Home » Posts tagged 'Jeremy Hunt' (Page 2)
Tag Archives: Jeremy Hunt
Baroness Young’s furious letter: a Conservative smear campaign against Andy Burnham unravels
Baroness Young, a Labour Peer, was yet again “used” in a horrific smear campaign by the Conservatives last week over the Prof Sir Bruce Keogh Mortality Review. Needless to say, Baroness Young was not mentioned either in the Keogh mortality review.
This is an extract from Hansard.
The specific issue is about whether there was ministerial pressure, not the Civil Service.
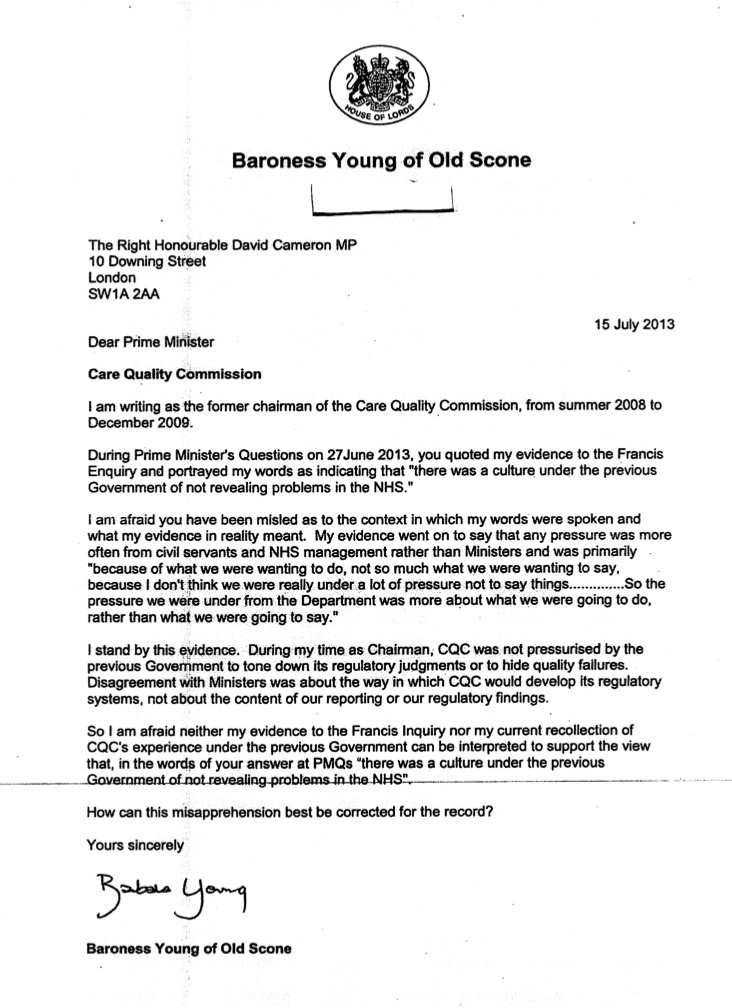
And this was Baroness’ Young furious reply to her previous mention in Prime Minister’s Question Time:
And, already, it is reported that Bruce Keogh privately apologised to Andy Burnham MP in yesterday’s Guardian:
“It is understood that Keogh was furious that his findings had been used to blame Labour for the unnecessary deaths of 13,000 patients, a figure that he did not recognise. Keogh was overheard apologising to Burnham, the former Labour health secretary at the centre of the attacks, when the two men were at government offices on Millbank, where the Sky and BBC political teams are based.
A source at the offices said Keogh told Burnham, “Andy, I’m so sorry”, and appeared to show his disgust at what Keogh described as a “political operation”. Burnham was overheard insisting that Keogh had “nothing to apologise for”, adding: “It’s a good report.””
Last week was a low-point in a vehement smear campaign against Andy Burnham MP. Jamie Reed MP has a done an excellent article for LabourList, entitled “The Anatomy of a Lie”. Twitter possibly saw the biggest brunt of it last week.
Standardised cigarette packaging policy: Lynton Crosby, Jeremy Hunt, public health and political lobbying
Ducks in a row
Jeremy Hunt, after a disastrous day in the House of Commons where he made a statement on the Keogh mortality report which bore little relation to the contents of that report, as Secretary of State for Health for England currently met up with Eddie Mair last night on Radio 4 on the ‘PM programme’. You can listen to his interview here (from 40 minutes).
Jeremy Hunt has a problem in denying that political lobbying has not had an effect in his policy over cigarette smoking. There have previously been allegations that Jeremy Hunt had 799 text messages with Rupert Murdoch’s lobbyist, and this was indeed a core focus of investigation in the infamous Leveson Inquiry on press regulation. The issue here is that Jeremy Hunt does not fundamentally disagree with the statement that, “There is limited evidence from Australia as to the effect of standardised packaging, so far, largely due to the short period of time since its introduction“. Eddie Mair had found that the views of the Department of Health bore an uncanny resemblance after their meeting with Philip Morris, a meeting which would have been considered unimagineable under Andrew Lansley, Mair proposes.
Jeremy Hunt was furthermore adamant that it is not a question about the “harm” which would occur if standard packaging were not introduced: Hunt was at pains to state the issue was whether it would “work”. This also has an uncanny resemblance to the briefing note of Philip Morris (New Zealand) on standardised cigarette packaging.
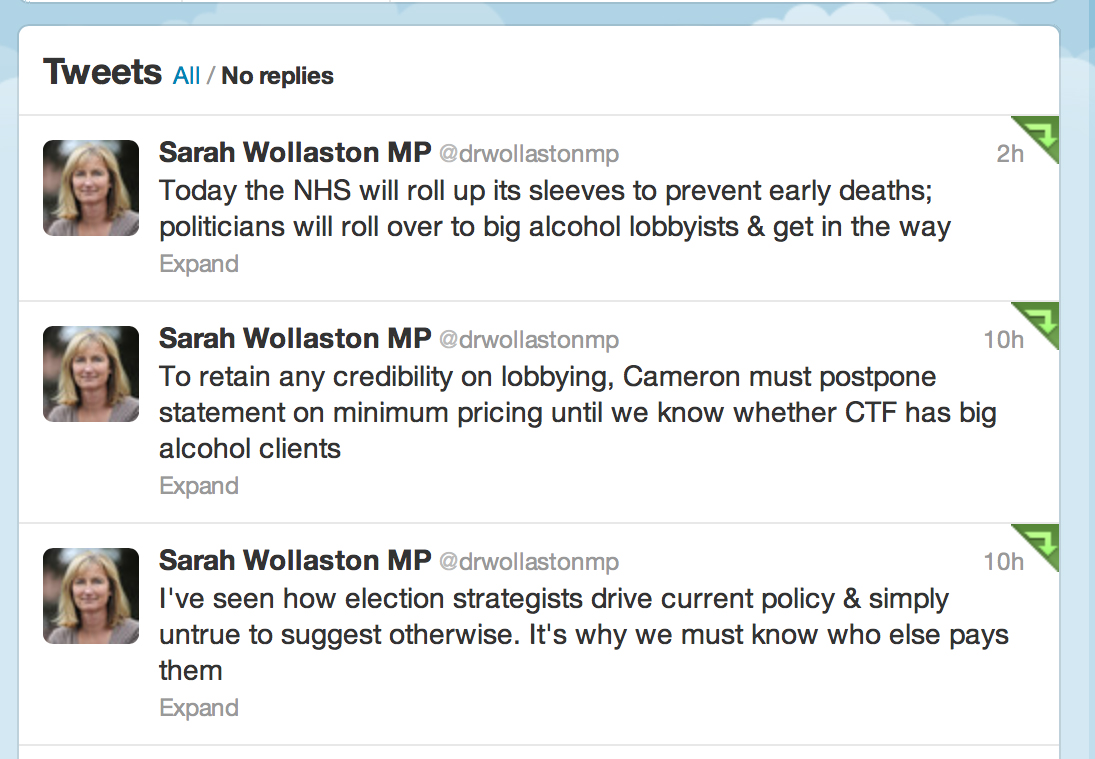
The question about Lynton Crosby is clearly relevant still, and is of concern even to Conservative MPs, especially Dr Sarah Wollaston (@drwollastonmp).
Eddie Mair: Turning to something which has killed far more people than all the failing hospitals put together. Tobacco, and I want to ask you about this… Do you agree that “cigarette smoking is the greatest single cause of illness and premature death in the UK”?
Jeremy Hunt: Yes I do.
Eddie Mair: Do you find much to disagree with in these words? Quote: “There is limited evidence from Australia as to the effect of standardised packaging, so far, largely due to the short period of time since its introduction“.
Jeremy Hunt: Yes.
Eddie Mair: You find.. You don’t find much to disagree with this statement?
Jeremy Hunt: Correct.
Eddie Mair: They are the words – direct quotes – of Philip Morris International at a meeting the company had with your officials [in the Department of Health] in January. We only know about this from a freedom of information request, of course. A few months later, your department is using very similar words to defend its decision to wait for further findings from Australia? Is there anything funny going on?
Jeremy Hunt: Not at all, and – I think – if I may say, it’s totally wrong for you to say that we’re taking ‘Philip Morris’ line’ because we’re not. We are..
Eddie Mair: You agree with it completely?
Jeremy Hunt: No – what I’ve said is .. I agree with that particular sentence, taken out of context. And by the way, I was not at that meeting. I don’t know what was said at that meeting?
Eddie Mair: Was Lynton Crosby at that meeting?
Jeremy Hunt: No, he was not – and I’ve never asked before you ask me, I can just tell you,
Eddie Mair: Please do not anticipate my questions. Will you stick to the ones I asked?
Jeremy Hunt: I’m happy to answer any questions you ask, Eddie. Let me say this. I am committed to doing what it takes to reduce the number taking up smoking. It is our number 1 killer, as you rightly said. However – and you need to let me answer – the reason we decided to wait for the evidence to come out of Australia is because these decisions are so legally fraught. If you don’t have the right evidence base, there’s a danger they can be overturned. There is a legal case going on in Australia at the moment. This is the Government which banned the display of tobacco behind counters. We’re absolutely committed to this agenda. We decided for such an important decision. We’re very committed to this agenda, but we need absolutely to “get our ducks in a row”. We want it to stick.
Eddie Mair: Why was Philip Morris in the room at all? Under your previous predecessor, Andrew Lansley, this would never happened. Or at least he said: “We won’t be engaging with tobacco companies on this. There is no common ground.” There’s no two ways about it – smoking kills and we have to do something about it. What was Philip Morris doing in the room at all?
Jeremy Hunt: I agree with Andrew Lansley. The advice from the Civil Service was fair, we did have to engage with all parties – doing something with the Department of Health, and for Ministers to authorise. To make the consultation process far, we had to engage with all parties. Their advice was if we didn’t engage was that any decision to introduce standardised packaging would be legally vulnerable, and that’s something neither you nor I want.
Eddie Mair: Does it help to get a meeting with your officials if the Conservative Party employed the person employed by a lobbying firm as you have done since last November?
Jeremy Hunt: Absolutely not and there’s no connection whatsoever.
Eddie Mair:
Jeremy Hunt: Well I can tell you he has never communicated with me, and I don’t know exactly whom he has communicated with outside me as I don’t know every single person he’s spoken to.
Eddie Mair: Will you check for us?
Jeremy Hunt: He has not been to any meeting in this department.
Eddie Mair: What harm do you think would be done by introducing standardising packaging without waiting for information from Australia?
Jeremy Hunt: It’s not a question about what harm would be introduced. It’s a question about whether it would work about reducing the number of people who take up smoking. That’s what you’re looking for evidence for. Given that there was a country that introduced this in January, we may not have to wait terrible long before seeing whether these measures work. It was on that business of waiting and seeing what the impact is that we decided that that was the sensible and prudent decision to make.
Eddie Mair: Why not say to the tobacco companies – we’re going ahead, we’re being bold, we’ll see if we’re wrong, and if so we can take us to court?
Jeremy Hunt: And if we took them in court and we lost, you’d be the first to invite me onto the show to say, “why didn’t you get your ducks in a row?”
Eddie Mair: You’re anticipating my questions again. This is lovely. Do you do lottery numbers as well?
[laughter]
Jeremy Hunt: No I don’t.
Eddie Mair: I want to ask you about one final thing. The Shadow Minister Lord Hunt has said he will try to force the Government to make an amendment.
Jeremy Hunt: He’s welcome to use any amendments he wants as a member of the Opposition. It’s his prerogative to use whatever parliamentary procedure he wishes. What I will say is this. The decision has not been made. We’ll be in a position to know whether it works. We’ve got a country next door which is piloting this. We won’t need to have any of these discussions, as I hope it’s clear to you, that if the evidence is strong, I will support the measure.
Eddie Mair: Jeremy Hunt, thank you.
To turn the CQC into a “NHS disaster” story is for some hitting a target but totally missing the point

Hitting the target, but missing the point?
Some very well known people have totally missed the point. They are supposed to be professional commentators or editors. What happened yesterday, with the publication of the long-awaited report by CQC, was not another NHS “disaster story”. Such a story is intended to make you want to go #facepalm at the thought of needing to go into a NHS Trust. It may even be a story to tell you that the NHS is not a “national religion“, and is a ‘sacred cow’ which ought to be sacrificed on the Hayek Altar of Privatisation.
No, I’m being very ironic.
The CQC was set up to expose problems in hospitals and care homes. It had far-reaching powers of inspection which allow it to order reforms or even close health services which put patients at risk. The interviews between James Titcombe and John Humphrys and David Prior, this morning, on the BBC Radio 4 programme are here. The CQC has been found, however, wanting in a drastic way yet again. The BBC TV programme Panorama broadcast evidence of mistreatment on residents of a Castlebeck hospital on May 31, 2011. Despite evidence concerning the same institution having previously been given to the Care Quality Commission, the body failed to act and has since admitted “an unforgivable error of judgment”. Major changes unsurprisingly have been made in the upper echelons of the Care Quality Commission, with a number of senior people leaving the organisation. According to “Caring Times”, its Director of finance and corporate services John Lappin announced he had a new post last year but agreed to stay on to finalise CQC’s budget for 2013/14 and deputy chief executive Jill Finney left CQC in February to take up a senior role in the private sector. Louise Guss, director of governance and legal services, was reported to be set to leave at the end of May, as was director of operations delivery Amanda Sherlock. Director of human resources Allison Beale will apparently leave in September. David Prior is now the Chairman of CQC; his biography is here.
In future, CQC hospital inspections will include 15-20 experienced people for a month, according to David Prior this morning. However, the report published this morning winded an already beleaguered NHS. Regulators apparently deleted the review of their failure to act on concerns about University Hospitals of Morecambe Bay NHS Trust, where police are investigating the deaths of at least eight mothers and babies. James Titcombe (@JamesTitcombe) and his wife, Hoa, arrived at the Furness General Hospital at Morecambe Bay, Cumbria, on 27 October 2008. Their son, Joshua, was born that morning. Nine days later, James Titcombe, a nuclear engineer from Barrow-in-Furness, tragically witnessed his son die. Midwives and medical staff at Furness General had failed to detect and monitor an infection, which became so serious that Joshua had to be transferred for intensive care at two different hospitals. Joshua died on 5 November. James has led a very public campaign for a public inquiry into “serious systemic failures” at the University Hospitals of Morecambe Bay Trust which manages Furness General. The horrific story is laid bare by James in this account here.
Kay Sheldon (@kayfsheldon), a director of the Care Quality Commission, also accused its senior managers of “deceit and evasion” in refusing to be straightforward about its failings. Kay sits on the CQC’s board as a non-executive director, and her role is to hold it to account. She has now spoken out, having refused to sign a wide-ranging gagging order in the wake of attempts to have her removed by the former chairman after she gave evidence about its failings to the Mid Staffs inquiry. James was asked about the situation now.
“… One of the key things is… One of the things I need to say John [Humphrys] is how amazingly grateful I am to Kay Sheldon as a non-executive Director. This report would not have come out if it were not for Kay. She was very courageous, and she faced what whistleblowers often face in the NHS, which is a vilification of their actions, ..in quite an appalling way. This report vindicates those concerns, and I think CQC – and David Prior to whom you’re talking afterwards – could demonstrate a commitment to the kind of the culture people want to see. David Prior could publicly reinstate Kay Sheldon and will remain on the board of CQC. That would go a long way. Other than that, I will judge the CQC how it will react in the next few weeks, and lays out its proposals how nothing like this can ever happen again.”
The chairman of the CQC, David Prior, who has been in the post for four months, said he was “desperately sorry” that the situation had arisen.
Particularly in the aftermath of the global financial crisis, all the international financial regulators have reciprocal relationships to help them conduct their duties of public protection by sharing information. Any lack of sharing of information in a facilitatory way may be a fundamental barrier to effective regulation in healthcare, and time will tell. Prior said that,
“Unbeknown to us there was an investigation being held by Pauline Fielding which had been going on for four months, and found the maternity service was dysfunctional and unsafe. Her report was not finished at the time. We were not set up then and we are now set down to inspect hospitals…Our job is to inspect hospitals. We sent people in who had not worked in a hospital before. How could they do a proper job? We have been in the job of giving reassurances to the public.”
Among the various findings, the CQC was “accused of quashing an internal review that uncovered weaknesses in its processes“. David Prior was asked this morning by John Humphrys why one person in the CQC was asked to “destroy” evidence, to which Prior said that the “management board was dysfunctional.”
“I had known for a few months that we were not ‘fit for purpose’ as far as hospital inspections are concerned.”
Humphrys asked repeatedly if anybody who had left CQC were “punished”, and Prior said no. This issue of people moving on from failures in one job in NHS management to get a highly paid job elsewhere continues to haunt the NHS. Caroline Molloy very recently on the ‘Our NHS’ blog has described how this phenomenon has gathered momentum pursuant to the Health and Social Care Act (2012):
“In an increasingly marketised system, the opportunities for financial conflicts of interests are clear. It is curious that the media has chosen to focus on the conflicts of commissioning GPs. Whilst problematic, the sums involved are dwarfed by the huge fortunes to be made by the corporate clients of the big four currently embedding themselves at the heart of policy making.”
In August 2012 David Behan, chief executive of CQC, commissioned a report by management consultants, Grant Thornton. Names of those accused of a cover-up within the CQC were removed from this report. Humphrys explictly asked why the names in this Report had been redacted. Prior answered, “We had to make the decision on Friday to not publish the Report or publish the Report with the names, but we would have been breaching the Health Protection Act.” However, @dbanksy later on Twitter reported that:

Anyone who knows how English law works will know that the English law is there for all parties to interpret freely. A person will pay for legal advice, instruct the lawyer according to what result he or she wants. If a party were to instruct a lawyer to protect the identities of certain individuals, rather than to disclose a narrative which is clearly in the ‘public interest’, that would be perfectly possible. It would also be perfectly possible to instruct a different lawyer with different instructions. Get this – Hunt can sue the CQC if he wants. The NHS and CQC are not the same thing, shock horror!
Incredibly, some accounts failed to mention even Kay Sheldon, a key member of all this. James Titcombe was incredibly impressive as ever, in articulating what is clearly not a vendetta against the NHS, but an earnest desire for everyone in the NHS to learn from its mistakes. There are issues about what happened to Kay’s opinions, why healthcare regulators appear to coordinate poorly their regulatory inquiries, and the concerns of Kay Sheldon and a similar band of people Dr Heather Wood, David Drew, Dr Kim Holt, who have become sacrificial lambs in the whole cathartic process. People who whistleblow tend never to work again in the #NHS, and, for all the heroism, their opinions are marginalised at best, at worst ridiculed and humiliated. This episode is very clearly a debate about the efficacy of healthcare regulation. There is an urgent question to be had about the efficacy of the CQC’s regulation: why does England persist with a non-specialist “one size fits all” generic method of regulation in some parts? To have turned this into a privatisers’ charter was perhaps hitting the target for some, but missing the point, I feel.
How not to lead in a crisis: Jeremy Hunt and A&E

Earlier this week the King’s Fund warned that waiting times for A&E patients had hit a nine-year high and the number of people waiting more than four hours to see a doctor had almost doubled since last year.
Jeremy Hunt is supposed to be the “leader” in the “A&E crisis“, having just been recruited to implement a £3bn reorganisation of the NHS which, historically, has been opposed by all the Medical Royal Colleges.
Mayor Mike Bloomberg, who won a third term, and is widely regarded as an adept city leader, but came under fire for inefficient snow removal in New York City. Most of the complaints came from residents in the so-called outer boroughs — e.g., the four that are not Manhattan. However, Newark Mayor Cory Booker has received acclaim for his response to his snowfall, despite accepting criticism on a host of other matters.
Some failures can be useful if leaders learn from them, according to Robert Mittelstaedt, Dean of Arizona State University’s business school. The three biggest causes of failures he sees are not believing data, disregarding new phenomena, and not taking responsibility for problems. Hurricane Katrina holds plenty of those lessons, according to Mittelstaedt. He points out that for years a wealth of information was available that New Orleans could not withstand a major storm, but officials didn’t act on the data. Officials then ignored information about the scope of suffering by those stranded in the city. He blamed President Bush and others for not taking responsibility and instead arguing about whose job it was to rescue people. “When you see people on rooftops, you don’t sit around worrying about whose responsibility it is,” according to Mittelstaedt.
Erika Hayes James, an organisational psychologist at the University of Virginia’s Darden Graduate School of Business,categorises five phases of crisis that require specific crisis leadership competencies in “smoldering crises“. Smoldering crises differ from sudden crises in that they begin as minor internal issues that, due to manager’s negligence, develop to crisis status. These are situations when leaders are blamed for the crisis and its subsequent effect on the institution in question. Each phase contains an obstacle that a leader must overcome to improve the structure and operations of an organisation. James’s case study on crisis in the financial services sector, for example, explores why crisis events erode public trust in leadership. James’s research demonstrates how leadership competencies of integrity, positive intent, capability, mutual respect, and transparency impact upon the trust-building process.
John Baldoni (2011) in the Harvard Business Review views that important lessons can be derived from how a ‘good leader responds to a crisis’.
- Take a moment to figure out what’s going on. The problem is that everything under the sun has been blamed for the crisis, apart from the current operations management of this Coalition, by Jeremy Hunt. Reasons cited by Hunt have included winter, “The UK Labour Party”, immigrants, women GPs, and targets. To compound the farce which has been “the blame game”, Stephen Dorrell, the Tory chair of the health select committee, very publicly disagreed with Hunt recently, over linking the crisis in A&E departments to GPs opting out of working nights and weekends.
- Act promptly, not hurriedly. A leader must provide direction and respond to the situation in a timely fashion, but acting hurriedly only makes people nervous. However, it is really in dispute whether Hunt in fact acted promptly. According to Jamie Reed MP, a recent Freedom of Information request submitted to the Department of Health shows that Jeremy Hunt had spent six months as Health Secretary before visiting his first A&E unit. When he finally got around to it, the A&E unit he visited was only yards from his own office.
- Manage expectations. When trouble strikes, people want it to be over right now — but seldom is this kind of quick resolution possible. It falls to the leader in charge to address the size and scope of the crisis. You don’t want to alarm people, yet do not be afraid to speak to the magnitude of the situation. Winston Churchill was a master at summing up challenges but offering a response at the same time. As he famously stated in 1940, when assuming office, he said,”You ask, what is our aim? I can answer in one word. It is victory; victory at all costs; victory in spite of all terror; victory, however long and hard the road may be, for without victory there is no survival.” However, the plan proposed by Hunt is neither decisive or prompt. He has announced a fundamental review of emergency care, conceding that “we have failed to give the public confidence that there’s anything between GP surgeries and A&E”. The review, which will result in action by next April, will focus on “vulnerable older people”, whom Hunt said were the heaviest users of the NHS. However, at least the review will not be a panicked response.
- Demonstrate control. When things are happening quickly, no one may have control, but a leader can assume control. That is, you do not control the disaster — be it man- made or natural — but you can control the response. This is a man-made crisis. Unfortunately, there’s an element that Hunt is still in denial over this crisis, with him having only a few hours ago tweeted:

- Keep calm. A hallmark of a crisis is its ability to change quickly: “your first response may not be your final response.” In these situations, a leader cannot be wedded to a single strategy. He or she must continue to take in new information, listen carefully and consult with the frontline experts who know what’s happening. However, his first response was to blame GPs, and this has been rebutted very robustly by the Royal College of General Practitioners. Hunt has been forced to back-track on this as the evidence to support him simply not there.
And above all Jeremy Hunt has offended the first rule of crisis leadership: he has not taken responsibility for the crisis personally, nor vicariously on behalf of the current government.
Jeremy Hunt says that ‘NHS 111′ is now “up-and-running”, but that targets should not be gamed

The reality is that the vast majority of hospitals in the NHS are currently failing to see 95% of patients within four hours. Jeremy Hunt was interviewed on the BBC ‘The Andrew Marr Show’ this morning in a wideranging interview which also covered membership of the European Union.
Jeremy Hunt first underplayed the severity of the NHS 111 fiasco, but claimed that things are better now. Of course, one tragedy in care is one too many. The NHS says it has experienced seven “potentially serious” incidents in the first few weeks of its 111 urgent care helpline in England. One case involved a patient in the West Midlands who died unexpectedly and there have been reports of calls going unanswered and poor advice being given. All the cases are being reviewed. Other organisations are also running 111 lines for NHS England and have been warned they must deliver good care or face financial or contract penalties.
In 2010, critics had claimed the change from NHS Direct to NHS 1111 would undermine the quality of the service by reducing the number of qualified nurses answering calls, but chief executive of NHS Direct Nick Chapman said that new helpline would be better and more cost effective.
Jeremy Hunt, meanwhile, this morning stated, “There are short-term pressures and long-term pressures. We did have teething problems with NHS 111. It is up-and-running now in 90% of the country. We need to have better alternatives in primary care, a better personal relationship between patients and their GPs”.
“Under the last government, we had a culture of ‘hitting targets at any cost’.” Hunt then went onto blame ‘the target culture’ for bringing about the problems which Mid Staffordshire NHS Foundation Trust had faced, leading to two inquiries by Sir Robert Francis QC.
Hunt further added that, “I would never blame GPs, because they work extremely hard. I have just been in one.”
Of course, nobody reasonable, seriously, would take the blindest bit of difference of Hunt comparing his brief time work experiencing in a GP surgery to seven years of basic medical training, including pre-registration training, even prior to specialist GP training.
GPs have experienced a number of contractual changes over time (described here), and latterly it has been mooted that the personal income of GPs, following the latest change, has been steadily eroded as funding levels have been frozen, whilst the running costs of surgeries and staff pay have increased.
Hunt further provided this morning, “That Contract is one of the contributing causes, because after hours and at weekends the service deteriorates. I don’t want to go back to those days where GPs are personally on call at 2 am.”
Hunt added that, “GPs should have responsibility that people on their list have a good service.”
It is difficult to see what exactly Hunt means by this, as it is hard to separate out the effect of a medical decision taken out-of-hours compared to a decision compared to during ‘conventional hours’, and one assumes that each Doctor is still responsible for his/her own medical actions to the General Medical Council, wherever he or she provides care.
Hunt then gave a response which managed to combine a welcome for targets in improving care, with direct criticism of those managers clearly gaming the system.
Regarding the A&E target, Hunt opined, “It is a very important target, and we have never said we do not have to have good targets. We don’t want people to follow targets at any cost.” However, he then described a series of measures how managers would then ‘game’ the system.
“We had beds which hadn’t been cleaned, ambulances circling hospitals before they entered the front door because they didn’t want the clock the start.”

Jeremy Hunt says that 'NHS 111' is now "up-and-running", but that targets should not be gamed

The reality is that the vast majority of hospitals in the NHS are currently failing to see 95% of patients within four hours. Jeremy Hunt was interviewed on the BBC ‘The Andrew Marr Show’ this morning in a wideranging interview which also covered membership of the European Union.
Jeremy Hunt first underplayed the severity of the NHS 111 fiasco, but claimed that things are better now. Of course, one tragedy in care is one too many. The NHS says it has experienced seven “potentially serious” incidents in the first few weeks of its 111 urgent care helpline in England. One case involved a patient in the West Midlands who died unexpectedly and there have been reports of calls going unanswered and poor advice being given. All the cases are being reviewed. Other organisations are also running 111 lines for NHS England and have been warned they must deliver good care or face financial or contract penalties.
In 2010, critics had claimed the change from NHS Direct to NHS 1111 would undermine the quality of the service by reducing the number of qualified nurses answering calls, but chief executive of NHS Direct Nick Chapman said that new helpline would be better and more cost effective. Jeremy Hunt, meanwhile, this morning stated, “There are short-term pressures and long-term pressures. We did have teething problems with NHS 111. It is up-and-running now in 90% of the country. We need to have better alternatives in primary care, a better personal relationship between patients and their GPs”.
“Under the last government, we had a culture of ‘hitting targets at any cost’.” Hunt then went onto blame ‘the target culture’ for bringing about the problems which Mid Staffordshire NHS Foundation Trust had faced, leading to two inquiries by Sir Robert Francis QC. Hunt further added that, “I would never blame GPs, because they work extremely hard. I have just been in one.” Of course, nobody seriously would take the blindest bit of difference of Hunt comparing his brief time work experiencing in a GP surgery compared to seven years of basic medical training, including pre-registration training, even prior to specialist GP training.
GPs have experienced a number of contractual changes over time (described here), and latterly it has been mooted that the personal income of GPs, following the latest change, has been steadily eroded as funding levels have been frozen, whilst the running costs of surgeries and staff pay have increased. Hunt provided this morning, “That Contract is one of the contributing causes, because after hours and at weekends the service deteriorates. I don’t want to go back to those days where GPs are personally on call at 2 am.”
Hunt added that, “GPs should have responsibility that people on their list have good service.” It is difficult to see what exactly Hunt means by this, as it is hard to separate out the effect of a medical decision taken out-of-hours compared to a decision compared to during ‘conventional hours’, and one assumes that each Doctor is still responsible for his/her own medical actions to the General Medical Council, wherever he or she provides care.
Hunt then gave a response which managed to combine a welcome for targets in improving care, with direct criticism of those managers clearly gaming the system. Regarding the A&E target, Hunt opined, “It is a very important target, and we have never said we do not have to have good targets. We don’t want people to follow targets at any cost.” However, he then described a series of measures how managers would then ‘game’ the system.
“We had beds which hadn’t been cleaned, ambulances circling hospitals before they entered the front door because they didn’t want the clock the start.”
The big NHS underspend: Andy Burnham writes to Jeremy Hunt
This is the rather dramatic start of the HSJ article yesterday:

At a time of a huge financial squeeze being put on hospitals and when treatments of all sorts are being cut or delayed (or “rationed”), it turns out that the Department of Health – the unit in charge of the NHS – has a huge surplus that it is returning to the Treasury.
Andy Burnham MP has written to Jeremy Hunt MP as follows.
Dear Jeremy
NHS Budget underspend
Figures published today by the NHS Information Centre show that in December 2012 there were 4,887 fewer nurses working in the NHS than in May 2010. This followed the Care Quality Commission Care Update, published earlier this month, which warned that 11% of hospital services inspected were failing to meet the standard on adequate staffing levels.
You can therefore imagine my surprise when reading figures published in the detail of the Budget document yesterday that show the Department of Health is expected to underspend against its 2012-13 expenditure limit by £2.2bn.
Furthermore, the table on page 70 of the Budget document appears to show that none of this has been carried forward to be used in subsequent financial years as part of the Budget Exchange programme.
At a time when the NHS is facing its biggest financial challenge, when almost 5,000 nursing posts have been lost since the general election, and when one in ten hospitals are understaffed, I find it staggering that £2.2bn of the NHS budget is to be returned to the Treasury.
It would be helpful if you could therefore answer a number of important questions.
1. Were you aware of the £2.2bn underspend before yesterday and did you authorise the decision not make any use of the Budget Exchange programme? Or were you overruled by the Treasury?
2. If so, when did you make your decision?
3. Can you confirm that this means the Department’s underspend for 2012-13 would be 2%, higher than the 1.5% figure that your Department says is consistent with “prudent financial management”?
4. Do you accept the recent findings of the Care Quality Commission that one in ten hospitals are failing to meet the CQC standard on adequate staffing levels? Did you consider this when making your decision?
5. Why did you not make use of this underspend to prevent job losses and ensure all hospitals have adequate staffing levels?
6. Yesterday, a Department of Health spokeswoman told the Health Service Journal that the NHS underspend would “still be available for NHS organisations to ensure high quality, sustainable health services are delivered to patients now and in the future”. Can you confirm that this will not be the case, as none of the £2.2bn underspend has been carried forward for future use?
I look forward to your response.
Best wishes
Rt Hon Andy Burnham
The plot thickens…

efficiency savings

The big NHS underspend: Andy Burnham writes to Jeremy Hunt
This is the rather dramatic start of the HSJ article yesterday:
At a time of a huge financial squeeze being put on hospitals and when treatments of all sorts are being cut or delayed (or “rationed”), it turns out that the Department of Health – the unit in charge of the NHS – has a huge surplus that it is returning to the Treasury.
Andy Burnham MP has written to Jeremy Hunt MP as follows.
Dear Jeremy
NHS Budget underspend
Figures published today by the NHS Information Centre show that in December 2012 there were 4,887 fewer nurses working in the NHS than in May 2010. This followed the Care Quality Commission Care Update, published earlier this month, which warned that 11% of hospital services inspected were failing to meet the standard on adequate staffing levels.
You can therefore imagine my surprise when reading figures published in the detail of the Budget document yesterday that show the Department of Health is expected to underspend against its 2012-13 expenditure limit by £2.2bn.
Furthermore, the table on page 70 of the Budget document appears to show that none of this has been carried forward to be used in subsequent financial years as part of the Budget Exchange programme.
At a time when the NHS is facing its biggest financial challenge, when almost 5,000 nursing posts have been lost since the general election, and when one in ten hospitals are understaffed, I find it staggering that £2.2bn of the NHS budget is to be returned to the Treasury.
It would be helpful if you could therefore answer a number of important questions.
1. Were you aware of the £2.2bn underspend before yesterday and did you authorise the decision not make any use of the Budget Exchange programme? Or were you overruled by the Treasury?
2. If so, when did you make your decision?
3. Can you confirm that this means the Department’s underspend for 2012-13 would be 2%, higher than the 1.5% figure that your Department says is consistent with “prudent financial management”?
4. Do you accept the recent findings of the Care Quality Commission that one in ten hospitals are failing to meet the CQC standard on adequate staffing levels? Did you consider this when making your decision?
5. Why did you not make use of this underspend to prevent job losses and ensure all hospitals have adequate staffing levels?
6. Yesterday, a Department of Health spokeswoman told the Health Service Journal that the NHS underspend would “still be available for NHS organisations to ensure high quality, sustainable health services are delivered to patients now and in the future”. Can you confirm that this will not be the case, as none of the £2.2bn underspend has been carried forward for future use?
I look forward to your response.
Best wishes
Rt Hon Andy Burnham
The plot thickens…

Instead of “coasting clinicians”, target your wrath at those mediocre meddling managers

“Great spirits have always encountered violent opposition from mediocre minds.” Albert Einstein
Not all managers are ‘mediocre and meddling’ but some are. I was told by a English NHS consultant last night how nurses in his outpatients clinics are now clocking him in and clocking him out, and gives him permission to leave the clinic when he’s done his allotted time, instead of frontline nursing. Also, he is now expected to stay on site in his 40s during certain hours at night. This has actually caused much resentment across the Consultant workforce in his Trust, such that the managers bombed in their recent staff survey apparently. But these results are not going to be made public. It is easy to target ‘coasting’ from clinicians in the NHS, but it is overwhelmingly clear there are hotspots of meddling, mediocre poor management in the NHS, of overpaid NHS managers making the wrong decisions, but making the wrong decisions quite efficiently for their generous salary. That is why they will never become leaders.
One good aspect about the Francis Report is that the NHS seems to be able to tolerate failure. Failure on quite a large scale – distressed relatives of loved-ones who saw patients drinking water out of flower vases, and clinical regulatory authorities which have yet to make a single sanction years down the line. For all the discussion about the independence and autonomy of entities within the National Health Service, as the toxic culture which might have caused this disaster appears so widespread, it has been argued that there is little point in ringfencing the blame. The problem with this approach is that it is possibly tantamount to be giving up on ‘contagion’, and indeed it is most unlikely that Mid Staffs represents an isolated locus of pathology within the NHS. There is still the unresolved issue about the use of ‘gags’ and ‘supergags’, paid for through the tax payer, of NHS managers, and an overall acceptance that we have to put up with a culture of mediocrity in management in the NHS.
It is very hard to think of ‘great managers’ in the NHS, partly because managers are supposed to be doing things right rather than being identified for doing the right things. Therefore, you are more likely to identify a “good manager” because a disaster has not happened. And yet you never hear of anyone (who isn’t on the NHS graduate management scheme) who says, ‘Yeah, I really want to be a NHS manager’. Compared to a leading cardiologist or brain surgeon, nobody says, ‘I want to be the next David Nicholson’. This is because David Nicholson can be said to be the epitome of ‘coasting'; of someone who is virtually unsackable, as he is surrounded by too many ‘supporters’ in the establishment who ‘need’ him to implement these unpopular, costly, flawed reforms. Whilst the salary for junior doctors is far worse, and the conditions considerably worse (for example a week of nights, often carrying ‘the arrest bleep’), junior doctors on-the-whole are highly motivated people. This of course will be unknown to Jeremy Hunt, who never trained in the NHS, or many on the corporate healthcare lobbying circuit, but this is the reality of gifted people in the NHS. If anything, the brilliance of these junior doctors has been potentially suppressed by relatively poor pay for anyone who has completed effectively a seven-year intensive degree, and the sheer knowledge and skills required to ‘make it’ in medicine far outweighs those needed to command a bonus as an investment banker.
It is not uncommon for junior physicians who wish to train with the “best”, for example be on the clinical firm of Sir Richard Thompson, President of the Royal College of Physicians, in gastroenterology, or Professor Sir Ian Gilmore, the previous President, a hepatologist. However, the mediocrity culture of management is striking here. People who want to train with Sir David Nicholson probably do so more because they consider themselves using it as a passport to getting a well-paid position in the NHS, rather than the fact they wish to ‘train with the best’. Indeed, if you wished to be superb in management in the NHS, many younger people would prefer to do a sabbatical in Harvard Business School, and work with someone like Professor Clay Christensen, Professor of Innovation at Harvard, or Professor Michael Porter, Professor of Strategy at Harvard, than work with Sir David Nicholson. This is possibly an unintended consequence of a deep-seated ethos of mediocrity in NHS management.
When you look at the actual business management and leadership literature, you can see immediately the intimate relationship between leadership and dissipation of mediocrity. Take for example the effect of Fox Conner on a young Eisenhower; Fox Conner is a shining example of ‘one-to-one’ nurturing of a junior talent by somebody senior who wished to give up some of his time. Conner first met Eisenhower in 1919 at the Infantry Tank School at Camp Meade and the two men immediately developed a great mutual respect. Following his promotion to brigadier general in the Regular Army April 27, 1921, Conner took command of the 20th Infantry Brigade in Panama. He invited Eisenhower to join his staff and for three years Conner conducted a systematic course of study for Eisenhower that ranged from extensive readings in military history to daily practical experience writing field orders for every aspect of the command.
Mediocrity was probably at most about a sixth of Jeremy Hunt’s famous speech. However, it has generally been interpreted as a demoralising influence on the workforce of the NHS at a critical time, from a person who is known to have said disparaging things about the NHS, and who indeed is reputed to have not wanted the Danny Boyle item in the Olympics ceremony which he raved about at the beginning and end of that speech. The problem was that Hunt cames from a position of low integrity in criticising the medical profession. He has never worked as a medical professional in the NHS, so has no moral fitness-to-criticise about mediocrity in the NHS. Furthermore, he didn’t as such offer any solutions. This is exactly akin to a GP who tells you you have a cancer, but changes subject before he or she gets a chance to tell you about a possible treatment. Maybe this is because Jeremy Hunt knows the problems over his treatment: there is no Fox Conner figure to look up to. There is a plethora of people who’ve done the Jeremy Hunt job, like Hewitt, Dobson or Milburn, but who have not been there for a very long distance; they can perhaps offer their ‘expertise’ elsewhere. These are people who are unlike the junior doctors who qualify into the NHS at the age of 24 and possibly become Consultant at the age of 40. Secondly, Hunt cannot point to a single NHS manager who is not mediocre; who is a great visionary, or who has been known to be NHS management equivalent of Fox Conner. To be honest, Hunt has very little experience in NHS management himself, but this may be a growing trend in how the UK is run (take for example the report of a headteacher at the weekend who has never taken a lesson, indeed cf the Secretary of State for Education.)
Of course, these criticisms do not, in themselves, invalidate Jeremy Hunt’s argument. One of the major problems that the NHS, whilst it cannot be elevated to a position of immunity from criticism, is repeatedly cited as one of the most efficient health systems in the world; for example the US which spends much more has worse outcomes. And the corollary of this is that there is plenty of mediocrity in the private sector; indeed many ‘fat cats’ are truly ‘coasting’ as their shareholder dividends rocket from a flatlining performance in a market where it is impossible to fail (such as privatised gas, water, or telecoms). But medicine and nursing are professions, and Hunt’s language is inappropriate, because pervasive in Hunt’s thinking is that he treats medicine and nursing as commodities, parts of which can be readily packaged for private equity companies to make a ‘fast buck’. That is the distorted perverted concept of ‘wealth creation’, popular with some. That is possibly the biggest threat to the NHS becoming ‘mediocre’, and restoring dignity to a battered pair of professions at a time when they have been undermined by a complex reform they never asked for, would help to motivate its workforce. Calling them ‘mediocre’ from a position of relatively little authority, however, is utterly futile.

Andy Burnham MP's letter to Jeremy Hunt MP following comments by Sir David Nicholson

The letter below has been sent below by Andy Burnham MP to Jeremy Hunt MP, following the astonishing remarks by Sir David Nicholson as reported here in the Observer. The reforms have cost about £3bn, it is reported, at a time when the UK economy has been managed poorly. The Nicholson Challenge is certainly an admirable ’cause’ of finding efficiency savings in the NHS, but clearly difficult when you have to spend billions on a massive top-down reorganisation, spending money like simply pouring money down a drain. Andy Burnham MP would be failing in his duty in Shadow Secretary of State for Health if he did not draw attention to these issues, and it is of course open to Jeremy Hunt MP to admit, deny or put-to-proof any of the specific points therein.
Dear Jeremy,
I was astonished to read in today’s Observer that the man charged with implementing your Government’s re-organisation of the NHS has serious doubts about it and fears it could end in “misery and failure”.
Right now, the NHS is in a dangerous position, facing unprecedented financial and organisational upheaval. As I am sure you will appreciate, the timing of these comments from the Chief Executive of the NHS, David Nicholson have the potential to increase the growing crisis of confidence in your Government’s reforms.
We already knew that there was widespread professional concern about your re-organisation but it is now clear it goes right to the top of the Department. To reduce any potential for confusion, I would be grateful if you could set out whether David Nicholson has raised his concerns directly with you and, as a result, whether you will make any changes to the plans you inherited from your predecessor?
One of the most serious concerns David Nicholson raises is the warning against “carpet bombing” the NHS with competition – a clear reference to the enforced open tendering of NHS services under the Any Qualified Provider process.
In Labour’s recent NHS Check report, we revealed the accelerating pace and scale of competition in the NHS. 396 separate community services have been forced out to competition under the first wave of AQP. Despite promising to put clinicians in the driving seat, your Government has ordered PCTs to put successful services out to tender – in many cases, against their stated plans.
Worryingly, before any evaluation of the first round of AQP, you are now planning a major expansion of the policy with a further 39 services opened out to competition before next April.
I have major concerns about this rapid expansion and its potential to de-stabilise successful NHS services – and it now appears my concerns are shared by the Chief Executive of the NHS.
In light of these comments, and to bring some stability to the NHS, I believe there is now a clear case for the suspension of the next wave of the Any Qualified Provider process, pending a full review of wave one and the effect it has had on existing services and quality of patient care.
I ask you to give this sensible proposal serious consideration. David Nicholson’s comments are a stark reminder of the gamble your Government is taking with the NHS and should provide pause for thought.
Best wishes
RT HON ANDY BURNHAM MP
