Home » Posts tagged 'language'
Tag Archives: language
Sticks and stones may break my bones
I had first become interested in the language surrounding dementia in 2014, when I presented a poster on the G8 pitch, at the Alzheimer’s Europe conference in Glasgow.
At that point, I realised that sticks and stones could break my bones, but words could hurt me.
I have long since not attended any national or international conferences, not simply because I found the same topics being discussed in perpetuity, but because I felt the conferences were for an in-house cliques who were far more into massaging their own egos and putting themselves up in flash hotels than the reality of dementia.
But I later returned to the issue of language, in relation to stigma, in my second book on dementia ‘Living better with dementia’ published in 2015 by Jessica Kingsley Publishers. As my own mother lives with me, and as her dementia advances, I’ve genuinely found my own book to be a source of information and support. For example, only last night I was reading up on my own thoughts of the ‘sweet tooth’ in dementia and the neuroscientific evidence for why it occurs. Latterly, I’ve toyed with the idea of writing a cookbook for unpaid carers, living with limited resources including scarce money and time, of people living with dementia. I would love to work with someone who’s interested in this specialist field, such as a nutritionist or dietician, to help me.
I became physically disabled in 2007 after more than a month unconscious on the intensive care unit of a local hospital, where I was invasively monitored for acute meningitis. Although I subsequently read Goffman on stigma about a decade later, I had the misfortune to experience stigma first-hand. The sense of ‘otherness’ is something you experience if you’re in a wheelchair, and a London cab refuses to stop despite the cab having its yellow light on. Of course, I had direct experiences of ‘otherness’ as other medical professionals disowned and excluded me when I needed help the most – both in my alcoholism and in recovery. I am currently doing professional dilemma questions, and the knowledge that senior clinical people I worked with turned a blind eye, or did not know what to do and did not admit it, to my illness still frightens me.
As a result of this, I have a low threshold to calling out ‘otherness’, that is where you define people as different to you, and, more than than that, try to discredit them. This might include supporters of Brexit or not, Jewish or Muslim citizens or not, or even living with a long term condition. I don’t think the key to destigmatising stigma is by segregating people. At worst, this might include the ghettoization of people with dementia or mild cognitive impairment such that they all safely live in the same ‘dementia village’, to all intents and purposes ‘out of sight’ and ‘out of mind’. Care homes used to be criticised, by some, for potentially warehousing individuals if the prescription of chemical or physical restraints was frequently abused, similarly. This is not real integration and inclusion, in other awards appreciating the diversity of individuals, but actually lumping all people together with the same label.
For example, in ‘dementia friendly communities’, we don’t acknowledge individuals have different qualia of cognitive impairments, in memory, language or whatever, at various degrees of severity. We don’t discuss how the social determinants of health impact on the health and wellbeing of people, such as poverty or the shutting of day centres. We just clump all people together as ‘dementia’. This is not a million miles off of creating vast groups comprising unique individuals, such as ‘learning disabilities’ or ‘the elderly’.
Whilst the counter-argument is that identification of these groups of people means that their needs can be serviced, often the opposite is true. Recently, a paper has been published on identifying the most ‘frail’ people so that we can be aware that they are the most intense in resource allocation. But think about this carefully. This can mean that we use the information to discriminate actively against the most vulnerable – ‘equity’ and ‘justice’ are not necessarily compatible ethically.
Above all, I am scared how language is used to legitimise discrimination, ‘otherness’ and to embolden other people’s vulnerabilities and weaknesses.
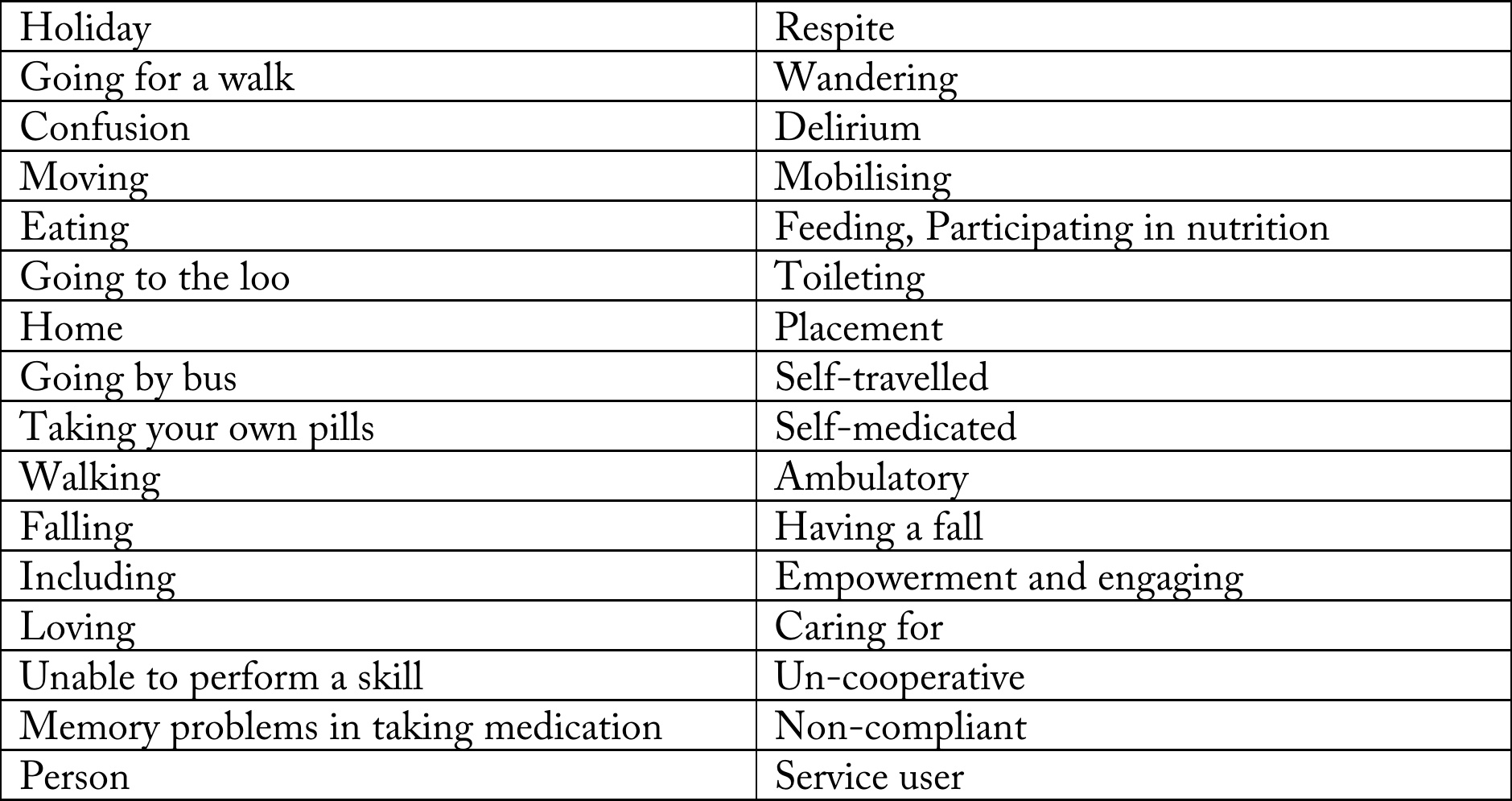
I did a brief scan of some ‘offending’ words, and I compiled them into a table.
I have been much derided for talking about “assets” and “strengths” as well as “deficits”. For example, one person commenting on a piece I wrote in the Guardian remarked similar to, “We don’t need to worry about this patient lying on the operating theatre table with advanced pancreatic cancer. She has great teeth.”

But I strongly believe that it is not difficult to slip into the patronising ‘does he take sugar mentality?’ I don’t wish to turn the medico-legal concept of ‘paternalism’ into a “dirty word”, but, as for our experiences with individuals with special needs, it is a slippery slope to outright dehumanisation and depersonalisation.
I never really understood what it was like to lose your sight until I went blind in one eye last year – but this was surgically operated upon with success. Likewise, I think many of us think we won’t be the ones who get diagnosed with cancer or dementia. But the law of averages means that some of us will be.
And we should think about how “we” would feel if “other people” talked about “us” like that.

It’s not the word ‘dementia’ itself which is stigmatising, but the words which are used around it
“the truth is dementia now stands alongside cancer as one of the greatest enemies of humanity”

An analysis of 75 English language web articles on the G8 dementia summit
Background
Experience has suggested that academic scientists can be as ‘guilty’ as the popular press in generating a ‘moral panic’ causing mass anxiety and hysteria. Take for example the media reporting of the new variant Creuztfeld-Jacob disease, a very rare yet important cause of dementia (Fitzpatrick, 1996).
How dementia is represented in the media is a good surrogate market of how the issue can be represented in certain segments of the culture of a society (Zeilig, 2014).
According to George, Whitehouse and Ballenger (2011), the concept of dementia, a term which they attribute to Celsus in the first century A.D. — has long carried “social implications for those so diagnosed and has been associated with reduced civilian and legal competence, as well as with entitlement to support and protection.
A range of emotionally charged metaphors about dementia pervades the popular imagination, and these are found in newspaper accounts, political speeches, and in both documentary and feature films. The ‘G8 dementia’ summit allowed many of these recurrent motifs to resurface unchallenged.
I’ve been intrigued how the G8 Dementia Summit was covered in the English-speaking media on the web. So I did a Google search for “G8 dementia”, on the UK Google site. It only came up with languages in English article, and I included the top 75 search results.
I excluded some search results. I excluded webpages consisting of only videos. Flickr photos or Pinterest boards. I decided to exclude articles less than 100 words long.
Aim
The aim of this piece of work was to complete a preliminary exploration of how the #G8dementia summit was reported on the internet in the English language.
The literature in this field is very small, and no study to my knowledge has ever been undertaken for the actual reporting of the G8 dementia summit which was unprecedented.
Methods
For the text analysis, done online using this tool, I excluded the author names, titles, location of authorship of the article (e.g. London). also excluded the endings, invariably, “Read more” “You may also like”, “You can read more about” and list of other ‘links’ to look at. I excluded duplicates. Finally, one article which was largely a compilation of tweets was excluded.
Results
Unsurprisingly, the word “dementia” featured 955 times, but encouragingly “people” featured 280 times. I found this quite gratifying as I have just published a book on the rôle of the person and the environment for living well with dementia – though the vast majority of articles did not have wellbeing as their main thrust.
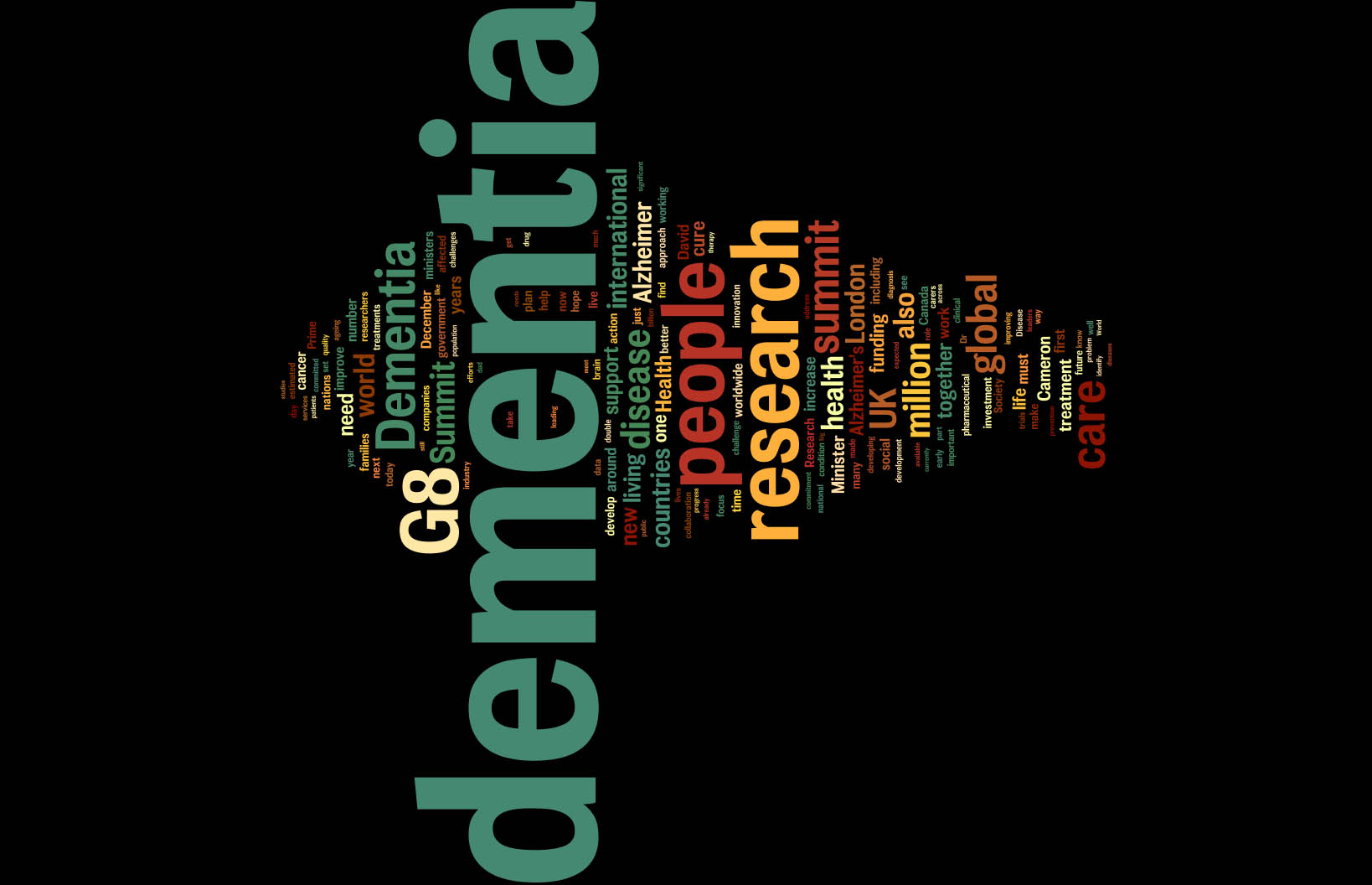
I think the problem in English policy is revealed in the finding that “research” appears 334 times, and yet “wellbeing” is there fewer than eight times. The facts that “data” is used thirty times, with “collaboration” 28 times, hint at the overall drive towards data sharing for the development of cross-country trials and personalised medicine.
There seems to be a greater need for “funding” somewhere, a word used 66 times. There’s clearly an “international” focus, a word used 103 times.
The word “carers” was only used thirty times – a bit of a knee in the groin for the caring community?
The term “social care” is used 14 times across the 75 articles, but this is dwarfed by the use of the term “innovation” used 37 times. “Innovation” is of course a key meme of Big Pharma, as demonstrated by this infographic by Eli Lilly, a prominent company in dementia neuropharmacology.

The ideological bias towards the medical model for dementia is reflected in the frequency of the word “disease” or “diseases”, totalling 203; “treatment” or “treatments”, totalling 91; and “cure” or “cures”, totalling 72.
There’s clearly a bias towards Alzheimer’s disease, in that “Alzheimer” was used 145 times, with the word “vascular” used only six times. Strikingly, no other forms of dementia were mentioned. There are probably about a hundred known forms of diagnoses comprising the dementias, including some very common ones such as “frontotemporal” or “diffuse Lewy Body”.
Various authors, including Kate Swaffer who lives with a dementia herself, have often remarked on this bias known in the literature as “Alzheimerisation” (Swaffer, 2012).
“Cameron” is mentioned 60 times, and “Hunt” is mentioned 24 times. “Hughes”, as in Jeremy Hughes, CEO of the Alzheimer’s Society, is only mentioned 5 times.
It’s also interesting to see which other conditions are mentioned alongside dementia in these 75 articles. Only three were, in fact: these are “cancer” (45 times), HIV (25 times) and AIDS (29 times); treating HIV and AIDS as distinct, which is of course is not necessary to do, and there may have been no intention on the part of the journalists to use these words specifically in their narratives.
Thankfully, the usual dramatic terms were not used often.
“Timebomb” was only twice – once by the BBC
“It also called on the World Health Organization to identify dementia as “an increasing threat to global health” and to help countries adapt to the dementia timebomb.
[http://www.bbc.co.uk/news/health-25318194]
and then by a blog for the “Humanitarian Centre:
“Dementia has been branded a ‘timebomb’, as ageing populations will exacerbate the problems and costs associated with dementia.”
[http://www.humanitariancentre.org/2014/01/tackling-dementia-the-g8-dementia-summit-2]
The terms “bomb” or “bombs” were only used four times, and encouraging one of these was complaining about in a passage complaining about military metaphors.
“To make matters worse people living with dementia were exposed to scaremongering rhetoric. We already know that people living with dementia are directly affected by stereotypes and negative attitudes to dementia. The widespread use of military style metaphors – time bombs, battles, victims and fights in addition to media promotion of the term ‘suffering from dementia’ combine to increase fear of the disease for those living with it. This fear exacerbates the isolation and exclusion that people with dementia often feel following diagnosis.”
[http://www.centreforwelfarereform.org/library/by-date/g8-dementia-summit.html]
The dementia “time bomb” crops up frequently in U.K. broadsheets (Furness, 2012) and tabloids. Time bombs are devices that could go off at any time; their most common use has been in politically motivated terrorism. The association of dementia with terrorist tactics is fascinating, invoking the sense of a threat
The only use of the word “tide” was in a direct quotation from a speech by Jeremy Hunt, current Secretary of State for Health:
“We have turned the global tide in the battle against AIDS. Now we need to do it again. We will bankrupt our healthcare systems if we don’t,” he said.”
[http://www.reuters.com/article/2013/12/11/us-dementia-g-idUSBRE9BA0HE20131211]
The danger of flooding has long been associated with dementia. A 1982 U.K. report was entitled: “The rising tide: Developing services for mental illness in old age” (Arie and Jolley, 1983).
Note Hunt’s ‘wordie’ contains ‘heartache’, ‘threats’, ‘battle’, ‘dreading’, ‘stigma’ and ‘fight’, but also includes ‘diagnosis’, ‘people’ and ‘research’.

It is indeed fascinating the on-running theme of promoting dementia research in the absence of a context of wellbeing.
David Cameron’s ‘Wordie’ is quite tame.

But the consequences for this media messaging are potentially quite profound.
Limitations
There is a sample bias introduced with how Google orders its ranking.
Page ranking is not only calculated on the basis of traffic, but also in terms of degree of linkage with other websites.
It is possible that higher ranking articles, particularly online versions of newspaper articles, have a common root such as the Press Association, leading to a lack of independence amongst authors in their coverage of the Summit.
Conclusion
Whitehouse concludes a recent abstract as follows:
“Creating a more optimistic future will depend less on genetic and reductionist approaches and more on environmental and intergenerative approaches that will aid in recalibrating the study of AD from an almost exclusive focus on biochemical, molecular and genetic aspects to better encompass ‘‘real world’’ ecological and psychosocial models of health.”
Encouragingly though the frequency of words such as ‘timebomb’ and ‘flood’ were not as much as one might have feared, from the (albeit small) literature in this field.
If you assume that the 75 articles form a representative cohort of copy on the G8 dementia summit, the picture presented has a clear emphasis on a magic pharmacological bullet for dementia. The copy represents not a balanced debate, on behalf of all stakeholders, but reads like a business case to invest more in neuropharmacological-based research into dementia.
References
Arie, T., & Jolley, D. (1983). The rising tide. British Medical Journal, 286, 325–326.
Fitzpatrick, M. (1996) Creutzfeldt-Jakob disease and bovine spongiform encephalopathy, BMJ, 312, 1037.3.
George, D.R., Whitehouse, P.J., Ballenger, J. (2011) The evolving classification of dementia: placing the DSM-V in a meaningful historical and cultural context and pondering the future of “Alzheimer’s”, Cult Med Psychiatry. 2011 Sep;35(3):417-35.
Furness, H. (2012, March 7). Dementia is ‘next global health time bomb.’ The Telegraph. Retrieved from http://www.telegraph.co.uk/health/healthnews/9127801/Dementia-is-next-global-health-time-bomb.html
Swaffer, K. (2012) Dementia, denial, old age and dying, blogpost here.
Whitehouse, P.J. (2014) The end of Alzheimer’s disease-From biochemical pharmacology to ecopsychosociology: A personal perspective. Biochem Pharmacol. 2014 Apr 15;88(4):677-681. doi: 10.1016/j.bcp.2013.11.017.
Zeilig H. (2014) Dementia as a cultural metaphor, Gerontologist, 54(2), pp. 258-67.

When we know when “the war against dementia” is over?

In writing this article, I have no intention of ‘sanitising’ dementia. I’m mindful of two recent comments which fell in my path indirectly: “Dementia is such a cruel disease” (by a daughter of someone living with dementia), and “I don’t know of anyone who doesn’t suffer something as a result of his or her dementia”. The purpose of this article is just to review common motifs in dementia media communications.
When will know when the “war against dementia” is over? This is not an altogether frivolous question, as a MP once famously asked Tony Blair in Prime Minister’s Questions, “When will the war against terrorism be over?”
On 28 November 2013, about dementia, Jeremy Hunt wrote in the Telegraph: “It is a truly horrible disease“.
This set the ‘mood music’ for some of the G8 dementia conference, but the G8 conference was indeed a very positive occasion.
Recently, in “The Loss of Sadness”, Horwitz and Wakefield (2007) wrote that, while depressive disorder can certainly be a devastating condition warranting medical attention, the apparent “epidemic” in modern culture reflects the way the psychiatric profession (perhaps under the influence of pharmaceutical companies looking to widen markets) has understood and reclassified normal human sadness in the DSM-IV as a largely abnormal experience.
The popular metaphorical framing of dementia seems to operate on two levels. It is generalised as a vast, natural or monstrous force that we must “fight”, and it is also located as a very specific condition that affects individuals in extreme ways. In both cases, the effect is to make us feel both terrified and relatively powerless. As Terry Pratchett, who is reported in the public media as having a condition akin to posterior cortical atrophy, viewed: “People seem to think of Alzheimer’s as something rather terrible and dreadful, almost as if witchcraft is involved”
Literally meaning ‘‘away’’ or ‘‘out’’ of ‘‘mind’’ or ‘‘reason’’ in Latin, the actual term ‘‘dementia’’ entered the English language from the French ‘‘de ?mence’’ via the French psychiatrist Philippe Pinel, who made notable contributions to the categorisation of mental disorders in the late 18th and early 19th centuries. Over the centuries, the phenomenology of dementia has been causally associated with witchcraft, moral degeneracy, bad blood and a dissipation of vital energy from the brain, among other factors.
The Wordie for David Cameron’s speech at the G8 summit is indeed interesting, and to be fair in the vast majority is largely upbeat and positive. Whilst there is no recording of the speech on YouTube, the full text of the speech at the ‘G8 dementia summit’ at Lancaster House on 11 December 2013 is available here.

The opening to this speech was pretty chilling, however:
“It doesn’t matter whether you’re in London or Los Angeles, in rural India or urban Japan – this disease steals lives; it wrecks families; it breaks hearts and that is why all of us here are so utterly determined to beat it.”
What exactly is this “it”? What kind of creature is it which steals, wrecks and breaks? This is the fundamental problem. Dementia is not a creature, it’s not an alien, it’s not a mega monster even. It’s an umbrella term covering about 200 different conditions where parts of the brain lost structure and function, leading to problems for that individual; however certain functions remain in the earlier stages, which is why it is potentially unfair to use such graphic language.
It is therefore with some irony Jeremy Hunt had concluded his piece in the Telegraph thus:
“With advances in medical science, the commitment of governments across the world and a willingness from everyone to change attitudes, we truly can be the generation that beats dementia.”
And it’s not the first time David Cameron had used this turn of phrase. In his keynote speech about increasing funding for dementia, the U.K. Prime Minister talked about “the quiet crisis, one that steals at lives and tears at the heart of families” (March 26, 2012). As was noted at the time, this language echoes descriptions of primeval monsters such as Grendel in the Anglo Saxon poem “Beowulf”. Dementia becomes an invader or evil monster that creeps up on people and steals them from themselves. Correspondingly, people living with dementia correspondingly become “victims”.

Noticeably, the Wordie includes “malaria” and “AIDS”. This is because of the following line:
“In generations past, the world came together to take on the great killers. We stood against malaria, cancer, HIV and AIDS and we are just as resolute today.”
Jeremy Hunt in the Telegraph had written:
“In the Sixties people were too scared to talk about cancer. In the Eighties the same happened with HIV/Aids. After a long and painful journey, we are now much more open about both – and better able to tackle them.”
It seems that this parallel with HIV/AIDS and cancer has been very carefully choreographed. There are indeed some successful treatments for many cancers, but cancer like dementia is an umbrella term covering a wide variety of conditions. A “cure for dementia” is meaningless as a term, as the frontotemporal dementias particularly common in the younger age group are a different pathological entity to the most common type, the dementia of the Alzheimer type.
And how exactly has cancer done? According to the world statistics from WCRF, there were an estimated 12.7 million cancer cases around the world in 2008, of these 6.6 million cases were in men and 6.0 million in women. This number is expected to increase to 21 million by 2030. How is a similar “war” against HIV/AIDS doing? According to AmfAR, more than 35 million people now live with HIV/AIDS, 3.3 million of them are under the age of 15; in 2012, an estimated 2.3 million people were newly infected with HIV, and 260,000 were under the age of 15. Every day nearly 6,300 people contract HIV—nearly 262 every hour.
Dementia has replaced cancer as the “scourge of modern times”. The discourses of the scientific community reinforce this pervasive sense of horror about the dementias. For example, the prevalence of dementias is described in dramatic terms as an “epidemic”. The prevalence of dementia in the UK has in fact thought to be falling in recent times (hence explaining the formidable Prof Burns’ relative unease about dementia being called a ‘timebomb’ by Emily Maitlis on BBC News, a ‘timebomb’ which crucially scientists have failed to address.)
In 2011 in an article entitled “Dementia crusade’s £20m breakthrough”, the Care Services Minister at the time announced a multi-million pound boost in funding for the fight against dementia. The word “crusade” achieves an interesting multiplicity of effects, including an emphasis on faith and battle and on something that not only is metaphysical but can also be “won.” The overall impression is of dementia as huge and ancient, and of massive significance. It appears beyond our grasp and can only be understood through reference to massive natural phenomena (usually disasters) or in biblical/mythical terms.
Flooding is a particular popular literary turn. The danger of flooding has long been associated with dementia. A 1982 UK report was entitled: “The rising tide: Developing services for mental illness in old age“. Rising tides continue to inform the language of contemporary politicians when discussing dementia.
Cameron likes it too, apparently. He referred to the need for Britain to change its attitude to the “rising tide of people suffering with dementia” (May 26, 2012). Alistair Burn’s article “The number of people with dementia in England: turning the tide – Alistair Burns” continued this “tide” theme.
The press and television documentaries abound in “personal” stories about dementia and in tales of cures that are imminent or preventative measures that can be taken to ward it off. Classifying the hundreds of different types of dementia has also been politically powerful. It has undoubtedly facilitated funding and research into diseases for which it is implied that there will eventually be a cure. Ultimately, this broad brush approach is now being used to argue for a “one glove does not fit all” approach: the big corporate winner of personalised medicine, as explained by Cameron thus:
Take just one initiative – Bio Bank. More than half a million people have volunteered to take part in this providing blood samples, getting their vital signs checked, so we can see how diseases like dementia get signalled. The plan is to use Bio Bank to take brain scans of up to 100,000 people – allowing us to see the earliest stages of Alzheimer’s and other diseases. That is the kind of ambition we’re seeing here in the UK ambition that should give hope to people right around the world.
There’s something subtle at work here with the words “ambition” and “ambitious”. Of particular concern to those worried about overmedicalisation is that some experts are now arguing for treating asymptomatic (‘‘normal’’) people with ‘‘abnormal’’ imaging and cerebrospinal fluid biomarker profiles with long-term preventative therapies. This is exactly what seems to be happening here with Cameron’s comment. In a sign of desperation of Pharma wishing to resurrect an ‘ailing industry‘, multi-national Big Pharma believes that early treatment is key to finally achieving a treatment success of any meaningful magnitude.
There are some expected financial memes: like “economy”, “genomics” and “reinvest”. Whilst the spokesmen officially don’t officially promote particular ‘brands’, the speech explicitly mentions UK life sciences companies, like Ixico, Cambridge Cognition, Psychology Online and Proteome Sciences, in developing new tests for Alzheimer’s Disease. As such dementia can’t be seen as “wealth creating”, so the need to promote private markets and innovation is a delicate one to take. However, David Cameron has increasingly appeared giving speeches in the manner of CEO wishing for corporate investment. As such, ‘cure’, not ‘care’, is where the money is at possibly. Cure’s in the wordie; care is not.
“Fight” is THE BIG prominent word. This recurring linguistic device in the cultural framing of dementia is the reliance on military and war-like metaphors. Cameron has been fighting for some time, it’s a wonder he himself isn’t exhausted. On March 26, 2012, he proclaimed rather triumphantly: “We need an all-out fight-back against this disease; one that cuts across society.”
The dementia “time bomb” crops up frequently in U.K. broadsheets and other tabloids. Time bombs are devices that could go off at any time; their most common use has been in politically motivated terrorism. The association of dementia with terrorist tactics is fascinating, invoking the sense of a threat. So when will we know when the war against dementia is over..?
Now listen carefully. As sure as night follows day, academics won’t be able to fight these horrible journalists, destroying the ambitions of people trying to live with dementia in a positive light. Whilst the electoral timebomb continues to tick tock, we can find a cure for this government and their partners trying to demonise those people currently trying to live with dementia. While the war will be long, we can turn the tide on the Pharma companies destroying minds with their false promises, and encourage a new dawn after this crisis where wellbeing interventions are treated seriously at last.
See what I did there?

Are individuals living with dementia “recipients” of care?
Language is very important. Only this week, the media was stuffed full of talk of dementia being a ‘horrible disease’, and people ‘suffering’.
A recent Telegraph article cited, “Health Secretary Jeremy Hunt says it is “utterly shocking” that only half of people suffering from dementia are being formally diagnosed.”
Society has a certain image of dementia. It really is no use denying that this image is horribly negative, and feeding on this fear can be low-hanging fruit for raising funds through charity.
In this scheme of thinking, those with the dementia are only viewed through the prism of their illness, and this is often reduced to the image of its last and most tragic phases.
It is as if as soon as a diagnosis of a progressive dementia is made, the person in question, it is perceived by the rest of society, automatically becomes incapable of taking any autonomous decisions, loses his/her personality and identity and immediately needs to be cared for.

In reality, however, this illness can develop quite slowly: between the moment when it is diagnosed and the terminal phase, there may be years of development. Moreover, people living with the illness can rarely have the opportunity to express their thoughts and feelings about it: there is communication about them, but only rarely with them. The individual sadly disappears behind the blanket label of an illness.
The term “suffering”, however, sounds negative, and does not support the concept of “personhood”, and certainly does not fit with a philosophy of “hope” and “wellness”.
The way the NHS has latterly been structured as a market also reinforces this customer-supplier master-servile relationship. Dementia care is a ‘service’ you can pay for, with or without a personal health budget.
The dominant notion itself that the need of people with dementia to socialise should be met by “services” is disempowering, for the concept of service incorporates the notions of “providers” and “recipients”; of the “helpers” and “the helped”, of “us” and them”.
These notions further perpetuate the stigmatising assumption that people with dementia are only able to participate in relationships as “receivers”, and that relating to them is a problem for those who do not have the disease: they further advance the widespread perception that people with dementia are, essentially, a “burden” on their families and society.
This term “burden” can perhaps help validate the ‘burden’ some caregivers experience, but should not be assumed and should be avoided when speaking in generalities such as public presentations.
This language and terminology are in desperate need of change, and the prevailing perception of people past the first stages of dementia as just receivers of care, and users of services, needs drastic reframing.
The truth is that, as the symptoms of the disease progress, people with dementia can still play an active role in society, if provided with support, and this support can very often be provided by fellow citizens, rather than by professionals paid to deliver a service.
The purpose of person-centred language is to recognise the impact of language on thoughts and actions, to ensure language does not diminish the uniqueness and intrinsic value of each person.
Personhood is pivotal. This is the standing or status that is bestowed upon one human being by others in the context of relationship and social being. It implies recognition, respect and trust.
The aim is to create the positive conditions where the person can live without stigma; where people are treated with warmth and authenticity, listened to without judgment and are given opportunity for self-expression.
There are, however, ways to ‘reframe’ this debate.
Framing is a fast developing concept, as much in communication sciences as in other disciplines. This is partly due to the fact that it is a rather flexible approach that lends itself to many applications.

When there is a question relating to knowing how a particular subject is presented, in the media for instance, framing immediately springs to mind.
Instead of painting the illness as a homogenous and unchanging totality, it would be preferable to place the accent on its progressive and developmental nature.
One can put the accent on continuing to be a real person despite the decline due to the illness: acknowledge the personality, the identity and the life journey of those with a progressive dementia.
One can also develop empowerment and social inclusion with people with a progressive dementia. Such individuals are more than passive and dependent consumers of help and care services. They have resources that should be mobilized. The principle of inclusion implies that society is composed of all its citizens. However, this needs competent leadership.
Let those who living with dementia speak. It will provide others with one of the most powerful counter-examples in relation to the current dominant image, which often makes the individual disappear behind his/her illness.
Let your respect for those living with the dementia be obvious in what you have to say.
It is useful also never to forget that people with Alzheimer’s disease also have their own life story, their own personality and character. This is because their long-term memories are relatively preserved, due to a phenomenon first characterised by the French neurologist Ribot in the 1880s. Enable these aspects to be expressed too.
Those who disseminate messages, especially via texts designed to influence people, may deliberately choose a frame that the reader is supposed to pick up and appropriate so as to henceforth view reality in this way.
Given that frames form part of any culture, many of them are common to both the sender and the recipient of a given message.
The question of whether framing is a conscious process remains open to discussion: how far will the writer of a given text deliberately choose a frame that serves his own interests?
As we approach the G8 leading on the subject of what is important in dementia diagnosis, research and care, it is all the more important that we frame the discussion properly.
There are so many stakeholders in English dementia policy, it can be quite uncertain know where the current dementia policy has come from.
David Cameron has often argued that ‘it is not where you’ve come from, it’s where you’re going to’. If one of the goals is destigmatising dementia in society, how we articulate the present debate today is vital to our progress tomorrow.
This means not talking about ‘horrible’ and ‘suffering’ in a way as to encourage ‘moral panic’.
This means treating people with dementia, living at all stages with any particular condition, with the dignity they deserve; this will enormously help carers too.
Sustainability: a hopelessly misused word in English health policy, popular for its misleading potential

For Twitter or Google, whose revenue potential is stratospheric, analysts have difficulty in defining how ‘sustainable‘ their business model is.
Turning the NHS into a Darwinian ‘survival of the fittest’ always implied that there were bound to be winners and losers. With recent legal decisions firmly deciding that NHS Foundation Trusts, as “enterprises”, cannot merge on purely economic competition law grounds is a profoundly significant decision, you can certainly say we are living in dangerous times.
And yet ‘sustainability’ is possibly the most misused word in English health policy. It means different things to different people. Its ambiguity means that it is highly popular, particularly for its midleading potential.
I was having dinner with a senior lawyer in Stockwell the other evening, and we both decided that, for many, the word had become synonymous with a meaning of ‘maintained’. We felt this usually led to a discussion of ‘we can’t go like this’, thus softening up the discussion to save money.
There is some method behind this madness, however. Rather than spreading money thinly around various hospitals, possibly there can be fewer hospitals with a ‘safe’ level of resources.
This argument clings onto the idea that the NHS funding is finite, and increasingly ‘unaffordable’. This of course is a perfectly rationale argument if you assume that the Government is incapable of producing economic growth. And for the last three years, the Government has taken us on a turbulent rollercoaster ride of GDP when the UK economy had been recovering in May 2010.
It is currently argued by some that the most successful healthcare organisations are those that can implement and sustain effective improvement initiatives leading to increased quality and patient experience at lower cost. Indeed, the NHS itself has produced a “Sustainability Model and Guide” to support health care leaders to do just that.
Next year, the “NHS Sustainability Day 2014” will feature tools and case studies with proven technologies, methods and projects that have yielded promising results. Technology is often cited as a potential source of the ballooning NHS budget, but the NHS simply has to learn how to order and use technology which is most appropriate for the needs of employees.
So why have the media and other professionals actually lost sight of the actual definition of ‘sustainability’? The politicians have an agenda to make the NHS more ‘affordable’, given the parties en masse wish to embrace ‘savings’ and not be THE parties of high taxation. This, however, means that politicians are being somewhat economical with the truth, and a responsible media here is critical.
Sustainability is the “capacity to endure“. In ecology the word describes how biological systems remain diverse and productive over time. Long-lived and healthy wetlands and forests are examples of sustainable biological systems. For humans, sustainability is the potential for long-term maintenance of well being, which has ecological, economic, political and cultural dimensions. It usually comes from an idea that you look after the people involved, and the environment.
Thee most widely quoted definition of sustainability, as a part of the concept sustainable development, is that of the Brundtland Commission of the United Nations. It was provided on March 20, 1987: “sustainable development is development that meets the needs of the present without compromising the ability of future generations to meet their own needs.”
However the neoliberal approach taps into the oft-quoted saying, “The richer get richer; the poor get poorer.” Power always gets in the way of fairness in the game of sharing. With ‘finite resources’, unfortunately there will always be winners and losers. For parties which claim to offer ‘comprehensive, free-at-the-point-of-need’ NHS, clearly it is impossible to square this particular circle.
Irrespective of the ageing population, which is a sensitive argument as it implies that aged individuals are a ‘burden’ on the rest of society despite the value that they have generated over their lifetime, “demand” appears to be fundamentally outstripping “supply”.
According to the 2008 revision of the official United Nations population estimates and projections, the world population is projected to reach 7 billion early in 2012, up from the current 6.9 billion (May 2009), to exceed 9 billion people by 2050.
In 2009, McKinsey says the NHS can save an initial £6bn-£9.2bn a year over the next three years through “technical efficiencies”. This produces a cumulative three year saving close to the £20bn NHS chief executive David Nicholson has been talking about since his annual report in May.
But the McKinsey report went further, suggesting the NHS could save a further £10.7bn a year on top by improving quality and shifting care to the most cost effective settings. Sir David Nicholson, as in effect the NHS’ CEO, grabbed the bull by the horns. Unfortunately, some Foundation Trusts have used ‘efficiency savings’ to run skeleton staff who are always a number of patients ‘behind’ in the Medical Admissions Unit or A&E.
According to a previous report from the National Audit Office, in 2011-12 there was a large gap between the strongest and weakest NHS organisations. The difference was particularly marked in London. At the time, there were 10 NHS trusts, 21 NHS foundation trusts, and three Primary Care Trusts (PCTs) reported a combined deficit of £356 million. The NAO estimated, based on their census of PCTs, that without direct financial support, a further 15 NHS trusts and seven PCTs would have reported deficits.
Sustainability is an issue in the Lewisham case (judgment here). Judge Silber remarked that on occasions it has proven impossible to improve speedily the performance of a failing NHS organisation sufficiently to secure an adequate quality of care for its patients within sustainable resources. For that reason, an exceptional bespoke procedure was introduced to deal with situations which arise,
At paragraph 3, Silber describes it as follows:
“in the words of a senior official of the Department of Health, Dr. Shaleel Kesevan, “where very occasionally it proves impossible to improve the performance of an NHS organisation sufficiently to secure adequate quality of care within sustainable resources”. This regime is entitled the “Unsustainable Providers Regime” (“the UPR”), which as its name shows was intended to deal with failing NHS organisations.”
It is clear then that some of the basic, actual, definition of ‘sustainability’ has got lost in translation. This is unfortunate given that the primary purpose of politicians, of all shades, should not to be to mislead the general public whether intentionally or unintentionally.
Above all, the NHS should be in touch with its wider environment. This does mean that the NHS should look to the forests or trees for inspirations. It means that when 50,000 protest lawfully in Manchester, there is no news blackout and people are genuinely concerned about why people are so upset.
It means listening to local residents in Lewisham. It does not mean instinctively using hardworking taxpayers’ money to appeal against a decision from the High Court in the Court of Appeal.
It also means listening to the views of nurses when they’re in a job, and listening meaningfully to them if you need to sack them. It is not as if the NHS is actually short of work to do, which is why some find it objectionable that there are staff cuts with ever-increasing demand.
That is the true meaning of ‘sustainable’. Unfortunately, the current Government is producing amendments to the insolvency regime to make neoliberal closures easier for the State, quicker than you can say, “Earl Howe”.
The NHS might be truly ‘sustainable’ if you pay especial attention to hardworking hedgies, as per the Royal Mail privatisation. To take the neoliberalisation of the NHS to the limit, you could sell it off as an initial public offering (or flotation). But is this another difficult choice the public are being shielded from?
The word “sustainable” has been bastardised. It has been taken away from its true meaning from the macroeconomics. Such abuse of language is symptomatic of an abuse of political power.
Many posts like this have originally appeared on the blog of the ‘Socialist Health Association’. For a biography of the author (Shibley), please go here.
Shibley’s CV is here.
