Home » Posts tagged 'David Cameron'
Tag Archives: David Cameron

Another 5 years of David Cameron? I really hope not.

What is most intriguing in the in-depth analysis of Ed Miliband as Prime Minister is that most people I know would rather emigrate from the UK rather than to face another five years of David Cameron.
David Cameron has presided over an unbelievable mess in welfare benefits. I’ve lost count of people including myself who suddenly had their welfare benefits stopped (in my case disability living allowance due to physical disability), who just ‘fell off’ the benefits register. I had to have two appeals, and then go to a tribunal, before I was restored to the benefit I had received previously. And in the meantime there had been absolutely no improvement in my disability symptoms.
David Cameron has presided over an economy which works well for the very wealthy – but this is a dangerous time to be vulnerable. It is sheer bare faced cheek to claim the economy is healthy when it can’t muster enough tax receipts to keep public services going. A record number of people in employment, with a growing population in the UK, is short shrift for a society which cannot pay benefits in a timely manner such that a record number of people has to go to food banks. This is precisely what you get when you a bargain basement low wage economy, fuelled by zero hour contracts, with slashing of employment rights.
The Conservative narrative is a highly fraudulent one. Shortly before Lehman Brothers crashed, George Osborne had been boasting about how he would match Labour on spending commitments. So far from giving keys back to the driver who crashed the car, Osborne was the co-driver. Osborne wrote in ebullient terms about the deregulated Iceland – the one which crashed big time. It’s simply a pack of lies, needed to produce a malnourished State of public services, whereas corporates still get their cushy state handouts – such as proceeds from the privatisation of Royal Mail. This time, the Liberal Democrats, under Nick Clegg and Danny Alexander, have been first in the queue chanting repetitively their pack of lies.
David Cameron’s cardinal sin was never to mention the devastating £3 billion reorganisation of the NHS. This four hundred page piece of law, only made possible with the Liberal Democrats on the accelerator pedal not the brake, did not have a single clause on patient safety (apart from abolition of the National Patient Safety Agency). It was the wrong piece of law at the wrong time. With social care on its knees, it did nothing to make the health and care systems fit for purpose. Hospitals simply cannot discharge NHS patients in a timely fashion to social care currently. Add on top of this the chaos in A&E waits, it’s now a case that individuals cannot both enter hospital and cannot leave hospital. The NHS simply could not cope with another five months of this utter mess, let alone another five years under David Cameron.
Cameron and Hunt have presided over a disastrous NHS. How dare they.
But the legislation was not a waste of time for the people who have been behind this Government every step of the way. Lurking in the shadows of ‘The Big Society’ are the big private equity backers. They’re the ones who have controlling stakes in private finance initiative hospitals which they can slept a profit. Eye watering contracts of NHS services are being flogged off to the private sector. Even the late Harold Macmillan, a previous Tory prime minister, resented the selling off of the ‘nation’s silver’ under the prime successor, Margaret Thatcher. Privatisation is simply transfer of resources from the public sector to the private sector. You’d have to be an idiot not to understand that.
Somebody who is far from an idiot, Oliver Letwin, has explained the critical rôle of outsourcing of services (source here).
Just in case there is a hung parliament it’s become vital to think who could prop up another failed Tory administration. Vote for Alex Salmond or Nick Clegg at your peril.

Concerns about the paired associates learning test for dementia
To begin to understand how a cathode-ray TV set works, I could remove one component called the “transistor”, and the picture disappears. It would be an incorrect conclusion to say that the purpose of that transistor is to produce the picture. However, I could argue correctly that the transistor was somehow part of the system required to produce the picture.
If I showed the transistor was particularly “hot” while the TV set was on, producing a picture, it might be reasonable for me to conclude the transistor was involved in producing the picture.
This is the sort of basic approach still used to work out what is going on in the brains and minds of people with Alzheimer’s disease, typical presentations of which might be memory problems. You can see whether removing parts of the brain in humans produces similar effects to the problems in thinking found in Alzheimer’s disease. Or alternatively, you could just try to look at the system of components in the brain which might be contributing to memory in brains working normally.

Whatever, it’s a puzzle. In this particular case, it’s a puzzle to solve correctly.
An innovation culture in the diagnosis of Alzheimer’s disease
David Cameron praised Cambridge Cognition’s work in developing new innovative tests for Alzheimer’s disease in the G8 summit held towards the end of last year.
There has been concern that some individuals with Alzheimer’s disease do not receive their diagnoses in a particularly fast way. A number of explanations for this have been offered, including medical personnel not being able to spot the symptoms of Alzheimer’s disease easily.
It is also helpful to understand what an “innovation” is. An innovation might be a product which enables you do something much more easily, and depends for its success popular uptake by the user. Strictly speaking, paper was an innovation too. However, the rise in cost of diagnosing Alzheimer’s disease, arguably, is an intriguing example of “Baumol’s cost disease“.
Individuals with Alzheimer’s disease have memory problems which are typically not thought to be qualitatively similar to those found in ageing elderly individuals. Often such people have real problems in navigating around environments. It is clearly a very laudable aim to have a bedside test which might be able to alert a physician to an underlying memory problem in Alzheimer’s disease.
The benefits and concerns, and my passing involvement
There are a number of important caveats here. Not all dementias are Alzheimer’s disease. There are in fact hundreds of dementias, some of which are reversible. Whatever test is used, the test should be sensitive enough to identify reliably a genuine thinking problem in Alzheimer’s disease, but should not be so ‘broad brush’ the test also misattributes memory problems, say found in the ‘mild cognitive impairment’ or even depression, to Alzheimer’s disease. Such mislabelling can perceivably cause distress, and cause people to be caught up in the medical system for further lengthy tests when they should not have been in the first place. On the other hand, it is of concern that the diagnosis might be missed in some people, and hence the drive from the Department of Health and the Alzheimer’s Society in “The Prime Minister’s Dementia Challenge”.
I wish Cambridge Cognition well, not least because I have worked with CANTAB whilst a graduate student at the University of Cambridge. In fact, some of my papers are cited in their bibliography. Their search facility is here.
The CANTABmobile “paired associates learning” test
To explain the “paired associates learning” test from first principles, and I’m not using actual screenshots, imagine me presenting you with a number of blank boxes dotted around the screen.

And I open each box in turn and reveal a shape to you. I can present the problem with a varying number of shapes.

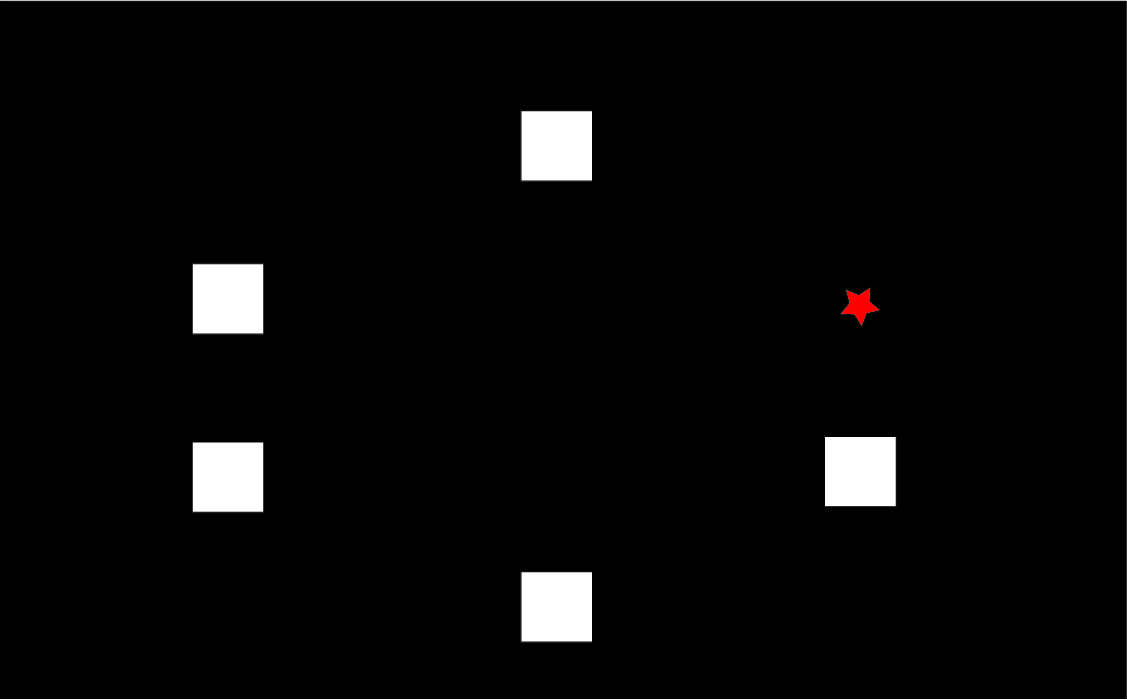
After showing you all the shapes, I then present to you a shape and ask you to identify the box in which it was first presented.

Cambridge Cognition in welcoming the Draft National Plan to Address Alzheimer’s disease in my opinion set out entirely correctly the advantages of this computerised testing battery; including fast, not culturally biased, not heavily loading on language, norm-referenced, culturally unbiased, and easy-to-use.
The reasoning behind it being sensitive to early Alzheimer’s disease – but what about mild cognitive impairment?
To understand why the narrative for the test being so attractive in early Alzheimer’s disease, you have to understand that this test has been found to be sensitive to functions of particular brain areas. If you chop out bits of the brain near the front of the head (frontal cortex) or near the ear (temporal cortex), performance on this task is impaired, as Prof Adrian Owen showed when he was a post-doctoral fellow (paper here). With hindsight, perhaps Owen should have looked at the effects of other brain areas further back in the brain, such as the parietal cortex, which are also now thought to be important in memory for spatial cues.
A consistent finding has been loss of brain cells in the “entorhinal cortex”, in the temporal cortex, early in Alzheimer’s disease (see for example here). Therefore, that the paired associates learning test should identify memory problems in early Alzheimer’s disease immediately makes intuitive sense.
But the issues I feel are much more complicated, and I wish Cambridge Cognition well in clarifying them.
If it’s not Alzheimer’s disease, what else could be causing the memory problems?
One possibility is “mild cognitive impairment”. It is described, for example on the authoritative Mayo Clinic website, that:
“Mild cognitive impairment (MCI) is an intermediate stage between the expected cognitive decline of normal aging and the more serious decline of dementia. It can involve problems with memory, language, thinking and judgment that are greater than normal age-related changes. If you have mild cognitive impairment, you may be aware that your memory or mental function has “slipped.””
David Hart, Senior Business Development Manager of Cambridge Cognition, kindly sent Dr Peter Gordon the rationale for the use of the CANTAB task by Dr Andrew Blackwell, their Chief Scientific Officer (as produced on Peter’s blog here).
Cambridge Cognition concede that distinguishing between MCI and Alzheimer’s Disease “is difficult”, but this is a distinction that must be arrived at otherwise a test potentially will give “false positives” – but no test is perfection, and it basically is impossible to strive for perfection. What we all trying avoid is where a test for possible dementia itself is expensive followed by a further expensive investigation to show the original result was a false positive – or as the Express euphemistically called it recently, “Dementia diagnosis proved wrong by new super scanner”. (It is important to state clearly here that no details are given how a diagnosis had been arrived at previously for Ros Davies.)
To give them credit, Cambridge Cognition cite the Chandler et al. (2008) paper, but the full citation of this is “Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association Volume 4, Issue 4, Supplement , Pages T551-T552, July 2008″ – i.e. it is a supplement of abstracts not full papers. This particular abstract can be viewed here.
It is hoped that this full study will have been published elsewhere, and if so Cambridge Cognition will need to update their website with the full paper. Notwithstanding this, the numbers of individuals in each group are disappointingly low: there are seventeen with putative MCI and twelve with putative Alzheimer’s disease.
Is this task actually sensitive and specific?
However, the discussion by Dr Andrew Blackwell and colleagues in his 2004 paper is useful. I have more than a passing interest in that paper as the main author on that paper was one of my PhD supervisors at Cambridge, Prof John Hodges. John has also kindly written one of my three Forewords for my book, “Living well with dementia” to be published on January 14th 2014.
Blackwell remarks correctly that this task has been used to distinguish between unipolar depression and Alzheimer’s disease in Rachel Swainson’s study. But is this enough? I looked to the previous Beats study in “geriatric depressive”, and there was nothing forthcoming there. How confident can one be that only early patients with Alzheimer’s disease, and not those severely depressed or with an underactive thyroid, will perform abnormally on the PAL? Personally, I’m not at all confident yet, despite the Swainson study, but these fears can easily be allayed with a sensitivity/specificity study of much higher power.
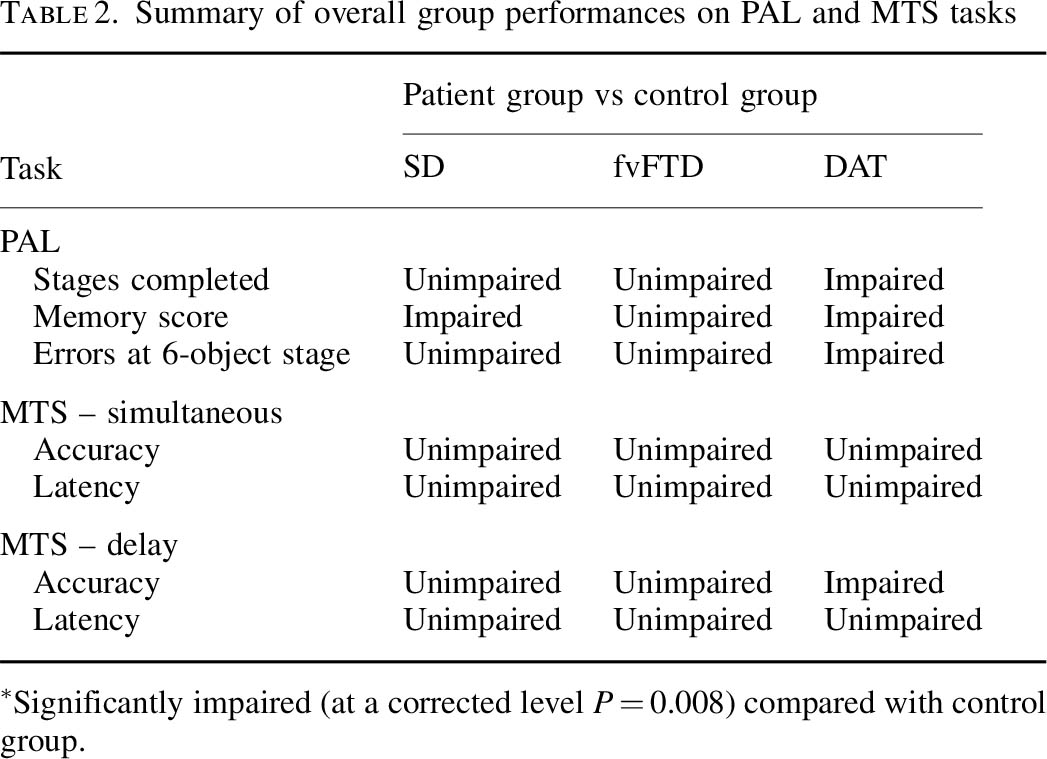
Blackwell is however correct in citing my study with Dr Andy Lee in that patients with semantic dementia and behavioural variant frontotemporal dementia are relatively unimpaired, though the clinical presentations of the frontotemporal dementias can be quite clearly different in the clinic from Alzheimer’s disease. Completing the double dissociation, I did find that the behavioural variant of frontotemporal dementia did present with rather specific risk-taking decision-making of its own.
But in the meantime the comparison with frontotemporal dementias is useful.
Nonetheless, this approach is being rolled out.
On 28 June 2013, the use of CANTABmobile was described as follows:
“The Guildford and Waverley Clinical Commissioning Group (CCG) is leading the use of an innovative new iPad-based memory assessment system as part of a national push to decrease dementia diagnosis waiting times and streamline the referral process. Accessed through NHS medical professionals, CANTABmobile enables GPs to test a patient’s episodic memory through an easy to use and administer 10-minute cognitive assessment.”
The CANTAB paired associates learning test is pictured under the heading “intuitive touchscreen interface”. if you go to “download information” on this page.
It was covered in the national media here: for example Victoria MacDonald’s report (this page provides a criticism of another report by Victoria MacDonald this time over Prof Brian Jarman’s proposed HSMR data by NHS Consultant, Dr Jacky Davis).
So what does this task test?
In understanding how the task works in reality, I found a paper where Prof Ed Bullmore and colleagues put individuals with Alzheimer’s disease and control subjects performing the task into a scanner really helpful. Bullmore and colleagues frontloaded their discussion with the following comment:
“Independent of the level of difficulty, the majority of subjects in both groups activated a network of brain regions, including the anterior cingulate, lateral, and medial occipitoparietal and frontal cortices, during successful encoding and retrieval.”
This is interesting as it doesn’t point to the usual suspects of the narrative, i.e. the entorhinal cortex and other parts of temporal lobe. Even Andrew Blackwell had described how the damage to the entorhinal cortex might possibly account dor deficits on the paired associates task:
“The transentorhinal region is a complex transitional area located between the entorhinal region proper and the adjacent temporal isocortex. It has been suggested that damage to this site in early [Alzheimer's disease] disrupts reciprocal connections with the hippocampal formation and that this disruption underlies deficits in episodic memory.”
But on reflection is this wholly a surprise? Ed Bullmore and colleagues from their results, also from Cambridge, discuss that the lateral parietal activations reported during episodic memory tasks are thought to reflect recognition processes and retrieval processing of spatial information. Medial parietal activity has been proposed to underlie imagery and retrieval success.
I don’t feel it’s altogether surprising given what is known about the build-up of pathology in Alzheimer’s disease, either. The authors of one study looking at this report that:
“[18F]FDDNP-PET signal was significantly higher across widespread cortical regions in subjects with poorer neuropsychological test performances. Strong correlations were seen in the entorhinal, orbitofrontal, and lateral temporal cortices, temporoparietal and perisylvian language areas, parietal association cortices, and much of the dorsolateral prefrontal cortex.”
But the Sahakian lab elsewhere did find something was up with the parts in “the hippocampus and associated structures”, i.e. the structures in the temporal lobe, in this task.
But that study was only comparing MCI with normal controls. It did not include patients with Alzheimer’s disease. This is relevant, if you happen to believe that MCI ‘predates’ Alzheimer’s disease, as the authors of that study clearly do:
“Later in the course of the transition from MCI to clinical Alzheimer’s disease, functioning of the MTL deteriorates further to an extent that such compensatory activity is no longer possible. The hyperactivity in early MCI might then represent a possible predictor or biomarker of the progression to Alzheimer’s disease.”
But in the real world this is far from clear.
However, the evidence of progression of MCI (mild cognitive impairment) to DAT is currently weak. It might be attractive to think that MCI is a preclinical form of dementia of Alzheimer Type, but unfortunately the evidence is not there to back this claim up at present: only approximately 5-10% and most people with MCI will not progress to dementia even after ten years of follow-up (Mitchell and Shiri-Feshki, 2009). Drug companies have been trying hard to push the identification of “biomarkers”, possibly subtle psychological ‘deficits’, scan results or changes in substances in the fluid surrounding the brain (or cerebrospinal fluid). It is no accident that psychological testing and biomarkers were heavily promoted in David Cameron’s G8 dementia speech in Lancaster House at the end of last year.
In summary, I don’t think it can be taken as red that entorhinal cortex problems are causing the observed deficits in the CANTABmobile paired associates learning task.
Conclusion
Overall, my personal view is that the deficits on the CANTAB paired associates learning task are real in early Alzheimer’s disease, but possibly not for the reasons felt by some in their groups. Above all, I don’t care as such, as long as greater numbers of people benefit from a correct diagnosis of Alzhemer’s disease, but I do feel that the logic in their reasoning has gone a bit awry.
My academic viewpoint is utterly irrelevant actually, as above all I wish the whole of the medical profession well in their “war against dementia”.
I’d be the first to admit I’ve got it wrong. I am simply raising the issues in a constructive way that I hope is beneficial for the public interest.
But Dr Mitul Mehta, Reader in Neuroimaging at the IoP, does have his concerns.

The “dementia prevalence calculator”: for a person to access a timely diagnosis, or for private markets to access the person?
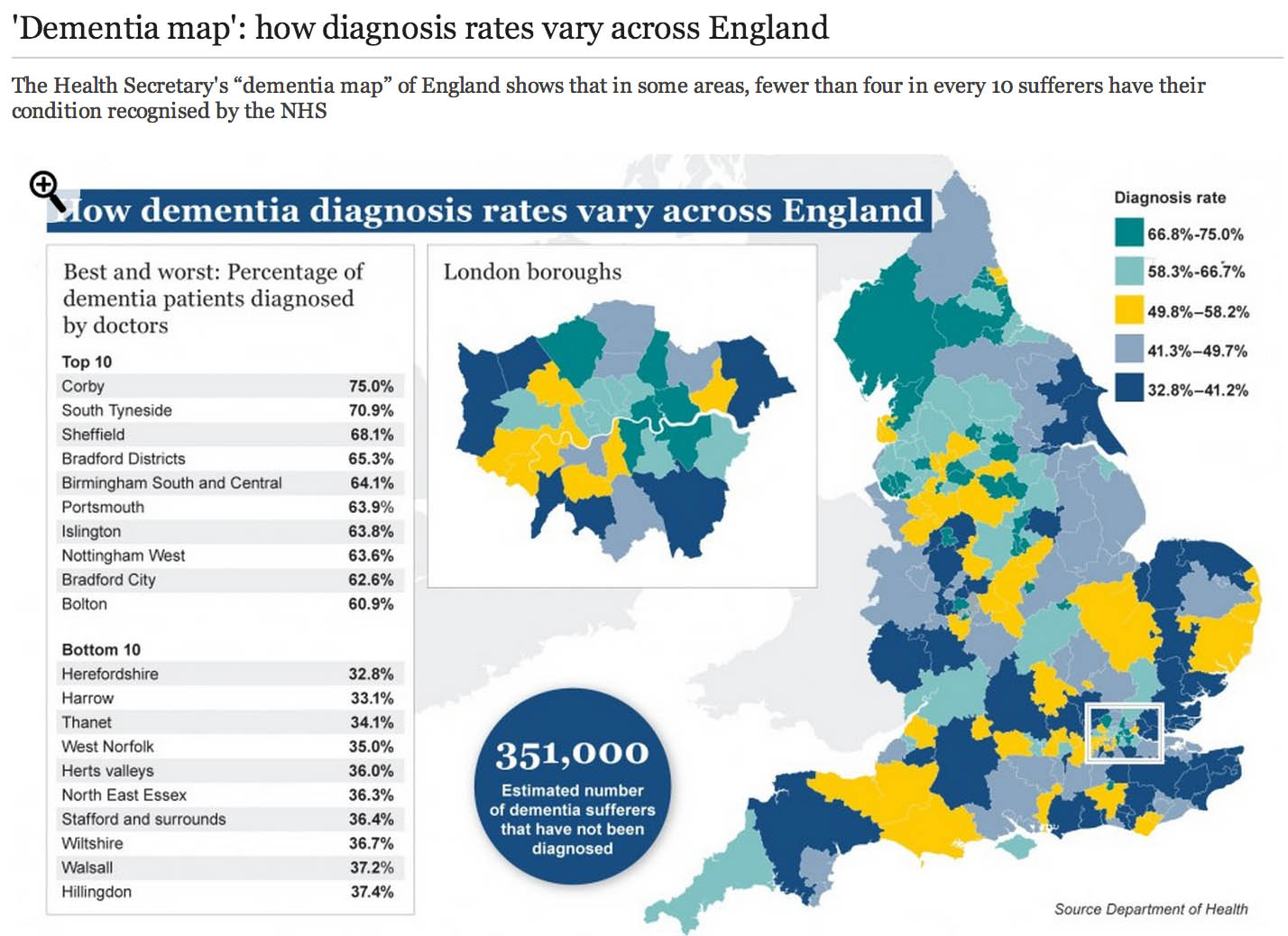
The market philosophy has gripped the NHS by the jugular through policy developments from successive governments. It is argued that all health care systems in the world have to design effective allocative mechanisms for the available “scarce health care resources”. The “dementia prevalence calculator” tool also enables health and care communities to: calculate local dementia diagnosis rates, forecast local dementia prevalence, view trajectories and set “ambitions” (aka targets) for improvement in diagnosis rates and compare diagnosis rates with other localities. Its main problem has been that it has been crowbarred in through various side windows, except nobody knows why public health experts didn’t call for this calculator to come in through a front door. One can now view and compare diagnosis rates on the “Ambition Map”, and link to the “Knowledge Portal” to access a wealth of resources to improve dementia diagnosis rates, and diagnosis pathways. All of this will have taken time, effort and money to set up, so the question of whether it’s worth it, given ‘scarce resources’, is clearly in the public interest. Here is one such example of the Department of Health’s attempts and their partners to disseminate information about “the dementia map”.
So what’s the point of these data? Burns concedes that estimating the number of people who have dementia is important for both local planning and national guidance. Burns freely admits too there have been problems in the past:
“Most current estimates of dementia prevalence (the number of people affected by the disorder) and incidence (the number of people developing it over a defined period, usually one year) are based on studies dating back to the 1980s.”
It’s become clear that a huge “democratic deficit” has engulfed the English dementia policy. The problem for Prof Alistair Burns, who is a genuinely a nice and well-meaning man, is that he can become indundated with various complaints from academics and practitioners. An example is the G8 dementia summit which was presented as a ‘once in a lifetime opportunity’ to talk about dementia. What did, however, happen was that it became a ‘once in a lifetime opportunity’ for various myths to be propagated by the media, using highly charged words such as ‘shocking’, ‘devestating’, ‘crippling’, ‘horrible’, ‘horrific’, portraying the notion that people now on receiving a diagnosis of dementia are just counting their hours until their death. It, likewise, cannot be overstated that the drugs for memory or attention simply do not have a huge effect in the vast majority of patients, and certainly after about fifteen years of published studies on these “cholinesterase inhibitors”, the evidence that they slow down the rate of loss in critical parts of the brain is not terrific. Academics in dementia are currently collaborating across geographical boundaries, so the idea of there now being suddenly a world collaboration is FALSE. A cure for a single dementia is FALSE as there are hundreds of different causes of dementia. Dementia charities of course can mobilise individuals with dementia to contribute in pan-global drug trials in what has been euphemistically been called ‘co-production’, discovering new drugs based on the basis of personal DNA genomic information. Looking at your genetic make-up might tell a practitioner or drug-company your risk of subsequently developing dementia, and so it goes on. The issue is not subjecting the designers of English dementia policy with time-consuming vexatious ‘attacks'; it is hopefully that we can all have an open, transparent discussion of some of the ‘unintended consequences’ of the English dementia policy currently in progress.
In March 2012 the Prime Minister, David Cameron, published his challenge on dementia which set out an ambitious programme of work to push further and faster in delivering major improvements in dementia care and research by 2015, building on the National Dementia Strategy (published on 3 February 2009). Central to the challenge is the requirement that from April 2013, there needs to be a quantified ambition for diagnosis rates across the country, underpinned by robust and affordable local plans (NHS Mandate). This is of course so remarkable in itself in the State having such a strangehold on policy which should in theory be devolved as locally as possible to experts and professionals. A painfully obvious point to those who have done a medical degree is that there will be variation in some rates of particular dementias across the country anyway. For example, in some populations with a predominantly Asian immigrant population with certain risk factors, they might be at high risk of vascular dementias. As it happens, near Warsaw in Poland is thought to have a high prevalence of dementia due to copper overload due to a genetic cluster of an inherited copper metabolism problem called Wilson’s disease. But presumably certain dementia charities and certain politicians want you ‘to get angry’ at those GPs who are underdiagnosing dementia, because they are somehow colluding in keeping this information away from you. This is by the way against their professional code, but you cannot expect people without a medical background who are quite senior in charities or politics to know that necessarily.
I have found that having lack of ability to have a balanced debate (due to enormous information asymmetries) has been quite dispiriting, and clearly hampered by the virtual lack of published research papers in the medical professional literature. Hopefully, the University of Stirling will be able to diminish this ‘research gap’, now that they have been awarded a major grant to investigate this issue properly with no vested interests. This is the only paper on Medline from 1996 if you search for the term “dementia prevalence calculator”. And there is no doubt that the claims of some of the drugs used to treat early dementia in the NHS have been overinflated. Luckily, largely thanks to the work of Glenis Willmott MEP who has been leading negotiations as the European Parliament’s rapporteur on the clinical trials regulation, pharmaceutical companies and academic researchers will be obliged to upload the results of all their European clinical trials to a publicly accessible database, if a deal reached this week is approved, according to a recent report. Indeed, Pharma have got it right about “openness”, but not in the sense of using regulation to allay fears about patient privacy and confidentiality – Big Pharma need to share with the general public their results, and their particular motives and intentions for dementia policy especially if the descriptions are otherwise not easily forthcoming.
I openly admit to being extremely disappointed at one particular plank of English dementia policy: the “dementia prevalence calculator”. It’s incredibly easy to get hold of the marketing shills for CCGs about how they can overcome “the diagnosis gap” for the reported lack of diagnosis of dementia; but there again, the discussion of how there are hundreds of different types of dementia in different age groups is not forthcoming, together with a less than candid explanation of how risk factors for dementia might be tackled. For something so fundamental to English dementia policy, it was deeply distressing to see Prof Carol Brayne’s question on where the Prime Minister saw his “Challenge” progressing on dementia to be passed ‘down the line’ like a rugby ball going backwards with effortless ease first to Mr Jeremy Hunt and then with Dr Margaret Chan. To get a decent grasp on why there has been such a drive to improve dementia rates, you have to go across the Atlantic and research terms such as “needs based resource allocations” in health maintenance organizations (sic). These papers are written entirely from the business model perspective, so do not have any intention of wishing to address remotely the professional concerns of senior clinicians in dementia.
Like all 500 pages of the Health and Social Care Act (2012), there was no open discussion of the need to “turbo boost” the outsourcing of NHS contracts to the private sector. Likewise, meaningful discussion of the perils of ‘case finding’ and ‘screening’ in dementia have largely been throttled at source (though Dr Martin Brunet has been raising awareness of the perils of incentivising GPs to up their rates of dementia diagnosis through ‘case finding’ in primary care, of course drawing attention to the hugely stigmatising “false diagnoses of dementia”). Nonetheless, through the combined efforts of the European ALCOVE project (including Prof Burns and Dr Karim Saad), it’s been successfully argued that,
“Dementia happens to people, living in their families and their communities. It does not happen just to their brains. When people have worrying symptoms they want health care professionals who can spot the signs, take their concerns seriously, diagnose the problem accurately, so they can get the most up to date treatment and advice.”
This is a helpful slide from Prof Dawn Brooker’s presentation for the UK Dementia Congress Conference 2013 entitled, “Benchmarking against ALCOVE recommendations for timely diagnosis in dementia”:

This discussion embarrassingly even led to Prof Burns trying to find Dr Brunet at his practice for a frank chat about the policy, but Martin unfortunately was away that day.

Of course, if you’re going to introduce a policy to ‘up the dementia rate’, it possibly will run into problems given that the actual prevalence of dementia has appeared to be falling. The first UK Cognitive Function and Ageing Study (CFAS), known as the Medical Research Council (MRC) CFAS, began in 1989. One of a suite of European prevalence and incidence studies (forming the EURODEM collaboration), it was designed to test for geographical differences within the UK, across populations with widely varying characteristics, including vascular health. The study published by Matthews and colleagues (2013) in the Lancet confirmed that later-born populations have a lower risk of prevalent dementia than those born earlier in the past century. The general prevalence of dementia (overall numbers of people) in the population might be subject to change. Factors that might increase prevalence include: rising prevalence of risk factors, such as physical inactivity, obesity, and diabetes; increasing numbers of individuals living beyond 80 years with a shift in distribution of age at death; persistent inequalities in health across the lifecourse; and increased survival after stroke and with heart disease. By contrast, factors that might decrease prevalence include successful primary prevention of heart disease, accounting for half the substantial decrease in vascular mortality, and increased early life education, which is associated with reduced risk of dementia. Where possibly primary care will have the greatest impact will be in tackling the risk factors they do anyway for cardiovascular disease, i.e. better diabetic control, tackling cholesterol, smoking, ‘poor diet’, or high blood pressure. This in itself is not a valid reason to avoid improving diagnosis rates of dementia (especially these are treatable risk factors for vascular dementias.)
Health maintenance organizations (HMOs) have been argued by their supporters as a “cost-effective’ way to provide health care. In the United States, in allocating resources in the HMO, the rationing of preventive services appears to be one of the principal questions where the potential benefits (i. e., efficacy) of a service are considered in relation to costs of healthcare. The direct counterpart of the HMO in English health policy, following the enactment of the Health and Social Care Act (2012), is the “clinical commissioning group”, which act as state insurance schemes for pooling risk in population samples.
Just because there’s no effective treatment, there’s still a business case to be made for ‘opening up new markets’ of persons with dementia. For example in the NHS Outcomes Framework 2013/4 domain CB_A9 covers an estimated diagnosis rate for people with dementia, with an aim of “improving the ability of people living with dementia to cope with symptoms, and access treatment, care and support.“. The rationale is therefore stated as:
“A diagnosis enables people living with dementia, and their carers/families to access treatment, care and support, and to plan in advance in order to cope with the impact of the disease. A diagnosis enables primary and secondary health and care services to anticipate needs, and with people living with dementia, plan and deliver personalised care plans and integrated services, thereby improving outcomes.”
According to articulation of neo-liberal ideology, the main justification of the reforms is to make resource allocation “more efficient, more innovative and more responsive to consumers’ preferences” than centrally integrated health systems (Ven 1996, p. 655). The effect of this change in philosophy is the introduction of activity-based resource allocation and funding as a system of paying hospitals and other health care providers on the basis of the work they perform rather than previously applied defined budgets based en bloc global contractual considerations. This new system relies on cost-and-volume and cost-per-case contractual relationships, in which payments are closely linked with the services offered, and clearly the information from “dementia prevalence calculators” is useful here. Conceptually, “dementia prevalence calculators” have been presented on equity grounds, i.e. tackling the inequity of a postcode-lottery diagnosis of dementia. However, this makes a fundamental assumption that there cannot be geographical variations in the prevalence of dementia. I repeat the point – any practising physician would know that this assumption is entirely erroneous, as vascular dementia prevalence rates for cardiopaths for diabetic hypertensive individuals in Tower Hamlets in a ghee-laden diet might be hypothesised to be quite high? The actual drive for the ‘dementia prevalence calculator’ is to open up new active markets, in a form of ‘payment of results’. According to Gay and Kronedfeld (1990), the gradual evolvement of an activity based resource allocation can be traced to the United States, where from 1983 most reimbursement for health care providers had been based upon the Diagnosis-Related Group (DRG) where patients within different categories were classified as clinically similar and were expected to use the same level of hospital resources.
Having a ‘care plan’ for dementia is potentially advantageous in that it can provide harmonisation with private insurance systems. The ‘Kaiser Permanente Care Management’ program contains guidelines and recommendations on how dementia care should be provided to Kaiser enrollees. The new program is an informational resource only and is not a substitute for clinical judgment based on the individual needs of patients. The program includes nine “key principles” on diagnosing and caring for patients with dementia and support for their caregivers. These principles include early identification and diagnosis, connecting caregivers to vital community resources, developing a care plan, and monitoring and adjusting medication use. With the introduction of “whole person care” (or similar models of integrated care in the next government), it is likely health and social care will be taken down a “final common pathway” of the ‘personal budget’ or ‘individualised’ budget (see this article for a recent discussion of some of the key themes from the English healthcare thinktanks). The commercialisation of care, under the guise of control and budgets, is, in fact, of course a complete anethema to genuine principles of professional person-centred care. And merging a universal system which has lots of highly personal data (NHS) with one that is heavily conditional (benefits) has all kinds of risks. In the long run it could make it still easier to restrict access to healthcare on the basis of economic status or behaviour.
While GPs and the public are clearly none-the-wiser about the goal of upping the diagnosis rates, already work is being done on the barriers and solutions for implementation of personal health budgets in dementia. Claire Goodchild’s report for the Mental Health Foundation from October 2011 still makes for interesting reading. Goodchild argues that, “individualised, tailored support and care that a personal budget can facilitate can have enormous benefits to a person with dementia“. The irony is of course that Big Pharma may not actually end up the big beneficiaries of this drive, unless they can make their medications relevant to individuals with dementia in this brave new world. While the G8 conference was an effective pitch for personalised medicines for Big Pharma, relatively little attention was given to psychological therapies or carers, aside from ‘dementia friendly communities’ which bring competitive advantage to the included corporates (and benefits for persons with dementia too). Personal budgets are all about choice and control; it is unlikely that a person with dementia will be unaware of the personal spending decisions that he or she can make to improve wellbeing (deferred to a carer where that person does not have capacity); but other valid interventions do include the assistive technologies and innovations which curiously did also make a mention in the G8 dementia.
Therefore, at first blush, it might look a bit random having a ‘dementia prevalence calculator’ and then all the shennanigans of the G8 dementia summit, but whilst the English government cannot as such make dementia ‘wealth creating’, it can do its best to open up new markets. It hasn’t been an accident that the question, “Have you had problems with your memory?”, has been suggested for those ‘health MOTs‘ which private healthcare would love to get off the ground. And the big beauty of this plan when NHS budgets are looking to do ‘more with less’ or implement ‘efficiency savings’ (or cuts to frontline care, more accurately) is that the NHS budget itself won’t ‘take the hit‘. It is hoped that with the implementation of whole person care budgets somebody will be able to ‘top up’ payments for care (e.g. “co-payments”), and the patient (or customer) will now pay for care providers in the private sector too. Do the treatments actually have to be proven to work? Absolutely not, if the experience in personal health budgets is anything to go by, but that’s not the point. As David Cameron might say, “Oh come on.. please do keep up!”
Further reading
Gay E.G. and Kronedfeld J.J. (1990). “Regulation, retrenchment – the DRG experience: problems from changing reimbursement practice”. Social Science and Medicine. 31 (10), pp. 1103-1118.
Ven, W.P.M.M., van de. (1996). “Market-oriented health care reforms: trends and future options”. Social Science and Medicine. 43 (5), pp. 655-666.

The #G8Dementia Summit – a curious lack of a person-centred approach in the research strategy

David Cameron should be given credit for making ‘dementia’ the topic for discussion of the G8 on 11th December 2013. But the event runs the risk of being a trade fair for the pharmaceutical industry, becoming increasingly desperate to prove their worth in dementia and society.
However, it is widely acknowledged that cholinesterase inhibitors, drugs that boost levels of acetylcholine in the brain to improve attention and memory, have a modest effect if that in the majority of patients with early dementia of the Alzheimer type (‘dementia of the Alzheimer type’). There is no robust evidence that they slow down disease progression in humans from human studies of patients.
Many senior academic experts feel conversely that there has been insufficient attention put into interventions that actually do help people to live well with DAT. Such interventions include improving the design of the home, design of the built environment (including signage and pavements), non-statutory advocacy, dementia-friendly communities, assistive technology and ambient living innovations.
On Wednesday 4th December 2013, a ‘research summit’ was held for the press for “research into dementia”. The main focus of this research summit was how can one best predict who will get dementia or when, do we even know what causes dementia yet, what “cures” are there in the pipeline, what can be done to prevent dementia, what obstacles are pharmacological researchers facing, does Pharma have sufficient resources, and what needs to be done to make the Dementia Summit a success.
The focus of this ‘summit’ into ‘research into dementia’ was not living well with dementia, which is a gobsmacking tragedy for all those involved in promoting living well with dementia.
What is overwhelmingly absent is a ‘person centred approach’ which has been a major force for good in contemporary dementia care in England.
The panel members, according to the brief, were: Dr Doug Brown, Director of Research and Development, Alzheimer’s Society; Prof Nick Fox, Professor of Neurology, MRC Senior Clinical Fellow, Institute of Neurology, University College London; Prof Simon Lovestone, Professor of Old Age Psychiatry, Director of NIHR Biomedical Research Centre for Mental Health at the South London and Maudsley NHS Trust and Institute of Psychiatry, King’s College London and Lead for the Translational Research Collaboration in Dementia (a network of 6 centres established by the NIHR); Prof Peter Passmore, Professor of Old Age Psychiatry, Queen’s College Belfast and Lead for Dementia for The British Geriatrics Society; and Dr Eric Karran, Director of Research, Alzheimer’s Research UK.
To show how little there was on wellbeing, and discussing innovative ways to allow people to live well with dementia, here’s the official write up from the BMJ this week:
“Nick Fox, professor of neurology and a Medical Research Council senior clinical fellow at the Institute of Neurology at University College London, said, “We should be asking the G8 collectively to double the research spending on dementia within five years.
“And I think there is a lovely equitable way of looking at this. We ask the G8 countries to commit 1% of their dementia costs to add another doubling of research spending within 10 years.”
Brown said the aims of the research were to enable more accurate and timely diagnosis of dementia; to create disease modifying treatment to try to stop, slow, or reverse the condition; and to find drugs to treat the symptoms. Most importantly, he said, researchers needed to understand how dementia developed to enable the risk to be reduced and onset of dementia to be prevented or at the very least delayed. “If we could delay the onset by five years we could probably cut the numbers of [people with] dementia in half,” he said.
Fox said that past trials of treatments had concentrated on people with symptoms of the disease, which was “like trialling chemotherapy when people are already in a hospice.” Now, he said, treatments were beginning to be tested in people who were at higher risk of dementia because they had a family history or other genetic risk factors or because scans had shown early features of the disease.
Scans and other techniques could then be used to track the effects of treatment before symptoms appeared. “Only if we can identify people where we can see whether our therapies are having an effect will we ever make progress,” Fox said.
Peter Passmore, professor of old age psychiatry at Queen’s College Belfast and the British Geriatrics Society’s lead on dementia, said that as more was known about the mechanism of dementia, researchers were looking at drugs licensed for other conditions that might impinge on those mechanisms. “That’s cheaper drug development: those drugs are off patent,” he said.”
Many thanks to @sam4wong for sharing this with us on Twitter this morning.
Sadly, this representation of research for #G8dementia has taken on more of an appearance of a corporate international trade fair, which is a crying shame. This is, ironically, in the week that the World Trade Organization has apparently agreed its first-ever global deal aimed at boosting commerce.
A trade fair (trade show, trade exhibition or expo) is an exhibition organised so that companies in a specific industry can showcase and demonstrate their latest products, service, study activities of rivals and examine recent market trends and opportunities. In contrast to consumer fairs, only some trade fairs are open to the public, while others can only be attended by company representatives (members of the trade, e.g. professionals) and members of the press, therefore trade shows are classified as either “Public” or “Trade Only”. However, the G8 next week would be at considerable risk of being hijacked by market forces, if it were not for the valiant efforts of the Department of Health and people who have devoted their lives to raising dementia awareness too. Trade fairs are helpful for marketing of products to a wider audience.
James Murray-White (@sky_larking) is a film-maker, and campaigns perennially for raising dementia awareness. James announced yesterday that he was proud to be part of a central network of dementia ‘activists’ on Twitter, but had just reported on the same media network that he had recently been refused ‘press accreditation’ for #G8dementia.
Earlier this year, filmmakers and scientists came together at this event to increase the public understanding of dementia. This event comprised series of short films about dementia, curated by Murray-White, will precede a discussion with researchers from the University of Bristol and other institutions supported by @AlzheimersBRACE, a local charity that funds research into Alzheimer’s disease and other forms of dementia. Panel speakers included: Professor Seth Love (Professor of Neuropathology); Laura Palmer (South West Dementia Brain Bank Manager); James Murray-White (filmmaker).
However, all is not lost, by any means. Beth Britton (@BethyB1886) will be participating in a short film for #G8dementia. Prof Alistair Burns (@ABurns1907), the Clinical Lead for Dementia in England, has written of Britton:
“Beth Britton has been a breath of fresh air in the discussions and debates around dementia. She brings a clarity of thought and originality of ideas which I have always found very refreshing and helpful when considerations and discussions of the importance of people with dementia and their carers are concerned. She has a unique writing style and a gifted ability to convey ideas and experiences”
Beth is one of the U.K.’s leading campaigners on dementia. Her experience of supporting her father, who was living with dementia, and her professional background, give her unparalleled insight into effective ways of campaigning for change, it is widely felt.
There are people who are simply interested in individuals with people – the person not the drug. For example, Lucy Jane Masters (@lucyjmasters) is a dementia nurse specialist, advocating for change, an educator, and primarily passionate about that person with dementia and those who care for him or her.
Alistair has for long time emphasised the importance of “a timely diagnosis”, rather than an “early diagnosis”. This is very much in keeping with the notion that the potential diagnosis should be offered at a time personally appropriate to any particular individual. Alistair also believes, in his rôle as part of NHS England, that there should be a reasonable level of “post-diagnosis support”. Academics generally agree that the tenure of Alistair as the National Lead for Dementia in England has been a very successful experience for all involved.
There are few people as inspirational too as Norman McNamara, who has campaigned tirelessly to dissolve the stigma which can surround dementia. He can be very easily found on Twitter for example (@NormanMcNamara). McNamara has written poignantly about his own personal experiences of ‘living with dementia’.
Sally (@nursemaiden) was a senior nurse, but likewise now promotes heavily wellbeing in dementia, with her father with dementia of the Alzheimer type having passed away on 1st September 2012.
And it truly is an international ‘effort': Kate Swaffer (@KateSwaffer) in Australia – who has just met up with Gill Phillips who advocates ‘paths to personalisation’, has written brilliantly about her experiences of the dementia diagnosis.
Indeed, it would not be hyperbolic to say that many people have given up much free time into the world of the dementias, as a vocation. Lee (@dragonmisery) has produced an incredible information provision website for carers of people with dementia, and this has advanced the policy plank promoting choice and control in wellbeing.
Twitter has been particularly successful at giving people a voice at last. Charmaine Hardy (@charbhardy) is one of the most prominent members of this very close community. Her profile reveals that her husband, whom she adores, has a rare dementia known as primary progressive aphasia. Anyone following Charmaine knows exactly the emotional intensity of someone caring for somebody with dementia.
Likewise, Thomas Whitelaw (@TommyNTour) has literally been ‘on tour’ talking with amazing authentic emotion, affectionately, about his mother, Joan Whitelaw, who had been living with dementia.
So why such a focus on pharmacology?
Why so little on ‘person centred care’?
This glaring omission of person centred care in #G8 dementia apart from representations below is utterly embarrassing and humilating for the thousands of researchers and practitioners who work in this area. @MrDarrenGormley‘s award-winning blog is a most useful introduction to this area.
And, although deeply enmeshed in the English health policy which has sometimes been far from controversy, the efforts of the Department of Health itself have been most impressive.
Anna Hepburn (@AnnaHepburnDH) is Digital Communications Manager for Social Care at the Department of Health. Anna is well known to be genuinely interested in the views of people living with dementia, and those closest to them.
Anna remarked recently,
“When people with dementia and their partners were invited to the Department of Health recently, there was one simple statement that stuck in my mind: “We are still people”. It came as a bit of a shock coming from one of the articulate and funny people gathered round the table. But it says it all about the misconceptions and stigma surrounding dementia.”
Anna Hepburn continued,
“On 18 November, I had the privilege of meeting more people with dementia, as well as current and former carers of people with dementia, who came to London to make short films to show at the G8 dementia summit. This is so we can bring their voices – and the reality of dementia – into the room on 11 December.”
But as a result of the research summit and other efforts from the media and select researchers, the headlines have been rather sensational and sadly all too predictable, viz:
“Unprecedented breakthrough in the hunt for a dementia drug within ‘five years'” (Independent)
“G8 ministers warned to prepare for global dementia ‘time bomb’” (Times)
“Monthly injection to prevent Alzheimer’s in five years” (Telegraph)
“Jab to slow Alzheimer’s ‘is just five years away': Monthly treatment could be given a decade before symptoms” (Daily Mail)
“Dementia cases ‘set to treble worldwide’ by 2050” (BBC)
The last one has been the most difficult for real experts in the research community with real knowledge of the problems facing international research.
On the other hand, Mr Jeremy Hughes, chief executive of the UK’s Alzheimer’s Society, according to that final BBC report cited above, said: “Dementia is fast becoming the biggest health and social care challenge of this generation.”
“We must tackle dementia now, for those currently living with the condition across the world and for those millions who will develop dementia in the future.”
There has been much media interest in improving diagnosis rates in England, driven more by the dementia charities than public health physicians or GPs. Whilst undoubtedly a ‘cure’ for dementia would be wonderful, it is rarely reported that dementia rates are in fact considered to be dropping. Medical doctors such as Dr Peter Gordon (@PeterDLROW; a NHS Consultant Psychiatrist) and Dr Martin Brunet (@DocMartin68; a NHS General Practitioner) have been invaluable as “thought leaders” in forging ahead with an evidence-based approach to this complex issue, cutting through the media garb and spin (and promotional copy).
Very recently in the prestigious New England Journal of Medicine, it was reported that, “Although demographics will drive an increase in the number of dementia cases, recent reports — generally based on population-based community studies or survey data — point to declining age-specific prevalence or incidence rates among people born later in the first half of the 20th century”
You can follow live digital coverage of the G8 dementia summit on the Dementia Challenge site on 11 December 2013. Well done to all those involved, particularly the grassroots campaigners, Anna Hepburn, and the Department of Health!
For Ed Miliband, can it be a simple choice between the State and the markets?

David Skelton once produced a very interesting document called ‘Renewal’ which had as its aim explaining various ways in which the Conservative Party could extend its appeal to voters nationally. Instead, it has become a rather convenient checklist for the Left to annotate how it has come to be that the Conservative Party under David Cameron has deteriorated so precipitously.
For Ed Miliband, can it be a simple choice between the State and the markets? In a way, of course ‘yes’. You can answer this question by saying you can’t be ‘half-libertarian’ or ‘half-socialist’. The problem here is that a legacy of the Thatcherite era has been for Labour to triangulate itself both into and out of government. The fervour for a ‘third way’ has meant that even that a “progressive” brand of politics from the left has become problematic. Even the incorrigible David Miliband was getting nostalgic about progressive politics this morning in the context of energy prices.
‘Responsible capitalism’, whilst a coherent concept in economic theory and practice, does have a political semblance of trying desperately to make capitalism work. The fundamental desire of responsible capitalism is to make capitalism make for both the company and for society, given an ‘assumption’ that a company’s directors must deliver a positive dividend for its shareholders to remain in business. That it has, however, been justified more in terms of delivering a competitive advantage for businesses more than being a worthy ethos in itself should raise eyebrows on its own. Its analogy for NHS hospitals is that safe hospitals delivers some sort of competitive advantage, meaning a patient should prefer to go to a safer hospital, rather than being a necessary and proportionate ideological drive in itself.
One might not be able to ‘hate markets’ in the same way that it is possible to ‘hate people’, but the ideological drive against markets often fails to draw the distinction between a contempt for the consequences of some markets, and a contempt for the markets themselves. On that point, markets can be compared to religions. It might be easier to draw up a list against fanatics of certain religions than the religions themselves. Markets which come anywhere close to perfect competition, rare as they are, can deliver good customer value on the basis of the good relationship between supply and demand. The voters Ed Miliband perhaps hopes target to get him into Downing Street are possibly not that much interested in the difference between perfect competition, an oligopoly or a monopoly. However, they might share ‘the state of shock’ when they open their exorbitant energy bill.
I suppose Ed Miliband is hoping people will wish to blame the market and to blame politicians. I don’t suppose Ed Miliband realistically wishes people to embrace socialism on the basis of the rejection of the market. If he were to achieve this, he would be achieving something which had not been achieved with the failure of the securitised American mortgage products when the US market ‘overheated’ around 2008. However, the problem with this strategy is that people might begin to blame the politicians who actually were in charge at the time. Whatever the deconstruction of the energy bill per se, for example in the contribution of ‘green taxes’ which the Liberal Democrats may or may not support for their short-term political dividend, the fundamental failure was the State either creating or failing to stop a faulty market of six players instead of fourteen. Ed Miliband is able to do this, because people see the size of their energy bills. David Cameron is hoping to do this with water bills next week. And so it goes on. As Tony Benn says, most politicians aren’t in the business because they fundamentally wish to change things. They are in the business they want to appear to be managing things ‘a bit better’.
There will be some Labour voters who would prefer Ed Miliband to adopt this approach, to get his team into Downing Street rather than to produce a manifesto of unworkable policies. The ‘cost of living’ gulf, compared to real income, has undoubtedly been a success for Ed Miliband to shift the narrative from a rather dry discussion of the deficit and Labour spending too much to the real day-to-day lives of people. And it is helpfully a policy which appears to bridge the Left and Right. Another such issue is ‘the living wage’, which many expect Labour to adopt as a flagship policy in their 2015 manifesto. Miliband’s drive to incentivising private companies into providing a living wage for the wonks will be predistribution. For others, it will be attempting to solve a problem to do with the unfairness of a policy at the source. Miliband will successfully be able to produce the rather Aunt Sally argument that such an approach from multinationals is far better than those multinationals fleecing the worker on less than the minimum wage, and for the State having to make up the difference somehow. The trick for Ed Miliband must be to frame the argument on his terms, like he’s framed the argument on the economy on his terms. Given that the mayor of London and the Evening Standard are about to ‘big up’ the policy from their vantage points on the right, and that Matthew d’Ancona says, for example, that Chuka Umunna is one of the most impressive young politicians he has ever met, means that David Cameron cannot afford to sit on his laurels for too long over this one.
When people point to the fact that the Conservatives appear to be more ‘trusted on the economy’, they tend to ignore almost unanimously that Labour is trusted more than the Conservatives on the basis of utility bills and workers’ rights. That Nick Clegg and his colleagues in the Liberal Democrat Party have turned their party into an irrelevant wooly-hat and sandals -wearing brigade is no minor feat. Crucially, there is absolutely no doubt that the narrative has changed. This means that David Cameron has now next to chance in leading his Conservative Party to a first election victory for years. No doubt there will be numerous column inches written on where it all went wrong for the Conservatives in times to come, but there will be some who say victory is still within his grasp. Even with the boundary changes. Even in producing a stagnant economy for three years. Even in producing the worst winter A&E crisis for years. Even in causing a climate for rent-seeking fiascos in the outsourced provision for services. Even for closing down legal aid in England and Wales. David Cameron does, nonetheless, need a miracle.
The critical thing now is for Ed Miliband to win the election. It is clear David Cameron has already lost it. People, I suspect, won’t be that much interested in an Oxbridge tutorial-style explanation of the failure of markets coming from the Left. The usual things will come to dominate the campaign: Labour defending its record of ‘spending too much’ and ‘letting too many immigrants in’. It’s not so much that the Conservative record is stuck, it’s more of a problem that it’s well-and-truly broken. Ed Miliband has produced his cake, in the manner of an overscrutinised contestant for the ‘Great British Bake-Off’. And the bad news keeps on coming. The excessive profits from hedge funds, allegedly, on the Royal Mail privatisations. The dodgy conflicts-of-interest allegedly in the turbo-boosted market of the NHS. Certainly David Cameron and crew have to worry when criticisms of a giant rat produced by a Union fail to produce much other than a reaction from Labour that any intimidating behaviour from the Unions is to be deplored. The giant rat nonetheless has given a lot of air-time to how the company achieved quite a good deal, but the works of Grangemouth. And you have to worry, if you’re on the Right, when there’s a huge cheer for Paris Lees even slightly mooting the idea of state ownership of energy, water, and – you guessed it – the National Health Service.
The 2015 general election is there to lose. Anything or anyone will be able to throw Ed Miliband off course, such as a rapidly improving economy (this happened for Ted Heath in the early 1970s). If the economy is not rebalanced, however, as many suspect, with too few private companies running badly critical functions which had been the preserve of the State, the Conservative Party will be in trouble. On that occasion, the well-worn anecdotes of ‘do you want a State-run delivery van service like the 1970s?’ or ‘do you remember when you had to wait six months for British Telecom to fix your phone line?’ will become even more mind-numbingly boring than they are now.
The most spectacular phenomenon to happen was not Ed Miliband suddenly making an intellectual debate between the State and markets sexy. It was the failure of the Conservative Party to observe the most cardinal of market principles, ironically. That is – if you’re an antiquated ‘incumbent’ – you lose all flexibility and fail to adapt. It is this failure to adapt that many feel will cost the Conservative Party dear in 2015.
Many posts like this have originally appeared on the blog of the ‘Socialist Health Association’. For a biography of the author (Shibley), please go here.
Shibley’s CV is here.
It's in his eyes. Not even David Cameron expects to win the 2015 election.

It’s in his eyes. Not even David Cameron expects to win the 2015 general election, to be held on May 7th, 2015 according to the fixed term legislation.
The contrast with Ed Miliband’s barnstorming speech last week could not have been greater. Miliband’s speech had a good attempt at intellectual gravitas and a coherent narrative on the abuse of markets in relation to the public good, but did admittedly suffer from a borderline use of clichés and standard rhetorical devices. Still, against the best efforts to discredit him through Damian McBride’s latest pissed-and-tell, Miliband delivered an output which both potential voters and the Unions could agree to agree on.
David Cameron delivered his package like a newsreader trying to make appropriate emotional gestures on reading a flat autocue script. The end result was lack-lustre, unimpressive and frankly unappealing.
It looked as if even he didn’t know what he was doing there. Whoever the script writer (sorry I meant speech writer) was, he or she should be sacked. David Cameron looked as if he was reading a boring an executive summary of an annual report of his organisation. He did not appear like a leader with a vision. He looked like a manager who had consulted with his Chief Finance Officer, George Osborne, that, even after staring the decimal points, he could give a confident projection to investors about future performance.
That bit I can’t blame Cameron for. He was reading out his Annual Report to his corporate investors, quite literally, the people who can make or break his party. Hard-nosed hedgies were there to check their investments would bear fruition. After all, many members of the audience were there to check that High Speed 2 would remain part of the business plan.
Cameron could not of course mention that Labour would definitely repeal the Health and Social Care Act (2012). Such a statement would, of course, send uncontrollable shockwaves to corporate investors, who wish to live long enough to witness their return-on-investment through a swathe of procurement contracts in due course.
The key ‘shared values’ were there like ‘aspiration’, ‘opportunity’, ‘wealth creation’, ‘low taxation’, and ‘strong communities’, in keeping with the Conservative Party corporate mission statement. However, they were delivered devoid of emotion, totally ignoring the plight of disabled citizens who had had their lives screwed up because of the benefits system, no reference to the closure of law centres, libraries or Sure Start, for example.
There wasn’t anything controversial there. No mention of ‘zero hour contracts’. No mention of the closure of law centres. No mention of the inequity of Workfare. No mention of the failures of the privatised utilities industries. It was a deadpan speech for an audience whose average age was close to retirement time.
There was no mention of the failure of how he had achieved ‘the Small State’. No mention of the outsourcing failures to the handful of companies, largely the same bunch who were bidding for the NHS procurement contracts, and many of whom have been involved in one fraud allegation or another.
The speech in a sense was quite representative of a totally uninspiring mob of Conservatives: overprivileged, inarticulate about basic macroeconomics, very pro-employer, and frankly delusional in places.
I would rather have had my testicles attached to the National Grid than to travel up to Manchester voluntarily to listen to that. No. I perhaps would have preferred to have all my teeth extracted without any anaesthetic. I am only glad that I have no interest in the performance of the Conservative Party, or I would have been distressed by today’s performance. It was less ‘Breaking Bad’, more like ‘Unbelievably Bad’. It was a performance that even a Carlton newsreader would have been embarrassed at.
It’s definitely in his eyes. He’s already making plans for his retirement.

Labour has become the Samsung to the Conservatives’ Apple (or vice versa)

You don’t especially need a ‘focus group’ to tell you as many different views as you have participants. “Big data”, whilst flavour of the month, is not necessarily ‘best’. A recurrent theme that Labour regular voters find themselves returning to is the question of why bother voting Labour, when they simply seem to be a “Tory Lite”.
A member of any political party is worth his or her own weight in gold. Patrick O’Flynn, Chief Political Correspondent for the “Daily Express”, recently nailed his colours in the UKIP mast. In his recent speech to party members, O’Flynn’s love of his Party was obvious. A particularly effective line in his speech, which was more than a pithy soundbite, was his remark, “We are not a party of Little England – we are a party of Great Britain.” This in marketing terms known as ‘strategic positioning’, when you think about what your product is offering that is so distinct from other people on the market.
And that’s as far as I wish to push the ‘lessons from marketing’ narrative. Many grassroots members of Labour are totally exasperated about the ‘new lick of paint’ approach to politics, perhaps embodied by Mandelson’s rebrand of “New Labour” or Cameron’s reference to Ronseal. The practical problem that Ed Miliband faces, nonetheless, is that his ‘crisis of confidence’ could be a problem fundamentally with the song (Labour party policy) or the singer (him). As for the singer, attention has been given to his onstage demeanour and singing style, as this might seem like a worthy train of enquiry. The wait for policy details has been exasperating. One suspects there might be less criticism of the singer if the song were better defined. For example, the method of delivery of low-paid workers from Europe undercutting domestic English workers might have been more successful if Miliband had a song with clearly defined lyrics concerning a living wage in the first place.
When you ask people ‘what the perceived problem is for which the solution is the Conservative Party’, some people churlishly say ‘The Labour Party’. This is not as trivial as it first seems, as the idea of bin liners not being evacuated from the streets of our cities is deeply entrenched in the minds of some voters above a certain age. Some voters have genuine concerns about the Unions, and the relationship of the Labour Party with the Unions. Labour is in a position of being damned if it does and damned if it doesn’t. It can have wish to have a dialogue with the voters on hedge funds leading English NHS privatisation behind closed doors, but will find itself ever-frustrated if the media refuse to cover the issue at all.
It could be that Labour has simply lost a sense of its values. The argument that Labour lost the plot, and changed from a socialist party to a social democratic party, is often instantaneously rebutted by the argument that ‘But Tony Blair was the best election-winning machine which Labour ever had.” To which point, many invariably stipulate that Labour began to lose its core support as early as 2002/3, long before Labour finally relinquished office in 2010.
This perceived lack of clarity is linked to Ed Miliband’s performance as a leader. Miliband is quite good doing ‘reactive’, but Miliband often seems at his best when responding to a crisis, whether this is phone hacking or horse meat. The UK does seem to have been a perpetual state of crisis since the General Election of 2010, but Miliband does impressively appear to have ‘called the right shots’. This does not make up for a lack of policy, or ‘vision’. The usual argument that ‘we are two years away from the election’ merely confirms the idea that Labour is in no particularly hurry to outline a clear vision of settled values and principles on which it can progress. It instead confirms a notion of Labour making policy ‘on the hoof’, whether this is, for example, a ‘response’ to a ‘buy to let’ housing policy or a ‘response’ of vans which are allegedly racist.
There is possibly no single more significant policy plank than the UK economy over which there is genuine concern as to whether Labour is following or leading. It is possible that the economy is making a feeble recovery, over two years after it was also feebly recovering in 2010. It is possible that this new recovery is being fuelled by a temporary housing boom in London. There are many events which can be identified as to why the UK economy has been given a turboboost in the opposite direction by the Coalition. Ed Balls’ policy is perceived as ‘cutting not as deep, and not as fast’, and yet Balls seems fully signed up to a path of austerity. Balls seems as if he wishes to ‘have his cake and eat it’, criticising the Coalition’s economic policy while simultaneously supporting it.
If the economy does go into a sustained recovery, it is possible that the Conservatives will receive a ‘bounce’ for being more trusted on the economy. Voting data do actually provide that both the Conservatives and Labour Party are equally mistrusted on the economy. Labour seems to have been wishing to act ‘butch’ on the economy, hoping that voters will ‘learn to love’ Labour on the economy. This doesn’t add up. The Labour Party, in the style of an overcomplicated Oxford tutorial or Cambridge supervision, have failed overwhelmingly unconvincingly to establish a need for a £860 billion bailout. This failure means that the Conservatives still have some mileage with the fraudulent message, “Would you return the keys to the people who crashed the car?”, blaming the State for the global financial crash not the bankers in the City.
Labour’s problems are further compounded in that it doesn’t seem to offer anything much distinctive. Labour has become the Samsung to the Conservatives’ Apple (or vice versa). Labour supports PFI and Nicholson’s “efficiency savings”. The Conservatives do. Labour appears to support generally free schools or Academies, partly depending on what day it is. The Conservatives do. Labour seems to support acting ‘tough’ on illegal immigrants. The Conservatives do. Labour seems up for ‘modernising’ public services, and privatising what it can from them. The Conservatives do.
The truth is that politics, like the market which it has tried to copy, has become alarmingly homogenised. There is an illusion of choice, but there is a cigarette paper now currently between the main English political parties. When will Labour reverse “the Bedroom Tax”? And so it goes on. The frustration with Ed Miliband is as contrived as is the frustration with David Cameron. It’s a general malaise about the political process, though people generally are very articulate and passionate about many societal issues conversely. Labour’s approach appears to be to ‘play safe’ so that people think it’s ‘safe’ to vote Labour, rather than offering anything exciting or distinctive. If it pursues this strategy, it is more likely to find itself in ‘hung parliament’ territory rather than having a large working majority. But Tony Blair had a huge majority in 2007, and his legacy is still being fiercely debated.
CV here

David Cameron's holiday, like an individual's tax arrangements, is actually none of your business

Why would you want David Cameron not to take a holiday? Perhaps you think that he should be chained to MI5 or MI6 24/7. Maybe you have some especial thing about him wanting to spend time with his wife or his family?
This “mean-mindedness”, about individuals feeling that it is their business to deprive David Cameron of a small break, beggars belief. More’s the point, it is even more astonishing that they inflict their views about this unimportant manner in such an impersonal public manner. It is a characteristic of all organisations that there is enough people in the team for operations to run smoothly. I am not saying that David Cameron, as Prime Minister, is simply a manager and we can run the country without him. But to think it is worth spending time writing about how he should not have a holiday, or even criticise him for his choice of destination, is petty, when you consider the real choices that this country faces. Should the UK government seek to crack down on aggressive tax avoidance unilaterally or is it simply an extension of shareholder primacy under the company law of many jurisdictions, not just ours? Should we seek to have more NHS services run by the private sector, so that they possibly can be run not at a loss, but to seek to deliver higher quality or value, even if returning a profit? Whatever your ideological viewpoint, these are more interesting questions that all parties need simply not to sit on. Labour didn’t do anything for years on tax avoidance, and contributed in introducing the private sector to the NHS. This may upset you: but David Cameron’s holiday is none of your business. That’s why you won’t find his holiday snaps in the newspapers, because it would be an unlawful invasion of his privacy.
A third of people will like you whatever you do. A third of people will dislike you whatever you do. A third of people will be completely indifferent whatever you do. The fact that people are concerned about David Cameron’s holidays, in the news, is more of an artefact that the media choose to report this, say, ahead of events in Syria. Or, even better, they have finally become exhausted by their own reportage on UKIP. The enthusiasm of scrutiny on this parallels the amount of disproportionate interest given to the Eton Entrance Scholarship examination past paper. The general paper is not testing the tenacity of bigoted right-wing beliefs, deeply engrained in the education system. Nor is it testing whether people are ‘fit to rule’ the country. Such paranoid beliefs simply serve to confirm what the Left hate being criticised about – the politics of envy. They also show deeply prejudiced opinions which reasonable people should find deeply worrying.
What, though, is weird about this entire thing is that people writing newspapers are generally not working class, not even in the Daily Mirror. And some of the people protesting the most loudly about class issues have graduated with good degrees from the University of Oxford in an arts based subject such as English. It is not long ago that black and ethic minority candidates, from relatively disadvantaged backgrounds, felt pressurised to study a vocational subject such as engineering, law or medicine, to maximise their chances of succeeding in life. But taking this argument to another extreme, nobody would wish for Oxford graduates in English to avoid deliberately discussing these topics on class or lifestyle which deeply interest them. Freedom of expression is extremely important as a qualified human right, and so long as listening to somebody exerting their freedom of expression is not automatically taken to mean ‘tolerance’ of those views, it should be a right to be defended strongly. It is clearly worrisome if professional politicians should wish to censor those people with views which are extreme, but not unlawful or illegal.
But then again this is not the first time that this country would get its knickers in a twist about the difference between the law and ethics. Tax avoidance is actively frowned upon by the professional bodies of accountancy, and everyone knows it’s complex. All sorts of people making tax decisions for entirely personal reasons, including ISAs. People’s tax affairs are none of your business. You can argue that the tax affairs of Google, Starbucks or Amazon impact upon society, but, so long as it is legal, it is strictly speaking, it is none of your business. If you have a serious gripe against the economy, tax, or the NHS, you can remedy your grievance by voting for a party which more represents your views on May 8th 2015. However, if you are interested in David Cameron’s holiday, or Eton scholarship exam questions, just realise it’s pontificating. Lazy journalism. “Entertainment”. It’s nothing interesting, or intelligent. It certainly doesn’t make this country a better place.
Why David Cameron's "lurch to the right" must not be above the law

Like John Hirst, the former prisoner who studied law and put the UK on-the-spot about the proportionality of imposing a total ban on prisoners using the vote, David Cameron is not above the law. In a question on fox hunting once in Prime Minister’s Questions, Cameron voluntarily offered the information that he had not done anything unlawful; this was a stupid strategic error, as nobody had accused him of having done anything unlawful. The ‘rule of law’ holds the supremacy of the law, everyone is equal in front of the law, and nobody is above the law.
David Cameron does make the law however for the time-being. He can effectively do what he wants: hence the famous aphorism of parliamentary supremacy of Sir Leslie Stephen ((1832–1904), “If a legislature decided that all blue-eyed babies should be murdered, the preservation of blue-eyed babies would be illegal; but legislators must go mad before they could pass such a law, and subjects be idiotic before they could submit to it.” [The Science of Ethics, p. 145 (1882).]
Eastleigh was a tragedy for Cameron. Having set things up nicely on how his party would offer a referendum on Europe in 2015, which kept the Tory Euroskeptics happy for the time-being, the UKIP backlash was fully active last Thursday. Whilst UKIP does not have a single MP yet, they still threaten the Conservatives with the power to deny them an overall majority. And yet, David Cameron knows that he cannot unilaterally have special terms for the UK’s membership of Europe. Sure, directives can be applied by our Government according to parliament’s wishes, but if he wants anything more he will have to leave Europe. He is not above the law, but he could repeal the European Communities Act (though it would be difficult for him to do so). Even if David Cameron decides that he wishes to tear up the Human Rights Act, he will still have to submit human rights allegations to Strasbourg unless he decides not to become a signatory to the European Convention of Human Rights. Louise Mensch has described that the Human Rights Act itself is faulty, whereas most learned experts feel that the implementation of its analysis could be improved, and we are better off doing the proverbial in the tent than outside it. Leaving the European Convention of Human Rights denies us any moral authority on commenting on the human rights of other jurisdictions, and sets out a very dangerous signal in terms of reputation on our attitude towards inalienable human rights as per Delhi for example.
The more insightful conclusion is that David Cameron is desperate. He was initially tolerated as Prime Minister, but generally even this has deteriorated to being positively loathed by people within his party and outside of it. His Coalition, for example, has legislated for the Health and Social Care Act, which contains one clause section 259(10), which in conjunction with the Data Protection Act and Human Rights Act, is an area where the European Court of Human Rights could easily find the approach of GPs to data confidentiality unlawful; this could be determined one day in a test case similar to S and Marper v UK. It is helpful indeed that lawyers are able to act on poor legislation, as indeed they recently had to do with Iain Duncan-Smith’s mandatory work placement schemes (in the case of Cait Reilly). However, it is the democratic deficit, that laws appear to come from nowhere (and certainly not contained in any party manifesti at the time of the 2010 general election), which is most worrying. It is not so much a case of this Coalition ‘running out of things to do'; it is rather a case of this Coalition ‘running out of things to destroy’.
Unpacking the legacy of this Coalition is going to be extremely painful. George Osborne’s “badge of honour”, the triple A rating, was humiliatingly stripped off the Government, as Moody’s caste judgement on their deficit reduction plan. Construction performance hit a 41 month low this morning. Anyone with the most rudimentary understanding of economics will appreciate that the Coalition terminating ‘Building Schools for the Future’, and other key infrastructure projects, put the brakes on the economy which had been recovering in May 2010. Add to this an increase in 2.5% in the VAT rate, encouraged by corporate CEOs writing letters to the Times, and murder of consumer spending, and you can easily understand how corporate interests saw the UK’s economy being sent down the river. But it’s ok because we don’t have a functional BBC. The BBC, which is not covered by the Freedom of Information Act, is not obliged to explain its ‘creative authority’ for why its journalists never explain why the deficit exploded in 2009 due to a £1 tn recapitalisation of the banks. It does not need to explain either on the basis of its creative licence either why it barely mentioned the activities of the NHA Party in Eastleigh, or why the criticisms of the 2012 Health and Social Care Act (and the concomitant statutory instrument 2012/057) evade scrutiny. However, the reality is that the UK has been trashed like a Bullingdon restaurant party; whether this is the scrapping of the education support allowance, the implementation of tuition fees, the shutting of libraries, the poor regulation which allows ‘value’ horsemeat to be fed in school dinners, the privatisation of the NHS, the triple dip recession, rioting in the streets, or otherwise, the UK at the moment is a disgrace compared to what it could and should be. David Cameron’s “lurch to the right” will not get round that – his only way to get above the law is to rewrite it fast. The other way to get above the law is to annihilate access-to-justice, and by stopping access to the European Court of Human Rights, or any high street mechanism of achieving justice (for example, high street law centres or citizen advice bureaux). No comment.

Why David Cameron's "lurch to the right" must not be above the law
Like John Hirst, the former prisoner who studied law and put the UK on-the-spot about the proportionality of imposing a total ban on prisoners using the vote, David Cameron is not above the law. In a question on fox hunting once in Prime Minister’s Questions, Cameron voluntarily offered the information that he had not done anything unlawful; this was a stupid strategic error, as nobody had accused him of having done anything unlawful. The ‘rule of law’ holds the supremacy of the law, everyone is equal in front of the law, and nobody is above the law.
David Cameron does make the law however for the time-being. He can effectively do what he wants: hence the famous aphorism of parliamentary supremacy of Sir Leslie Stephen ((1832–1904), “If a legislature decided that all blue-eyed babies should be murdered, the preservation of blue-eyed babies would be illegal; but legislators must go mad before they could pass such a law, and subjects be idiotic before they could submit to it.” [The Science of Ethics, p. 145 (1882).]
Eastleigh was a tragedy for Cameron. Having set things up nicely on how his party would offer a referendum on Europe in 2015, which kept the Tory Euroskeptics happy for the time-being, the UKIP backlash was fully active last Thursday. Whilst UKIP does not have a single MP yet, they still threaten the Conservatives with the power to deny them an overall majority. And yet, David Cameron knows that he cannot unilaterally have special terms for the UK’s membership of Europe. Sure, directives can be applied by our Government according to parliament’s wishes, but if he wants anything more he will have to leave Europe. He is not above the law, but he could repeal the European Communities Act (though it would be difficult for him to do so). Even if David Cameron decides that he wishes to tear up the Human Rights Act, he will still have to submit human rights allegations to Strasbourg unless he decides not to become a signatory to the European Convention of Human Rights. Louise Mensch has described that the Human Rights Act itself is faulty, whereas most learned experts feel that the implementation of its analysis could be improved, and we are better off doing the proverbial in the tent than outside it. Leaving the European Convention of Human Rights denies us any moral authority on commenting on the human rights of other jurisdictions, and sets out a very dangerous signal in terms of reputation on our attitude towards inalienable human rights as per Delhi for example.
The more insightful conclusion is that David Cameron is desperate. He was initially tolerated as Prime Minister, but generally even this has deteriorated to being positively loathed by people within his party and outside of it. His Coalition, for example, has legislated for the Health and Social Care Act, which contains one clause section 259(10), which in conjunction with the Data Protection Act and Human Rights Act, is an area where the European Court of Human Rights could easily find the approach of GPs to data confidentiality unlawful; this could be determined one day in a test case similar to S and Marper v UK. It is helpful indeed that lawyers are able to act on poor legislation, as indeed they recently had to do with Iain Duncan-Smith’s mandatory work placement schemes (in the case of Cait Reilly). However, it is the democratic deficit, that laws appear to come from nowhere (and certainly not contained in any party manifesti at the time of the 2010 general election), which is most worrying. It is not so much a case of this Coalition ‘running out of things to do'; it is rather a case of this Coalition ‘running out of things to destroy’.
Unpacking the legacy of this Coalition is going to be extremely painful. George Osborne’s “badge of honour”, the triple A rating, was humiliatingly stripped off the Government, as Moody’s caste judgement on their deficit reduction plan. Construction performance hit a 41 month low this morning. Anyone with the most rudimentary understanding of economics will appreciate that the Coalition terminating ‘Building Schools for the Future’, and other key infrastructure projects, put the brakes on the economy which had been recovering in May 2010. Add to this an increase in 2.5% in the VAT rate, encouraged by corporate CEOs writing letters to the Times, and murder of consumer spending, and you can easily understand how corporate interests saw the UK’s economy being sent down the river. But it’s ok because we don’t have a functional BBC. The BBC, which is not covered by the Freedom of Information Act, is not obliged to explain its ‘creative authority’ for why its journalists never explain why the deficit exploded in 2009 due to a £1 tn recapitalisation of the banks. It does not need to explain either on the basis of its creative licence either why it barely mentioned the activities of the NHA Party in Eastleigh, or why the criticisms of the 2012 Health and Social Care Act (and the concomitant statutory instrument 2012/057) evade scrutiny. However, the reality is that the UK has been trashed like a Bullingdon restaurant party; whether this is the scrapping of the education support allowance, the implementation of tuition fees, the shutting of libraries, the poor regulation which allows ‘value’ horsemeat to be fed in school dinners, the privatisation of the NHS, the triple dip recession, rioting in the streets, or otherwise, the UK at the moment is a disgrace compared to what it could and should be. David Cameron’s “lurch to the right” will not get round that – his only way to get above the law is to rewrite it fast. The other way to get above the law is to annihilate access-to-justice, and by stopping access to the European Court of Human Rights, or any high street mechanism of achieving justice (for example, high street law centres or citizen advice bureaux). No comment.
