Home » Dementia (Page 3)

Continuity of care and support is vital in dementia policy. We are a long way from that.


In a way, the second ever English dementia policy poses more of an acid test than the first one. The reason for this is because we already have a set of yardsticks by which the first five years can be assessed, with a view to projecting forewards.
I don’t doubt the enthusiasm with which we have tried to close the ‘diagnosis gap’ in England. The heart of this is the high quality diagnosis, as stipulated in the original policy co-authored by Prof Sube Banerjee at Brighton and Sussex Medical School. What we have tended towards, rather, is a culture of high volume mediocre quality. And people readily admit they would rather wait that little bit longer to get the correct diagnosis.
I do not subscribe to the idea that anyone can easily make a diagnosis of dementia. When a diagnosis of dementia is finally given, it’s given not just to the person with dementia, but to his or her friends, or her family. As Kate Swaffer says, she is not a person with dementia primarily; she is a person with friends, family and feelings.
This approach prioritising the person has to be right from the word go. We are all persons, but we become patients when we become ill enough to present to the health and care services or not. We become paying consumers when we part with money. We are consumers if we spend any resources from the pot of money paid into from national insurance.
And so on. This analysis of money is a sideshow only as far as to how to service is delivered is actually matters. If you have services in dementia and support commissioned in a highly piecemeal manner, at worst from clinical commissioning groups who don’t know what wellbeing is, nor what they’re looking for, it can be a mess.
The hunt is definitely on for effective commissioning as well as any commissioning at all. The next Government will have to provide much better clarity on this, and some objective guidelines on how, say, the delivery of wellbeing might be ensured on an ongoing basis, not just at the start and finish of a commissioning contract.
But it is the fragmented approach from different providers which is a threat. Low pay of carers, not meeting the national minimum wage, or zero hour contracts, is a problem, and the reason specifically why private providers can be an issue here is that large corporates with scrupulous employment practices can hide behind a veil of being unperturbed from freedom of information legislation.
It is very easy to argue that entire health policy, and even dementia policy, is not political. I don’t believe this is justifiable for a minute. How we prioritise care at all is a reflection of our collective solidarity as a society, and our success in ‘pooling risk’. If I know for example I have a high genetic risk of developing a dementia from my genetic make up, my insurance premiums is likely to go through the roof unless there is tight anti-genetic discrimination law in place in England (which there isn’t).
Having a piecemeal system promotes lack of continuity of care. I think this is fatal for any new English dementia strategy. I think this piecemeal system, whether an artefact of private markets or not, or political ideology, can adversely affect people living with dementia and carers in a number of different ways.
First of all, the caregiver relationship, whether paid or unpaid as carer, fundamentally depends on that caregiver knowing the person with dementia. The happiest relatives I have ever spoken to are the ones who report that they haven’t had a regular changing of the guard as regard carers. This is important for building meaningful relationships with time, as people with Alzheimer’s disease for much of their time, even if they have weak memories for events have strong enduring memories for emotions. Besides, change here can be very distressing, and mental distress can impact on lack of physical wellbeing (although ill being is not necessarily the same as lack of wellbeing).
Secondly, continuity of care by a physician or an appropriate specialist in clinical psychology acts as a safeguard to check the actual diagnosis is right. Some initial cognitive impairments do not progress – they remain mild. A ‘wrong diagnosis’ of dementia does not necessarily mean someone has goofed up as such – it could mean that something that was predicted to progress didn’t. The drive to diagnosing dementia, particularly with financial incentives, could mean we accidentally mislabel mild cognitive impairment as dementia, and this is clearly a tragedy for all involved.
Therefore, a diagnosis disclosure can never be a single hit and run event. There needs to be follow up from the system, whether it’s by the same GP, a hospital physician or psychiatrist, a different member of the memory clinic possibly somewhere totally different; a second ‘set of eyes’ to see whether the initial diagnosis is correct. Granted I agree that knowing what the diagnosis is can be the key to opening services, being armed with information and hence empowered, and all the usual arguments, but the diagnosis must be correct. There is no alternative on this.
Say, for example, you are in fact depressed, not living with dementia, and a clinician in a hurry informs you you are living with dementia. You have presented in response to the question, “Do you have problems with your memory?”. Such a misdiagnosis is likely to make you even more depressed; and not receiving effective treatment for depression, whether as a psychological therapy or medication, or otherwise.
Thirdly, somebody who knows a person well will be able to spot when a person with dementia changes in any way. This could be a ‘difference’, such as the development of a sweet tooth, a ‘deterioriation’ such as in memory, or even an ‘enhancement’ as in acquisition of a love of music, or artistic and creative talents. You can only ascertain this with time. This is where the idea of the review has to change fundamentally.
I don’t feel this review should take place in the hands of medics who repeat scans and tests, ask a few random questions, and document the decline (as dementia is progressive if it is not ‘reversible’ such as vitamin deficiency). Implementation of a ‘year of care’ for dementia, or a national network of clinical specialist nurses, will be able to manage a caseload of individuals living well in a pro-active fashion, each with an individualised care plan; where the goal is to live well, not to firefight in a crisis.
Fourthly, the fundamental crunch time for a person living with dementia is an inability to retain information for a decision, an inability to make that decision, and an inability to communicate that decision. The starting point is that we can make decisions or have ‘capacity’. This capacity can come or go; and it’s dangerous if we get into the mindset that capacity is all or nothing, but that is the legal shortcut we have in place.
But this capacity needs review on a regular basis, as it fundamentally changes our view as to whether a person can consent or not. People living with diffuse lewy body dementia, for example, can notice themselves one day they’re performing quite well, other days not so well. If we don’t get into the good practice of reviewing capacity and consent on a regular basis, through continuity of care, we will easily arrive at a situation where people are languishing inappropriately on medications. It’s generally felt that, while appropriate for some, antipsychotics prescribing is too high, often inappropriately; some side effects such as drooling of the mouth can be very distressing. It’s currently, rightly, a plank of policy to address the inappropriate prescription of antipsychotics particularly in care homes.
In summary, the ideal would be somebody to accompany a person from the point of diagnosis to the time of end of life; not chopping and changing. I was told by a senior specialist nurse at the National Hospital for Neurology and Neurosurgery, Katy Judd, that one of the most disturbing phenomena for persons with dementia and families is when their ‘contacts’ have ‘moved on’ on such a frequent basis. There clearly needs to be proper signposting with the system, known as care coordinators, but we need to avoid the situation where there is an abundance of signposts and a dearth of frontline care.
But I feel fundamentally continuity of care and support is critical. Having the same mutual followers on a social network on Twitter has the potential to improve wellbeing, and having somebody there by you that you trust is likely to have the same effect. People living with dementia who are stimulated psychologically by positive experiences are likely to find their experience fundamentally of a different nature to those who don’t.
For these reasons I feel that, whatever tactics are used, and whichever government is in office and/or power in England, for the next few years, an overall strategy of prioritising the continuity of care is pivotal.

Living better with dementia: a “Year of Care” for dementia?

This is an extract from my book ‘Living better with dementia’ by me (Forewords by Prof Alistair Burns, Kate Swaffer, Chris Mason and Dr Peter Gordon), to be published by Jessica Kinglsey Publishers 2015. It comes from the chapter on whole person care (chapter 10).
Acute medicine is ideally suited to the medical model where you make a diagnosis on the basis of investigations, and then you immediately implement a management plan. There should of course be prompt action on acute situations for people living with dementia, but this is rather different to the usual needs of a person trying to live better with dementia. A person with a long term condition “lives with the condition day by day for their whole life and it is the things they do or don’t do that will make the difference to their quality of life and the long term outcomes they will experience” (Royal College of General Practitioners, 2011).
Shirley Ayres (2014) argues in her article entitled “The long term care revolution: a provocation paper” that “people in later life offer wisdom, experience, perspective and a wide range of skill sets and capacities”, reflecting that that long term institutional care is not the correct setting for them. This argument also holds true, perhaps, for people living well with advanced dementia.
The burning question still remains, as it was in the genesis of the first English dementia strategy, how a framework of post-diagnostic support for people living with dementia could best take place in England. I have already discussed earlier in chapter 10 of my book the policy of ‘whole person care’, and the critical rôle of social care practitioners and clinical nursing specialists in a multidisciplinary approach. It is also worth noting that the “year of care” initiative has seen some crystallisation of the approach for living well. It offers a framework that supports delivery of the Domain 2 of the NHS Outcomes Framework ‘Enhancing quality of life for people with long-term conditions’. Through this, it is hoped that ‘far more people will have developed the knowledge, skills and confidence to manage their own health’, but there are clear implications for the implementation of whole person care, namely, “care which feels more joined-up to the users of services”, and “care [which] centres on the person as a whole, rather than on specific conditions” (Year of Care website, accessed December 2014).
There will always be the criticism that self management, rather than having the prime goal of encouraging health and wellbeing, is meant as a ‘cover’ for essential services being cut. Benefits of “self management” which have previously been proposed are, nonetheless, proposed in Box 1.
—————
Box 1. Benefits of ‘self management’ [Source: Royal College of General Practitioners (Clinical Innovation and Research Centre) (2011) (authors: Nigel Mathers, Sue Roberts, Isabel Hodkinson and Brian Karet) Care Planning: Improving the Lives of People with Long Term Conditions]
When people self care and are supported to do this, they are more likely to:
- experience better health and well-being
- reduce the perceived severity of their symptoms, including pain
- improve medicines compliance
- prevent the need for emergency health and social services
- prevent unnecessary hospital admissions
- have better planned and co-ordinated care
- remain in their own home
- have greater confidence and a sense of control
- have better mental health and less depression
—————
Indeed, this policy agenda has been slowly ‘cooking’ for about year. For example, nearly a decade ago, Department of Health (2005) issued its document “Supporting People and integration with Long Term Conditions – An NHS and Social Care Model to support local innovation: Improving Care Improving Lives” had proposed a number of key priority areas, namely:
- To embed into local health and social care communities an effective, systematic approach to the care and management of patients with a long term condition.
- To reduce the reliance on secondary care services and increase the provision of care in a primary, community or home environment.
- Patients with long term conditions need high-quality care personalised to meet their individual requirements.
This follows on from an elegant analysis from one of Derek Wanless’ numerous reports, this time “Securing our Future Health: Taking a Long-Term View” from 2002. This one envisages one scenario for the future involving full public engagement.
Wanless (2002) describes this as,
“levels of public engagement in relation to their health are high. Life expectancy increases go beyond current forecasts, health status improves dramatically and people are confident in the health system and demand high quality care. The health service is responsive with high rates of technology uptake, particularly in relation to disease prevention. Use of resources is more efficient.”
(Derek Wanless, Public Enquiry Unit (2002))
It has become increasingly acknowledged that under this approach, the “care plan” is pivotal. The care plan “should set out the patient’s agreed health objectives and care needs, including what the individual can contribute towards their own self care, and what each professional and agency will do to help them meet these. It will include preventive and health promotion actions (such as avoiding accidents, reducing infection or nutrition).” (Department of Health, 2005).
In a pamphlet from the King’s Fund (2013), entitled “Delivering better services for people with long-term conditions”, the authors, Angela Coulter, Sue Roberts and Anna Dixon describe a co-ordinated service delivery model – the ‘house of care’ – that incorporates learning from a number of sites in England that have been working to achieve these goals.
They describe that the “house of care” model differs from others in two important ways:
- it encompasses all people with long-term conditions, not just those with a single disease or in high-risk groups;
- and it assumes an active role for patients, with collaborative personalised care planning at its heart.
This model is a system innovation, as applied to dementia, as it proposes a shift in power from professionals to persons living with dementia play an active part in determining their own care and support needs. Such an approach, it is hoped, would respect autonomy dignity, promote independence and offer maximum choice and control for need help from the health and care systems. The philosophy of “whole person care” moves the NHS towards an integrated health and care system, which is concerned about individuals during health as well as disease, a critical time when the coordination between the NHS and social care could not possibly be worse.
Self care is about individuals, families and communities taking responsibility for their own health and wellbeing. It includes actions people take in order to stay fit and maintain good physical and mental health, meet their social and psychological needs, prevent illness or accidents and care more effectively for minor ailments and long term conditions.
Both dementia and diabetes mellitus can be viewed as disabilities, and each may be a co-morbidity of the other. Sinclair and colleagues (2014) have outlined the key steps in an integrated care pathway for both elements of this clinical relationship, produced guidance on identifying each condition, dealt with the potentially risky issue of hypoglycaemia, and have outlined important competencies required of healthcare workers in both medical/diabetes and mental health settings to enhance clinical care. In the overall construct, people living with a long term condition, disability or a minor illness, as well as carers, can benefit enormously from being supported to self care.
The ‘Common Core Principles to Support Self Care’ aim to help health and social care services give people control over, and responsibility for, their own health and well-being, working in partnership with health and social care professionals (Skills for Care/Skills for Health, 2007) Seven principles have been elaborated. These are shown in Box 2 below.
—————
Box 2. Seven principles to support ‘self care’ [Source: Skills for Care/Skills for Health (2007)“Common core principles to support self care: a guide to support implementation” http://www.skillsforcare.org.uk/document-library/skills/self-care/commoncoreprinciples.pdf]
- Ensure individuals are able to make informed choices to manage their self care needs
- Communicate effectively to enable individuals to assess their needs, and develop and gain confidence to self care
- Support and enable individuals to access appropriate information to manage their self care needs
- Support and enable individuals to develop skills in self care
- Support and enable individuals to use technology to support self care
- Advise individuals how to access support networks and participate in the planning, development and evaluation of services
- Support and enable risk management and risk taking to maximise independence and choice.
—————
The “NICE quality standard for supporting people to live well with dementia: information for the public” is intended to support people to live well with dementia. It sets out how high-quality social care services should be organised and what high-quality social care should include, so that the best support can be offered to people with dementia using social care services in England (NICE, 2013). This has provided a very useful yardstick against which services which purport to improve the quality of life of people with dementia can be judged.
It is, further, reported that the ‘Year of Care’ (YOC) programme was successful in implementing the key features of care planning in diabetes, for example. The YOC Programme has two components, according to ‘Diabetes UK’ (2011). Firstly, it enhances the routine biomedical surveillance and ‘QOF review’ with a collaborative consultation, based on shared decision making and self management support, via care planning; and then it ensures there is a choice of local services people need to support the actions they want to take to improve their health, wellbeing and health outcomes.
People are involved in the care of their diabetes in quite a new way and enjoying it. People are setting personal goals and action plans relevant to their everyday life; take up of education programmes has improved and in very disadvantaged populations, poor attendance rates, biomedical outcomes and service use are also improving.
(Royal College of General Practitioners, 2011)
It is likely that the health and care sectors will seek to engineer the ‘best’ solutions on offer for post diagnostic support, within a framework of ‘whole person care’.
Such solutions might include ‘dementia advisers’, ‘clinical nursing specialists’, or ‘a year of care’. The solutions most appropriate for “living better with dementia” might be drawn, for example, from best practice in other long term conditions, such as diabetes or cancer. The quality of local commissioning, undoubtedly, is going to be pivotal in this. It will be a sensitive policy balance to make the argument that responsibilities of the State are not shunted across to the third sector in an unaccountable or unorthodox manner. But many will argue that there is valid and crucial role for the third sector to play. Actually, the policy imperative for this could not be clearer – many persons living well with dementia report not expecting to see a professional until the end of life phase, having seen one for the initial diagnosis. This is clearly not on if policy truly wishes to promote living better with dementia in England.
References
Department of Health (2005) “Supporting People and integration with Long Term Conditions – An NHS and Social Care Model to support local innovation: Improving Care Improving Lives”, accessed 6 December 2014,available at: http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/Browsable/DH_4965951
Diabetes (UK) “Year of Care: Report of findings from the pilot programme” (date June 2011), accessed 6 December 2014,available at: http://www.diabetes.org.uk/upload/Professionals/Year%20of%20Care/YOC_Report.pdf
Innovate UK (2014) The long term care revolution: a provocation paper. (author Shirley Ayres), accessed 6 December 2014,available at: https://connect.innovateuk.org/documents/15494238/0/LTCRprovocationPaper.pdf/45cf1947-c477-4f21-913e-4eb3f9061aa0
King’s Fund (2013) (authors: Angela Coulter, Sue Roberts and Anna Dixon, October 13) “Delivering better services for people with long-term conditions”, accessed 6 December 2014,available at: http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/delivering-better-services-for-people-with-long-term-conditions.pdf
NICE quality standard 30 April 2013 NICE quality standard for supporting people to live well with dementia: information for the public, accessed 6 December 2014,available at: https://www.nice.org.uk/guidance/qs30
“Policy: A Year of Care”, accessed 6 December 2014,available at: http://www.yearofcare.co.uk/policy-0
Public Enquiry Unit (2002) “Securing our Future Health: Taking a Long-Term View. Final Report” (author Derek Wanless), accessed 6 December 2014, available at: http://si.easp.es/derechosciudadania/wp-content/uploads/2009/10/4.Informe-Wanless.pdf
Royal College of General Practitioners (Clinical Innovation and Research Centre) (2011) (authors: Nigel Mathers, Sue Roberts, Isabel Hodkinson and Brian Karet) Care Planning: Improving the Lives of People with Long Term Conditions, accessed 6 December 2014, available at: http://www.impressresp.com/index.php?option=com_docman&task=doc_view&gid=75&Itemid=70
Sinclair AJ, Hillson R, Bayer AJ; National Expert Working Group. Diabetes and dementia in older people: a Best Clinical Practice Statement by a multidisciplinary National Expert Working Group. Diabet Med. 2014 Sep;31(9):1024-31. doi: 10.1111/dme.12467.
Skills for Care/Skills for Health (2007) “Common core principles to support self care: a guide to support implementation”, accessed 6 December 2014,available at: http://www.skillsforcare.org.uk/document-library/skills/self-care/commoncoreprinciples.pdf

The presentation may be awful, but sharing of information can be very useful for clinical decision making

Whenever I hear of somebody refer to ‘Big Data’ and the NHS, it’s an immediate ‘facepalm’.
When I saw a blogpost shared by a Twitter pal shared yesterday, a blogpost written by Sir Jeremy Heywood, my first instinct was completely to ignore it.
I am, though, mindful of the Civil Service’s prolonged campaign to measure wellbeing; this first came across my RADAR from Lord O’Donnell.
I have a disclaimer to make: I am not a corporate shill.
Having done certain training, I am aware of the hard sell of ‘Big Data’ as the next big thing by the multi-national corporates. “Big data” seem to have been given a somewhat pedestal status, like 3-D printers.
We are often told how intelligent technology rather than being a costly burden to the NHS could bring great benefits and outcomes for the NHS.
Undoubtedly, a lot of democratic deficit damage was done by the Health and Social Care Act (2012). At close to 500 pages, it was very easy to say it was too incomprehensible to be analysed. I always felt the Act, for anyone trained in commercial and corporate law, was in fact relatively straightforward.
The Health and Social Care Act (2012), often called “the Lansley Act”, has three essential prongs of attack: one to introduce a competitive market through legislation for a heavy penalty for non-one-commissioning not going out to tender, a beefed up regulator for the market (Monitor), and some detail about insolvency regimens (but not all).
In this, it was completely consistent with work by Carol Propper; and other noises from ‘independent think tanks’, such as the King’s Fund.
However, the acceleration of this Act through parliament by two parties which are extremely sympathetic to the free movement of multinational capital has done long-lasting damage.
I think there are problems with having data so transparent. When I did my Masters of Law practice-focused dissertation in cloud computing law, I unearthed a huge literature on data security and data confidentiality/sharing.
When I later did my pre-solicitor training, I discovered the regulatory requirements on the balance between confidentiality and disclosure to be complicated.
When I later came to revise ‘Duties of a Doctor’ (2013), the General Medical Council’s code of conduct, I found there to be equally onerous considerations.
I am aware of the problems in my own field of work; about concerns that NHS patients will be scared from going to see their GP for fear of being diagnosed, incorrectly, with ‘incipient dementia’ because of a GP’s practice wanting to meet a financial target.
Or a junior Doctor not wishing to share his alcoholism with his own Doctor, for fear that this information will end up with the clinical regulator, with a super-un-sympathetic sanction. This is a subject close to my heart, as you will well know.
Indeed, if you’ve been following me on Twitter, you’ll know that a year after erasure by the GMC (in 2006 to be endorsed by the High Court in 2007), I spent a year sitting in a pub with no family or job. I later was then admitted to the Royal Free Hospital having had a cardiac arrest and epileptic seizure, then to spend six weeks in a coma.
I am now knowledgeable about what both the legal and medical regulators expect me to do, as I am regulated by them.
The next Government will be wishing to implement ‘whole person care’. While I think some of Jeremy Heywood’s claims are a tad hyperbolic (for example saying unleashing data will lead to wellbeing improvements), and while I don’t feel he currently ‘owns’ the data (the data are confidential property of the people who provide the data), there are clinically-driven merits to information sharing.
From now on, I will avoid the word ‘data’ and use the word ‘information’. But ‘information’ does not necessarily mean ‘knowledge'; and it certainly doesn’t necessarily mean ‘wisdom’.
One scenario is somebody prescribed Viagra for erectile dysfunction in the morning. He then has sex with his partner in early evening, and has Angina. He has longstanding ischaemic heart disease, and then takes his GTN spray. His blood pressure then goes through the floor, and he collapses. He then is blue lighted into his local emergency room.
Do not take this anecdote as ‘medical advice’ or any such like where I could get into regulatory trouble please.
Viagra is a class of drug which can interact with the GTN spray to send blood pressure through the floor. If this information were known to an admitting Doctor in the emergency room, this would be useful.
I can come up with countless examples.
A lady from a care home turns up in hospital at 4am. An admitting Doctor wishes to prescribe a heavy-duty blood pressure lowering drug, but notes she has had a series of falls. This is found out by looking at her electronic medical record. She indeed has a history of osteoporosis; weak bones could mean that she might fracture a bone if she had another fall.
But I could come up with countless examples. And I won’t.
I am not a corporate shill. I understand completely the concerns about the loopholes in current legislation meaning that ‘big data’ could go walkies to drug companies, though this is vehemently denied.
I am also aware of ‘cloud failures’ – the Playstation one for some reason springs to my mind.
That’s another reason to keep an eye on ‘My NHS’.
But we do need, I feel, to take a deep breath and to discuss this calmly.

Dementia Friendly Employers
HRM TV: Ita Buttrose on dementia at work from AHRI on Vimeo.
Writing my book ‘Living better with dementia: champions for enhanced dementia friendly communities’ has been a real eye opener for me.
I think it’s terribly easy to carp from the sidelines about the ‘dementia friendly communities’ policy as implemented in England, but England is in fact helping to lead the way with this policy. ‘Dementia friendly communities’ is a policy which has a strong global backing, with links to the World Health Organisation’s “Age friendly cities”.
The WHO “Age Friendly Cities” recognised that there are basic design features of an urban city, wherever in the world, which might make living in it much easier; such as ‘inclusive design’ which is accessible to people.
Dementia is not just about ageing, so it is a challenge to think about what a dementia friendly ‘community’ might be. It’s important for this to be a ‘community’ not just a city, as it is recognised that around the world there are remote or rural areas where people who’ve been diagnosed need to feel welcomed.
When I went up to the Alzheimer’s Europe conference in Glasgow earlier this year, I had the good luck to meet Ann Pascoe in the hôtel where we weree having her fringe events. She has been doing groundbreaking work on rural dementia friendly communities in Scotland. I subsequently met one of team doing great work on dementia friendly rural communities in Wiltshire at the Dementia Action Alliance meeting the other day.
I met Toby Williamson from the Mental Health Foundation too at Glasgow, as well as Grainne McKettrick who first started her work on equality and equity at the Alzheimer’s Society in Scotland. I am delighted that Grainne has allowed me to quote from her speech in my one of my book chapters for the book I am submitting.
That chapter is on reconciling a rights-based approach promoting dignity and autonomy, with other mechanisms to promote ‘choice’, in a more consumerist way, through ‘personal budgets’ or ‘self directed support’.
Grainne remarked in her email to me yesterday how she had been really impressed with how fast the policy stream for this has taken pace in the last few years.
I think this is indeed worth noting for England. In the last fee years, we have seen a number of aspects suddenly converge at once, which have made a really big impact: these include the recognition of the UK government of the UN Convention on rights for disabled citizens (a few years ago), the Equality Act (2010), “dementia friendly communities” and the Prime Minister’s Dementia Challenge.
A welcome move will be there will be some sort of ‘standard setting’ for dementia friendly communities. It is far too easy for some communities to claim that they are ‘dementia friendly communities’, for their own promotion, rather than meeting an accepted reasonable level of requirements.
I think it’s great that people living with dementia can expect now a better level of service in the high street, say from a high street bank. But it’s important that this policy doesn’t raise inappropriate expectations.
But it is also true that this policy should raise expectations on employers dealing with people of a certain age, say in their early 50s, who might be developing a dementia in the younger age group, such as diffuse levy Body disease, vascular dementia or Alzheimer’s disease.
It’s a legal obligation for employers to make ‘reasonable adjustments’ against anyone with a ‘protected characteristic'; and dementia is one such characteristic, coming under the disability umbrella.
So why are there not many test cases for unfair dismissal for people who are sacked ultimately because of developing dementia? I have given this some considerable thought in the last few months since meeting Toby Williamson, and I reckon the answer is predominantly two fold.
Firstly, I don’t think it’s thought to be certain that the problems faced by an employee is due to a dementia at the time of ‘sacking’ with an element of mutual collusion that neither party is hoping for the likelihood of such a diagnosis. There are also intrinsic problems in England in areas of the country for achieving the diagnosis in a prompt manner. Prof Sube Banerjee warned recently how policy should not promote ‘high quantity, low quality’ of dementia diagnoses, on the other hand.
Secondly, I don’t think people are also aware of their legal rights under discrimination law, and, even so, don’t wish to take their employer to court for fear of losing any retirement packages or loss of goodwill, or inherent problems in access to justice. In England, under the current government, the legal aid budget has been slashed due to the Legal Aid and Sentencing and Punishment of Offenders Act (2012).
And another reason is that whilst we may have been promoting dementia friendly communities encouraging companies to cater for their customers living with dementia we haven’t been so keen to push ‘dementia friendliness’, a responsibility (rather obligation) of the employer.
There is, though, encouraging progress being made in other jurisdictions. I think we could no worse than to take a leaf out of the consumer action group of the Alzheimer’s Australia set up in England in pursuing this policy further.

‘Friendly’ is one thing, but communities need to ensure people with dementia have the law working for them
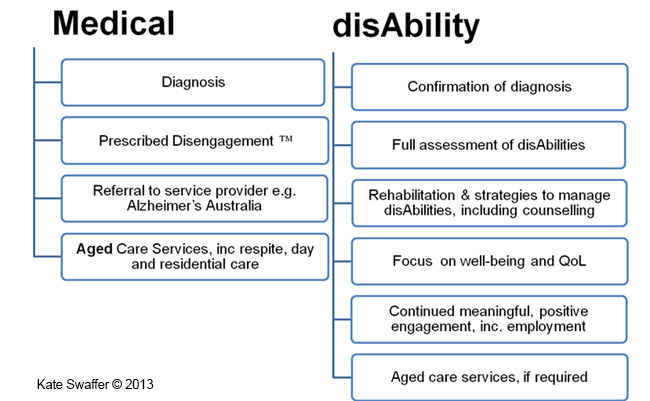
Kate Swaffer (2014) has written about her perception of the receipt of a diagnosis of dementia. The account given by Swaffer is widely held, it turns out.
“The cost of this Prescribed Disengagement™ sets up people with dementia to become victims or sufferers, their partners to eventually start behaving like martyrs and to take over for the person diagnosed. It sets up people with dementia to believe there is no hope, there are no strategies to manage the symptoms of dementia, and more importantly, that it’s not worthwhile trying to find any. It negatively impacts self-esteem, a person’s finances, relationships and the ability to see any sort of positive future. Having dementia does not mean you have to give up living a pre-diagnosis life, nor living beyond your diagnosis. For some, following a diagnosis of dementia, their whole life becomes about dementia and many seem to forget to keep living the other parts of their lives. This is the negative effect of the Prescribed Disengagement™.
Prescribed Disengagement™ also takes away any power or control of the person diagnosed, giving it all to the family carers and service providers. It is unhealthy and wrong. Dementia is the only terminal illness I know of where people are told to go home and give up, rather than to fight for their lives. Prescribing disengagement also lowers a person’s own expectations about how they can live, and it lowers others’ expectation about how we can function and live, including employers, health care professionals and service providers.”
(Swaffer, 2014)
Under international law, the Convention on the Rights of Persons with Disabilities exists to protect citizens with disability.
a) of the Preamble states:
“The States Parties to the present Convention,
- Recalling the principles proclaimed in the Charter of the United Nations which recognize the inherent dignity and worth and the equal and inalienable rights of all members of the human family as the foundation of freedom, justice and peace in the world,”
The Equality Act (2010) in England and Wales makes discrimination against persons living with disabilities unlawful. Dementia is a disability.
On 6 December 2014, the BBC news website ran article with the title “Disabled people’s access to High Street ‘shocking’, audit finds”.
According to the report, accessibility experts DisabledGo visited all of the 30,000 venues in person to assess them, in the largest ever audit of its kind in the UK. They found a fifth of shops had no wheelchair access, only 15% of restaurants and shops had hearing loops and three quarters of restaurants did not cater for those with visual impairments.
If we are shocked about this lack of access for people who are physically disabled, we should be equally shocked for lack of accessibility for people with cognitive or behavioural problems from living with dementia.
Swaffer in her analysis goes onto compare the medical and the social responses to the event that is the disclosure of the dementia diagnosis.
“Misguided and preconceived misconceptions about the symptoms of dementia are used to support telling us to give up living our pre-diagnosis lives. Instead, the recognition of the symptoms as disabilities would assist with a more equitable and dementia-friendly experience for the person with dementia after diagnosis. In contrast to the medical model, the disAbility model of care is positive and supports continued engagement with our prediagnosis lives. “
This picture is from: here.
For the sake of parity of esteem, in other words not treating mental health as inferior to physical health, we need to apply the same rigour for ‘reasonable adjustments’ for cognitive or behavioural interventions as for physical ones.
Equality law recognises that bringing about equality for disabled people may mean changing the way in which employment is structured, the removal of physical barriers and/or providing extra support for a disabled worker (see, for example, the Equality and Human Rights Commission website, 2014).
Coincidentally, yesterday, the British Psychological Society (2014) launched its new publication on care pathways for early stage dementia and psychological interventions in early dementia.
Here’s Agnes by their stall in Glasgow (Scotland).

In other words, buildings should have adequate signage for people living with dementia of the Alzheimer Type. It is beyond reasonable doubt that early dementia of the Alzheimer type is characterised by problems in learning and memory, including in spatial navigation (Serino and Riva, 2013).
It is also beyond reasonable doubt that people with such cognitive disabilities will benefit from specialist design as a reasonable adjustment (Habell, 2013).
The recognition process for dementia friendly communities is currently being developed by the Alzheimer’s Society (2013). I feel itwill be a valuable opportunity for people to demonstrate that they are not only obeying the letter of the law, but they are also entering into the spirit of it.
References
Alzheimer’s Society (2014) Recognition process for dementia friendly communities. http://www.alzheimers.org.uk/site/scripts/documents_info.php?documentID=2136
BBC News website (6 December 2014). “Disabled people’s access to High Street ‘shocking’, audit finds” http://www.bbc.co.uk/news/uk-politics-30342957
British Psychological Society. 3 Days To Go to Launch of ‘Clinical Psychology in Early Stage Dementia Care Pathway’ and ‘A Guide to Psychosocial Interventions in Dementia’ (1 December 2014) http://www.psige.org/news/33/3+Days+To+Go+to+Launch+of+%27Clinical+Psychology+in+Early+Stage+Dementia+Care+Pathway%27+and+%27A+Guide+to+Psychosocial+Interventions+in+Dementia%27
Equality and human rights commission. (2014) Workplace adjustments. http://www.equalityhumanrights.com/private-and-public-sector-guidance/employing-people/work-place-adjustments
Habell M. Specialised design for dementia. Perspect Public Health. 2013 May;133(3):151-7. doi: 10.1177/1757913912444803. Epub 2012 Jun 22.
Serino S, Riva G. Getting lost in Alzheimer’s disease: a break in the mental frame syncing. Med Hypotheses. 2013 Apr;80(4):416-21. doi: 10.1016/j.mehy.2012.12.031. Epub 2013 Jan 29.
Swaffer, K. (2014) Reinvesting in life is the best prescription (1 December 2014) Australian Journal of Dementia Care, http://journalofdementiacare.com/reinvesting-in-life-is-the-best-prescription/
UN Convention on the Rights of Persons with Disabilities, http://www.un.org/disabilities/convention/conventionfull.shtml

Clinical nursing specialists for dementia put the precise rôle of the third sector to the test
Ed Miliband, most people agree, is set to be the leader of the largest party at Westminster next year at least. This would give him overall charge of the legislature and the executive on 8 May 2015.
He has also pledged to produce 20,000 extra nurses, though talk is cheap. George Osborne has failed on virtually all ambitions that were set for the economic performance of the current Government. The Conservative-Liberal Democrat coalition therefore bequeath the next Government with a society with a terrible frail economy.
This UK economy is essentially a bargain basement one. It is easy to spot the major fault with ‘the record number of jobs’ meme, as the actual till receipt income is very low. And yet the Conservative want to pay for tax cuts – we’ve gone from an over bloated state to an under nourished one.
I had the enormous pleasure, with two other Dementia Friends Champions Chris Roberts and Jayne Goodrick, of giving a Dementia Friends information session at my law school yesterday. I can’t praise enough the amount of support we were given from the people who run Dementia Friends.

Forgive my photography. I am no David Bailey*. We actually had a good turnout, but I managed to capture the part of the audience which was very lean. Chris Roberts (@mason4233) lives well with a mixed type of dementia, thought to be a mixed Alzheimer’s disease and vascular dementia.
Somebody came up to me at the end of the audience and said, “It was absolutely brilliant as it was just incredible to see for my own eyes somebody living well with dementia.”
The “Dementia Friends” initiative has been a successful one. From the Alzheimer’s Society, and supported at a distance by Public Health England, it is modelled on the Japanese ‘caravan befriending’ movement. Its aim in policy terms was to break down the stigma, prejudice and discrimination which can happen against people living with dementia. These factors can contribute to the social isolation often experienced by people on receipt of a probable diagnosis.
“Dementia Friends” has been brilliant for myth busting, with actual facts about dementia too.
Recently, Kate Swaffer (@KateSwaffer), leading international advocate living well with dementia, and working with Alzheimer’s Australia, leading for the Dementia Alliance International, met Dennis Gillings this week in a small group of people for dinner. Gillings is the newly appointed World Dementia Envoy.
For reasons which are completely inexplicable, there is no established substantial representation on that panel from the communities of people living with dementia or caregivers, although Hillary Doxford was documented in the Communiqué of the last meeting just gone.
When Dennis met Kate recently, Kate quipped, typically characteristically in a beautiful tongue-in-cheek manner, she had not ben dribbling into her soup (Kate’s blogpost here).
But “Dementia Friends” is an interesting example of a private-public initiative with a £2.4 million funding base. Had this been left entirely to ‘market forces’, it is unlikely there would have been national outreach for this unique project. Inevitably the topic in policy terms is whether the substantial cost of Dementia Friends is offset by the value of raising the profile of dementia and caregivers. Where it might fail on its outcomes, and time will tell, is how the pledges of turning communication into action are actually hard evidenced through the number of pledges (irrespective of whether it will hit its target of one million within an extended deadline of the end of 2015).
In my opinion, it has been.
Two days previously, I enjoyed being at the Methodist Central Hall for a day for the Dementia Action Alliance.

And yet it is also true that social care is on its knees.
You don’t have be a great story teller to communicate a tale of the NHS on its knees.
This is somewhat cognitively dissonant with MPs wearing their Dementia Friends badges with pride, one could argue.

I agree with Jeremy (tweet here) in that the third sector should not need to apologise for fundraising. Making a surplus for a charity is a raison d’être for a charity akin to the duty to maximise shareholder dividend for a business.
But larger charities share many operational and cultural characteristics with corporates conceivably, and therefore the principles of a good ‘corporate citizen’ could easily apply to large charities with substantial revenues.
Sube Banerjee, long time supporter of the Alzheimer’s Society, and, perhaps more significantly here, co-author of the previous 2009 English dementia strategy came to the Dementia Action Alliance table with some noteworthy criticisms of how the current strategy had been executed.
Firstly, Sube, now a Chair of dementia at the Brighton and Sussex Medical School, commented on the devaluing of the ‘cost’ of a diagnosis to £45, and commented specifically on the culture of a ‘high quantity low quality’ approach to diagnosis.
Indeed, the 2009 English dementia strategy, called ‘Living well with dementia’, refers to the need for high quality diagnosis.
And the English dementia policy as it was then, before it got taken over by the Prime Minister’s Dementia Challenge, due to expire next March 2015, also warned about the lack of post-diagnostic support.
People living with dementia, and their family members, have consistently remarked to me how they have been told by medical professions that their rôle is at the very start and very end of “the dementia journey”. They won’t be there for them in between.
We are all aware of recent findings that 9 out of 10 care homes failing to meet standards set by the regulator the Care Quality Commission, reported not just in the Daily Mail.
So there is an overwhelming sense that people with a possible diagnosis of dementia are being set up for a fall by an inadequate care system, which is disjointed, increasingly privatised, and undervalued.
One of the undesirable consequences of this bargain basement economy is the sheer undervaluing of paid carers on zero hour contracts, some not even getting any travel expenses or the national minimum wage.
This poses serious questions about us as a society. So does the lack of support we appear to be giving unpaid family caregivers, an army of which nearing a million are the backbone of the entire system.
But Jeremy’s tweet does also pose serious questions about what charities could or should fundraise for. I say this as I remember one of own interview questions to read medicine at Cambridge – which I did between 1993 and 2001 – “to what extent should charities take the place of a properly funded NHS?”
Well, this question has taken on a new twist. I do not see there to be a ‘competition’ as such between ‘dementia advisers’ of one charity and ‘specialist nurses’ from another third sector charity. I think they co-exist. ‘Dementia advisers’ are possibly more useful for the more independent parts of the support of “the dementia journey”. ‘Specialist nurses’ are pivotal at all parts, including the care part of ‘the dementia journey’.
It has struck me how not only cost effective clinical specialist nurses are, in providing proactive case management for people with dementia with personalised care plans, ‘nipping in the bud’ complications from medical conditions. I know internationally one of the campaigning for fundraising themes is the substantial co-morbidity of dementia. People living with dementia often have a plethora of other problems, such as in joints, heart or lung.
Sally Greengross has long made it been known that the post diagnostic support for dementia is not good enough. Sally Greengross is the current Chair of the All Party Parliamentary Group on dementia. Her predecessor, Jeremy Wright MP, currently the Government’s Attorney General, launched the highly successful policy here in England of an ambition to reduce the number of inappropriate prescriptions for antipsychotics predominantly in care homes.
Hospitals can be some of the worst places a person with dementia to end up in. Likewise, it shouldn’t be conceived that secondary hospital care is necessarily synonymous with someone who has ‘failed’ somehow. But, say, end of life nurses will be able to provide expert help, wherever the appropriate care setting is deemed to be for a person living with dementia (and his/her friends or family).
And it is therefore possible charities such as Dementia UK and others might be able to fill these gaps in service provision. For a start, clinical nursing specialists comprise an innovative way of delivering the dementia post-support service. And the NHS has a statutory duty to promote innovation.
 However, I should say that that statutory clause (14X) on CCGs is from the much loathed Health and Social Care Act (2012), about to be repealed by the next Labour government.
However, I should say that that statutory clause (14X) on CCGs is from the much loathed Health and Social Care Act (2012), about to be repealed by the next Labour government.
It is sometimes the case innovation can be incubated in places other than the NHS, and we’ve already seen a lot of goodwill and real-life financial support for Macmillan nurses. It would be impossible now to think of palliative care for nursing in cancer to be without Macmillan nurses – and the prime contractor model could be a way of providing sustainability in critical areas of services. This is ONLY provided that the quality and cost effectiveness components are managed correctly and for the benefit of the taxpayer. The next Labour government wishes to bring out a huge systemic innovation of integrating health and care into whole person care. This is long overdue, as, for example, it is impossible in places to discharge NHS patients to social care in s timely fashion. This is not cost effective; it is insulting particularly to patients including frail old citizens who do not wish to be in hospital anyway, and do not deserve the pejorative insulting label of “bed blocker”.
I am sure Alistair (@ABurns1907), or whoever ends up predominantly penning the new English dementia strategy, will wish to give careful consideration to how this post diagnostic support can be provided. Jeremy has a point, but up to a point.
*Joke by @JayneGoodrick.
The final conclusion to my book on living better with dementia
Anything can happen to anyone at any time. Despite all the best initiatives in the world, it will be unachievable to extinguish all negative perceptions about dementia. Nobody can deny the imperative for communities and society to be inclusive and accessible for people with dementia, but is no mean feat to rationalise with more individualistic approaches ranging from personal budgets, human rights and equality law responsibilities. It really is not a question of what a person can no longer do. It is an issue of what a person can currently do, and this might include, for example, unleashing of previously unwitnessed artistic and creative talents.
All jurisdictions converge on the right for a timely diagnosis and a right to timely post-diagnostic support, but political grandstanding over cures will be small change to those people currently wanting to live better with dementia. People who have received a diagnosis of dementia are not all consumers, and some do not even interact with health and care services as patients. They are all persons, however, and wish for inalienable dignity and respect. Everyone knows that the diagnosis affects not just the person with dementia,but their whole network of friends and family. There now must be a political will to do something about this, and this is not just a societal issue for the G7. Silos must be abolished; for example, in considering eating better with dementia, the emphasis can no longer be on the design of ‘finger snacks’, but responsible thought has to be put into how certain mealtime environments work (or do not work). It is utterly pointless talking about joining initiatives to encourage ‘dementia friendliness’, while words such as ‘victim’ continue to litter the mainstream press. And “leading” scientists and practitioners can unwittingly perpetuate stigma through somewhat perjorative language such as ‘wanderer’; the willful blindness to this must stop too. Living better with dementia is not just an aspiration; it is in many places legally enforceable.
Bring it on.

When cultural change catalysts turn into inhibitors

To argue that ‘cultural change catalysts’ can turn into inhibitors is, as quite usual for the management literature, is re-inventing the wheel.
The idea is that ‘catalysts’ in cultural change act like catalysts in chemical reactions. Exploring this analogy further, catalysts in chemical reactions do not produce more of the intended products, speed up the generation of the product, and are unaffected by the process.
I do not feel that this analogy is appropriate, on account of the three arms of the quality of what a ‘catalyst’ is.
I am unconvinced that there has been more of the “intended products”. How you measure these ‘key performance indicators’ is more of the domain of people with a management training rather than experienced practitioners or clinicians.
The number of re-tweets on Twitter is a metric of sorts, but so is the traffic to a page 3 supermodel on the internet.
In my own field, has the number of retweets of tweets containing the term ‘living well with dementia’ led to a ‘transformational change’ in what people understand to be wellbeing?
I doubt it.
Do ‘cultural change catalysts’ speed up the generation of the product?
I am not convinced about this either. In fact, I would like to propose that the #hashtag activism can put a lot of people off from participating.
The people who are put off, ironically, are exactly the sort of people this campaign was trying to embrace – people at the “edges”.
People at the “edges” will not be able to become the Chief Inspector of Social Care at the Care Quality Commission through wacky ideas on Twitter.
Conversely, they might be singled out for worth ‘keeping an eye on’ in a negative sense.
When I know of well meaning people who have been diagnosed with severe mental illness for the first time having worked in the National Health Service, this is not trivial.
Nor is the fate of whistleblowers, and the inadequacy of the Public Interest Disclosure Act (1998).
And whether “radicals” are in fact “radicals” demands proper scrutiny.
I have often marvelled at the term “shared values” of corporate glossy prospectuses. Such shared values in my experience have been used to stamp out diversity, freedom of expression, and to encourage a rigid sense of conformity.
We’ve seen a similar mathematical approach to an analysis of when ‘hipsters’ become ‘conformists’.
When people doing their job in the health and care systems take to Twitter to talk of their resentment of non-clinicians and non-practitioners talking of ‘radicalism’, you have to begin to worry.
This ‘radicalism’ is the ultimate sin for what innovation management values, in my experience.
Innovation management is, if anything, all about ‘environment sensing’ and making connections between different disciplines. If a part of your environment ‘resents’ your work, it’s time you should NOT adopt an approach of ‘there is no alternative’ and continue with #boatrockers regardless.
And my final concern?
That catalysts are unaffected through the process.
I am not entirely convinced about this, as there is scope for a two-tier system of ‘registered catalysts’ and those who are not.
Of course, business management has taken two prongs of attack latterly – promoting competitive advanced and increasing shared social value.
The increased shared value, I argue, can be so intense so as to be quite off putting.
And when the same beneficiaries are at the same events with the same awards and the same projects, with the same commissioning targets, compared to others who have not participated in ‘catalysing the transformative change’, you do really have to query whether they are genuinely unaffected by the process.

A lot more unites us in English dementia policy than divides us, potentially
It’s sometimes hard to see the big picture in the policy of England regarding dementia.
I don’t mean this in terms of the three key policy strands of the strategy, which is currently the Prime Minister’s Dementia Challenge. This extra layer was added onto the English dementia strategy, “Living well with dementia”, from 2009-2014.
There will be a renewal of this strategy next year. We currently don’t know what Government will be in office and power in 2015. But I am hoping the overall direction of travel will be a positive one. I would say that, wouldn’t I?
There are 3 dementia challenge champion groups, each focusing on 1 of the main areas for action: driving improvements in health and care, creating dementia friendly communities and improving dementia research.
But it is in my political philosophy to encourage a pro-social approach, not a fragmented one.
I’d like to see people working together. This can all too easily be forgotten in competitive tendering for contracts.
And things can be just as competitive in the third sector as for corporates.
This is the clinical lead for dementia in England, Prof Alistair Burns, who has oversight over all these complicated issues.

But we need to have a strong focus for the public good, especially as regards looking after the interests of people living with dementia, and their closest including all caregivers. State-third sector initiatives can work brilliantly for particular outcomes, such as encouraging greater sharing of basic information about dementia, but all concerned will hopefully feel that the people whose interests we want to protect the most benefit from a plural space with many stakeholders.
There is definitely a huge amount which has been achieved in the last few years. I do definitely agree with Sally Greengross, Chair of the All Party Parliamentary Group for dementia, that we should really take stock of what has worked and what hasn’t worked so well in the last five years, in our wish to move forward.
I say this, as it has come to my attention while reviewing the current state-of-play in policy and in research that there are potentially problematic faultlines.
1. One is diagnosis.
On the one hand, some people feel that we are under diagnosing dementia, and that there are people languishing in England waiting for a diagnosis for weeks or months.
Chris Roberts, himself living with a dementia, and a greater advocate for people living with dementia, often warns that it is essential that, despite the wait, that the diagnosis is correct.
I know of someone else in the USA who has battled on for years while waiting for a diagnosis of dementia, despite having symptoms of dementia.
On the other hand, there are concerns, particularly if teams in primary care are financially incentivised for doing so, that there might be a plethora of over diagnosed cases.
The concern here is that there might be alternative interests for why such people might be diagnosed, such as being recipients of compounds from drug companies which attach to proteins in the brain, and which might be useful in diagnosing dementia.
Or we are building a ‘new model army’ of people who are ageing, but being shoehorned into the illness model because of their memory problems?
2. Another is potential ‘competition’ between dementia charities.
Essentially, all dementia charities in England want the same thing, and will need to attract an audience through various ‘unique selling points’ through that awful marketing terminology.
But in the next few years we may see commissioning arrangements change where the NHS may involve the third sector doing different complementary rôles, such as advising and providing specialist nursing, in the same contractual arrangement.
The law might force people to work together here.
3. Another is the ‘cure versus care’ schism.
This debate has accelerated in the last few years, with the perception – rightly or wrongly – that cure – in other words the drive to find a magic bullet for dementia – is vying for attention with care. This narrative has a complicated history in fact, in parallel with moves in the US which likewise have overall seen a trend towards some people wishing for a ‘smaller state’.
But claims about finding a cure for dementias have to be realistic, and, while comparisons can be made with HIV and cancer about the impact of a cure has for absolving stigma potentially, such a debate has been done incredibly carefully.
For example, attention for cures and collaboration between Pharma and ‘better regulation’ constitute a diversion of resources away from care, potentially. In the NHS strategy for England, with social care on its knees, a drive towards personalised medicine on the back of advances from the Human Genome Project can end up looking vulgar.
I’ve also seen with my own eyes how the ‘cure vs care’ schism has seen different emphases amongst different domestic and international dementia conferences, with some patently putting people with dementia in the driving seat, and some less so (arguably).
4. Another is the exact emphasis of ‘dementia friendly communities’.
It is impossible to object to the concept of inclusivity and accessibility of communities, with recognition of the needs of people living with the various dementias.
But the term itself is possibly not quite right; as Kate Swaffer says, a leading international advocate on dementia, you would never dream of ‘black friendly communities’ or ‘gay friendly communities’ as a term.
Another issue is what the precise emphasis of dementia friendly communities is: whether it is an ideological ‘nudge’ for companies and corporates to enable competitive advantage, or whether it is driven by a more universal need to enshrine human rights and equality law.
As Toby Williamson from the Mental Health Foundation mooted, the need for an employer to make reasonable adjustments for cognitive disAbility is conceptually and legally is actually the same as the need for an employer to build an access ramp for a person who is in a wheelchair and physically disabled?
There can also be a problem in who wishes to be “the dominant stakeholder”. Is it the person with dementia? Or unpaid caregiver? Or paid carer? Or professional such as CPN, physio, OT, speech and language therapist, neurologist, physician or psychiatrist? Is it a dementia adviser or specialist nurse?
If we are to learn the lessons from the Carers’ Trust/RCN “Triangle of Care”, it is essential to learn from all stakeholders in the articulation of a personalised care and support plan? I feel this is important in whole person care if we are to have such plans in place, which recognise professional pro-active clinical help, in trying to assist in avoidable admissions to hospital.
But here we have to be extremely careful. An admission to hospital or appearance at A&E should not always be sign of ‘failure’ of care in the community.
5. Yet another source of division is that we all do our own things.
This is problematic, if we do our own things. We end up being secretive about which people we’re talking to. Or which conferences we’re going to.
Or if countries don’t talk to each other, even if they have similar aims in diagnosis, and post-diagnostic care and support (including the global dementia friendly communities policy). Or if we don’t share lessons learnt (such as, possibly, the beneficial impact of treating high blood pressure on dementia prevalence in one country).
Or if certain people become figureheads in dementia. But no man is an island.
I still feel that there’s a lot more that unites us than divides us.
Anyway, I’ll leave it to people on the frontline, and in communities, much more able than me, to work out what they want.

Money is tight, but the person remains pivotal in dementia care and support
There’s no question that there is a greater number of people who are old needing to be looked after by care and support services in England.
But dementia is not simply a disease of older people, one of the critical messages of “Dementia Friends”.
Indeed, much of the budget goes into the health and care of younger people, as health technologies, say for treating cardiovascular disease through stents, get better.
The reality is there is pressure on service and the workforce simultaneously in dementia, as the Nuffield Trust and Health Foundation have argued in a sophisticated way.
Earlier in this year, in an article for ETHOS Journal “Living well = greater wellbeing”, I argued a joined up approach would now be needed to deliver a better standard of care and support for people living well with dementia.
In 2010, the UK government became among the first countries to officially monitor people’s psychological and environmental wellbeing. Academic research and policy developments have recently converged upon the notion of ‘living well with dementia’, which transcends any political ideology. This means promoting the quality of life of any person with dementia. It views each person as a unique individual and champions his or her involvement in making decisions whenever possible.
England actually leads the way with the ground-breaking ‘first mover’ exploration by academic Tom Kitwood of ‘personhood’ in the late 1980s: “It is a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being. It implies recognition, respect and trust”.
It’s estimated that there are at least 800,000 people currently living with dementia in the UK. These individuals are likely to come into contact with a number of different people and services in an extensive network including carers (paid and unpaid, including family caregivers), care home staff, transport services, social housing, welfare and benefits and the police to name but a few.
I am, indeed, grateful for Paul Burstow MP’s excellent reply to my article.
The current Government in England has made substantial progress with policy in dementia in my opinion.
The current Care Act (2014) could not be clearer.
In the statutory guidance, the importance of wellbeing is signalled extremely strongly.
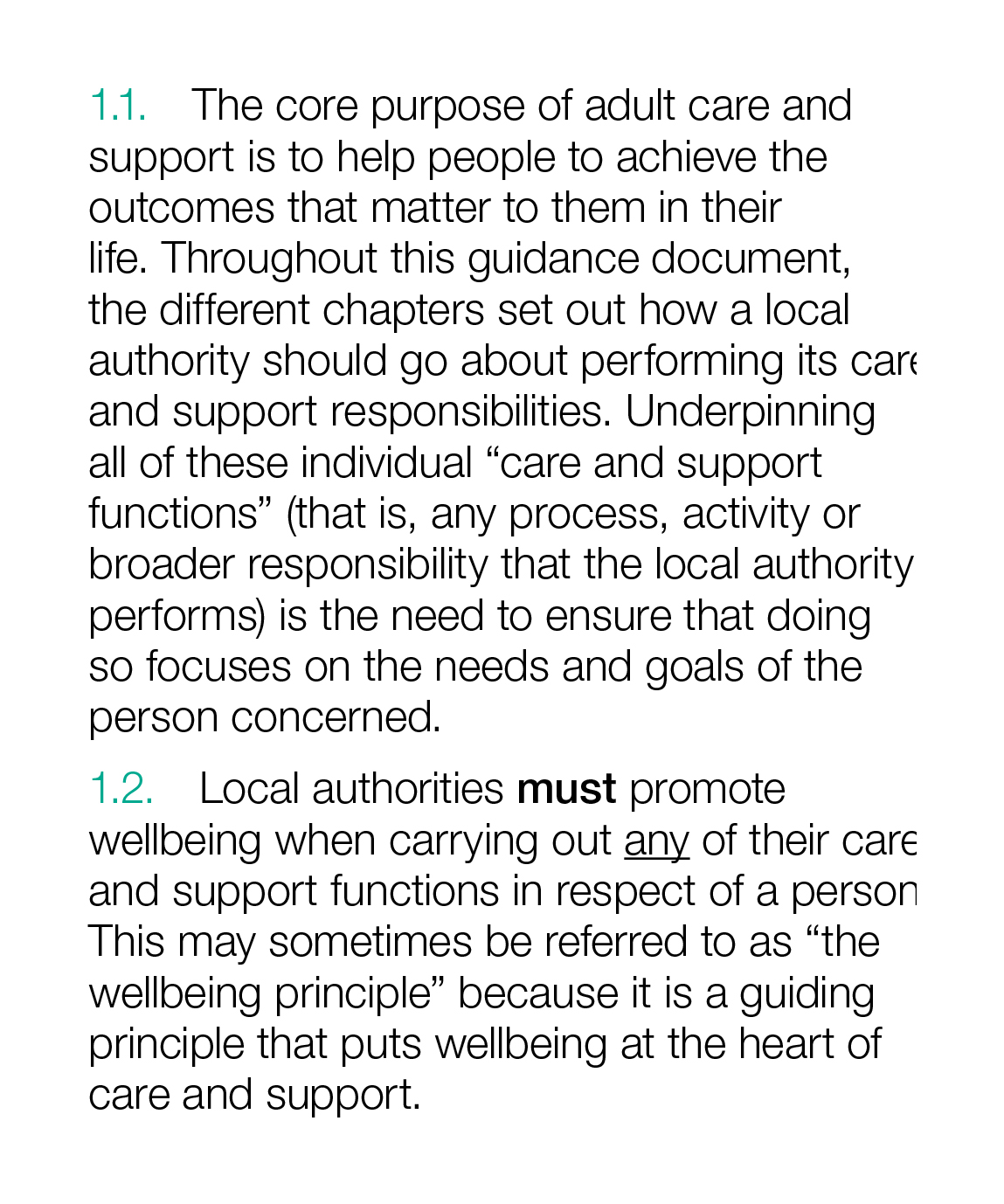
It is important for commissioners not to lose sight of this, and not to treat ‘living well with dementia’ not as a slogan but as a reality.
Helping people to live well has been a key aim of the current Government, and I hope future governments, perhaps implementing ‘whole person care’, will retain this strong focus.
Enabling people to live well leads to a fairer society. The value of people living with dementia for society cannot be denied either.
But people in power and influence have a rôle to play.
The Alzheimer’s Society has played its part in addressing stigma and discrimination through its successful ‘Dementia Friends’ campaign. I myself am a “Dementia Friends Champion”, and proud to run my sessions.
One of the key messages in this campaign is that ‘there is more to the person to the dementia’.
This message is currently a critical global one, across many jurisdictions. Here is friend and colleague Kate Swaffer with a huge banner in Australia to the same effect.

And dementia and loneliness already occur together all too often.
The wider community is essential. This is about compassion. It is also about the right people showing the right leadership.
But this should not just simply include household names, although the distress caused by lack of inclusion of people with dementia in high street shops cannot be underestimated.
This community must include all caregivers and professionals.
And central to this recognition of the role of the wider community is a new deal for carers.
As the number of people living with chronic conditions grows rapidly, so does the number of carers. There is a huge army in England currently consisting of selfless individuals giving of themselves to support a loved one.
According to Carers UK, family carers currently save the Government £119 billion every year.
Carers themselves need help.
Carers are invaluable as I discuss here.
And we need to make sure in the next Government that all paid caregivers are given a statutory minimum wage, which could also be a living wage.
We are a society which values footballers more than caregivers for people with dementia. This is simply abhorrent.
I thank the current Government for progress made in this direction, but more has to be done whoever holds office and power next year.
We need collectively to support the Dementia Action Alliance Carers Call to Action. By achieving the shared vision, the aim is to have positive impact on people with dementia and carers and improve their quality of life.
In the Dementia Action Alliance “Carers Call to Action”, carers of people with dementia:
- have recognition of their unique experience – ‘given the character of the illness, people with dementia deserve and need special consideration… that meet their and their caregivers needs’ (World
Alzheimer Report 2013 Journey of Caring are recognised as essential partners in care – valuing their knowledge and the support they provide to enable the person with dementia to live well - have access to expertise in dementia care for personalised information, advice, support and co-ordination of care for the person with dementia
- have assessments and support to identify the on-going and changing needs to maintain their own health and well-being
- have confidence that they are able to access good quality care, support and respite services that are flexible, culturally appropriate, timely and provided by skilled staff for both the carer and the person for whom they care
But we do need some sort of standards, whether aspirational or regulatory, for example?
This situation had become known to Norman Lamb by February 2013:
In light of the recent Stafford Hospital Scandal, an independent review was carried out, underlining irregularities in staff training. According to today’s BBC report, as of March 2015, UK care staff and assistants in care homes, hospitals, and private homes are to be required to complete a training certificate within 12 weeks of starting a new position.
The current UK stance is that there is no minimum standard of training. With over 1million care workers in the country, it came as alarming news to Care Minister, Norman Lamb, to discover that these untrained workers were completing skilled tasks normally undertaken by medical professionals such as taking bloods. He confirmed the responsibility for the certificate would “…rest with employers and I think that’s where the training responsibility should lie.”
I expect the next Government will wish to think about a register for paid carers to help the fight against neglectful care which can tragically happen. It can be hard to achieve a successful prosecution of ‘wilful neglect’, but likewise carers need to be able to do their job with dignity and without fear.
The broad consensus has been for some time “that the principles of person-centred care underpin good practice in the field of dementia care”. Their principles assert:
- the human value of people with dementia, regardless of age or cognitive impairment, and those who care for them
- the individuality of people with dementia, with their unique personality and life experiences among the influences on their response to the dementia
- the importance of the perspective of the person with dementia
- the importance of relationships and interactions with others to the person with dementia, and their potential for promoting well-being.
In a presentation called “Developing nursing in dementia care” in May 2014 influential expert Rachel Thompson outlined a “Commitment to the care of people with dementia in hospital settings”, calling for increase in specialist nurse roles –building evidence and supporting leaders.
I believe strongly this need has not gone away. Indeed, it is stronger than ever.
Thompson there mentions the SPACE principles to support good dementia care
Staff who are skilled and have time to care.
Partnership working with carers.
Assessment and early identification of dementia.
Care plans which are person centred and individualised.
Environments that are dementia-friendly.
The financial case for ‘Admiral nurses’, an innovation from Dementia UK, is compelling; see for example the recent report from the University of Southampton Centre for Innovation and Leadership in the Health Sciences.
As is the case from the academic and clinical nursing literature on the importance of proactive case management in avoiding admissions to hospital care.
Claims that nine in ten care homes and hospitals fail to provide the proper treatment are indeed astonishing. That particular Care Quality Commission review found widespread neglect, lack of care, poor training and failings in communication.

In the same way there can be enormous disparity between a ‘bad’ and ‘good’ care home, there can be a subtle difference between a ‘very good’ and a ‘superb’ care home.
We, one day, need to be able to celebrate the ‘outstanding’ in care homes: for example, person-centred activities or environment generally might make all the difference?
The next Government, whoever it is, will need to have the confidence to implement an organic, stakeholder-driven systemic innovation in dementia.
I have long felt that the health and care services need more than a minimum ‘protected funding’. As Roy Lilley, experienced health commentator, remarks, ‘more effort can be put into weighing the pig than actually fattening it’.
This is the danger we run if we do not place adequate resources into service provision and training.
However, even within these domains, I believe that innovation has, potentially, an important and responsible part to play (as indeed I argued in the Health Services Journal this year).
There is no question that money is tight.
But we need also to have a minimum in frontline services to maintain an adequate standard of care, as indeed is supposed to be enforced from the regulation of all clinical professions.
It is easy to jump on a ‘person-centre care’ bandwagon, but all too easily this can turn into selling courses and products for person-centred care.
Putting the person at the heart of how you behave with a person with dementia does not need to cost money. Tom Kitwood articulated it brilliantly.
But, whatever the budget constraints of the health and care and future, I believe personhood should be pivotal for living well with dementia.
This should include the whole person.
If we involve people living with dementia in the design of research and services, I feel, a lot of my concerns will be addressed. The ‘Dementia Without Walls’ project from the Joseph Rowntree Foundation, in collaboration with other stakeholders, has truly been outstanding, for example.
I am grateful to the current Government for taking us a long way down the journey. But we’ve only just begun.
