the Independent, subtitled “Fears and smears”, Ed Miliband MP writes:
“They want to distract attention from the issues that matter. With the support of a determined section of the press, they have decided that mudslinging matters more than the futures of millions of families across this country.”
Discussion of the NHS is an incredibly sensitive area and yet it has been done incredibly badly by many journalists and politicians.
Mid Staffs was an unacceptable disaster. It was THE low point in the NHS.
Relatives of loved ones have shown incredible bravery and resilience in the face of an unbelievably tragic intolerable event.
For many, the issues in Mid Staffs appeared to be simply brushed under the carpet for political purposes, and real patients and relatives suffered.
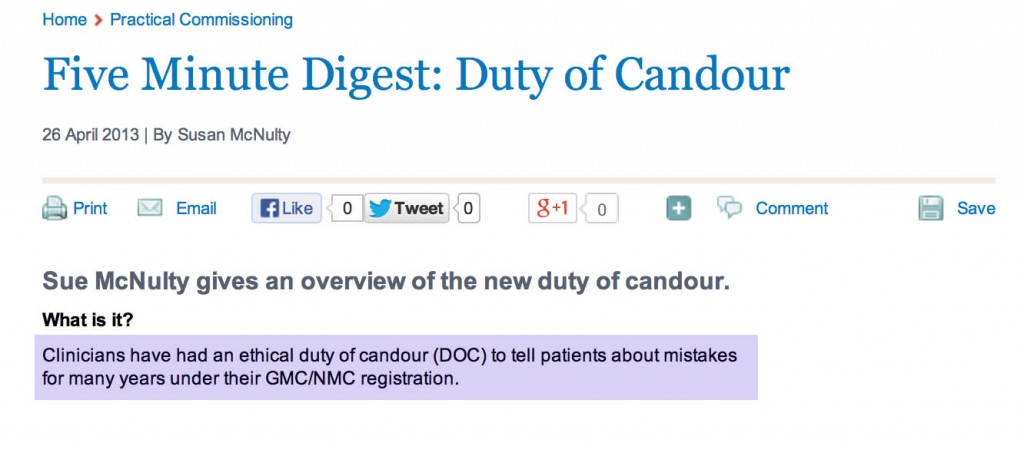
The claim over professional codes and a duty of candour
On Thursday, Jeremy Hunt gave an answer on Mid Staffs on the BBC programme ‘Question Time‘. Regarding making it easier for people to speak out, “people are going to be given protection in their professional codes which have happened before.”
Mr Hunt is therefore speaking as if this has sprung up from nowhere.
Not true, even from the briefest scan of ‘Five Minute Digest – Duty of Candour’ in ‘Pulse Today‘:
The claim that Burnham opposed an inquiry
There are two inquiries – when you read the rest of this article, be mindful that
- November 2009 – Robert Francis QC begins hearing evidence in private as part of his independent inquiry
- February 2010 – Robert Francis QC publishes his independent inquiry report into the poor care at Mid Staffordshire Foundation Trust
- May 2010 – Change of government and Health Secretary
- November 2010 – The public inquiry begins to hear evidence
- December 2011 – The public inquiry finishes hearing evidence after more than 12 months
In Question Time last week, regarding Mid Staffs, Mr Hunt explained, “Your party opposed a public inquiry. Andy Burnham decided to oppose a public inquiry.”
The Executive Summary of the Report of the public inquiry, published in 2013, is here.
The way the original private inquiry was set up by Andy Burnham MP, the then Secretary of State for Health, is described in the 2013 Francis report as follows.

A new Government was elected in the UK in May 2010. The way in which Andrew Lansley MP, the then Secretary of State for Health, set up a public inquiry is provided in the 2013 Francis report as follows.

This actually came as no surprise, as Andy Burnham MP had already stated that the second Inquiry would be held in public, as cited here.
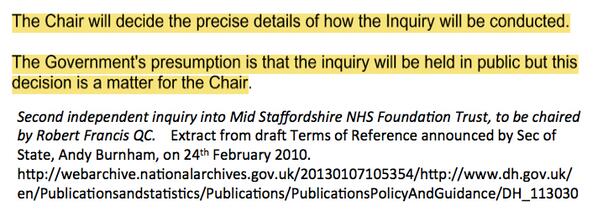
Francis himself did not want the first inquiry to sit in public for the first time, and is even reported as being satisfied with the arrangements, as cited here.
The problem here is in the media at large the genuine message that Burnham set up the first inquiry in 2009 ‘to give patients a voice’ has been swamped by the toxic meme from some, and they know who they are, that ‘Burnham blocked an inquiry’.
The claim that Burnham never apologised
Another blatant classic lie is that Burnham has never ‘apologised for Mid Staffs’.
This is addressed too, as cited here.
The claim that Burnham resisted an inquiry under the Inquiries Act
Burnham obviously did not have any powers as Secretary of State for Health after the General Election of May 2010. The decision for the second public inquiry comes after that date.
It has been claimed furthermore that Andy Burnham MP resisted his inquiry to take place under the auspices of the Inquiries Act, but Burnham did actually leave it all times to be directed by Francis, the Chair of the Inquiry.
This legally is a somewhat obtuse claim, as it was a Labour government which enacted the Inquiries Act in 2005 in the first place.
In Appendix 1 of the bundle of documents entitled “Independent Inquiry into care provided by Mid Staffordshire NHS Foundation Trust January 2005-March 2009 Volume 1″ Appendix 2, Andy Burnham MP as the then Secretary of State for Health in his Written Ministerial statement (21 July 2009) first cites his perceived need to set up an inquiry “swift so as not to unduly distract the new management and staff at the hospital from improving services for today”, but that he has the power to convert the Inquiry to one under the Inquiries Act should the Chair of the Inquiry (Robert Francis QC) should demand it.
This exact text of the statement is indeed evidenced in Hansard, for 21 July 2009 Column WS188 as per here.
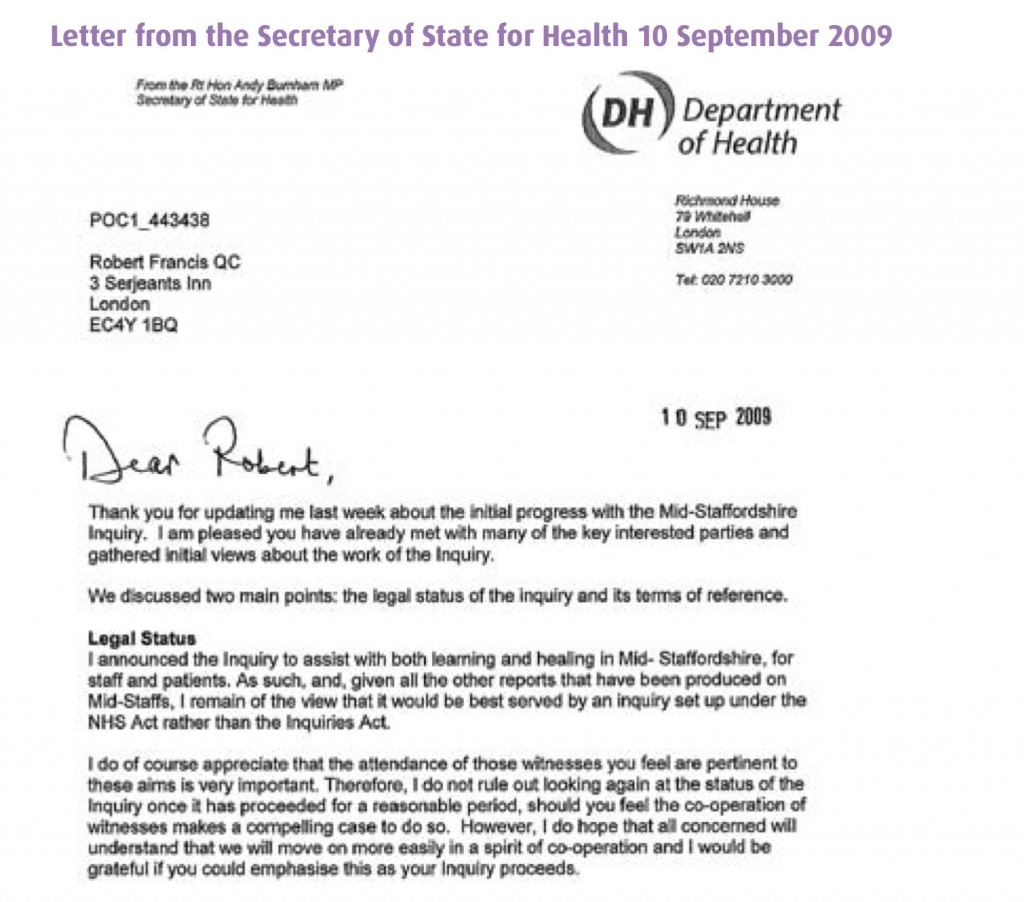
In Appendix 2 of the bundle of documents entitled “Independent Inquiry into care provided by Mid Staffordshire NHS Foundation Trust January 2005-March 2009 Volume 1″ Appendix 2, Andy Burnham MP as the then Secretary of State for Health repeats (10 September 2009) his willingness for his inquiry to be set up under the Inquiries Act not the NHS Act.
This is the evidence that Burnham gave to Francis 2 on 6 Sep 2011, page 178:
Indeed, parsimoniously, the option of ‘converting another form of inquiry’ into an Inquiry as under the Inquiries Act at any time is clearly good application of the law, under section 15 Inquiries Act (2005).
The claim that ‘wilful neglect’ legislation is a fundamental new shift in the law
The Berwick Report itself was all about constructive organisational learning, and only introducing a statutory crime of ‘wilful neglect’ for the most extreme cases.
Some vocal campaigners in Mid Staffs clearly desire targeted retributive justice, but the media thus far have refused to cover why the law of ‘wilful neglect’ in the form of section 44 Mental Capacity Act (2005) has failed to see a flurry of successful criminal prosecutions in Mid Staffs. We have instead discusssed it here. ‘Wilful neglect’ is NOT a fundamental new shift in the law, unless it can now be applied to adults with full capacity.
The claim that ‘there was a culture of cruelty in the NHS and no-one noticed”
Staff in various NHS Trusts have voiced loudly their resentment as being targeted in some sort of ‘hate campaign’.
Jeremy Hunt last week specifically referred to how a culture of cruelty ‘became normal in our NHS’, not in any particular Trust.

as cited in Hansard 19 November 2013.
Summary
The problem in this imbalance of irresponsible reporting is that it creates a culture of fear in NHS nurses, even in those ‘who have nothing to hide’. It is not a mature discussion of the technical problems in the law. It is instead ‘red meat’, ‘dog whistle’ politics of the worst kind, of a particular political inclination. As a result of memes about the Inquiry, candour and putting clinical staff in the clink, an irresponsible media has diverted attention from important issues.
By allowing copious air time for lies, the important discussion of why A&E is experiencing difficulties, a lack of a stated minimum level of safe staffing, why social care cuts have been so dangerous, or why NHS 111 has failed so dramatically, have not been explored in any level of acceptable detail.
Sadiq Khan MP tried valiantly to bring up how staffing levels had been so low, and ‘without the doctors and nurses, it’s all talk and no action.” But the stench of the narrative above diverted him from discussing the critical issues as much as he would have liked, although he did get in an official statistic about a cut in nursing numbers.
Real staff are none-the-wiser. Patient campaigners are led down the river without a paddle. Voters are completely bamboozled.

This is an unholy disgusting mess from those responsible. Call it wilful inattention.
Thanks to the public tweets of @gabrielscally for many of the extracts cited in the article.
What precisely is Jeremy Hunt legislating for in ‘wilful neglect’ which would have prevented a Mid Staffs?

The Leveson Inquiry had to work out why the culture of journalism had gone so badly wrong in places, even with enforceable criminal law, such as the interception of communications or tresspass against the person.
Hunt will be keen to provide enforceable ‘end points’ of the Francis Inquiry. But again, there is an issue here of what went so badly wrong in culture, where there were theoretically enforceable aspects from regulators such as the GMC or NMC.
There has been an intense debate about how many people may have died as a result of poor care over the 50 months between January 2005 and March 2009 at Stafford hospital, a small district general hospital in Staffordshire.
Clearly Hunt feels that there was a ‘culture of cruelty’ in the NHS, as he said yesterday (report in Hansard):
![]()
The report published on 6 February 2013 of the public inquiry chaired by Robert Francis QC was the fifth official report into the scandal since 2009, and Francis’s second into the hospital’s failings.
According to s.1(1A) Medical Act 1983, referring to a body corporate known as the “General Medical Council” (GMC)
The main objective of the General Council in exercising their functions is to protect, promote and maintain the health and safety of the public.
The difficulties that the GMC has had in successfully prosecuting Doctors over ‘the Mid Staffs scandal’ are comprehensively discussed elsewhere, and are therefore not the focus of this article.
Similar dead-ends have been experienced by the NMC (for example here), and are not the focus of this article either.
It was reported recently that Doctors and nurses found guilty of “wilful neglect” of patients could face jail as new legislation from the Government.
Wilful neglect will be made a criminal offence in England and Wales under NHS changes as a response to the Mid Staffordshire and other care scandals. The offence is modelled on one punishable by up to five years in prison under the Mental Capacity Act. So how does Jeremy Hunt envisage what this law will do?
Jeremy Paxman presented his interview with Jeremy Hunt, the Secretary of State for Health, last night on “Newsnight”. Paxman asked Hunt directly to give an example. At first, he spoke around the subject, talking about the need for criminal sanctions “for the most extreme cases”.
Hunt finally provided this answer:
Well I think an example might be someone who was responsible for caring for a dementia patient who didn’t give them [sic] food when they needed it and when they knew they needed food. That’s the kind of them I’m thinking about. It’s for people who deliberately neglect people. It’s a very small minority of people and they should feel the full force of the law.
The phrase “when they knew they needed food” is highly significant.
At no point did Hunt specify this was an older patient with dementia.
Since 1 April 2007, vulnerable people have been afforded an increased protection by the Mental Capacity Act 2005. The Mental Capacity Act (2005) created the criminal offences of ill-treatment or wilful neglect under Section 44 based on existing principles. This offence could be distinguished from the one contained in section 127 of the Mental Health Act 1983 which creates an offence in relation to staff employed in hospitals or mental nursing homes where there is ill-treatment or wilful neglect.
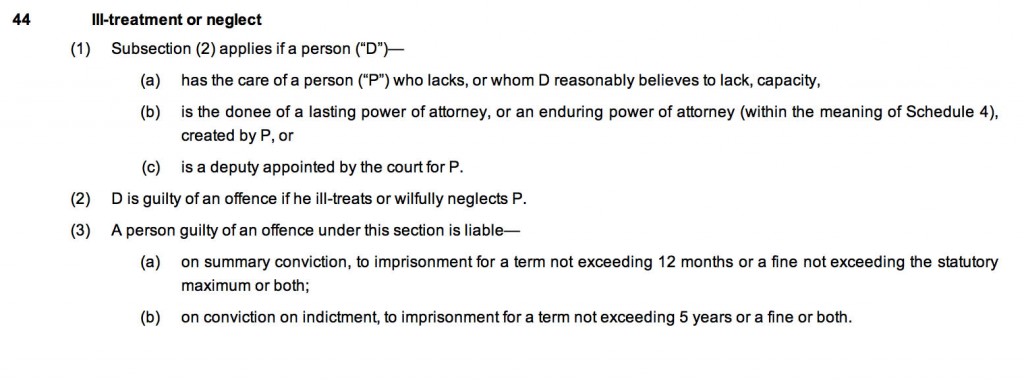
The offences can be committed by anyone responsible for that person’s care.
As can be clearly seen, the elements of this offence are that the offender:
- has the care of the person in question OR is the donee of a power of attorney OR is a court-appointed deputy;
- reasonably believes the person lacks capacity (or they do lack capacity);
- ill-treats or wilfully neglects the person.
- It can be expected that ill-treatment will require more than trivial ill-treatment, and will cover both deliberate acts of ill-treatment and also those acts reckless as to whether there is ill-treatment.
Wilful neglect can only apply to those who have a duty of care towards people who lack capacity.
Helpfully, part 14.3 of this Code of Practice (Code) accompanying the Mental capacity Provision gives examples of the kind of act that may constitute abuse and ill treatment. Specifically that Code includes “neglect” and “acts of omission”. This, it states, may include ignoring the person’s medical or physical care needs, failing to get healthcare or social care and withholding medication, food or heating. This appears to be alluded to in Jeremy Hunt’s example of a patient with dementia being denied a need – food.
Wilful neglect was supposed to represent a serious departure from the required standards of treatment and usually requires that a person has deliberately failed to carry out an act that they were aware they were under a duty to perform. Neglect or acts of omission could, therefore, include not responding to a person’s basic needs, i.e. assisting with feeding, drinking, toileting or in meeting personal care needs, preventing someone else from responding to those needs, or withholding or preventing access to medical care or treatment.
Back to Jeremy Hunt’s example, the caregiver knew the person with dementia needed food.
This responsibility is important when considering the meaning of the term “wilful” in this context which can be interpreted in two different ways:
- The person understood their responsibilities under the Mental Capacity Act and wilfully disregarded them;
- The person had a duty of care toward the service user and wilfully chose not to learn about it.
This may be reflected in previous cases such as R v Sheppard [1981] AC394 HL (which may be comparable; see discussion).
In consequence, defences could be raised to the effect that the elements of the offence set out in Section 44 are not made out in the following terms:
- there is no section 44 relationship (no care/power of attorney/court-appointed role);
- the person does not lack capacity and/or there was no reasonable belief in such a lack of capacity;
- there was no ill-treatment or wilful neglect.
It is well known that Hunt has been extensive discussions with patient campaigners for Mid Staffs.
But the problem is posed by the choice of Hunt’s example as a patient with dementia. The legitimate question has to be asked that, with the large number of ‘needless deaths’ repeatedly published in media reports, why reports of successful prosecutions under this provision of parliament might have been comparatively few?
From the timeline of the reported cases of neglect, and when this provision was in force, it would appear that this provision was ‘good law’ at the time. Many of the ‘needless deaths’ are widely reported in the media to have involved individuals who lacked capacity.
Why did the “wilful neglect” provision fail to do its stuff over Mid Staffs or Winterbourne, for example? How has Hunt tweaked it so that the law is actually effective for the public good?
It’s worth looking therefore carefully at the current operation of the section 44 provision.
There is no definition of “ill treats” or “neglects” within the Act so every day meanings of the word provide definition. The definition of ill treatment relies upon the definitions of the types of abuse which include physical, emotional, sexual, discrimination, psychological and financial.
Interestingly, neither section 44 of the MCA or section 127 of the MHA provides general protection for older people. Under these provisions they must either lack mental capacity or have a mental illness. In a case where an older person with capacity and no history of mental illness was found to be abused, the abuser would face the standard criminal charges of assault and battery (offences against the person in common law and in statute), and in a very extreme case where the sufferer dies, manslaughter.
So far most cases have involved the prosecution of direct frontline carers, where the evidence is very specific of wrongdoing by an individual. Owners and managers of small care homes have also been successfully prosecuted where there is clear evidence of what might be described as “institutional abuse”. Despite some attempts such charges have not been successfully prosecuted against large scale providers or their senior management, and this is still a longlasting concern of the implementation of the law. There is clear room for such NHS managers, care home managers and their private companies to be prosecuted particularly where they have failed properly to manage the delivery of such policies.
In a criminal context, the change must be proved beyond reasonable doubt, However, it is quite possible that guilt might be determined by magistrates or jurors who are likely to be very unsympathetic to care providers and staff.
One may be justifiably concerned, from the jurisprudence perspective, that the current lack of prosecution is based on a lack of appetite or understanding of care sector standards by prosecutors. A change in this attitude could see many more prosecutions. But again this is another ‘required’ change of culture?
Another problem is that the lawyers and regulators may not understand precisely the nature of what they are regulating against. The argument can be dismissed along the same lines as NHS managers do not ‘need’ to have any knowledge of medicine or nursing.
A prosecution of ‘wilful neglect’ Hunt admitted was so that the defendants could ‘feel the full force of the law’.
This document is typical of one of the many professional concerns of an appetite of being seen to punish hard retributively certain actions. The law must be necessary and proportionate, and one can see in principle how this provision could fulfil a worthy aim of parliament regarding patient safety.
Oncologists frequently perceive the discussion about whether or not to use or continue artificial feeding and/or hydration to be difficult. Successful approaches are not customarily demonstrated during medical training. Food and water are widely held symbols of caring, so withholding of artificial nutrition and hydration may be easily misperceived as neglect by the patient, family, or other professional and volunteer caregivers.
The response to the new ‘wilful neglect’ offence from clinical professionals and patients has been noticeably underwhelming.
There is furthermore a worrying aspect that people within the NHS system will be even more deterred from ‘whistle blowing’ under the Public Interest Disclosure Act [1998] than they were before, for fear of retribution over criminal sanctions.
For the offence of ‘wilful neglect’, the example that Jeremy Hunt gave last night has remarkable similarity to the sorts of offences you might have expected from Mid Staffs or Winterbourne View. The question therefore should be legitimately posed what it is that Hunt himself thinks is to be covered by the new law which was not covered previously. In summary, Jeremy Hunt needs to ask himself what his new law will achieve where section 44 of the Mental Capacity Act had failed.
“Lessons learned” – If every unemployment statistic is a tragedy, what was every ‘excess death’ at Mid Staffs?

It never fails to amaze me how certain policy strands run in parallel along a disastrous course, but silos in journalism mean that you’ll never get people joining the dots.
One example of this is the competitive tendering in legal services which Chris Grayling MP is currently shoehorning through, despite overwhelming opposition from lawyers including QCs. Everytime the unemployment figures up, or we have another revival in youth employment, Chris Grayling used to be the guy on TV saying that ‘every statistic is of course a personal tragedy’. Curiously you never get this phrase said about any excess death from the NHS which happened out of the ordinary. The concept that it is impossible to measure excess deaths at all will be alien to any professional in clinical negligence, who will be able to follow through the well-worn logic of duty-of-care of a clinician, failure of that duty causing breach, and that breach causing damage provided that there is not remoteness. We all know that the media is prone to hysteria, and indeed John Prescott once advised me not to believe everything written about ‘one’ in the papers. And an issue undoubtedly is that some are using what happened at Mid Staffs for their own agendas. You’d be forgiven for thinking some reports have the sole intention of shutting down the entire NHS as a national health service, blow all its credibility to smithereens, and to prepare its purchase price for the lowest bidder in a Government which has relish in outsourcing and privatisating the State infrastructure.
However, the sensationalism which was embraced whether there were any ‘excess deaths’ or not is perhaps distasteful at best, and frankly rude at worst. Mortality ratios are supposed to be the ‘smoke alarm’, but now that the inferno has happened, it is not time to remove the batteries from the smoke detector. The public inquiries at Mid Staffs I feel were essential. I don’t feel that this is an issue which could have been discussed behind closed doors ‘in camera’. It might be feasible to hold no-one accountable as the ‘culture’ is so widespread, but that has not led professionals to escape liability ever before for fundamental breaches in care, such as poor note-keeping, unprompt investigations, poor conduct and communication, from the professional regulators. The frustration has been there appears to have been very little accountability, and this is significant whether one feels the role of the justice system should be fundamentally restorative, retributive or rehabilitative. A certain amount of hysteria has instead engulfed proceedings at Mid Staffs, with the recently reported hostile behaviour towards Julie Bailey, remarkable campaigner and founder of ‘Cure the NHS’.
However, Julie has never wanted to ‘Kill the NHS’, but is deeply hurt about what happened to her Mum. Deb Hazeldine is very hurt about what happened to her mum. Any reasonable daughter would. These are times for reports of personal tragedies. Whilst we all have to move on, it is important to acknowledge accurately the distress of what happened, and this is precisely what we achieved in the Francis Inquiries. The accounts in those Inquiries are not figments of anyone’s imagination. It is even possible that we may have to learn from what happened there for other NHS Trusts. There is a trail of logic which goes that ‘efficiency savings’ were in fact cuts which included relative staff shortages, despite more being spent on the NHS budget overall including for salaries for certain personnel; this meant that key critical frontline staff were overstretched, there were genuine clinical events in patient safety which went beyond ‘near misses’, but they were not adequately dealt with. The Francis Inquiries should not be used to draw closure on the matters for the Labour administration, which I broadly supported. The reaction to the situation, a real one of personal tragedy, should not in my view a retweet of a blog which says that standard mortality ratios are unreliable, however correct that blog might be. This for me is not in any way personal – I like and respect very much people on all sides of what has been a highly charged discussion. I have known some of them for ages, and I will continue to support them publicly and in private.
We are not at the end of the solution of what happened in Mid Staffs, and for the time-being we should honestly recognise that.

If every unemployment statistic is a tragedy, what was every 'excess death' at Mid Staffs?

It never fails to amaze me how certain policy strands run in parallel along a disastrous course, but silos in journalism mean that you’ll never get people joining the dots.
One example of this is the competitive tendering in legal services which Chris Grayling MP is currently shoehorning through, despite overwhelming opposition from lawyers including QCs. Everytime the unemployment figures up, or we have another revival in youth employment, Chris Grayling used to be the guy on TV saying that ‘every statistic is of course a personal tragedy’. Curiously you never get this phrase said about any excess death from the NHS which happened out of the ordinary. The concept that it is impossible to measure excess deaths at all will be alien to any professional in clinical negligence, who will be able to follow through the well-worn logic of duty-of-care of a clinician, failure of that duty causing breach, and that breach causing damage provided that there is not remoteness. We all know that the media is prone to hysteria, and indeed John Prescott once advised me not to believe everything written about ‘one’ in the papers. And an issue undoubtedly is that some are using what happened at Mid Staffs for their own agendas. You’d be forgiven for thinking some reports have the sole intention of shutting down the entire NHS as a national health service, blow all its credibility to smithereens, and to prepare its purchase price for the lowest bidder in a Government which has relish in outsourcing and privatisating the State infrastructure.
However, the sensationalism which was embraced whether there were any ‘excess deaths’ or not is perhaps distasteful at best, and frankly rude at worst. Mortality ratios are supposed to be the ‘smoke alarm’, but now that the inferno has happened, it is not time to remove the batteries from the smoke detector. The public inquiries at Mid Staffs I feel were essential. I don’t feel that this is an issue which could have been discussed behind closed doors ‘in camera’. It might be feasible to hold no-one accountable as the ‘culture’ is so widespread, but that has not led professionals to escape liability ever before for fundamental breaches in care, such as poor note-keeping, unprompt investigations, poor conduct and communication, from the professional regulators. The frustration has been there appears to have been very little accountability, and this is significant whether one feels the role of the justice system should be fundamentally restorative, retributive or rehabilitative. A certain amount of hysteria has instead engulfed proceedings at Mid Staffs, with the recently reported hostile behaviour towards Julie Bailey, remarkable campaigner and founder of ‘Cure the NHS’.
However, Julie has never wanted to ‘Kill the NHS’, but is deeply hurt about what happened to her Mum. Deb Hazeldine is very hurt about what happened to her mum. Any reasonable daughter would. These are times for reports of personal tragedies. Whilst we all have to move on, it is important to acknowledge accurately the distress of what happened, and this is precisely what we achieved in the Francis Inquiries. The accounts in those Inquiries are not figments of anyone’s imagination. It is even possible that we may have to learn from what happened there for other NHS Trusts. There is a trail of logic which goes that ‘efficiency savings’ were in fact cuts which included relative staff shortages, despite more being spent on the NHS budget overall including for salaries for certain personnel; this meant that key critical frontline staff were overstretched, there were genuine clinical events in patient safety which went beyond ‘near misses’, but they were not adequately dealt with. The Francis Inquiries should not be used to draw closure on the matters for the Labour administration, which I broadly supported. The reaction to the situation, a real one of personal tragedy, should not in my view a retweet of a blog which says that standard mortality ratios are unreliable, however correct that blog might be. This for me is not in any way personal – I like and respect very much people on all sides of what has been a highly charged discussion. I have known some of them for ages, and I will continue to support them publicly and in private.
We are not at the end of the solution of what happened in Mid Staffs, and for the time-being we should honestly recognise that.
Jeremy Hunt says that ‘NHS 111′ is now “up-and-running”, but that targets should not be gamed

The reality is that the vast majority of hospitals in the NHS are currently failing to see 95% of patients within four hours. Jeremy Hunt was interviewed on the BBC ‘The Andrew Marr Show’ this morning in a wideranging interview which also covered membership of the European Union.
Jeremy Hunt first underplayed the severity of the NHS 111 fiasco, but claimed that things are better now. Of course, one tragedy in care is one too many. The NHS says it has experienced seven “potentially serious” incidents in the first few weeks of its 111 urgent care helpline in England. One case involved a patient in the West Midlands who died unexpectedly and there have been reports of calls going unanswered and poor advice being given. All the cases are being reviewed. Other organisations are also running 111 lines for NHS England and have been warned they must deliver good care or face financial or contract penalties.
In 2010, critics had claimed the change from NHS Direct to NHS 1111 would undermine the quality of the service by reducing the number of qualified nurses answering calls, but chief executive of NHS Direct Nick Chapman said that new helpline would be better and more cost effective.
Jeremy Hunt, meanwhile, this morning stated, “There are short-term pressures and long-term pressures. We did have teething problems with NHS 111. It is up-and-running now in 90% of the country. We need to have better alternatives in primary care, a better personal relationship between patients and their GPs”.
“Under the last government, we had a culture of ‘hitting targets at any cost’.” Hunt then went onto blame ‘the target culture’ for bringing about the problems which Mid Staffordshire NHS Foundation Trust had faced, leading to two inquiries by Sir Robert Francis QC.
Hunt further added that, “I would never blame GPs, because they work extremely hard. I have just been in one.”
Of course, nobody reasonable, seriously, would take the blindest bit of difference of Hunt comparing his brief time work experiencing in a GP surgery to seven years of basic medical training, including pre-registration training, even prior to specialist GP training.
GPs have experienced a number of contractual changes over time (described here), and latterly it has been mooted that the personal income of GPs, following the latest change, has been steadily eroded as funding levels have been frozen, whilst the running costs of surgeries and staff pay have increased.
Hunt further provided this morning, “That Contract is one of the contributing causes, because after hours and at weekends the service deteriorates. I don’t want to go back to those days where GPs are personally on call at 2 am.”
Hunt added that, “GPs should have responsibility that people on their list have a good service.”
It is difficult to see what exactly Hunt means by this, as it is hard to separate out the effect of a medical decision taken out-of-hours compared to a decision compared to during ‘conventional hours’, and one assumes that each Doctor is still responsible for his/her own medical actions to the General Medical Council, wherever he or she provides care.
Hunt then gave a response which managed to combine a welcome for targets in improving care, with direct criticism of those managers clearly gaming the system.
Regarding the A&E target, Hunt opined, “It is a very important target, and we have never said we do not have to have good targets. We don’t want people to follow targets at any cost.” However, he then described a series of measures how managers would then ‘game’ the system.
“We had beds which hadn’t been cleaned, ambulances circling hospitals before they entered the front door because they didn’t want the clock the start.”
