Home » Posts tagged 'andy burnham'
Tag Archives: andy burnham
Andy Burnham at the Fabian Society explaining a need for ‘whole person care’
Andy Burnham MP was invited to speak at an event called ‘Together’ on the subject of his Fabians pamphlet of the same name. This video was taken at the Labour Party Conference 2014.
Here he gives a vigorous defence of the proposed policy, not unique to this jurisdiction, on ‘whole person care’. In England, however, it will mean the formation of a National and Health Care Service. It therefore has profound policy implications.
Burnham announces plans to implement a National Health and Care Service over ten years

The Shadow of Secretary of State for Health, Andy Burnham MP, says that he has tried to produce an answer ‘which people can believe in, and which people can buy into’.
This is particularly timely, as it is well known that Labour intend to make the NHS a major general election issue next year.
The Conservatives and Liberal Democrats are now deeply unpopular over their management of the NHS, as evidenced, for example, by the campaigners who converged on Trafalgar Square recently on behalf of the “Darlo Mums”.
Over successive governments and most recently, the finances of social care have suffered massively.
Speaking at a fringe event for the Fabian Society in Manchester yesterday, Burnham felt that things are not satisfactory as the response to an ageing society has been through a medical model.
Burnham’s problem is that he is about to be bequeathed a fragmented illness service, not a national health service; and that the system is patient-focused on ill people not person-focused on people through health and illness. Burnham feels that focusing on people will enable a greater focus on friends and families too.
Burnham feels that the “ever-increasing hospitalisation” of an ill ageing population will not work, and that hospitals are becoming increasingly dysfunction all the year round due to a social care system which has been malnourished over successive governments.
“This failure piles pressure on the acute system”.
Burnham further adds that people “are battling in caring for people with complex needs”, and that “these silos are not ones which can afford any more”.
This policy is anticipated to bring in housing, education, and leisure strands in due course.
But the urgency for Burnham is to deal with people having to avoid recounting their personal stories repeatedly to different people; and that professionals are often making clinical decisions on the basis of incomplete information.
The intention is, ultimately, to bring together systems for physical health, mental health and care. Sir John Oldham had earlier in the fringe event observed that the general public can have a poor understanding of the word “social” in relation to ‘social care’.
Burnham intends to set out a ten year plan for a whole person care, fully accepting the findings of the Oldham Commission, and which “endorses” the findings of the Barker Commission from the King’s Fund.
Such a plan will be strongly attractive to those vociferous critics, such as Sir David Nicholson the immediate predecessor of Simon Stevens as the CEO of NHS England, that health policy has traditionally been adopted on the basis of the electoral cycle.
This system will be a “National Health and Care Service”, which will realign an activity-based tariff for episodes of illness to produce a single ‘year of care’ budget for each person covering his or her physical, mental or social meeds. This, Burnham feels, will support prevention and wellbeing.
At first the idea was to have a pooled integrated budget across health and care, but, in the subsequent question/answer session, Burnham made extremely clear that he was mindful of the need to move away from privatised fragmented care; and to move away from compulsory personal health budgets which had not been proven to work well.
Burnham, instead, signposted plans to be announced later this week that he would instead advocate a general ‘rights based approach’, where citizens could be given realistic expectations of the development of personal care plans according to their needs.
Burnham emphasised that he remained unconvinced that personal budgets were the sole instrument that could achieve this aim.
He is of course extremely mindful of the public’s overwhelming lack of appetite for the marketisation, outsourcing or privatisation of the NHS.
As an example of ‘market failure’, Burnham cites how councils in their wish to compete to keep council tax bills low end up failing on high quality care.
Interestingly, he also feels that this plan has the potential to be ‘radical’, allowing people can be supported to care, enabling full personalisation.
Such a system will involve a “care coordinator”. This has already been mooted publicly very recently by the Shadow Minister for Care, Liz Kendall MP, as a point of contact for the elderly to navigate themselves through the maze of information including care information.
Such a rôle, it is felt, might not be for general practitioners, but possibly for specialist nurses. The voluntary sector, such as Dementia(UK) which developed the innovative specialist “Admiral” nurses programme, might be well placed to act as these coordinators.
In the alternative, social care practitioners might be particularly well suited for a care coordination rôle for people with dementia, as they command expertise in decision-making and capacity. Social care practitioner leads in this context would help to overcome a barrier to cultural integration, furthermore; this is especially important given the often perceived hierarchies of the professions involved.
“Carers will no longer be peripheral to the system, but central to the development of a care plan.”
This plan would be established over a ten year period to integrate services around the individual, not through a sudden ‘top down reorganisation’.
A potent steer for this would come from the Health and Wellbeing Boards.
It is expected that the Labour Party will also use their party conference this year in Manchester to emphasise its intention to repeal the Health and Social Care Act (2012) in the first Queen’s Speech of an incoming government in 2015.
Jackie Ashley, Sir John Oldham, who chaired the Oldham Commission, and Kate Barker, who chaired the Barker Commission of the King’s Fund, panel members yesterday evening, all agreed that it was unlikely that politicians would openly wish to pledge to raise taxes for health and care. The way in which this had been politically debated in the 2010 UK general election, it is felt, had been unimpressive.
Nonetheless, the general sentiment was that the public would appreciate an open discussion of how sustainable funding for health and care systems could be achieved.
Jackie Ashley, who writes for the Guardian, explained the difficulties in the news media approaching this topic, when headlines consistently remained fixated on crises in the NHS.
The general policy trend has been try to support people who wish to live and to be cared for at home independently.
However, Ashley alluded to the need to avoid a narrative that hospitals are necessarily bad and non-hospitals are necessarily good.
It is felt that when the NHS was originally set up it was not designed to be catering for people in their 90s with their multiple clinical care needs.
Nonetheless, Oldham urged the need for NHS England to move away from the needs of hospitals, and urged, as an example, a greater number of representatives from local authorities (currently involved in commissioning social care) on NHS England.
For a condition such as one of the dementias, citizens have the perception of their care needs being financially punished through the need to pay for care; this is, for example, in contrast to a condition such as one of the cancers, where the NHS appears willing to pay for expensive medications often.
Equity, equality, fairness and justice will therefore be key aims of this new National Health and Care Service.
“These are some silos which we desperately must get rid of”, exhorts Burnham passionately.
Finally, Burnham wishes this to be a plan for the National Health and Care Service fit for purpose for a 21st century, synchronising at last the wishes of the public, professionals and politicians.
What is Clive telling Andy and does Andy need to listen?
I had the pleasure of going to two events at the weekend. On Saturday, I went to the event at Trafalgar Square for the #999CallfortheNHS #DarloMums arriving after their 300 mile-long walk across the country. Thanks to Jos Bell for inviting me, for which I am deeply grateful. The following day, I went to the National Health Action Party for their Annual Conference in Conway Hall, Red Lion Square, London. I enjoyed that afternoon as well.
The National Health Action Party are putting up parliamentary candidates for the General Election 2015, the vast majority of whom are known friends of mine. I am proud of them, and I really do wish them well. They give people a chance to vote for a party which has an established position against privatisation. The party is led by Dr Clive Peedell and Dr Richard Taylor, and they clearly have a strong position against privatisation of the NHS, and various manifestations of the NHS market including the private finance initiative and the EU-US free trade treaty.
They have made substantial progress this year. One of their challenges as a new party is having people recognise what they stand for, and this is clearly going to be hampered if the mainstream media do not give them a fair opportunity. Nonetheless, there have been noteworthy successes, such as appearances on Sky, LBC and “The Evening Standard”. And there is no doubt about the intensity of emotion in support of the National Health Service. A challenge is funding, and, whilst the party is in fact running a healthy surplus, having more funds will allow them to present a greater number of election candidates; an inevitably costly process.
It was very nice to chat with Dr Clive Peedell both before and after the event. I understand the misgivings about previous Labour policy, and indeed whether Labour can be said to be doing enough on abolishing the market. There are clearly strands of Labour policy which made room for private providers, but likewise it is also the case that the Lewisham judgment in the high court clearly stated that legislation under the present Government had been a clear departure from previous law under the last Labour government.
So it is not a surprise that many of the key pledges of the National Health Action Party will also be of concerns of some Labour voters with a keen interest in NHS policy. A slide of these were presented yesterday.

It is easy to underestimate the pernicious effect that the private finance initiative has had. Whilst it may have had good intentions of improving the infrastructure of the health service, one cannot deny how ‘cost savings’ allegedly in places have led to dangerous threats to patient safety, such as hospital infection, or in actual staffing numbers cannot be tolerated, not least by the general public and the clinical regulators. Whilst not all the problems can be held responsible from that desk behind Whitehall, the removal of the Secretary of State’s duty for the NHS is clearly symbolic. And Clive Efford MP perhaps would do well to learn from Peter Roderick, a public interest lawyer by training, and Prof Allyson Pollock, a world respected expert in public health.
Andy Burnham MP undoubtedly has a lot of goodwill too, and it is now likely that Labour will be the largest party of an incoming government at least under the leadership of Ed Miliband; they could win an outright majority, also, if the policy mix is right. Burnham has explicitly stated his desire to repeal the Health and Social Care Act (2012), but it is clear that a huge amount of work will be necessary to clear up the regimes for Trusts in financial distress, and for getting rid of competitive tendering tendering as being the default option.
It is not easy to let the Liberal Democrats ‘off the hook’, though it is clear that there are MPs such as Andrew George who have been strongly critical of the NHS reforms and indeed the “Bedroom Tax”. It is undoubtedly clear that the National Health Action Party will not be the main party forming Government next year, but they have never had aspirations to. They do allow the main political parties to be held to account, and their supporters are enthusiastic and well informed.
One of the critical tests for Labour will be letting go of the more neoliberal twangs to its policy, and to represent those people who had gone on the modern day NHS Jarrow march. It is not simply good enough to riposte every attack with ‘yeah but the NHS is free at the point of need’. There are genuine problems with solidarity, equity, justice, and comprehensiveness in current ethos, and a whole raft of problems which have arisen from indisputable marketisation and privatisation of the National Health Service.
It would be a mistake for Labour to discount the National Health Action Party as an insignificant blot on the landscape, when many of their concerns should be genuine concerns for Labour too. Andy Burnham is a highly skilled politician, but he has a strong vested interest in making a Labour government work properly for the NHS, and that might include for example not holding its staff to ransom yet again on a pay freeze. Andy as critical part of a Labour Government might wish to find a way to fund the NHS properly, especially since the economy is apparently making a recovery?
Whilst the present Coalition Government may seem ‘catastrophic’ to many of us, it has in fact been a blazing success for the Coalition parties. They have been able to do a lot of damage in the name of ‘austerity’. The evidence base for such policies is extremely poor, and indeed there is quite a lot of evidence that the welfare benefit ‘reforms’ have done a lot of damage to the mental health of citizens particularly those with disabilities.
Dr Clive Peedell has much to tell Andy, and – for what it’s worth – I do believe Andy needs to listen. And I have every confidence he will.

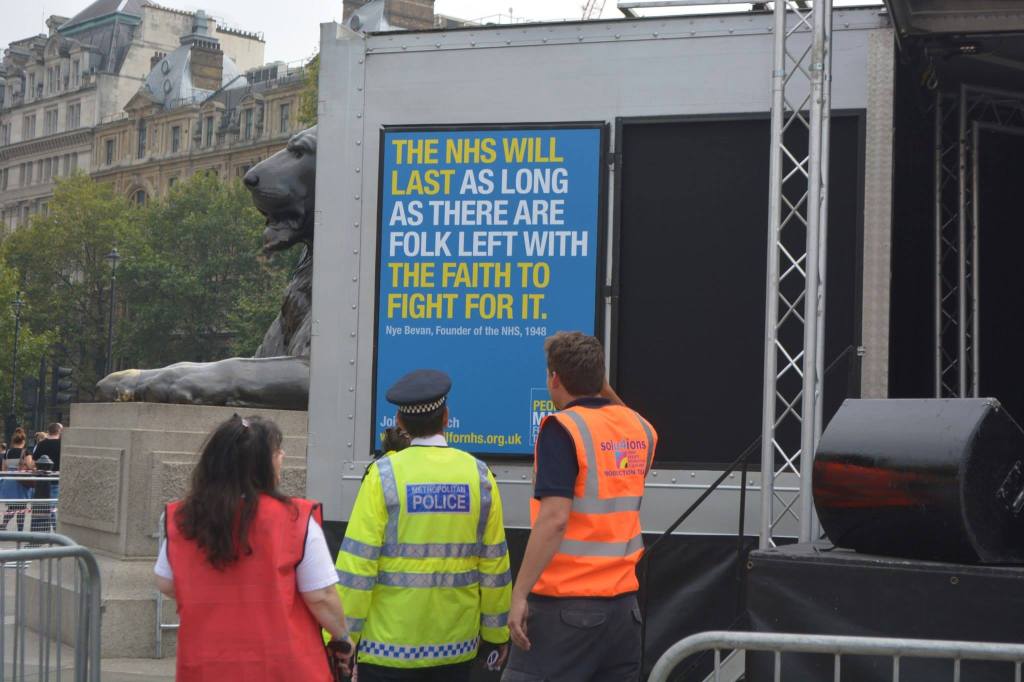
A triumph of optimism defeats cynicism as the Darlo Mums arrive in Trafalgar Square
The stench of sleaze from the backdoor lobbying culminating in the Health and Social Care Act (2012) was unable to overcome the sheer sense of euphoria and triumph of optimism defeating cynicism yesterday. Yesterday was history in the making, as all political parties were put on notice:
“Whose NHS is it? It’s our NHS”.
Whilst numerous governments have elaborated at length about the politics of ownership of public services, the message from the crowd of five thousand or so, within hearing distance of the Houses of Parliament, was loud and clear.
Many famous Labour members of parliament could be seen watching proceedings as the afternoon progressed, including Diane Abbot, Clive Efford, Jeremy Corbyn, Sadiq Khan, as pictured here.

It was a very sunny day here in Central London. There was a charged sense of energy, optimism and solidarity as about five thousand people attended a pro-NHS rally in Trafalgar Square, the culmination of a 300-mile march organised by a group of mothers from County Durham.
The group from Darlington, the Darlo Mums, are opposingthe privatisation of the NHS. It was very emotional when Rehana Azam announced the names of the Darlo Mums, “the most amazing people I’ve just spent the last three weeks with.”
The warmth of the #999CallfortheNHS campaign was evident throughout the whole afternoon. The event was immaculately organised, and was a thoroughly enjoyable event for all.

About 30 people had taken three weeks to march the full 300 miles from Jarrow in South Tyneside, organisers said.
Darlo Mums founder Joanna Adams said: “It’s been magic really. You only have to look over there [at the protesters gathered] to see people are behind the NHS and support what we’re saying. Joanna Adams described the mums as “ordinary”, but I beg to differ – they are entirely extraordinary in my opinion.
Andy Burnham MP, Shadow Secretary of State for Health, broke off all prior arrangements to attend, emphasising the indecency that would have occurred had he not come to represent the political party which had legislated for the birth of the NHS in 1945. Burnham’s speech was equally positive and optimistic about the future, speaking of the need to remedy public over privatisation, integration over fragmentation, people before profit, and collaboration over competition. Again, as is usual for Burnham who has great political gravitas, there was a sense of the current Government simply treading water in office until a person with substantial experience resumes office once again.
Burnham emphasised yet again that an incoming Labour government will repeal the Health and Social Care Act (2012) in its first Queen Speech, and said that it would then negotiate the UK out of TTIP, the transatlantic US-EU free trade treaty. Currently discussions are held in secret.
Sadiq Khan MP said the #Darlomums were the best England have had since 1966. As the MP for Tooting, Khan has been an ideal position to witness the effect the NHS changes have had on the nation’s capital.
Clive Efford MP described his Private Member’s Bill to repeal the damaging competition rules that the Tory-led Government inflicted on the NHS in its Health and Social Care Act 2012. The speech was very well received.

Even Dr Clive Peedell, Co-Chair of the NHS Action Party, called Andy Burnham’s speech “great”, having run 66 km himself to be there. It was announced that Dr Louise Irvine, an inner city GP and BMA council member, would be standing against Jeremy Hunt MP in the South West Surrey seat. Dr Peedell has of course seen at first hand the impact his specialty (oncology) has had on national politics, in the case of Aysha King.
And in the court of public opinion, according to the Daily Mirror last night, Dr Irvine was significantly more popular than Jeremy Hunt. We do know, of course, that the Daily Mirror do not comprise natural friends of Jeremy Hunt.

‘We keep on being told the NHS is unaffordable. THAT IS A LIE.”, said Rufus Hound. This lie has of course been one of the most powerful tools of the media who have called the consistent underfunding of services “unsustainable”.


Billy Bragg warned against blaming all cynicism on what one read in the media, saying that much cynicism was in people’s hearts – and this remained an obstacle for change.
Rehana Azam, as one of the marchers, NHS campaigner and leading light in GMB, and working mum, was one of the stars of yesterday’s event, explaining the necessary steps to get the NHS back on track.
Andy Slaughter, MP for Hammersmith and Fulham, recounted the demolition of his local NHS services, whilst Grahame Morris gave his account, as MP for Easington, of the fight against the Tories to protect the NHS. Andy Slaughter of course has a huge following in West London, and one of the key organisers of yesterday’s event Jos Bell was obviously pleased with the success of the event together with Andy Slaughter.
And finally, Question Musiq explained how he owes his life to the fast action of the Lewisham Hospital A&E in diagnosing his burst appendix, and performed his catchy rap song. Proceeds go to the Lewisham campaign.
A huge well done to everyone! A truly inspiring and memorable event.
Photos from the event









Dementia care in the whole person care age
The Australian jurisdiction have recently provided some helpful inroads here.
The narrative has changed from one of incessantly referring to people living with dementia as a ‘burden’ on the rest of society. For example, to push a sense of urgency that we have an ‘ageing population timebomb’, the cost of the ageing people with dementia flies completely in the face of other public health campaigns which emphasise, for example, “dementia is not a natural part of ageing”.
“The NHS as a whole and individual hospitals recognise that dementia is a significant, growing and costly problem for them” is the opening gambit of the Alzheimer’s Society “Counting the cost” report.
An easy to use online resource, Valuing People from Alzheimer’s Australia has been developed in collaboration with community aged care providers who have helpful in stablishing a person centred approach to service delivery.
Person centred care is a development to provide ervices provided in a way that is respectful of, and responsive to, the preferences, needs and values of people and those in the care and support network.
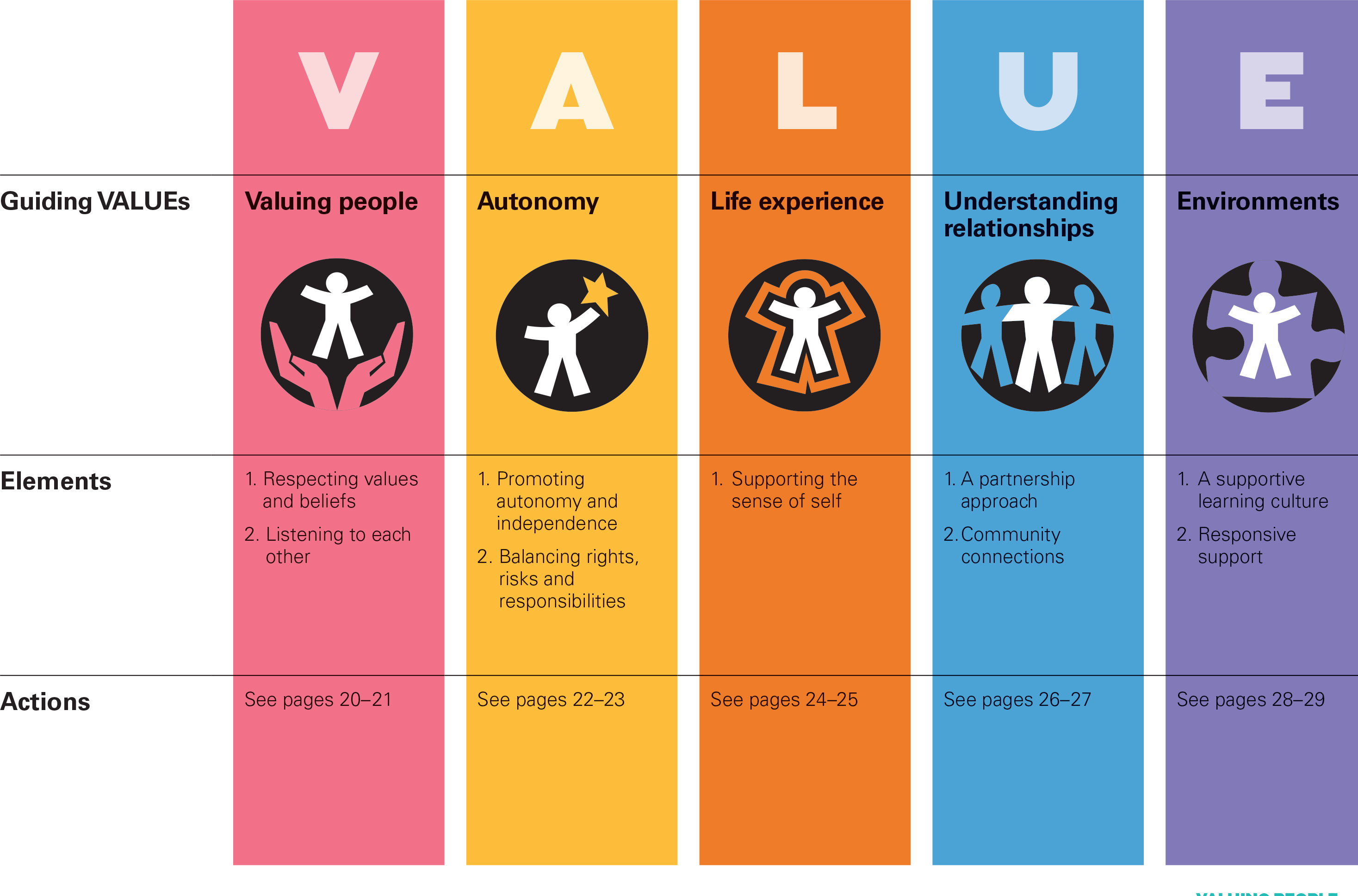
I cannot recommend this resource highly enough. The main source is here.
In fact, it summarises succinctly the conclusions I came to after my exploration of personhood in my book ‘Living well with dementia’. The late great Prof Tom Kitwood said of personhood, “It is a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being. It implies recognition, respect and trust”.
If a Labour government is elected on May 8th 2015, the first necessary step is to legislate for the repeal of the Health and Social Care Act (2012) and to enact new legislation to allow for integrated packages provided they are justified by clinical outcome. For this to happen, it will be necessary for Labour to undergo a ‘conscious uncoupling’ from all the baggage of EU competition law. For this, it is essential also that the UK government is able to carve out provisions from the investor protection clauses and/or the rest of the EU-US free trade treaty (TTIP).
The “whole person care model” has become attractive to those who wish to break down silos between different physical health, mental health and social care “silos”. It has been worked up in various guises by various parties.
A helpful construct is provided in the document, “Healthcare for complex populations: the power of whole-person care models” originally published by Booz & Company in 2013.
A major problem with dementia care, however it is delivered, is that it is full of divisions: public vs private care, fragmented vs national care, competitive vs integrated models. Operating in silos can’t work because of the nature of the dementias: the mood and cognition of a person with dementia profoundly affects how they might interact with the outside world, for example perform activities in the outside world. And we know that taking part in leisure activities can promote a good quality of life.
Their model is, though, a useful starting point.

Dementia cannot be only addressed by the medical model. In fact, it is my sincere belief that it would be highly dangerous to put all your eggs in the physical health basket, without due attention to mental health or social care. For example, last week in Stockholm, the international conference on Parkinson’s disease, a condition typified by a resting tremor, rigidity and slowness of movement, which can progress to a dementia, often is found to have as heralding symptoms changes in cognition and mood.
So it’s pretty clear to me that we will have to embark on a system of multidisciplinary professionals who could all have a part to play in the wellbeing of a person with dementia, depending on his or her own stage in life, and ability or need to live independently. “Care coordinators” have traditionally been defined incredibly badly, but we do need such an identity to navigate people with dementia, and actors in the care and support network, through the maze.
“Care collaborators” in their construct are very wonkily articulated, like “pre-distribution”, but the concept is not stupid. In fact it is very good. One idea is that people with dementia could act as support as other people with dementia, for people on receiving a diagnosis of dementia. The rationale for this is that people living with long term conditions, such as for example recovery from alcoholism, often draw much support from other people living with other long term conditions, away from a medical model. There needs to be safeguards in the system to safeguard against a lot of unpaid goodwill (which currently exists in the system.)
Informatics would have a really helpful rôle here, being worked up in telecare and assistive technology. But even simple disruptions such as a person living with dementia at risk of falling from problems with spatial depth perception being able to ‘hot email’ a care coordinator about perceived problems could trigger, say, an early warning system. And with various agents in the provision of care being involved in differing extents it will be up to NHS England to work out how best to implement a single accountable tariff. Falls are just the sort of ‘outcome metric’ which could be used to determine whether this policy of ‘whole person care’ for people living with dementia is working. And, even though everyone ‘trots it out’, the performance on avoided hospital admissions could be put into the mixer. It’s already well recognised that people with dementia can become very disoriented in hospital, and, and despite the best efforts of those trying to improve the acute care pathway, people with dementia can often be better off away from hospital in the community. But it’s imperative that care in the community is not a second-rate service compared to secondary care, and proper resourcing of community whole person care is essential for this before any reconfiguration in acute hospital services.
But the private sector has become such a ‘bogey term’ after arguably the current Government overplayed their hand with the £3bn Act of parliament which turbo-boosted a transfer of resource allocation from the public to private sector. Any incoming government will have to be particularly sensitive to this, as this is a risk in strategy for the NHS.
In October 2005, Harold Sirkin, Perry Keenan and Alan Jackson published a highly influential article in the Harvard Business Review entitled “The hard side of change management“. Whilst much play has in fact been made of politicians having to be distant from running the NHS, a completely lubricous line of attack when it is alleged that Jeremy Hunt talks regularly to senior managers and regulators in the NHS, the benefits of clear political leadership from an incoming Labour government are clear.
Andy Burnham MP has already nailed his colours to the mast of ‘whole person care’ on various occasions, and it is clear that the success of this ambitious large scale transformation depends on clear leadership and teamwork from bright managers. Take for example the DICE criteria from Sirkin, Keenan and Jackson:

But this is perfectly possible from an incoming Government. The National Health Service has a chance to lead on something truly innovative, learning from the experience of other jurisdictions such as Australia and the USA.
As alluded to in the new resource from the Alzheimer’s Australia, this cultural change will require substantial ‘unfreezing’ from the current mindset for provision of care for people with dementia. It will require a change in explicit and implicit sources of knowledge and behaviours, and will need to be carefully brought about by learning from the successes and failures of pockets of implementation.
The whole project’s pretty high risk, but the rewards for people living with dementia, and members of the care and support network, are potentially vast. But it does require the implementation of a very clear vision.
[First posted on the 'Living well with dementia' blog]
Care at the crossroads. Burnham has something big, and you may be quite pleased to see him
Social care funding is on its knees.
Andy Burnham MP, Shadow Secretary of State for Health, addressed a sympathetic audience at the #NHSConfed2014 yesterday, talking about unlocking resources for general medicine.
We live in crazy times. Newark saw the christening of the Conservative Party as the protest party you should vote if you wanted to STOP UKIP. But let me take you back to an era when the Labour Party had principles (!) In August 1945, Aneurin Bevan was made Minster for Health following the 1945 General Election. The National Health Service (NHS) was one of the major achievements of Clement Attlee’s Labour government. By July 1948, Minister for Health, Aneurin Bevan had helped guide the National Health Service Act through Parliament.
A full day has been allocated to the Opposition health on Monday in parliament in part of their discussions on her Majesty’s Gracious Speech. Simon Stevens – NHS England’s new chief – has asked for solutions for well rehearsed issues, and Andy Burnham is clear that this is no time for another apprentice like Jeremy Hunt. Whilst being upbeat about the future of the health and social care system, he wants to move away from a “malnourished system”, with carers employed on zero hours contracts and less than the minimum wage. Indeed, this is a serious issue which has caused me some considerably anxiety too. A “product of [my] time in Government”, clearly this framework has also benefited from a parliamentary term in opposition.
Burnham crucially identifies not an inefficiency in which money is spent (although the ongoing Nicholson savings rumble on). But he does identify an inefficiency in outcomes (such as the near-inevitable fractured neck of the femur in the leg for a seemingly-trivial cost-saving in not purchasing a grab handrail). Labour, inevitably, though has an uphill battle now. The system appears to encourage the medical model of care, according to Burnham, encourages hospitalisation of people, so it is not simply a question of throwing money at the service. People are more than aware that an ‘unsustainable NHS’ is in a nutshell code for a NHS starved of adequate fundings.
Burnham feels that you can’t half-believe in ‘integration’, and is mollified about the consensus about a need for integration across all main political parties.
“I am really worried that the ‘Better Care Fund‘ might give integration a bad name”, comments Burnham.
People who have watching Burnham’s comments will note how Burnham has openly commented how he feels he has been misled by certain think-tanks in the past. A period of opposition has enabled Burnham conversely to obtain a crisis of insight. And yet he talks about his “precious moment” in order “to build a consensus of shared endeavour, which I intend to use to the full and very carefully.” Intriguingly, he does not wish to ‘foist a grand plan’ on voters after the next general election. This is of course is political speak for his ‘shared agenda’, driving a cultural change by stakeholders within the system. This is precisely what Burnham feels he has achieved through the commission on whole person care by Sir John Oldham.
“Not a medical or a treatment model, but a truly preventative service, that can at last aspire to give people a state of physical, mental and social wellbeing.”
Burnham wants to put a stop to the ‘random set of disconnected meetings with individuals within the service.’
An exercise was carried out at the start of the NHS.
This is the famous leaflet.
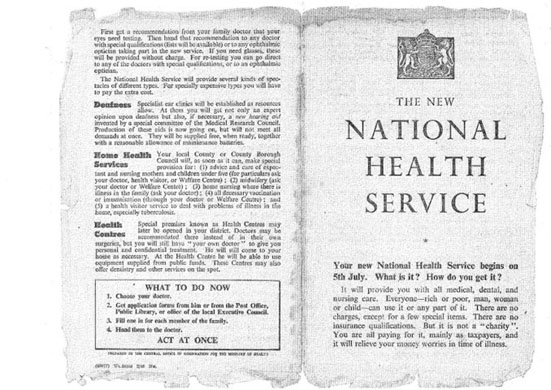
Burnham desires a new leaflet from an incoming Labour government to introduce how social care can become under the umbrella of the National Health Service.
“Going forward, you should expect to receive much more support in your home. The NHS will work to assemble one team to look after you covering all the needs you have. We want to build a personal solution that works for you, for your family, and for your carers, because if we get right at the very outset and the very beginning it’s more likely to work for you and give you what you want, and cost us all much less. We want you to have one point of contact for the co-ordination of your care. We know you are fed up with telling the same story to everyone who comes through the door. It’s frustrating for you, and wasteful for us. To get the care that you’re entitled to, when and where you want it, you will have powerful new rights set out in the NHS Constitution such as the right to a single point of contact for the coordination of all of your care and a personalised care plan that you have signed off. But – and there is a big but – to make of all this happen, you will changes in your local NHS, and, in particular, you will changes in your local hospital. We can do a better job of supporting you where you want to be, we won’t need to carry out as much treatment in hospitals, or have as many hospital beds. It is only by allowing the NHS to make this kind of change to move from hospital to home that we will all secure it for the rest of this century.”
Burnham feels that the NHS must be the ‘preferred provider’ and the DGH should be allowed to reinvent itself - building the notion of one team around the person. I personally have formed the opinion: “close smaller hospitals at haste, and repent at leisure“. Critics of marketisation will inevitably point out the blindingly obvious: that even with a NHS preferred provider, there’s still a market, and nothing short of abolition of the purchaser-provider split will remedy the faultlines. There could be a one person tariff or one person budget for a person for a year. It would give an acute trust a much more stable platform, according to Burnham, in contradistinction to the activity based tariff. This does require some rejigging of how we have the proper financial performance management system in place: there should be a drive, I feel, for rewarding behaviours in the system that promote good health rather than rewarding disproportionately the work necessary to deal with failures of good control, such as dialysis, amputations or laser treatment.
Burnham is clearly inspired by the ‘Future Hospitals’ soundings from the Royal Colleges of Physicians, focused on a new generation of generalist doctors working across boundaries of primary and secondary care:
“Since its inception, the NHS has had to adapt to reconcile the changing needs of patients with advances in medical science. Change and the evolution of services is the backbone of the NHS. Hospitals need to meet the requirements of their local population, while providing specialised services to a much larger geographical catchment area.”
Burnham even talks about possibly reviewing the “independent contractor” status of GPs.
Centralised care is mooted for people in life threatening situations. But Burnham has found that barriers to service reconfiguration exist through the current competition régime and market, with integration encouraging in contrast to collaboration, people before profit, and merge “without the nonsense of competition lawyers looking over their shoulders”. Therefore, Burnham repeats his pledge to remove the Health and Social Care Act (2012), which has driven “fragmentation, complexity and greater cost”. Under this construct, section 75 and its associated Regulations is disabling rather than enabling for health policy. There is clearly much work to be done here to make the legislation fit for purpose, as indeed I have discussed previously. Wider dangers are at play, as Burnham well knows, however. Here he is speaking about his opposition to TTIP (the EU-US Free Trade Treaty) which the BBC News did not seed fit to cover despite their Charter requirements for public broadcasting. And here is George Eaton writing about his opposition to TTIP in the New Statesman.
Burnham is clearly, to me, positioning himself to the left, distancing himself from previous Labour administrations. There are clearly budgets in the system somewhere, and while Burnham talks about unified budgets he does not put the emphasis on personal budgets. There is no doubt to me that personal budgets can never be ‘compulsory’, and each person group (e.g. people living with dementia) presents with unique challenges. It’s clear to me that deep down Andy Burnham is still in principle keen on something like the ‘National Care Service’, in preference to any gimmicks from the Cabinet Office. Burnham in the Q/A session with Anita Anand indeed describes how this had been thrown into the long grass at the time of Labour losing the general election in 2010, but how paying for social care in 2014 is as fundamentally unfair as paying for medicine had been pre-NHS according to Burnham. This would take some time to put in place, such as a mechanism for a mandatory insurance system, and a proper care coordinator infrastructure. And these are not without their own controversies. But, with Miliband playing safe one unintended consequence for neoliberal fanatics has been that it has not been possible to impose a strong neoliberal thrust to whole person care; and whatever Miliband’s personal preferences, the pendulum to me is definitely swinging to the left. Burnham talks specifically about a well planned social care system as part of the NHS.
And so Burnham looks genuinely burnt by previous administrations, and, whilst certain key players will want personal budgets and competition to be playing a greater part in policy, it appears to me that the current mood music is for Labour not appearing to promote privatisation of the NHS in any form. The ultimate success of the next Labour administration will be determined by the clout of the Chancellor of Exchequer, whoever that is. It could yet be Ed Balls. For matters such as ‘purse strings’ on the social impact value bond or the private finance initiative, Burnham may have to slog out painful issues with Balls in the way that Aneurin Bevan once did with Ernie Bevin in a previous Labour existence. Burnham’s problem is ensuring continuity with the current system where services have been proactively pimped out to the private sector, but ultimately it is the general public who call the shots. Burnham knows he’s onto something big, and, for once, some people may be quite pleased to see him.
Burnham goes from strength to strength as ‘striker’, but who’s the David Moyes?
There’s no doubt Andy Burnham MP drives the Conservatives potty.
Despite the Conservatives’ best attempts to annihilate Burnham MP, Burnham keeps on scoring goals.
Meanwhile Jeremy Hunt continues to score blanks, apart from where profits from ‘Hot Courses’ are concerned.
But Burnham is more concerned about the day job, and that is running the NHS to a level of some degree of competence.
Hunt meanwhile continues to run his NHS into the ground, paying for costly advice on the managerial implementation of compassion, when he could be paying nurses to do the professional job they’re trained to do.
So Burnham can certainly hold his head up high as chief striker or scorer for Labour United.
As the Conservatives spit out the oranges from their half-time pep talk, as the oranges were in fact horsemeat due to the abolished Food Safety Agency, it’s time to recapitulate.

Clive Peedell kindly tweeted the other day points on which he would like Labour to play ball.
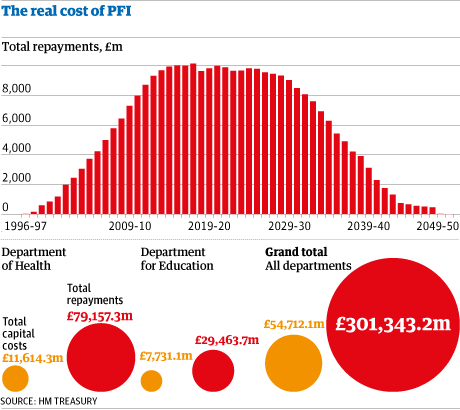
@legalaware @andyburnhammp 1. Fill £30bn funding gap by abolishing PFI & cracking down on tax avoidance 2. Get NHS exempted from TTIP
— Clive Peedell (@cpeedell) April 22, 2014
Before the 2010 election, Liberal Democrat leader Nick Clegg indeed condemned PFI as “a bit of dodgy accounting – a way in which the government can pretend they’re not borrowing when they are, and we’ll all be picking up the tab in 30 years”. It’s well known that PFI is a relic of the John Major government from 1995 (predating New Labour in fact). In opposition, Osborne pledged that the Conservatives would stop using PFI and denounced Labour for relying so much on a source of finance that he said was “totally discredited”. “We need to find new ways to leverage private-sector investment. Labour’s PFI model is flawed and must be replaced,” Osborne muttered in November 2009. Indeed Margaret Hodge, chair of the powerful Commons public accounts committee, said the coalition had failed to come up with the promised alternative since coming to power. The facts speak for themselves.
And Burnham is handicapped by not being the actual Secretary of State for Health at this crucial time for the NHS.
He nonetheless did go to Strasbourg last month to try to explain the case:
(This is a video recording I took of Andy’s talk at the Southwark Labour meeting recently.)
Labour will need to abolish PFI contracts or renegotiate them or both. But Ed Balls will need to be on the wing to help Burnham shoot. And it’s hoped the football manager is not asleep on the job. Labour has indeed proposed a five point plan to tackle ‘tax avoidance’. Labour supports a form of country-by-country reporting. It would extend the Disclosure of Tax Avoidance Schemes regime, which Labour introduced, to global transactions. It would open, further, open up tax havens, with requirements to pass on information about money which is hidden behind front companies or trusts. Crucially, Labour also wants to see fundamental reform of the corporate tax system. But Peedell’s work is not done.
@legalaware @andyburnhammp 3. Abolish purchaser provider split 4. Improve NHS accountability with transparency & openness — Clive Peedell (@cpeedell) April 22, 2014
The abolition of the purchaser-provider split remains one of the totemic political decisions to be made, as is not a ‘deal maker’ for many grassroots voters.
In fact, the whole issue of whether the general public is interested by public health or competition remains uncertain.
Nonetheless, a pioneering integrated healthcare scheme in New Zealand has improved the care of patients while reducing demand on hospital services.
On the contracting side, the report said that the abolition of the purchaser-provider split in the health system was important as it gave boards the autonomy to decide how to fund their hospitals.
The project was launched in 2007 in response to rising hospital admissions and waiting times and to a population that was ageing more rapidly than in other parts of New Zealand and other developed countries.
Similar to the drive towards whole person care in this jurisdiction, is aim was to create a “one system, one budget” approach to health and social care, together with various aspects as centrepieces: sustained investment in training, support for staff to innovate, and new forms of contracting, including abolition of the split between healthcare service purchasers and providers.
The outgoing NHS England chief executive Sir David Nicholson last year told HSJ his organisation was looking at “whether the straightforward commissioner-provider split is the right thing for all communities”.
Hospitals wish to focus on delivering better services to patients and often get frustrated by the amount of time they have to spend negotiating contracts with commissioners with the legal shutgun pointing in the direction of their necks.
And there’s no doubt there’s a steady stream of whistleblower tragedies, with Raj Mattu the latest in the long line of casualties.
People still struggle to think of a NHS whistleblower who has had a good outcome.
The Nursing Times ‘Speak Out Safely’ has only so far succeeded in signing up 30% of NHS Trusts.
Most people accept that the whole system is rotten, not least in how clinical regulators appear to pass the buck or even worse target whistleblowers.
Many do not think the Public Interest Disclosure Act, enacted by New Labour is 1998, is fit for purpose either.
So Clive Peedell is right, but Andy Burnham may have trouble in shooting goals on target with nobody on wing or a manager more concerned about ‘One Nation’.
Moyes, sacked by United on Tuesday after the 2-0 defeat at former club Everton on Sunday confirmed their failure to secure Champions League qualification, oversaw just 51 games in charge of the team after succeeding Sir Alex Ferguson last summer.
Moyes, like Ed Miliband, though had his army of people who thought he was doing a good job.
But Burnham like many, although focused on sorting out the undeniable problems of the NHS, is avoiding relegation for his team too.
I certainly don’t want to ask who the Ryan Giggs is. That certainly would be tempting fate.
I agree. The effects of the free market on the NHS are indeed terrifying.
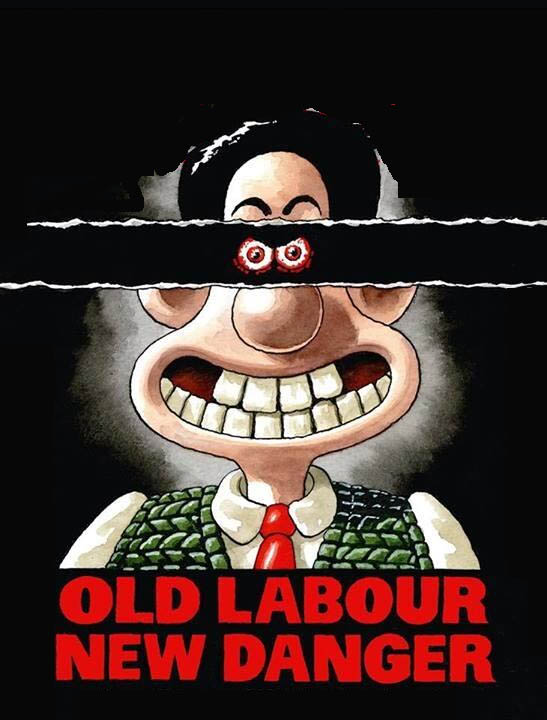
Tony Benn said famously, of Tony Blair, “It’s not up to Mr Blair to rename my party. I haven’t suddenly become a member of New Labour. I was never a member of Old Labour.”
There is a therefore a strange cognitive dissonance in this picture to come out of the Spectator factory.
It mixes a parody of the famous Tony Blair ‘evil stare’ with the letters ‘Old Labour’.
Presumably the overall message, unsubtle though it is, is that a vote for Ed Miliband is a vote for socialism.
And the advertising shill in this is that socialism represents a ‘danger’.
No.
Let’s get this clear.
The private finance initiatives led to some investors in the private sector making very good deals on the financing of hospitals and associated services, often with exorbitant profit.
Andy Burnham’s message of letting the market creep in too far is understating the severity of the problem.
There is a plethora of NHS trusts which have been crippled by PFI loan repayment debts.
These loan repayments possibly represent the biggest single threat to the financial stability of the NHS in the forthcoming decades, not the ageing population.
The PFI situation has gone beyond farcicle. An instrument first developed in John Major’s government in 1995, later welcomed with open arms by Tony Blair’s governments and beyond, has clearly been an abuse of power.
Not only can NHS entities conceal their staffing data under freedom of information, but PFI shares in hospitals which may ultimately shut down may be freely traded like carbon credits on the stock market.
That’s what letting the market has become.
You can now hire consultants who are experts and could make you millions on predicting whether your local hospital will shut.
There is no doubt that these market considerations have impacted on the provision of care, which should be made on clinical conditions. And yet the current regulatory set up, which gives a lot of power to Monitor’s elbow, is clearly unable to cope.
It is now widely recognised that the NHS has lacked both the expertise and the resources to cope with the aggressive pimping of services into the private sector.
And private investors are now lining up to provide financing for social value impact bonds, which could help to sustain multinational corporates to enter markets they otherwise would have dreamt of.
This further leads to leeching out of resources away from the NHS to the private sector.
So long as senior leaders in the NHS say technology and innovation need to drive the NHS, you will see further leeching of money into the private markets.
This shift on emphasis, to people ‘finding opportunities in the NHS’, is by far the biggest danger in the NHS. And the political dynamite question is to what extent does Ed Miliband produce a killer stroke?
Everyone concedes the PFI situation is a mess, but should Miliband simply buy back these hospitals into the public sector?
After all buying back shares is common currency currently in corporate land, pardon the pun.
And there is never any shortage of money for illegal wars.
That would be quite a break from New Labour, but the public, and the Spectator know this, might actually welcome a return to state ownership. This is borne out by all the polling evidence in fact.
Despite the undeniable popularity of issues such as immigration considered to be “right wing”, the Spectator might have done Labour a favour – in telling Labour that the Tories are in fact terrified of Miliband and Burnham.
Will Clive Peedell reply to Andy Burnham’s tweet?
It’s fairly well known that Ed Miliband is firmly fixed on the general election in the UK, to be held on May 7th 2015.
But, of course, he is aware of the impact that the European Elections can have, which can act as a useful barometer of the level of unpopularity at the current political incumbents.
On 29 December 2013, Andy Burnham MP tweeted at the NHA Party to ‘RT if you agree‘ if there needed to be a “broad campaign against market forces”:

It received 454 RTs.
But it did come across Clive Peedell’s RADAR. Clive is the co-chair of the National Health Action Party.
It was shared by Clive the same day in fact.

It received 20 RTs.
Clive has 12.1K followers.
Andy has 54.9 K followers.
To my knowledge, I don’t think the NHA Party or Clive ever took up Andy on the offer or replied to the tweet (but I could be wrong.)
But here, Louise Irvine, MEP candidate for the European Elections, who was the lead for the Save Lewisham campaign against Jeremy Hunt in the High Court and the Court of Appeal clearly has many of the same reservations as Labour and Andy Burnham.
Irvine is critical of how clause 118 (now clause 119), a legislative step would allow ‘unaccountable bureaucrats’ to make decisions about NHS reconfigurations, and an “acceleration of privatisation”.
She is also highly critical of the EU-US ‘free trade agreement’, which will ‘lock in privatisation, whereby ‘private companies could sue the British government”.
“Labour is in a muddle. It is a partly committed to the NHS, but feels it can flirt with privatisation.”
But Andy Burnham MP, Shadow Secretary of State for Health, recently rocked up at the Bermondsey Village Hall in 12th April 2014.
Burnham argued that “we need MEPs to protect the NHS from the EU-US free trade treaty.”
Burnham made special reference to the Lewisham campaign, mentioning a key campaigner in his speech, calling it a ‘famous victory… which was a message to an arrogant government.”
He also spoke of ‘unprecedented pressure in A&E’ in London, due to “massive cuts in primary care”.
And 8 mins 4 secs in, Burnham began a massive tirade on the aspects of the EU-US free trade treaty which he argued would damage our interests in the NHS:
“I have said that, before, even I think we let the market in too far into the NHS.”
“We can’t carry on letting this happen, or if – we do – it will devour the NHS and everything that is precious about it.”
“That’s why I am absolutely clear that the NHS has to be seen as a ‘preferred provider’. We repeal the Health and Social Care Act (2012).”
“Labour proudly stands for a public NHS again. That’s where we should be, and there’s where I want you to be too, fighting the privatisation.”
“That’s important for the European elections too. If we don’t get the European Parliament with our MEPs in it, the threat goes up to an whole different level.”
“Why? Our ability to protect the NHS moves to fall out of our hands. Why? – it’s because of this trade treaty that is being negotiated in Brussels right now; it’s between the EU and US which has some positive aims but, if it stays at it is, it could have the effect of opening up the NHS to US corporate entities.”
In the second Farage-Clegg debate on the BBC, Farage was vehemently anti-multinational corporations, but Burnham later remarks that UKIP have said previously the NHS should be ‘put out to tender’.
Burnham continues, “The issue – it’s the combination of the two entitires. The Health and Social Care Act having exposed the NHS to the full glare of the EU competition law, and then the US-EU free trade treaty, and then we are in a totally different world, and our ability, as I say, to protect the NHS has gone. It’s that serious.”
Burnham then talks about his ‘good hearing’ to argue for an exemption for the NHS from this legislation.
“They’ve said that the NHS should be in the scope of the EU-US free trade treaty. The LibDems have said nothing.”
The National Health Action Party appears to have blamed Labour too for contributing to the privatisation of the NHS.
However, it is currently unclear whether the Party as a whole is grandstanding as a protest vote in a ‘plague on all your houses’ way, or is offering constructive solutions to move things forward.
Clive Peedell has often spoken about his shared vision of Bevan for a public NHS.
Many of us in Labour like Clive much, so it will be interesting how things progress from here.

Thanks to Andy Burnham for emphasising “care co-ordinators” which I feel are pivotal to living well with dementia
This morning I had a present for Andy Burnham MP (@andyburnhammp), about to lead the Labour troops into battle for the European elections. The present is of course a copy of my book ‘Living well with dementia’, which is an account of the importance of personhood and the environment for a person living with dementia.



In my article entitled “Living well = greater wellbeing” for the ETHOS Journal (@ETHOSJournal), I highlighted the critical importance of the ‘care coordinator':
“So, if one had unlimited funds, what sort of service could be designed to provide care and support for people with dementia? In my opinion, the answer is a very different one. Ideally, all services, which could include healthcare, housing and legal systems, would adapt quickly and flexibly according to the needs of the individual living with dementia. This would need to be managed by a named, long-term co-ordinator of care and support.”
In reply to my article, Paul Burstow MP commented helpfully:
“The idea of a care navigator able to call on and coordinate all available health and social care, as well as housing support and voluntary sector provision is a persuasive one. It is something that the Richmond Group of charities, among others, have for a long time called for – and it is something I would like to see the Liberal Democrats deliver in the next government. Better managed and coordinated care would be a huge step forward and could make all the difference to dementia sufferers and their often strained carers.”
And Andy gave it much prominence this morning:
The King’s Fund (@TheKingsFund) has previously looked into co-ordinated care for chronic conditions.
In this framework, a “care co-ordinator” acts as a single point of contact and works with the patient, their carer(s) and the multidisciplinary team to develop a care plan.
Once this has been agreed, the co-ordinators work with the team, the patient, the patient’s family and other care providers to deliver co-ordinated and coherent care. Personal continuity of care is actively encouraged, and the care teams work hard to ensure an immediate response to care needs as they arise.
The care co-ordinator becomes he patient’s advocate in navigating across multiple services and settings ??providing care directly in the home environment.
He or she also ??communicates with the wider network of providers (outside of the core multidisciplinary team) so that information about the patient/carer is shared and any actions required are followed up.
The King’s Fund has previously found that the type of person undertaking the care co-ordination function varied greatly.
Most care co-ordinators had been community or specialist nurses, yet the role has also been taken on by non-clinical ‘link workers’ (in Sandwell) and health and social care co-ordinators (in Torbay).
There also appears to be a continuum from the non-clinical approach – primarily providing personal continuity to service users and acting as their advocate to ensure that care is co-ordinated around their needs – to the clinical approach, in which a case manager would also be able to provide clinical care directly.
This, I feel, is significant, as my book ‘Living well with dementia’ has a very non-medical thrust.
It’s very much a n0n-authoritarian, non-hierarchical approach where each person, including the person living with dementia, has an important part to play.
Influences on someone living well with dementia might include design of a home or ward, assistive technologies, ambient-assisted living, “dementia friendly communities”, for example.
With the introduction of ‘whole person care’, it’s possible that the care co-ordinator for a person living well with dementia might become a reality.
In this construct, Andy Burnham MP, Shadow Secretary of State for Health, is trying to stop the overhospitalisation (and overmedicalisation) of people.
